
Abstract
Keywords
Major depressive disorder (MDD) affects 2.3% of Australian children and adolescents [1]. However, the cost-effectiveness of recommended treatments has not been assessed in this population. Clinical practice guidelines recommend cognitive behavioural therapy (CBT) as the treatment of first choice because its efficacy is supported by evidence from randomised controlled trials (RCTs) [2], [3].
Pharmacological intervention is currently recommended as a second-line treatment [2], [3]. However, a more recent review of the research literature suggests that selective serotonin reuptake inhibitors (SSRIs) might also be considered as a first-line treatment [4].
As part of the Australian Assessing Cost-Effectiveness (ACE) – Mental Health project [5] we assessed the incremental cost-effectiveness of CBT and SSRIs for the treatment of MDD in children and adolescents. Both treatments were assessed as first-line therapy with current practice as the comparator. Selective serotonin reuptake inhibitors have also been assessed as a second-line treatment with no further treatment as the comparator.
Method
The incremental cost-effectiveness ratio (ICER) is calculated as the cost (A$) per disability-adjusted life year (DALY) saved. Children and adolescents eligible for the intervention are those aged 6–17 years in the Australian population in the year 2000 who are currently seeking care (‘consulting’) for MDD, but would have received types of care other than evidence-based medicine (EBM) under current practice (Fig. 1). All incident episodes of MDD in the year 2000 are included. For SSRIs as a second-line treatment, the eligible group is those children who do not remit by the end of treatment with CBT or do not adhere to treatment with CBT (Fig. 2). Of these, we assume that between 50% and 90% will actually be offered treatment with SSRIs.
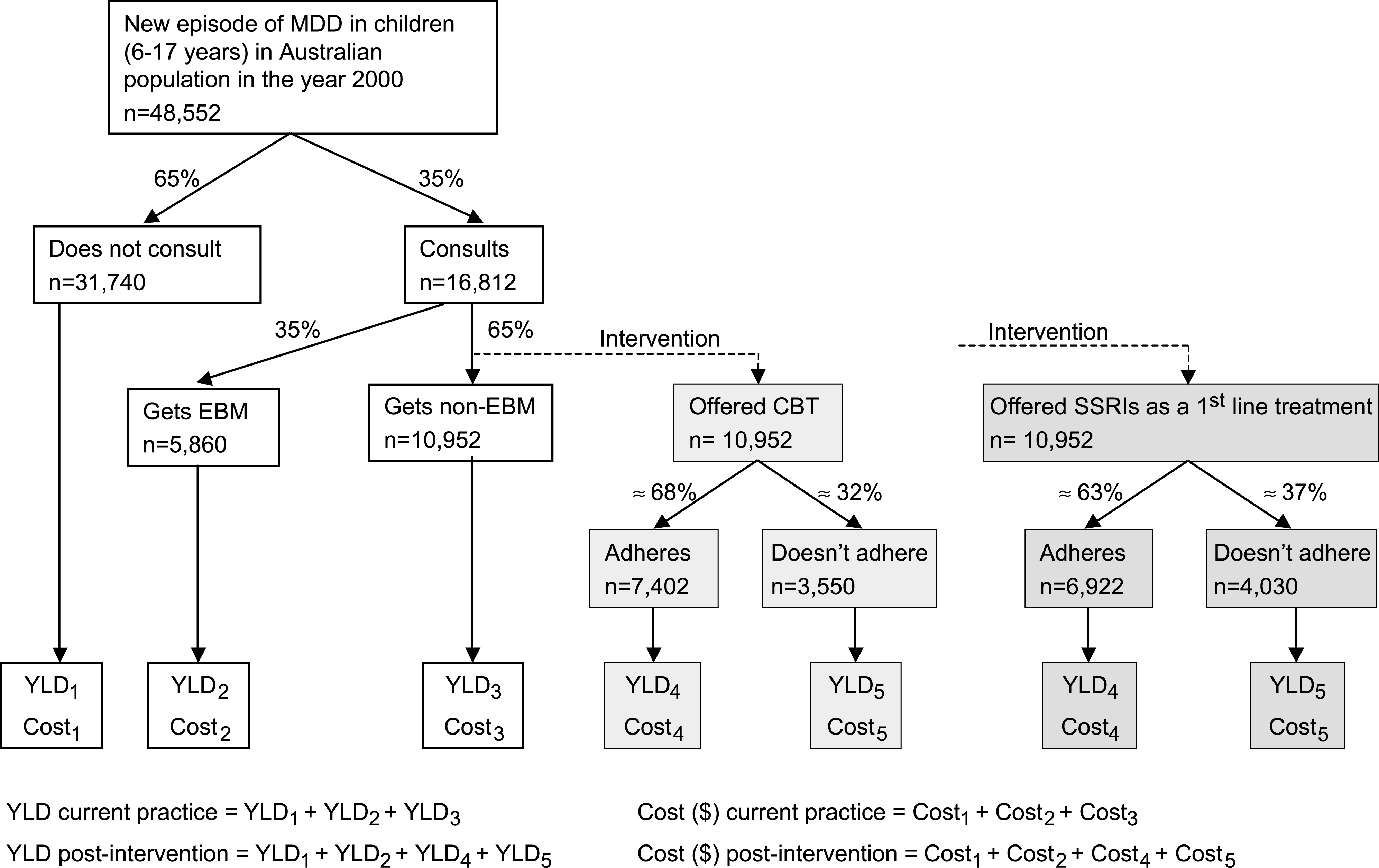
Pathway analysis for current practice (white boxes) and for cognitive behavioural therapy (CBT) and selective serotonin reuptake inhibitors (SSRIs) interventions (light and dark boxes, respectively). EBM, evidence-based medicine; GP, general practitioner; MDD, major depressive disorder; YLD, years lived with disability.
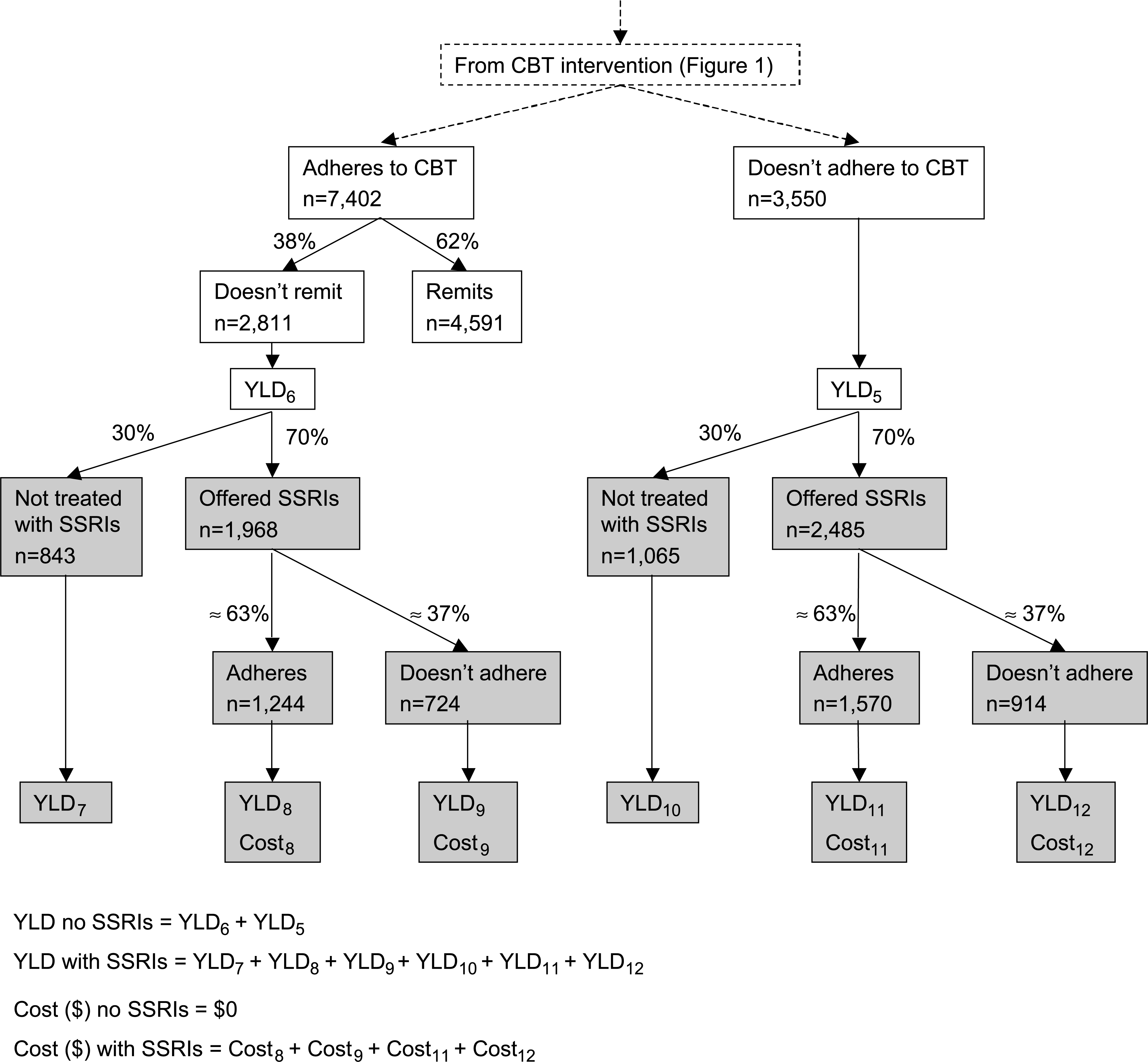
Pathway analysis for selective serotonin reuptake inhibitors offered as a second-line treatment (shaded boxes). The comparator is no further treatment following treatment with cognitive behavioural therapy (CBT). YLD, years lived with disability.
Health benefits are measured for the duration of the episode of MDD. Costs are measured for the duration of the intervention. Since the time horizon is less than one year, costs are not discounted. The perspective is that of the health sector, including government costs (both Commonwealth and states/territories) and out-of-pocket costs for patients and their families, that is drug and service costs.
Interventions
CBT
We model 12 × 1 hour individual sessions of CBT plus two parent/family sessions over 14 weeks (based on expert opinion and randomised controlled trials of CBT). A general practitioner (GP) visit for diagnosis and referral is also included. Four different provider scenarios are costed, with only the cost of the intervention and who bears the cost (government or patient) differing between scenarios. These are: private psychologist; public psychologist; private psychiatrist; and public psychiatrist.
SSRIs
We model 9 months of treatment with an SSRI, which includes 3 months for the acute phase and 6 months for continuation treatment (based on expert opinion and clinical practice guidelines [3]). The dose per day modelled is 20 mg fluoxetine, citalopram or paroxetine, 50 or 100 mg sertraline or 100 mg fluvoxamine [6], [7]. Fourteen doctor visits are included, assuming weekly visits in the first month, every two weeks for two months, and then monthly visits (based on expert opinion). We assume the proportion of patients consulting with a GP, paediatrician or private psychiatrist is the same as currently happening in those consulting (i.e. 53%, 31% and 16%, respectively [1]). Two different scenarios for the intervention are analyzed: SSRIs offered as a first-line treatment; and SSRIs offered as a second-line treatment.
Current practice
Current practice for the treatment of MDD was determined from the 1998 National Survey of Mental Health and Wellbeing – Child and Adolescent Component (NSMHW-CA) [1] in those with MDD in the previous 12 months (n = 88). A consult is defined as an attendance for emotional or behavioural problems during the past 6 months with a family doctor, private paediatrician, private psychiatrist, private psychologist or social worker, mental health clinic, hospital emergency department, hospital-based department of psychiatry, any other hospital based outpatient department or stayed overnight in a hospital.
Of those who consulted (35%), these were further split into treatment with EBM (12%) or non-EBM (23%). We defined treatment with SSRIs and/or CBT as EBM. Since there is not a specific question asking about CBT in the survey, we assumed that those who stated they had received counselling and had made at least four visits in the previous 6 months to a private psychiatrist, private psychologist or social worker, hospital psychiatry department or mental health clinic, had received CBT [1], which applies to 9% of the survey sample. Consultation with experts suggests that even these conservative assumptions are likely to have overestimated the number of children actually receiving CBT. Children and adolescents who we defined as receiving non-EBM under current practice each averaged 4.4 visits to a GP, 0.8 visits to a paediatrician, 0.1 visits to a private psychiatrist and 0.2 visits to a private psychologist or social worker [1].
Assessment of benefit
Benefits are calculated by a two-stage process. The first stage involves the estimation of the health gain that could be attributed to each intervention using the DALY. The second stage involves the assessment of issues that either influence the degree of confidence that can be placed in the cost-effectiveness ratios (such as the level of available evidence), or broader issues that need to be taken into account in decision-making about resource allocation (such as equity and acceptability to stakeholders).
Stage one: measurement of the health gain
There is no evidence in the literature that CBT or SSRIs can cause or prevent death, so only a change in the years lived with disability (YLD) component of the DALY is modelled. YLD are calculated as incidence × duration × the disability weight (DW).
YLD for the current practice comparator
To estimate the number of incident cases in the year 2000 we assumed that the prevalence rates calculated from the 1998 NSMHWCA [1] still apply in 2000 and that incidence can be derived from prevalence by using the formula: 1-year incidence = 1-year prevalence/(1 ++ average duration). This 1-year incidence figure (1.5%) is applied to Australian population figures for 6–17 year-olds in June 2000 (Australian Bureau of Statistics, Time series spreadsheet 3201.0) to give 48 552 incident episodes of MDD.
The average duration of an episode of MDD was calculated using the spread of durations found in the Oregon Adolescent Depression Project [8]. While the average duration of an episode of MDD is 26.7 weeks there is a difference in the average duration of an episode between those consulting and those not consulting for their MDD. We assume that there is a lag from onset of MDD to treatment of 4 weeks (range 2–6 weeks) so that children with episodes of 4 weeks or less would remit before getting to treatment (25.5%). Conversely, all children treated would have durations greater than the lag. Thus, we derive an average duration of 20.8 weeks in those children not consulting and 34.8 weeks in those consulting.
The disability weights (DW) used are based on the Dutch weighting system [9]. These are 0.14 for mild, 0.35 for moderate and 0.76 for severe MDD. Composite DWs were calculated separately for those who: did not consult; consulted and received EBM; and consulted and received non-EBM under current practice, based on the spread of severities in the Australian population. We extrapolated this severity information from the young adults (18–34 years) in the adult National Survey of Mental Health and Wellbeing [10] because the numbers with depression in the NSMHW-CA [1] were too small to obtain reliable estimates of the spread of severity of depression. We used the Mental Component Score of the SF-12 [11], which has a mean population value of 50 and a standard deviation of 10. We classified cases into: severe (> 2.5 SD below mean, i.e. < 25); moderate (> 1.5–2.5 SD below mean, i.e. 25–34.9); and mild (> 0.5–1.5 SD below mean, i.e. 35–44.9). The proportion of cases in each severity category is multiplied by the appropriate DW for the category to get a weighted average DW for those in each group. The resulting DWs are: ‘did not consult’ = 0.270; ‘received EBM’ = 0.397; and ‘received non-EBM’ = 0.417.
YLD for the comparator for SSRIs as a second-line treatment
To derive the average duration of an episode of MDD before becoming eligible for treatment with SSRIs under this scenario we assumed an average of 2 weeks treatment with CBT before being treated with SSRIs for those who do not adhere to CBT and 14 weeks of CBT for those who adhere but do not remit. This is in addition to the 4-week lag to treatment with CBT. This gives an average duration of 41.4 weeks in those not adhering to treatment with CBT and 74.0 weeks in those not remitting by the end of treatment with CBT. We assumed no health benefit from the prior treatment with CBT, so used a disability weight of 0.417 at baseline, consistent with the modelling of SSRIs as a firstline treatment.
Determining the reduction in YLD with treatment
The reduction in severity, and hence YLD, was modelled using the effect size and both the ‘conversion factor method’ and the ‘survey severity method’ [5] to translate the effect size into a reduction in the DW. For the ‘conversion factor method’ we multiplied the effect size by the DW conversion factor. This conversion factor is an average change in the DALY disability weights for the equivalent of a standard deviation change in severity for the particular mental disorder [12]. For the ‘survey severity method’ the effect size is applied directly to the Mental Component Score, which was used to determine the average DW at baseline. The severity of respondents is then reclassified and a new average DW calculated. The difference in average DW is the change attributed to treatment [5].
The effect size was calculated from a meta-analysis of the relevant RCTs. Although the interventions do impact on the duration of the episode of MDD, we assumed that the effect size captures the effects of both the reduced severity and duration. Reductions in the DW were only applied to the time from the commencement of the intervention. For cases not adherent to treatment no reduction in DW has been modelled (although they do incur costs of the treatment provided).
Meta-analysis
Trials of CBT and SSRIs were identified from published metaanalyses, searches of the Cochrane Controlled Trials Register and Medline, from reference lists in included trials, review articles, books and clinical practice guidelines and from authors of published trials. To be included, trial participants had to be less than 18 years and have diagnosed depression (MDD or dysthymia). For CBT seven studies fitted the inclusion criteria [13–19]. However, the study by Reed [14] could not be included in the calculation of the effect size for CBT due to lack of continuous outcome measures. For SSRIs four RCTs fitted the inclusion criteria [20–23].
The effect size (standardized mean difference) was calculated using Hedges’ g and the random effects method of DerSimonian and Laird [24]. We first calculated an effect size for each study by averaging across the relevant outcome measures within the study. All continuous outcome measures related to depression (including anxiety and mood) and health-related quality of life were included. Clinician, parent and child/adolescent reported measures were included. Some outcome measures that were considered to be relevant could not be included because data were not presented in a way that could be incorporated into the calculation of the effect size (e.g. data presented in figures only). For the study by Simeon et al. [20] no data were presented in the paper but it was stated that there were no significant differences between the treatment and control groups. Thus, an effect size of zero was assumed. The weighted mean effect size for CBT is 0.41 (95% CI = 0.15–0.67) and for SSRIs is 0.29 (95% CI = 0.11–0.46). Some unexplained heterogeneity was present in the effect size for CBT (Q = 12.04, df = 7, p = 0.099) but not for SSRIs (Q = 0.90, df = 3, p = 0.8).
Adherence
It was assumed that the completion rate of the treatment group in the RCTs reflects the best possible adherence with treatment. No longitudinal studies measuring adherence to CBT or SSRIs were available for MDD in children and adolescents so a minimum adherence rate of 50% was used in the uncertainty analysis (Table 1). This was done to better reflect what could be expected under routine health service conditions where results may vary due to the motivation of clinicians and patients, the availability of skilled clinicians and the capacity to vary the intervention to suit the needs of the patient.
Critical parameter values, uncertainty distributions and sources of information for determining the health benefit and costs
Stage two: the second stage filter criteria
The first stage of measuring benefit described above is characterized by a reliance on data sets and the application of quantitative methods based on health economics and epidemiology. The second stage incorporates, explicitly, broader aspects where decisions rest heavily on judgement and notions of ‘due process’. The filters chosen for the ACE–MH study were ‘strength of evidence’, ‘equity’, ‘feasibility’ and ‘acceptability to stakeholders’ [5].
Assessment of costs
Pathway analysis was used to identify the component activities of the interventions and their current practice comparator (Figs 1 and 2). Resource usage (i.e. dosage, number of visits, etc.) for the component activities was estimated from the published literature and supplemented by expert advice. Unit costs and data sources are shown in Table 2. Costs that would have been incurred under current practice are subtracted from the intervention (and non-adherence) costs to obtain the incremental cost.
Summary of unit cost information, data sources and assumptions
Children and adolescents who don't adhere to treatment with CBT or SSRIs incur some costs but no health benefit. However, there are no data available on their care-seeking behaviour. Thus, it is assumed that the cost of non-adherence is (on average) the same as the cost of non-EBM. However, for SSRIs as a second-line treatment, we assume that these patients behave differently from the average patient receiving non-EBM. Thus, for those not adherent to SSRIs as a second-line treatment, we model the cost of filling one or two scripts of the SSRI and 1–3 doctor visits (in addition to the GP visit for referral to a paediatrician or psychiatrist).
Uncertainty analysis
Simulation-modelling techniques were used to allow the presentation of an uncertainty range around the health benefits, costs and ICERs (Table 1). @RISK software [25] was used to conduct Monte Carlo simulations, which allow multiple recalculations of a spreadsheet, each time choosing a value from the specified distribution for each input variable (shown in Table 1). We used 2000 iterations for each of the two methods for translating the effect size into a change in the DW (i.e. the ‘conversion factor method’ and the ‘survey severity method’). Thus, the final results are based on the 2000 ++ 2000 iterations. Median values were calculated because results are not normally distributed. The ranges presented can be interpreted as the range within which the true result lies with 95% certainty.
Uncertainty analyses are used to address issues of uncertainty in the results due to sampling error (e.g. in the meta-analyses) and the need to make assumptions due to the lack of evidence for some parameters (e.g. the lag to treatment).
In addition to the uncertainty range, the @RISK analysis can also show which model parameters contribute most to the uncertainty in the results. We list the input variables that contribute to overall uncertainty around the cost-effectiveness ratios with a regression coefficient of ± 0.30 or greater.
Results
Cognitive behavioural therapy by public psychologists (or other effective providers at a similar salary level) is the most cost-effective intervention for child and adolescent depression at A$9000 per DALY saved (95% UI A$3900 – A$24 000) and is also the second most affordable first-line treatment option for the government at an incremental cost of A$3.7 million (95% UI A$1.9 – A$6.7 million) (Tables 3 and 4). CBT by other providers is likely to have ICERs < A$50 000 per DALY (> 80% chance). SSRIs are a cost-effective option, both as first-line and second-line treatments (Table 4). However, CBT has greater effectiveness in children and adolescents than SSRIs and therefore greater total YLD saved (Tables 3 and 4). Note that the costs and benefits of SSRIs as a second-line treatment are additional to those incurred from first-line treatment with CBT.
The incremental benefits, costs and cost-effectiveness of cognitive behaviour therapy for major depression in children and adolescents compared with current practice
The incremental benefits, costs and cost-effectiveness of selective serotonin reuptake inhibitors (SSRIs) for major depression in children and adolescents
The major contributors to uncertainty around the ICERs for CBT are the effect size and the variation factor around the cost to patient of private psychologist visits and cost to government of public psychologist and public psychiatrist visits. For SSRIs, the effect size is the major contributor to uncertainty around the ICERs. Other parameters contributing to uncertainty around the health benefit (YLD) and total cost of CBT and SSRIs are the proportion of children and adolescents currently receiving non-EBM, adherence with treatment and the prevalence of MDD.
A consideration of the second stage filters for each intervention is shown in Table 5.
Consideration of second stage filters
Discussion
Economic analysis raises important issues as to what constitutes ‘value-for-money’. It is not uncommon for a threshold ICER (or ‘shadow price’) to be set as a guide to assist decision-making. In ACE–MH, for example, an ICER of A$50 000 per DALY has been used. However, this should not be over-interpreted or taken out of context. It is important to reflect, for example, on how well the ICER captures the various dimensions of ‘benefit’ in mental health. The second stage filters are designed to allow the ICERs to be placed within a broader decision context.
Cognitive behavioural therapy is a cost-effective intervention for major depression in children and adolescents (Table 3). Whether delivered by private or public psychologists or psychiatrists the cost-effectiveness ratios are likely to be below our threshold of $50 000 per DALY saved (> 80% chance). Clearly, CBT delivered by a public psychologist is the most cost-effective option and is also the second most affordable option for the government at about $3.7 million per year if all eligible patients were offered treatment (Table 3). From the perspective of the government, CBT delivered by a private psychologist is the cheapest option. However, the fact that all treatment costs are borne by the patient and total more than A$1600 per episode suggests that the intervention would be unaffordable for many patients. This is likely to have a significant impact on both uptake and adherence to the treatment. SSRIs are also a costeffective intervention both as a first-line treatment and as a second-line treatment for MDD in children and adolescents (Table 4). However, SSRIs are less effective than CBT, resulting in lower total health benefit.
The higher effect size for CBT (compared to SSRIs) may reflect the greater remission with CBT, and hence shorter duration of the episode of depression. With CBT 62% of patients remitted by the end of treatment compared to 39% of the control groups [13–18]. With SSRIs 46% of patients remitted by the end of treatment compared to 30% of the placebo control groups [21–23]. Thus, the odds of remission are 2.59 (95% CI = 1.66–4.03) with CBT and 2.03 (95% CI = 1.40–2.95) with SSRIs. Both CBT and SSRIs have lower effect sizes (and hence are less cost-effective) in children and adolescents than in adults (i.e. 0.41 vs. 0.82 in adults [26] for CBT and 0.29 vs. 0.55 [27] in adults for SSRIs).
We could find only two other studies of the costeffectiveness of CBT for depression in the literature and none looking at its cost-effectiveness for children and adolescents [28], [29]. There are several economic evaluations of SSRIs for the treatment of depression (reviewed in Frank et al. [30]) but no studies in children and adolescents. However, the applicability of the overseas studies in adults needs to be carefully assessed, due to differences in health system design and cultural context.
When deciding to model alternative scenarios for the provider of CBT, we assumed that psychologists and psychiatrists have equal efficacy but this has not been proven. Nor is it clear whether other providers, such as GPs, social workers and nurses, are as effective or whether this is dependant on the amount of training they have in CBT. For the SSRI intervention we have assumed equal efficacy of the different types of SSRI although the evidence is limited to fluoxetine and paroxetine.
In the course of this analysis, several gaps in the research were noted. In terms of defining the CBT intervention there are no RCTs that investigate the optimum duration of treatment with psychological therapy in children and adolescents. Most of the studies in our meta-analysis investigate a set course of CBT, ranging from 5–16 sessions for patients and 0–8 sessions for parents. Only one study has looked at continuation treatment [18], with inconclusive results, and none have looked at the effect of varying the length of treatment or the number of sessions of CBT. This is important because it has implications for the cost, uptake and adherence to treatment. In terms of defining the SSRI intervention, there are no RCTs that investigate the optimum duration of treatment in children and adolescents. Most studies are limited to the acute phase of MDD and last for a maximum of 9 weeks. We are aware of only one longer-term study, which continues for almost one year, but the results have not yet been published in a peer-reviewed journal [31]. Finally, there are no RCTs in children and adolescents that compare the efficacy of combining pharmacological therapy with psychological therapy compared to treatment with a single therapy.
A significant issue in this cost-effectiveness analysis is the use of mean values to describe the natural history of MDD. For example, we use a mean duration of an episode of 27 weeks, although the duration probably varies from as little as 2 weeks to more than 5 years [8]. This use of mean values was necessary for a number of reasons, the most important being the limited data available on the natural history of depression (in children and adolescents particularly) and the limited information available from the treatment literature. Randomized controlled trials of treatment often exclude children with comorbid conditions and/or do not present the results stratified by subgroups. Thus, attempts to incorporate the heterogeneity of depression into our results are not supported by data. However, the results are likely to be a good reflection of what would happen ‘on average’ and allow meaningful comparisons between treatments. The results of these analyses are not intended to be a prescription for individual patients and we caution against generalizing the results to the most severe patients (e.g. inpatients) as these patients are not included in the published RCTs or the community study of depression duration [8] used in these analyses.
Another issue for this analysis has been the use of an episode-based analysis of MDD, which was necessary due to the limited data on the natural history of depression in children and adolescents. The disadvantage of this method is that the longer-term health benefits related to prevention of new episodes or delay in relapse or recurrence due to the intervention cannot be measured. This is particularly important for CBT, which in adult studies has been shown to prevent new episodes while not incurring ongoing costs [32].
The strengths of the current analysis include the use of the best available evidence for all parameters, the use of Australian data, calculation of ICERs for local circumstances and extensive uncertainty analyses. We have also undertaken steps through the second stage filters to incorporate a broader range of considerations that impact on resource allocation decisions. The limitations of the study are the lack of overall quality of life data in the calculation of the effect size, which is mostly limited to symptom measures, and the measurement of severity in DALY disability weights [5]. While the cost side is more straightforward, there are two issues to note. First, the estimation of cost offsets for CBT is very conservative (e.g. does not include impact of reduced use of antidepressants on PBS or resource savings resulting from reduction in relapse and severity of depression). Second, the economic analysis assumes ‘steady-state’ operation and costs associated with implementation (e.g. costs associated with ensuring adequate training and accreditation of providers) have not been factored in.
For several parameters, we could not find any data, and have relied on the advice of experts (Table 1). Because only 31 children and adolescents with MDD in the NSMHW-CA [1] had sought treatment in the previous 6 months estimates of the proportion of children treated with CBT, SSRIs and non-EBM are uncertain. The collection of further data on the treatment of depression in children and adolescents in Australia is required. However, it is important to note that these parameters only impact on the total cost and total benefit of the intervention because they influence the total number of children eligible for the intervention. They do not affect the cost-effectiveness ratio.
In conclusion, there are strong economic grounds to improve access to CBT as a first-line treatment for child and adolescent depression, especially for publicly funded psychologists as providers. The Commonwealth initiative to improve access to psychologists through GPs (as being piloted in the ‘Better outcomes in mental health care’ initiative [33]) shows that funding mechanisms outside of Medicare are feasible. Should no further action be taken, SSRIs may become the first-line treatment by default due to their greater affordability for consumers and easier access. However, readers should also note the debate that has arisen since this research was conducted over the efficacy and safety of antidepressants in children and adolescents [34]. Key decision points for policy makers regarding the CBT intervention are: public or private provider; psychologist or psychiatrist; or a mix of providers including other suitably trained health professionals (social workers, nurses, GPs). However, use of providers other than psychologists requires attention to training and accreditation if similar effectiveness is to be achieved. Greater use of publicly funded psychologists will require attention to ensuring an adequate workforce, particularly in outer metropolitan and rural regions.
Caveat
The ACE–Mental Health project was jointly funded by the Australian Department of Health and Ageing, Mental Health and Suicide Prevention Branch and the Department of Human Services, Mental Health Branch, Victoria in recognition of the importance of research into the cost-effectiveness of interventions in mental health treatment and care. This work draws upon, but is also limited by the available research and the assumptions necessary to complete the work.
The results of the analyses provide valuable material, likely to contribute to future policy deliberations by all service providers. Conclusions drawn from the economic evaluations should be considered within the context of the second stage filter process, which qualifies the results, taking into account issues of equity, feasibility, strength of evidence and acceptability to stakeholders. This second stage filter process addresses some of the practical considerations required for changes in actual service practice.
Footnotes
Acknowledgements
Principal investigators for the project are: Theo Vos, Rob Carter and Gavin Andrews. Analyses draw on the Child and Adolescent Component of the National Survey of Mental Health and Wellbeing which was sponsored by the Mental Health and Suicide Prevention Branch of the Department of Health and Ageing, facilitated by the National Collaborating Group, and conducted by staff in the Department of Psychiatry at the University of Adelaide. The average cost of various types of medical attendances and the various forms of SSRI were obtained from Medicare Benefits Schedule and Pharmaceutical Benefits Scheme data from the Department of Health and Ageing. We thank Kristy Sanderson, Jeremy Anderson, Peter Birleson, Colin Brown, Neil Coventry, Michael Gordon, Richard Harrington, Tony Lawrence and Jenny Smith for advice on various aspects of the analysis.
We thank members of the ACE–Mental Health steering committee for their input into the project: David Barton, Graham Burrows (Chair), Sue Caleo, Vaughan Carr, Dermot Casey, Joy Easton, William Hart, Helen Herrman, Barbara Hocking, Assen Jablensky, Anthony Jorm, Lyn Littlefield, Patrick McGorry, John McGrath, Paul Morgan, Lorna Payne, Deb Podbury, Kristy Sanderson, Suzy Saw, Bruce Singh, Bruce Tonge, Ruth Vine, Harvey Whiteford.