
Abstract
Objective:
Depression has economic consequences not only for the health system, but also for individuals and society. This study aims to quantify the potential economic impact of five-yearly screening for sub-syndromal depression in general practice among Australians aged 45-64 years, followed by a group-based psychological intervention to prevent progression to depression.
Method:
We used an epidemiological simulation model to estimate reductions in prevalence of depression, and a microsimulation model, Health&WealthMOD2030, to estimate the impact on labour force participation, personal income, savings, taxation revenue and welfare expenditure.
Results:
Group therapy is estimated to prevent around 5,200 prevalent cases of depression (2.2%) and add about 520 people to the labour force. Private incomes are projected to increase by $19 million per year, tax revenues by $2.4 million, and transfer payments are reduced by $2.6 million.
Conclusion:
Group-based psychological intervention to prevent depression could result in considerable economic benefits in addition to its clinical effects.
Background
Major depression is a common mental disorder. Taken together with anxiety, it is the largest single cause of disability among both men and women in Australia, and is responsible for 10% and 18% of years lived with disability in men and women, respectively (Begg et al., 2007). Anxiety and depression were second only to ischemic heart disease in terms of the number of disability-adjusted life years (DALYs) lost in the 2003 Australian Burden of Disease and Injury study (Begg et al., 2008). Results from the 2010 Global Burden of Disease study suggest that around 70% of this joint burden of anxiety and depression is attributable to depressive disorders (Whiteford et al., 2013). Other countries have similarly high burdens, with the 2010 Global Burden of Disease study reporting that unipolar depression is the 11th leading cause of disease burden worldwide, up from 15th in 1990 (Murray et al., 2012).
Depression also comes with economic costs. The allocated health care expenditure for depression and anxiety in Australia is substantial, with the most recent estimates totalling $1.4 billion per annum (Australian Institute of Health and Welfare, 2010). Depression reduces productivity and workforce participation (Lerner and Henke, 2008; Beck et al., 2011; Schofield et al., 2008). This may have significant economic consequences for the individuals concerned (Schofield et al., 2011a). People with depression who leave the workforce early have substantially lower incomes and savings compared to their full time employed counterparts (Schofield et al., 2011b; Schofield et al., 2011c).
There is increasing evidence that part of this burden of depression can be prevented, and that at least some interventions are cost-effective (Mihalopoulos et al., 2011a). Recently, Mihalopoulos et al. investigated the health impacts and health costs of interventions to prevent depression and found that a comprehensive group-based psychological intervention following opportunistic screening for sub-syndromal depression in general practice offered good value for money from a health sector perspective, compared to no intervention (Mihalopoulos et al., 2011b).
Preventing depression is likely to result in wider economic benefits. This study will build upon the findings of Mihalopoulos et al. and estimate the impact on labour force participation and personal income of depression prevention using screening and treatment with a group-based psychological intervention in Australians aged 45-64. Recent evidence suggests that group therapy is no less effective than individual therapy (Cuijpers et al., 2008), and on a per patient basis it is cheaper, and therefore more cost-effective, than individual therapy. This age group is considered particularly important as it has a high rate of early retirement associated with depression (Schofield et al., 2008) and will make up an increasing proportion of the working population as Australia’s population ages (Commonwealth of Australia, 2007).
Method
We estimated the extra number of years in the labour force of people aged 45-65 years in 2010 had they not developed depression if a screening and intervention program to prevent the onset of depression were in place. We further estimated the potential increase in the personal incomes of the individuals concerned as a result of staying in the workforce, and the consequences for government revenue.
Depression and labour force participation
The prevalence of depression was estimated from a microsimulation model, Health&WealthMOD2030, which was based on the Australian Bureau of Statistics (ABS) Surveys of Disability, Ageing and Carers (SDAC). Health&WealthMOD2030 models health, labour force participation, personal incomes and savings, and was specifically designed to measure the economic impacts of ill health leading to early retirement of Australians aged 45-64 years.
The base population of Health&WealthMOD2030 was unit record data for those aged 45-64 years extracted from the two Surveys of Disability, Ageing and Carers (SDACs) conducted by the Australian Bureau of Statistics (ABS) in 2003 and 2009 (Australian Bureau of Statistics, 2005; Australian Institute of Health and Welfare, 2010). These nationally representative (Australian) household survey data consist of information on demographic variables (such as age, sex, family type, and state of residence), socioeconomic variables (such as level of education, income, type of home ownership, and benefits received), labour force variables (such as labour force participation, employment restrictions, and retirement), and health and disability variables (such as chronic conditions, health status, type and extent of disability, support and care required) for each individual in the household. The 2003 and 2009 SDAC data were reweighted to reflect the profile of the 2010 Australian population aged 45-64 years by using a reweighting algorithm GREGWT developed and commonly used by the ABS to reweight their survey data (Bell, 2000). The mathematical technique is described in Singh and Mohl (1996) and an implementation of the same algorithm for small area estimation is described in Tanton et al. (2011). The reweighting was done to account for changes in disability and illness, demographics, labour force participation and other features of the population that had occurred between the years for which we have data (2003 and 2009) and 2010.
The SDACs included limited economic data which were presented in ranges. More detailed information on income, government benefit, individual income tax paid and wealth were derived from a separate microsimulation model called the Australian Population and Policy Simulation Model (APPSIM), which is a dynamic population microsimulation model that was developed to provide a snapshot output of the socio-demographic and economic characteristics (such as income and government support payments) of the population in each year (Keegan and Kelly, 2009). It is maintained and developed by the National Centre for Social and Economic Modelling (NATSEM). Detailed economic information such as income and wealth from the APPSIM snapshot output for year 2010 were imputed onto the base population of Health&WealthMOD2030 by identifying persons with similar characteristics on APPSIM and using a process commonly used in microsimulation models called synthetic matching (Rässler, 2002). Ten variables that were common to both datasets and strongly related to income were chosen as matching variables for synthetic matching: labour force status (4 groups), income unit type (4 groups), income quintile (5 groups), receiving/not receiving age pension (2 groups), receiving/not receiving disability support pension (2 groups), sex (2 groups), age (4 groups), hours worked per week (5 groups), highest educational qualification (2 groups) and home ownership (2 groups).
The 2010 prevalence of self-reported depression and the labour force participation rates of those without depression and of those with depression were estimated for each 5 year age group and gender from Health&WealthMOD2030. Labour force participation was defined as being either employed or looking for work. People who were neither employed nor looking for work were categorised as “out of the labour force”. Differences in the labour force participation rates of those with no depression and with depression, adjusted for highest level of education attained and number of co-morbid conditions (Gunn et al., 2012) were estimated by gender and 5 year age group using a binomial regression model with identity link. The age-sex specific differences in median incomes between those who were in the labour force without depression and those who were not in the labour force and who had depression, adjusted for highest level of education attained, were estimated using quantile regression models. This difference in income was considered as the additional income an individual would have if they did not develop depression because of the intervention and remained in the labour force, assuming the rate of employment distribution between full time and part time was the same as for those without depression. Analyses were repeated for total amount of tax paid and government transfer payment received by the individuals to estimate the impacts on income tax collection and government benefit payments, of interventions to prevent depression.
Reduction in the prevalence of depression due to interventions
An epidemiological Markov model was used to predict the percentage reduction in the prevalence of psychiatrically confirmed depression that would have been achieved if a screening program for sub-syndromal depression and group therapy intervention for those identified with sub-syndromal depression had been in place. Full details of the model are available elsewhere (Mihalopoulos et al., 2011a). Briefly, intervention consisted of screening of people who attend general practice for symptoms of depression (by a practice nurse). People who screened positive were then referred to a psychologist for further assessment. If found to be eligible they were offered the intervention consisted of eight group based psychological therapy sessions with a psychologist. The effectiveness of this intervention was based on a meta-analysis of 19 randomised controlled trials (Cuijpers et al., 2008). All studies in this meta-analysis examined the effects of preventive interventions on the incidence depressive disorders and used a standardized diagnostic interview to exclude the presence of a fullblown depressive disorder at baseline and to examine the incidence of depressive disorders at follow-up. The analysis suggested that interpersonal therapy was more effective than cognitive behavioural therapy.
The current model used the same probabilities as used by Mihalopoulos et al. Briefly: 50% of GPs participate in the screening program; the proportions of men and women seeing a GP in any one year were 76% and 86% respectively (Australian Bureau of Statistics, 2009). The proportions who met the criteria for the intervention, agreed to further screening and agreed to undertake the intervention were all sourced from the 2007 National Survey of Mental Health and Wellbeing (NSMHWB) and the trials upon which the analyses were based (Cuijpers et al., 2008).
Assumptions
In modelling the effects of both interventions, we made the following assumptions.
First, we assumed that the percentage reduction in the prevalence of self-reported depression in the SDAC surveys with the screening and intervention program would be the same as the percentage reduction in the prevalence of psychiatrically confirmed depression that was the outcome of the trials reporting on the screening and intervention programs. Second, we assumed that screening would, on average, take place every 5 years, and that this would result in an averaging out of the effects over these years. The original depression model assumed that the effects diminish exponentially over time until less than 7% of the initial effect is left at year 5 (Mihalopoulos et al., 2011a).
Simulation
We estimated the number of additional persons in the labour force for each age-sex group as a result of reduction in psychiatrically confirmed depression prevalence because of the screening and intervention as

Where ΔP(LF)i is the difference in the labour force participation rates between those without depression and those with depression for each age-sex group and AddDepFreei is the reduction in the number of self-reported depression cases (i.e. additional number of depression free persons) in each age-sex group because of interventions, which is estimated as

Where Depi is the estimated number of self-reported depression cases in 2010 and DepRedi is the percentage reduction in psychiatrically confirmed depression prevalence for each age sex group due to interventions.
The expected number of additional persons in the labour force in 2010 was then multiplied by the adjusted difference in median incomes between those who were in the labour force and had no depression, and those who were not in the labour force and who had depression, to estimate the total additional income they would have collectively earned if they did not have depression and stayed in the labour force. In order to simulate the results for the entire Australian population of age group 45 to 64 years, we performed a weighted analysis using the weights that represented the number of similar individuals in the 2010 Australian population. All modelling was done separately for males and females. To derive uncertainties around the estimates, 1000 bootstrap replicate datasets were created and 95% uncertainty intervals were derived using non-parametric bootstrapping methods.
Ethical approval was not required, but the research conformed to the Helsinki Declaration and to local Australian legislation.
Results
Out of 25,104 records in Health&WealthMOD2030 base population of 45-64 years old, 1087 reported having depression. Once weighted, this represented about 227,900 Australians aged 45-64 years old who had self-reported depression (3% of men and 5% of women) in 2010 (Table 1). Opportunistic screening for sub-syndromal depression in general practice and treatment followed by group therapy every 5 years was estimated to prevent around 2.3% of these cases. As labour force participation would have been higher with intervention, there would be commensurate increases in income.
Self-reported depression by age group and sex, Australia 2010.
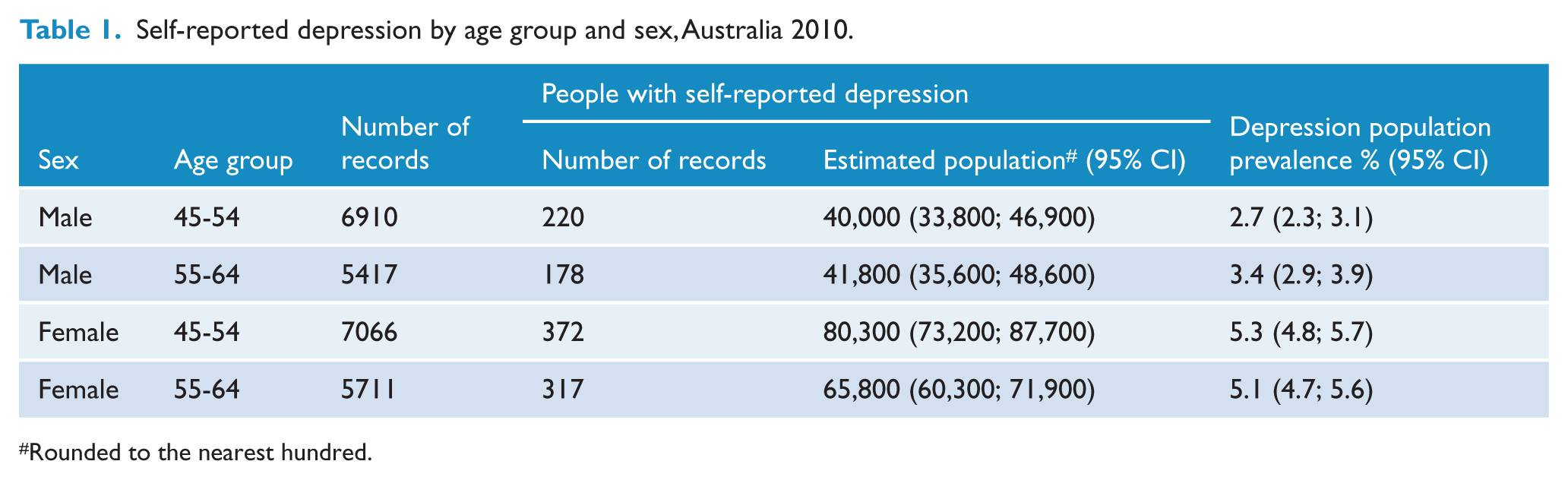
Rounded to the nearest hundred.
Men in this age group, who have depression, had a 14-17 percentage-point lower probability of being in the labour force than those who do not have depression. For women, that probability is lower by 9 percentage-points at age 45-54 years and 5 percentage-points at age 55-64 years (Table 2).
Association of depression with labour force participation and per capita economic outcomes, Australia 2010.
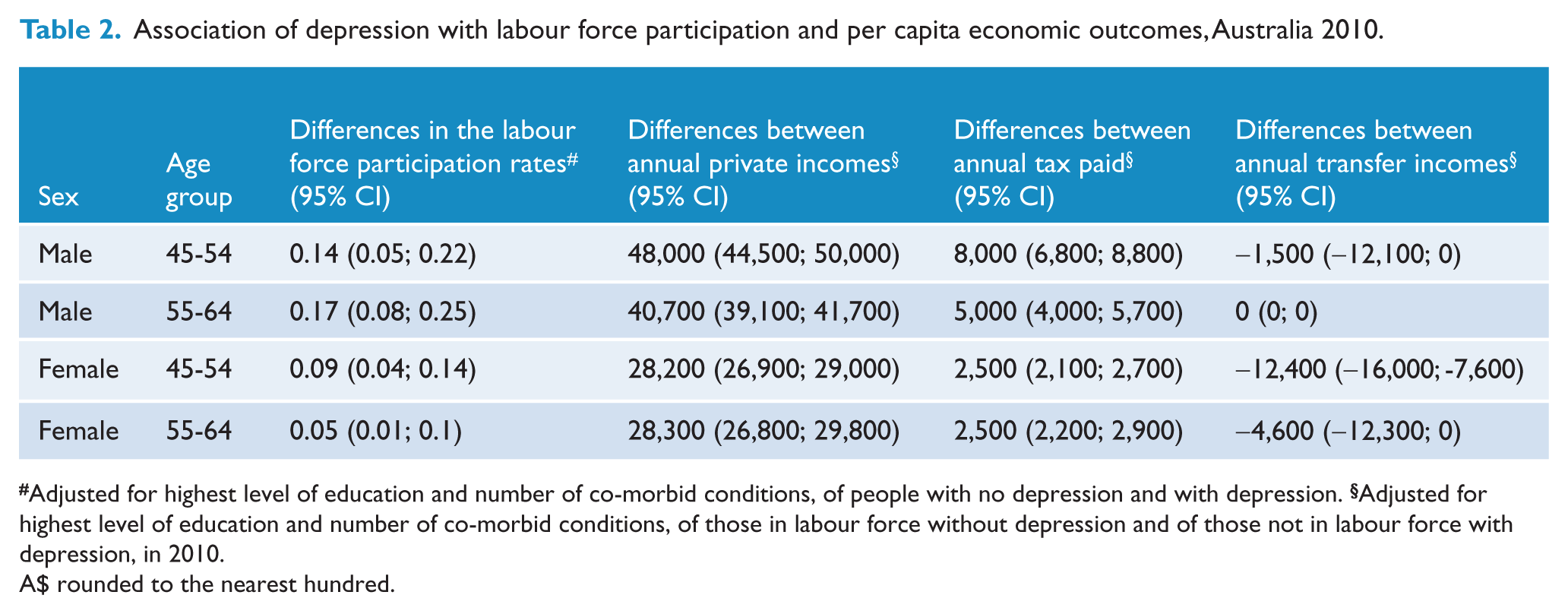
Adjusted for highest level of education and number of co-morbid conditions, of people with no depression and with depression.
A$ rounded to the nearest hundred.
The income difference between those in the labour force without depression and those not in the labour force with depression was about $48,000 per year for men aged 45-54 years and $28,200 for women of the same age group. While the income difference was higher for men aged 45-54 years compared to the older age group of 55-64 years, they were similar for both age groups among women.
Men aged 45-54 years who were not in the labour force with depression paid around $8,000 less in taxes and received $1,500 more in transfer incomes every year compared to those who were in the labour force and who did not have depression, so the net increase in government revenue was $9,500 per year per person for this age group. For women of this age group, the net increase was about $14,900 (Table 2). The annual increase in government revenue from the older age group of 55-64 years was slightly lower compared to the younger age group, with $5,000 per person for men and $7,100 for women.
Table 3 shows that screening plus group therapy could prevent about 5,200 prevalent cases of depression among of 45-64 year old Australians, and add 280 men and 240 women to the labour force. Private incomes are estimated to increase by a total of $19.3 million per year, tax revenues by $2.4 million, and transfer payments would be reduced by $2.5 million.
Effects of group-based psychological intervention on depression prevalence and national impacts on labour force participation and economic outcomes, Australia 2010.
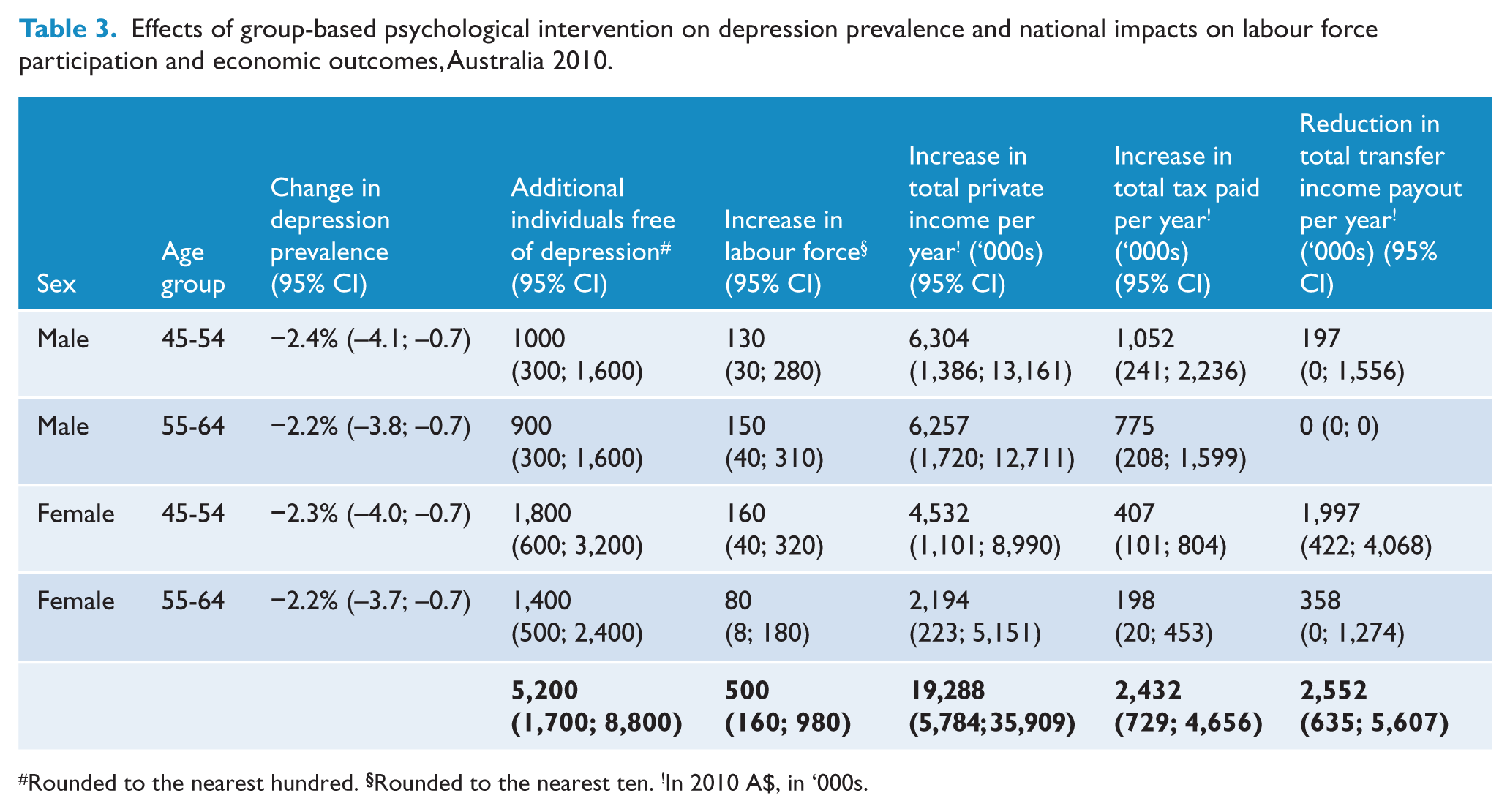
Rounded to the nearest hundred.
Discussion
Summary of findings
In this paper we have estimated the potential impact of a depression prevention program on labour force participation and income generation among people at high risk of developing depression. The results suggest that considerable benefits, in terms of both additional working years and increased personal income, could be made by introducing either a group therapy intervention to prevent depression. On average, those who were able to remain in the workforce as a result of the prevention of depression would earn between $28,000 and $48,000 more per year, and net government revenues would increase by around $5 million.
Limitations
Some caution needs to be taken in interpreting these findings. We have assumed that the reduction in self-reported prevalence of depression from a depression intervention would be similar to the reduction in depression diagnosed with validated diagnostic instruments. Although this seems plausible, it has not been assessed. It is reassuring, however, that the 2007 National Survey on Mental Health and Wellbeing found 12-month prevalences for medically diagnosed depression that are very close to the self-reported prevalences we used in this study (3.1% among men and 5.1% among women aged 16-85 years, compared to 3% and 5%, respectively, in our study) (Australian Bureau of Statistics, 2009). Secondly, we assumed that the interventions would result in uniform reductions in depression prevalence across all levels of severity. It is possible that the effect would be smaller for more severe forms of depression than for less severe cases, in which case our approach may have led to overestimation of the effect on early retirement due to depression. Evidence on this point is lacking. To the extent that persons who retired with depression no longer had the disorder when they were interviewed, this could have led us to underestimate the workforce benefits of depression prevention.
Interpretation
Our results should be considered to be a conservative estimate of the impact of depression prevention interventions due to the approach taken. Firstly, we have only captured the lost working years and income among those who retire. Among those who continue in the workforce, depression is likely to reduce productivity through absenteeism and reduced productivity at work. The size of these effects is incompletely known (Donohue and Pincus, 2007). Secondly, the assumptions used for estimating reductions in prevalence were based on conservative levels of participation in the screening program by both GPs and patients. If participation rates could be increased, there would be greater reductions in the incidence of depression with consequent increases in workforce participation.
On the other hand, in a situation of high unemployment, a larger number of people in the labour force may manifest itself as an increase in the number of unemployed, rather than in the number of working persons. In that case, the economic results suggested by our analysis may not fully materialise.
This study shows that increased labour force participation as a result of preventing depression is likely to benefit not only the individuals concerned, but also has impacts on taxes and government support payments due to lost labour force participation. Previous studies have shown that in the 45 to 64 year age group persons who are out of the labour force due to depression pay virtually no tax and receive $228 per week in transfer income whereas those in employment pay $344 in tax and receive only $9 in benefits, on average (Schofield et al., 2011c). This is in addition to expenditure for depression-related health care.
Conclusion
Government reports have highlighted population ageing and labour shortages as potential pressures threatening the Australian economy (Commonwealth of Australia, 2007). Most other developed countries face similar challenges associated with the ageing of their populations, and many newly developed countries like China will soon see their dependency ratios (i.e. the ratio of inactive elderly to the total labour force) deteriorate as well (Organisation for Economic Co-operation and Development, 2008). Keeping a greater proportion of experienced, older workers in the labour force is of increasing concern to governments. This study suggests that prevention of depression with group-based interventions may increase labour force participation as well as incomes for the individuals concerned.
Footnotes
Author contributors
JLV: Concept, design, analysis up to the point of change in depression prevalence, write-up. RNS: Analysis from the point of change in depression prevalence; tables; critical review of manuscript. CM: Input on intervention effectiveness and data sources; critical review of manuscript. MEP and EJC: Discussion of design and analysis; critical review of manuscript. DJS, SJK and RT: Model construction and analysis; discussion of design and analysis; critical review of manuscript. All authors have read and approved the final manuscript.
Funding
This study is funded by the Australian Research Council (LP100100158), and Pfizer Australia is a partner to the grant.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.