
Abstract
Objectives:
We aimed to investigate antidepressant use, including the class of antidepressant, in mid-age and older Australians according to sociodemographic, lifestyle and physical and mental health-related factors.
Methods:
Baseline questionnaire data on 111,705 concession card holders aged ⩾45 years from the 45 and Up Study—a population-based cohort study from New South Wales, Australia—were linked to administrative pharmaceutical data. Current- and any-antidepressant users were those dispensed medications with Anatomical Therapeutic Chemical classification codes beginning N06A, within ⩽6 months and ⩽19 months before baseline, respectively; non-users had no antidepressants dispensed ⩽19 months before baseline. Multinomial logistic regression was used to calculate adjusted relative risk ratios (aRRRs) for predominantly self-reported factors in relation to antidepressant use.
Results:
Some 19% of the study population (15% of males and 23% of females) were dispensed at least one antidepressant during the study period; 40% of participants used selective serotonin reuptake inhibitors (SSRIs) only and 32% used tricyclic antidepressants (TCAs) only. Current antidepressant use was markedly higher in those reporting: severe versus no physical impairment (aRRR 3.86(95%CI 3.67–4.06)); fair/poor versus excellent/very good self-rated health (4.04(3.83–4.25)); high/very high versus low psychological distress (7.22(6.81–7.66)); ever- versus never-diagnosis of depression by a doctor (18.85(17.95–19.79)); low-dose antipsychotic use versus no antipsychotic use (12.26(9.85–15.27)); and dispensing of ⩾10 versus <5 other medications (5.97(5.62–6.34)). Sociodemographic and lifestyle factors were also associated with use, although to a lesser extent. Females, older people, those with lower education and those with poorer health were more likely to be current antidepressant users than non-users and were also more likely to use TCAs-only versus SSRIs-only.
Conclusions:
Use of antidepressants is substantially higher in those with physical ill-health and in those reporting a range of adverse mental health measures. In addition, sociodemographic factors, including sex, age and education were also associated with antidepressant use and the class of antidepressant used.
Introduction
Antidepressant medications are among the most highly prescribed medications in Australia, and use has been increasing over time. In 2011, 89 defined daily doses (DDD) (WHO Collaborating Centre for Drug Statistics Methodology, 2012) of antidepressants were dispensed per 1000 people per day (1000/day) in Australia, up from approximately 45 DDD/1000/day in 2000 (Organisation for Economic Co-operation and Development (OECD), 2013). Compared with other OECD countries, Australia had the second highest use of antidepressants in 2011, behind Iceland (Organisation for Economic Co-operation and Development, 2013). Evidence regarding the patterns of use of antidepressants in Australia, and the characteristics of users, is limited. Such evidence is important for informing a range of areas, including the quality use of medications, the cost implications of use and in understanding the likely impact of use on population health.
International studies have shown that health-related factors such as depressive symptoms, physical functioning impairment and number of medications used are strongly related to antidepressant use (Blazer et al., 2005; Ganguli et al., 1997; Grunebaum et al., 2008; Karkare et al., 2011; Pfeiffer et al., 2011). Social determinants—including age, sex, socioeconomic status, ethnicity and region of residence—that may predispose people to use antidepressants or affect a person’s ability to access them (Andersen and Newman, 2005), have also been linked to antidepressant use (Brown et al., 1995; Ganguli et al., 1997; Grunebaum et al., 2008; Pfeiffer et al., 2011). Differences in health care systems between countries mean the profile of antidepressant users, particularly in relation to socioeconomic factors, is likely to differ across populations. Most studies to date have used data from United States (US) populations and, given the differences between the Australian and US health care systems (Schoen et al., 2004), it is important to examine this issue using Australian data. To date, few Australian studies have been undertaken that examine individual-level factors associated with antidepressant use in non-institutional populations (Goldney et al., 2007; Page et al., 2009; Zhang et al., 2010), and most have been limited to using aggregated data. Further, we are not aware of any previous studies, Australian or international, that have examined whether health indicators and behaviors such as body mass index, physical activity, alcohol consumption and cigarette smoking, are associated with antidepressant medication use.
There is limited evidence suggesting that the characteristics of people using antidepressants may also vary by antidepressant class. A US study published in 1998 reported that men, those of African-American race and older people were more likely to use tricyclic antidepressants (TCA) than newer generation selective serotonin reuptake inhibitors (SSRI) (Sclar et al., 1998). However, little is known about what other factors may be associated with the class of antidepressant used or whether sociodemographic variations occur in Australia.
This study contributes to existing knowledge by linking detailed survey data to recorded dispensings of medication use to investigate the relative distributions of antidepressant use in mid-age and older Australians according to sociodemographic, lifestyle and physical and mental health-related factors. Secondarily, it examines whether the factors associated with antidepressant use vary according to the class of antidepressant used.
Methods
Data sources and study population
We undertook analyses using data from the 45 and Up Study baseline questionnaire linked to dispensing information from Pharmaceutical Benefits Scheme (PBS) records.
The 45 and Up Study is an Australian cohort involving 267,153 men and women aged 45 years or over from New South Wales (NSW), Australia. Participants in the study were randomly sampled from the database of Medicare Australia, which provides virtually complete coverage of the general population. Approximately 10% of the NSW population aged 45 years or older was included. Participants joined the study by completing a baseline questionnaire—distributed from January 2006 to December 2008—and giving signed consent for follow-up and linkage of their information to a range of health databases including the PBS database. The study is described in detail elsewhere (Banks et al., 2008) and questionnaires can be viewed at www.45andup.org.au.
The PBS is an administrative dataset containing information about dispensed prescription medications. The PBS allows Australian residents access to a large range of medications at subsidized costs (Department of Health and Ageing, 2013). People contribute a co-payment towards the cost of their medication and the remaining cost is covered under the PBS. Aged pensioners and other social security recipients pay a ‘concessional’ co-payment (this ranged over the study period from AU$3.80 in 2004 to AU$5.30 in 2009), which is lower than the ‘general’ population co-payment (AU$23.70 in 2004, AU$32.90 in 2009). The PBS dataset did not capture below co-payment dispensings to general beneficiaries before 2012, and thus this study was restricted to 45 and Up Study participants who were concessional beneficiaries (those with at least one concessional and no non-concessional claim) during the study period.
Selection of PBS records and participants for inclusion in this study
PBS records from 2004–2011 were available for 45 and Up Study participants. The study period was defined for each participant as the 19 months before completion of the baseline questionnaire. Participants who self-reported holding a Department of Veterans’ Affairs card were excluded, as these people have access to a broader range of subsided medications under a separate Government program.
The Sax Institute linked the baseline 45 and Up questionnaire data and the PBS data. The PBS data were supplied by the Department of Human Services.
Measurements
Outcomes
Dispensing of antidepressant medications were identified from the PBS dataset as those with Anatomical Therapeutic Chemical (ATC) classification codes beginning with N06A (World Health Organization Collaborating Centre for Drug Statistics Methodology, 2013). Consecutive dispensings were defined as at least two dispensings, where the time between the dispensings was less than or equal to the maximum standard supply period (based on the pack size, e.g. if pack size is 30 tablets, the maximum standard supply period is 30 days) plus a refill period of 8 days.
Participants were classified according to whether or not they had received any dispensing for an antidepressant during the study period. Study participants who received a dispensing of an antidepressant were further categorized as: current users; past-only users; and non-persistent users. As PBS data only provide information about dispensing, not actual use of the medications, we defined current and past-only users as those with two or more consecutive dispensings of an antidepressant (Andrade et al., 2006; Eaddy et al., 2005).
Current antidepressant users were further classified by the class of antidepressant dispensed during the study period including: SSRI-only use (ATC codes N06AB02–N06AB10); TCA-only use (ATC codes N06AA01–N06AA23); other antidepressant use (single type) (including monoamine oxidase inhibitors (MAOI) and serotonin-noradrenaline reuptake inhibitors (SNRI)) (ATC codes N06AF01–N06AF06, N06AG02–N06AG03 and N06AX01–N06AX26); and combination use (more than one antidepressant class dispensed).
Exposures
Consistent with the Anderson–Newman model of health care utilization (Andersen and Newman, 1973), a number of predisposing, enabling and need-related factors were examined as exposures. All exposures—except for region of residence, dispensing of antipsychotics and number of medications dispensed—were derived from self-reported baseline questionnaire responses. Region of residence was derived from the postcode obtained from Medicare data, and dispensing of antipsychotics and number of medications dispensed were derived from PBS data.
Predisposing factors were considered to be those that influence a person’s likelihood of using health care and medications (Andersen and Newman, 2005). These included: age; sex; marital status (categorized as married/de facto or not married/de facto); country of birth (categorized as Australia/New Zealand, Europe/North America or other); education (based on highest completed qualification and categorized as no school certificate, school certificate, apprenticeship/trade/certificate/diploma or university degree or higher); body mass index (BMI) (calculated as self-report weight in kilograms divided by height in meters squared and categorized as underweight (15 to <18.5kg/m2); normal weight (18.5 to <25kg/m2); overweight (25 to <30kg/m2); and obese (30–50 kg/m2)); physical activity tertile (based on the weighted number of reported weekly sessions of walking, moderate activity and vigorous activity (Australian Institute of Health and Welfare, 2003) and categorized as low, medium or high); smoking status (never, past, current); and alcohol consumption (drinks per week categorized as none, light (1–10 drinks for men and 1–5 drinks for women), moderate (11–35 drinks for men and 6–20 drinks for women) and heavy (>35 drinks for men and >20 drinks for women) (Power et al., 1998)).
Enabling factors are those that allow an individual to access health care and medications if they need or choose to (Andersen and Newman, 2005), and these included: pre-tax household income (categorized as <$20,000, $20,000–$39,999, $40,000–$69,999 or ⩾$70,000 AUD); private health insurance (yes/no); and region of residence (based on the Accessibility/Remoteness Index of Australia Plus (Australian Institute of Health and Welfare, 2004) score associated with the postcode of residence and categorized as major cities, inner regional or more remote).
Need-related factors included general indicators for health as well as factors measuring depression and other mental illness—these are factors that result in a person needing (or perceiving the need) to access health care and medications (Andersen and Newman, 2005). General indicators for health included: physical impairment (derived from the Medical Outcomes Score-Physical Functioning (MOS-PF), which is equivalent to items from the physical functioning scale of the SF-36 health survey (Stewart and Ware, 1992) and categorized as none/minor (score of 100–75), moderate (50–74), or severe (<50)); self-rated health (categorized as excellent/very good, good or fair/poor); and number of other medications dispensed (based on total number of unique medications other than antidepressants dispensed during the study period, categorized as <5, 5–9, or ⩾10). Proxy measures of depression and mental illness included: psychological distress (based on responses to the Kessler 10 scale (Kessler et al., 2002) and categorized as low (score of <16), moderate (16 to <22), or high/very high (⩾22)); ever doctor-diagnosed depression (yes/no); and current treatment for depression or anxiety (yes/no). The questions asked in the study questionnaire have changed over time, and up until a certain time the question about whether participants had ever been diagnosed with depression by a doctor was not included in the questionnaire; thus responses for this variable were missing for approximately 14% of participants. Antipsychotics are prescribed for managing psychosis which can occur in a number of different mental illnesses, most commonly in schizophrenia and bipolar disorder (Maher and Theodore, 2012), but also major depression (Papakostas et al., 2007). As such, we included antipsychotic use as a need-related exposure in this study. Antipsychotic use was ascertained by any dispensing of an item with ATC code beginning with N05A during the study period and was categorized as low, medium, high and combination doses based on the drug strength dispensed.
Statistical methods
The proportion of participants, by sex and age, dispensed at least one antidepressant during the study period was calculated. The proportion of participants in each antidepressant user category was then calculated in relation to the exposures, and differences between groups were compared using chi squared tests. We then used multinomial logistic regression to model the relationships between the exposure variables and antidepressant use.
Separate multinomial logistic regression models were used to: (i) estimate the strength of the relationship between each exposure and antidepressant user categories (reference: non-users); and (ii) estimate the strength of the relationship between each exposure and the class of antidepressant used for current antidepressant users only (reference: SSRI-only use). All models were adjusted for the non-modifiable factors: sex, age and country of birth.
The primary focus of this study was to compare current users with non-users. While we also examined factors associated with past-only and non-persistent users, the results for these are given in a supplementary table, and the results and discussion of this paper focus on current users.
The strength of association estimates generated from the multinomial logistic regressions are reported as relative risk ratios (RRR), which express the relative risk of having the outcome compared with not having the outcome in relation to different levels of the exposure variables (StataCorp, 2011). For example, a RRR of 1.5 for females currently using antidepressants can be interpreted as: for females compared with males, the relative risk of being a current antidepressant user compared to a non-user is 1.5. In all analyses, 95% confidence intervals were generated. All analyses were performed using Stata version 12.0 and were undertaken using the Secure Unified Research Environment (Sax Institute, 2014). Ethics approval for this project was obtained from the NSW Population and Health Services Research Ethics Committee and the Australian National University Human Research Ethics Committee.
Results
After excluding participants with no concessional-only PBS records during the study period (n=152,555) and those with a Departments of Veterans’ Affairs card (n=5), a total of 111,705 participants remained in the study. Summary characteristics of the study population by antidepressant user category are presented in Table 1 and Figure 1. Of the participants, 19% (21,750) had been dispensed at least one antidepressant medication (total dispensings=260,134) during the study period. Approximately 15% of males and 23% of females were dispensed an antidepressant, with the proportion of users decreasing with age from 30% in those aged 45–54 years to 18% in those aged 85 years or older. The pattern of antidepressant use by age was similar for both men and women (Figure 1). The proportion of people using antidepressants decreased with increasing level of education, income and self-rated health, and increased with increasing level of physical functioning impairment, psychological distress and the number of other medications dispensed during the study period (Table 1).
Sample characteristics by type of antidepressant user.
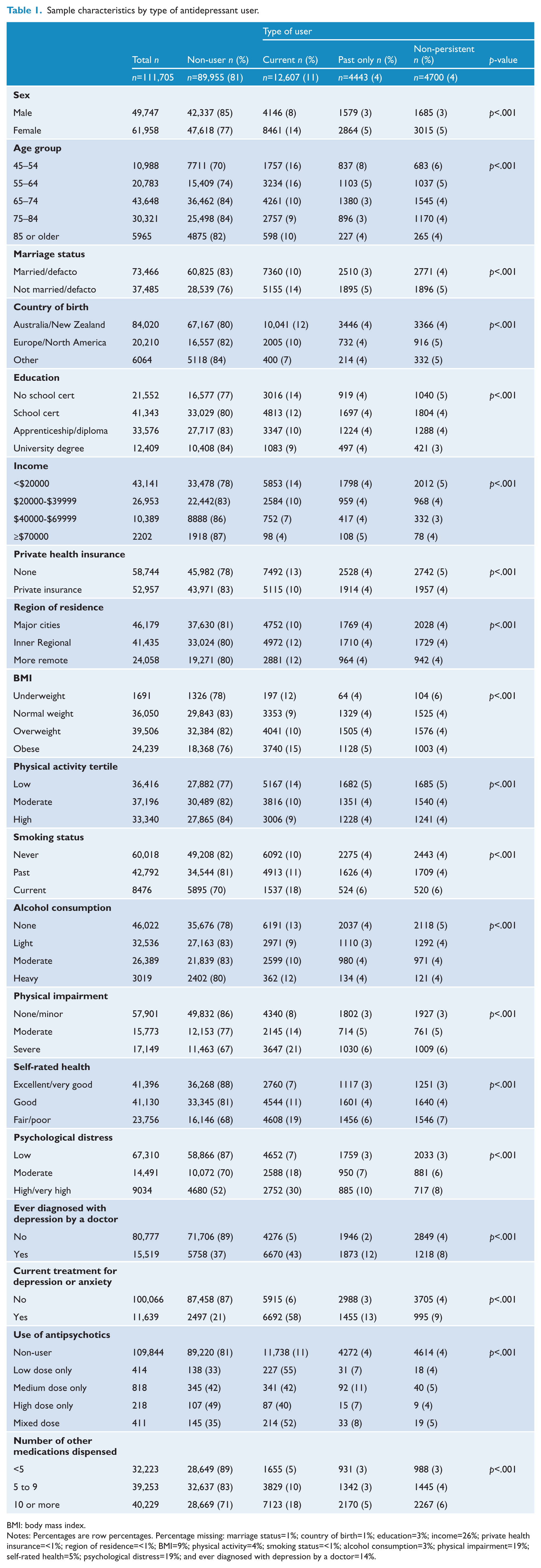
BMI: body mass index.
Notes: Percentages are row percentages. Percentage missing: marriage status=1%; country of birth=1%; education=3%; income=26%; private health insurance=<1%; region of residence=<1%; BMI=9%; physical activity=4%; smoking status=<1%; alcohol consumption=3%; physical impairment=19%; self-rated health=5%; psychological distress=19%; and ever diagnosed with depression by a doctor=14%.
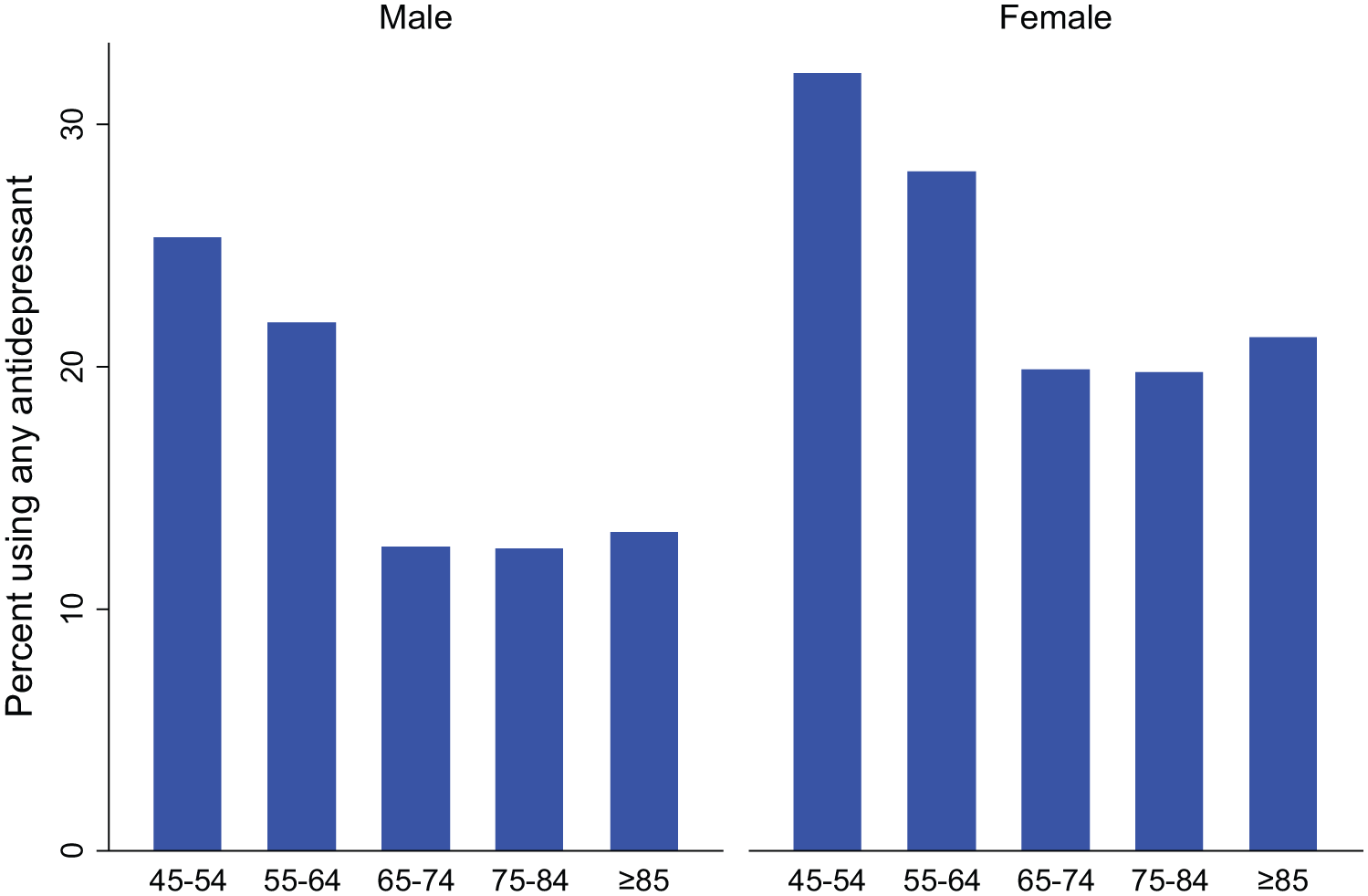
Percentage of study participants using any antidepressant during the study period, according to age group and sex.
Of the participants who reported at baseline that they were currently being treated for depression or anxiety, 58% were current antidepressant users, as were 6% of people who reported not being currently treated for depression or anxiety. Conversely, of those who were current antidepressant users, 53% reported that they were being currently treated for depression or anxiety, while 47% of current users reported not being currently treated for depression or anxiety.
Of those dispensed any antidepressant during the study period, 40% were dispensed an SSRI-only, 32% were dispensed a TCA-only, and 17% used another type of antidepressant (including MAOI and SNRIs). The remaining 11% were dispensed more than one class of antidepressant (combination use) (Table 2). The proportion of people using the different antidepressant classes was similar across current, past-only and non-persistent users, except that the proportion of people dispensed a TCA-only was higher for non-persistent users than current and past-only users.
Numbers and percentage of antidepressant users by antidepressant class among those dispensed any antidepressant.
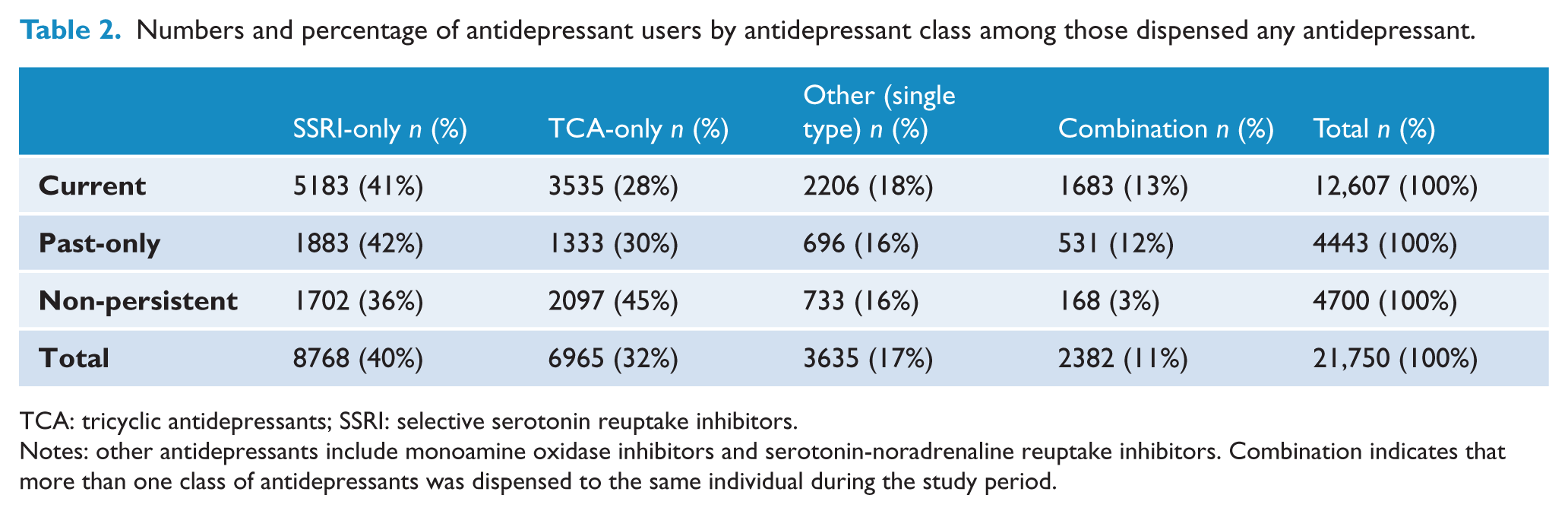
TCA: tricyclic antidepressants; SSRI: selective serotonin reuptake inhibitors.
Notes: other antidepressants include monoamine oxidase inhibitors and serotonin-noradrenaline reuptake inhibitors. Combination indicates that more than one class of antidepressants was dispensed to the same individual during the study period.
Predisposing factors related to current antidepressant use
After adjusting for sex, age and country of birth, all predisposing factors were statistically associated with current antidepressant use (Figure 2 and Supplementary Table 1). Females, younger participants (45–54 years), those born in Australia or New Zealand, those not in a married or de facto relationship and those with lower levels of education were more likely to use antidepressants than their counterparts. Those who were underweight, overweight or obese were more likely to use antidepressants than those with a normal BMI. People who were less physically active (compared with those in the highest physical activity tertile) and those who were past or current smokers (compared with never smokers) were also more likely to use antidepressants. Compared with those consuming a moderate amount of alcohol, those who did not drink alcohol and heavy drinkers were more likely to be current antidepressant users.
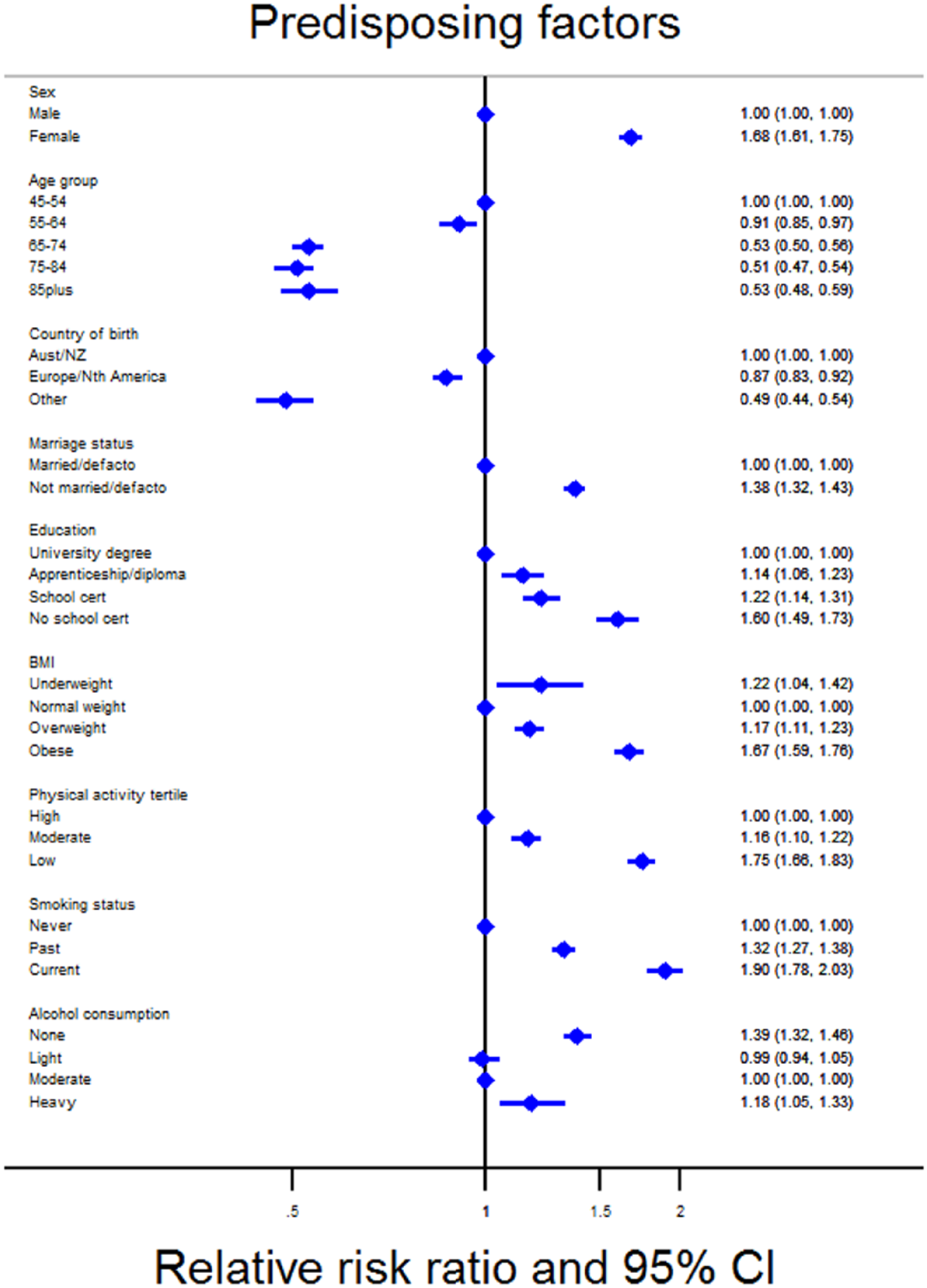
Adjusted relative risk ratio for current antidepressant use compared to no use according to predisposing factors.
Enabling factors related to current antidepressant use
Of the enabling factors, income and private health insurance were associated with current antidepressant use, after adjusting for sex, age and country of birth (Figure 3). Compared with people with an annual household income of $70,000 or more, those with a lower income were more likely to be current antidepressant users [RRR ranging from 1.67 (95% CI:1.34–2.08) for those with an income of $40,000–$69,999 to 3.51 (2.85–4.32) for those with an income of <$20,000]. People with private health insurance, compared with no private health insurance, were less likely to be current antidepressant users [RRR=0.76 (0.73–0.79)].
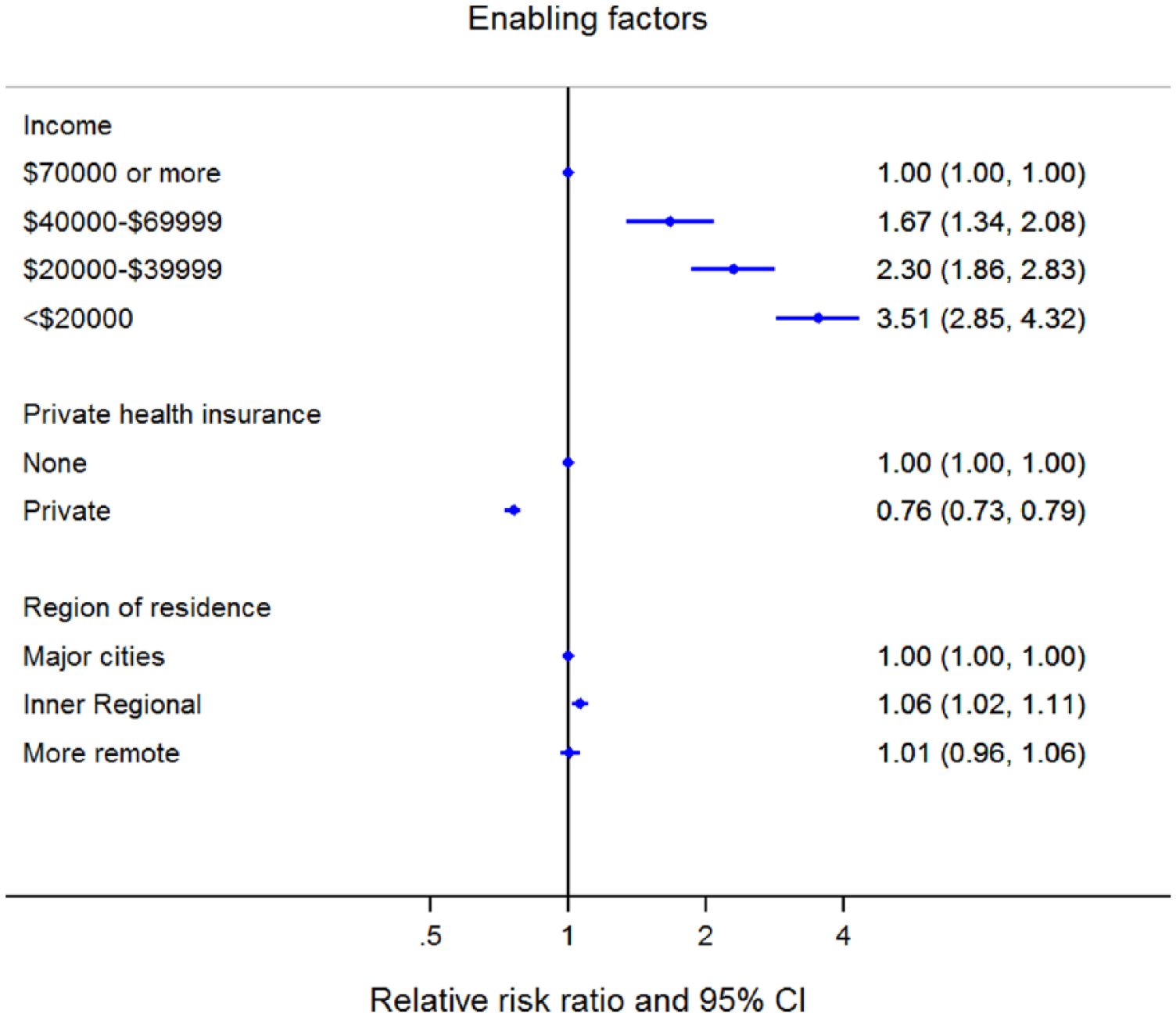
Adjusted relative risk ratio for current antidepressant use compared with no use according to enabling factors.
Need-related factors related to current antidepressant use
All need-related factors were strongly associated with current antidepressant use, after adjustment for sex, age and country of birth (Figure 4). People with physical impairment (compared with no/minor impairment), more dispensed medications (compared with <5) and poorer self-rated health (compared with excellent/very good health) were more likely to be current antidepressant users. Factors measuring mental health showed the strongest statistical association with current antidepressant use. Compared with people with low psychological distress, those with moderate and high/very high psychological distress were 3.16 (3.00–3.34) and 7.22 (6.81–7.66) times as likely to be current antidepressant users than non-users, while those who reported ever being diagnosed with depression by a doctor were 18.85 (17.95–19.79) times as likely to be a current antidepressant users than non-users, compared with those who had not been diagnosed with depression by a doctor. Similarly, those dispensed any antipsychotic during the study period (not necessarily at the same time as antidepressant dispensings) were more likely to be current antidepressant users than those not dispensed any antipsychotics [RRR ranging from 6.05 (4.50–8.13) for those using high-dose antipsychotics to 12.26 (9.85–15.27) for those using low-dose antipsychotics].
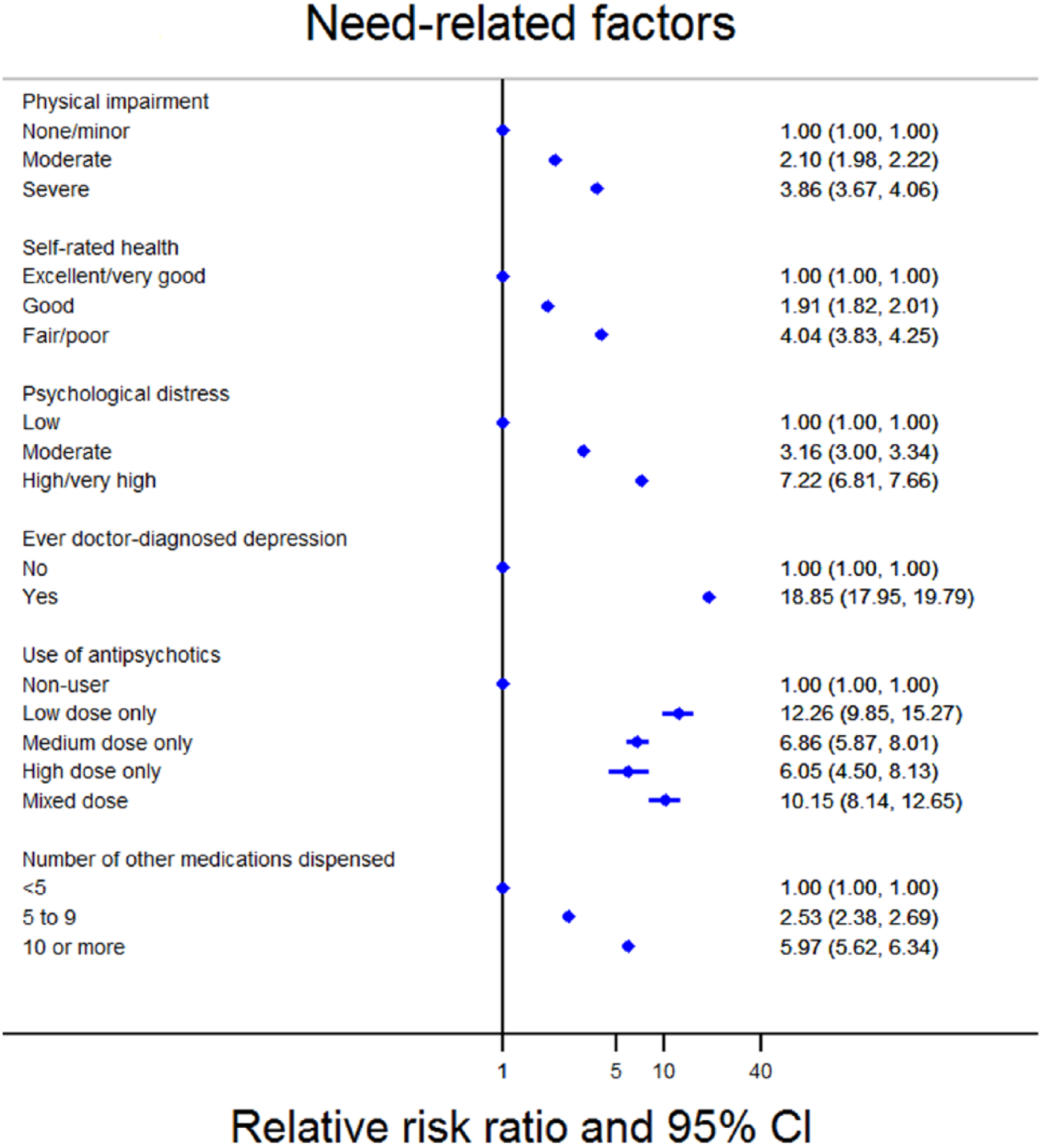
Adjusted relative risk ratio for current antidepressant use compared to no use according to need-related factors.
After adjustment for sex, age and country of birth, the exposures associated with past-only use and non-persistent use were the same as those associated with current antidepressant use (Supplementary Table 1).
Factors associated with use of different antidepressant classes
Table 3 shows the association between different factors and classes of antidepressant dispensed, among people who were current antidepressant users. Of the predisposing factors—after adjustment for sex, age and country of birth—females, older people (compared with those aged 45–54 years) and those with a lower education (compared with a university degree or above) were statistically more likely to use a TCA-only than a SSRI-only. In addition, compared with using a SSRI-only, people born in a country other than Australia or New Zealand, those not married or in a de facto relationship and those with a lower education (compared with a university degree or above) were more likely to use a combination of antidepressant classes, while older people (compared with those aged 45–54 years) were less likely to use a combination of antidepressant classes.
Adjusted relative risk ratio for different types of antidepressants compared to using a SSRI-only in relation to sociodemographic and health exposures, among current users only.
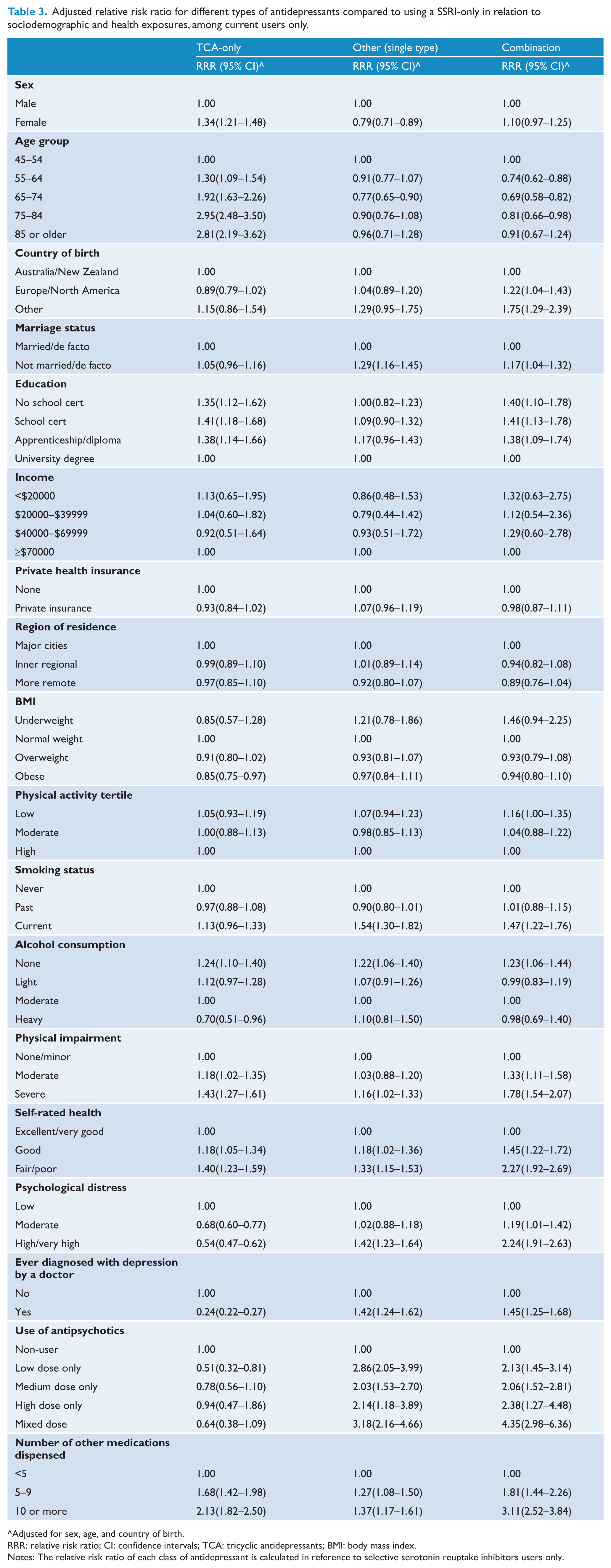
Adjusted for sex, age, and country of birth.
RRR: relative risk ratio; CI: confidence intervals; TCA: tricyclic antidepressants; BMI: body mass index.
Notes: The relative risk ratio of each class of antidepressant is calculated in reference to selective serotonin reuptake inhibitors users only.
Of the need-related factors, those with poorer health (good or fair/poor self-rated health; ⩾5 medications dispensed; and moderate or severe physical impairment) were generally statistically more likely to use a TCA-only, other type of antidepressant (single type) or a combination of antidepressant classes compared with using a SSRI-only. In contrast, people with poor mental health (moderate or high/very high psychological distress; having ever been diagnosed with depression by a doctor; and antipsychotic use) were less likely to use a TCA-only compared with a SSRI-only (although this was not statistically significant for use of antipsychotics), but were also more likely to use a other type of antidepressant (single type) or a combination of antidepressant classes compared with a SSRI-only.
Discussion
Principal findings
Factors related to an individuals’ general physical and mental wellbeing, i.e. need-related health factors and, to a lesser degree, some predisposing and enabling factors, are associated with current antidepressant use in our sample of Australian adults. Our findings show that people with poorer physical and mental health (as indicated by moderate–severe physical impairment; fair–poor self-rated health; moderate–very high psychological distress; ever diagnosis of depression by a doctor; antipsychotic use; and polypharmacy) were most likely to be current antidepressant users, as were females, younger people, those born in Australia/New Zealand, those with low levels of physical activity and those with a lower income. Sex, age, education and physical and mental health factors were also associated with the use different classes of antidepressants (TCA-only, single types of other antidepressants only, or a combination of antidepressants) compared with use of the more common SSRI-only.
Results of the study in relation to other studies
Our results are consistent with those of previous international and Australian studies which have shown that being female and having poorer physical and mental health is strongly associated with antidepressant use (Blazer et al., 2005; Brown et al., 1995; Ganguli et al., 1997; Grunebaum et al., 2008; Harris et al., 2011; Karkare et al., 2011; Pfeiffer et al., 2011; Zhang et al., 2010). Specifically, these studies have provided evidence that those with: poor self-rated health, more doctor visits; polypharmacy; high psychological distress; depressive or anxiety symptoms; cognitive impairment; physical functioning impairment; and one or more chronic conditions, are more likely to use antidepressants than their counterparts. Our studies confirm these findings, and further add to the literature by showing antipsychotic use—which is prescribed for managing psychosis and may be prescribed for those with diagnosed depression—and other health-related indicators and behaviors, including BMI, physical activity, smoking status and alcohol consumption are also associated with current use of antidepressants.
In contrast to other studies, while we found that people with lower levels of education and lower income were more likely to be antidepressant users, previous studies have shown the opposite or no association between these two factors and antidepressant use. A large study conducted in Finland (n=65,405) found that, in men, those with a primary or secondary education compared with a tertiary education were statistically less likely to use antidepressants, while no statistical association was seen for women (Kivimaki et al., 2007). Other studies (from the US) reported no statistical association between education and antidepressant use (Blazer et al., 2000; Grunebaum et al., 2008). Similarly, most previous studies that have investigated the association between income and antidepressant association have found no significant relationship (Blazer et al., 2000; Grunebaum et al., 2008; Soudry et al., 2008), with the results of another study suggesting that people with higher levels of income were more likely to use antidepressants (Brown et al., 1995). A possible reason for discrepancy between our results and those from other countries is that, because the concessional PBS benefits are available to low-income earners, access to medications in this subset of the Australian population may not be as tied to the ability to pay as in other countries. Instead, the association between higher antidepressant use and lower income observed in our study may reflect the increased burden of mental illness within this group of people. This is supported by a previous study using data from the 45 and Up Study, which showed an association between low income and low education and increased odds of high psychological distress (Banks et al., 2010). Furthermore, the observed association between low income and increased likelihood of antidepressant use in our study may reflect the lower cost of antidepressants and their widespread availability compared with psychotherapy. Indeed, we found that over half (58%) the people who reported at baseline that they were currently being treated for depression or anxiety were current antidepressant users. This suggests the other 42% of people may be accessing another form of treatment, such as psychotherapy.
With regard to the relationship between individual-level factors and the type of antidepressant class used, we found that women and older people were more likely than men and younger people to use a TCA-only compared with a SSRI-only. This is in contrast to the findings of a US study which showed that men rather than women were more likely to use a TCA than a SSRI, although they did similarly find that older people were more likely to use a TCA than an SSRI (Sclar et al., 1998). It is not clear why our study results were different to the US study in terms of the relationship between sex and antidepressant class; however, the US study used data from 1990–1994 so differences in time and setting may reflect a difference in patterns of prescribing. A further possible explanation is that SSRIs and TCAs may be prescribed for different indications, so the differences between the studies may reflect differences in the prevalence of conditions being prescribed for. For example, a previous Australian study found that SSRIs were used only for mental illness while TCAs were used for physical conditions (pain, migraine and urinary incontinence) as well as mental illness (Zhang et al., 2010). It is also possible that TCAs are prescribed secondarily to people who did not respond to SSRIs, so the results may reflect a difference in the proportion of people with more severe depression.
Our finding that not all antidepressant users report being currently treated for depression or anxiety supports the findings from a previous Australian study (Hollingworth et al., 2010). This study used Australian data from the 2007 National Survey of Mental Health and Wellbeing and PBS data (2002–07), finding that the prevalence of self-reported affective and anxiety disorders (including depression) were highest in those aged less than 50 years while antidepressant use was highest in those aged 90–94 years old (Hollingworth et al., 2010). Although these findings could be explained by inaccurate self-reporting of mental illness, a further Australian study of men and women living in the community or in residential care examined the reasons for antidepressant use, finding that 70% of use was for psychological reasons and 10% were reported for physical reasons (Zhang et al., 2010). While we were unable to explore the reasons for antidepressant use explicitly using our data, taken together, these results suggest that some people may be using antidepressants for both mental and physical health reasons. However, our finding may have been due to the 6-month ‘window’ that we considered current use, such that individuals may not have been taking the medication at the time of completing the questionnaire. It may also indicate that a proportion of people who are using antidepressants may not consider themselves to have a diagnosis of depression for some other reason.
Strengths and weakness of this study
The main strengths of this study are its large sample size; population-based nature; linkage of detailed questionnaire data to detailed independent administrative information on medication dispensing; and information on a variety of diverse exposures. There are three main limitations of this study. First, information on most exposures (with the exception of region of residence, use of antipsychotics and number of medications dispensed) was self-reported. While this is likely to be accurate for many exposures such as age, sex, education and country of birth, other factors such as weight, height, physical activity and alcohol consumption may be less accurately reported. However, this potential bias is likely to be non-differential as the accuracy of the self-report is unlikely to vary by whether or not a person was using an antidepressant; this would likely bias the results towards the null (no effect). Second, the PBS data do not provide information on actual use (only individual dispensings of medication). To deal with this we defined the main outcome of current antidepressant use as those with two or more consecutive dispensings rather than any dispensing of an antidepressant. Third, this study was restricted to only those within the 45 and Up Study who had concessional PBS dispensings during the study period. This sample is likely to be older, sicker and poorer than the general population and thus is not representative of all those using antidepressants in the Australian population. We found that 19% of our study population had been dispensed at least one antidepressant during the 19-month study period. While not directly comparable, this is higher than the prevalence reported in representative Australian surveys such as the 2004–05 National Health Survey in which 5% of people reported having used an antidepressant for mental wellbeing in the 2-week period before the survey (Australian Bureau of Statistics, 2006). While the absolute results, particularly the proportion of antidepressant users estimated in this study, should be regarded with caution, it has been previously shown that the relative measures of association calculated in non-representative cohort studies can be generalized to the broader population (Mealing et al., 2010).
The aim of this study was not to examine causal exposures of antidepressant use, but to instead examine how the distribution of antidepressant use varies by sociodemographic, lifestyle and health characteristics. Further, the PBS data do not provide information on the indication for which the medication is prescribed and thus, antidepressant use as described in this study should not be used as a proxy of the prevalence of depression.
What does this study mean?
Our results indicate that people with poorer physical and mental health are more likely to use antidepressants than their healthier counterparts. We also found a relationship between sociodemographic and lifestyle factors and antidepressant use; however, the analyses were only adjusted for sex, age and country of birth, and thus at least some of this relationship is likely to reflect underlying differences in health. Indeed, the results observed in this study appear to broadly reflect underlying distributions of mental illness in Australia. Results from the 2007 National Survey of Mental Health and Wellbeing showed that more women (22%) than men (18%) reported having a mental disorder in the 12 months before the survey and the prevalence of mental illness decreased with age (Australian Bureau of Statistics, 2013). Further, the prevalence of mental illness increased with decreasing labor force participation (which is strongly related to morbidity, education and income) and was higher in current smokers (compared with never smokers) and in those with severe disability (compared with no disability) (Australian Bureau of Statistics, 2008). This profile of mental disorder in the Australian population is similar to that observed for antidepressant users in this study.
Our finding that poorer physical health is associated with antidepressant use is also likely to reflect the complex relationship between psychological distress, chronic health conditions and disability. A previous study using data from the 45 and Up Study found that people with limitations to physical functioning such that they needed help for daily tasks were more likely to have high or very high levels of psychological distress compared with those who did not need help with daily tasks (Byles et al., 2014). Further, people with chronic health conditions such as diabetes and heart disease were also more likely to have high or very high levels of psychological distress (Byles et al., 2014).
While we found an association between antidepressant use and dispensings of antipsychotics, particularly low-dose antipsychotics, it is not possible to ascertain from the available data why there may be higher rates of antipsychotic dispensings among those who are antidepressant users.
Further, the patterns of use of different antidepressant classes may reflect the tolerability profile of different antidepressants. While their efficacy is estimated to be similar, SSRIs are considered to have a more tolerable side-effect profile than older-generation TCAs (Anderson, 2000). We found a higher proportion of TCA users were non-persistent users, although we cannot establish whether this was due to tolerability. People with indicators of mental illness (such as high psychological distress) were also more likely to be dispensed a combination of antidepressants during the study period than to be using a SSRI only, although we cannot ascertain from these data whether this was due to switching medication classes or being concurrently prescribed more than one class. Further, it has been previously found that the side-effect profiles of specific antidepressants are considered when a psychiatrist prescribes an antidepressant (Zimmerman et al., 2004); thus associations between classes of antidepressants and sociodemographic and health factors may reflect the differing importance of particular side effects to different groups of people.
Conclusions
In our sample of mid-age concession card holders, we found clear patterns of antidepressant use which varied across sociodemographic, lifestyle and health-related factors. Females, those with lower levels of income or education, and those with poorer health profiles (low levels of physical activity, being overweight or obese, or being a current smoker or heavy alcohol drinker) were more likely to use antidepressants than their counterparts. Our findings suggest, in addition to having poorer mental health, users of antidepressant medications are also sicker and are more likely to have impairments to physical functioning than people who do not use antidepressants.
Footnotes
Acknowledgements
We would like to thank Professor Scott Henderson for providing clinical advice and Dr Timothy Dobbins for providing statistical advice. This research was completed using data collected through the 45 and Up Study (![]() ). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; beyondblue; Ageing, Disability and Home Care, Department of Family and Community Services and the Australian Red Cross Blood Service. We thank the many thousands of people participating in the 45 and Up Study.
). The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; beyondblue; Ageing, Disability and Home Care, Department of Family and Community Services and the Australian Red Cross Blood Service. We thank the many thousands of people participating in the 45 and Up Study.
Funding
Emily Banks and Bryan Rodgers are supported by the NHMRC (Fellowship No. 1042717 and 471429, respectively). This project was supported by the Study of Economic and Environmental Factors in health project, funded by the National Health and Medical Research Council of Australia (NHMRC) (grant reference: 402810) and NHMRC project grant 1024450.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.