
Abstract
Objective:
Longitudinal trends in the dispensing of antidepressant, antipsychotic and ADHD medications from 2009–2012 were examined according to age and gender of patient and prescriber speciality. Of particular interest were changing trends in the prescription of psychotropic medications to children, adolescents and young adults.
Method:
Dispensing data for government-subsidised antidepressant, antipsychotic and ADHD medications were obtained from the database maintained by the Department of Human Services. Results were expressed in terms of number of prescriptions dispensed.
Results:
Over the four- year study period, the dispensing of antidepressants, antipsychotics and ADHD medications showed overall increases of 16.1%, 22.7% and 26.1% respectively. The most rapid percentage increases in antidepressant and antipsychotic dispensing occurred in children aged 10–14 (35.5% and 49.1% respectively), while ADHD medication dispensing rose most rapidly in those aged 20–24 (70.9%). Dispensing to males was more common during childhood for all investigated classes while two-thirds of adult antidepressant prescribing was to female patients. The most commonly prescribed antidepressants varied by age and were as follows: fluoxetine (3–19 year olds), desvenlafaxine (20–24 years) and venlafaxine (>25 years). Risperidone was the most common antipsychotic dispensed to children under 15, quetiapine to adolescents and young adults (15–24 years), and olanzapine to adults. Methylphenidate was the most common ADHD medication in those aged under 25, and dexamphetamine the most common in adults. Most antidepressants and antipsychotics were prescribed by GPs (89.9% and 70.6% respectively), while the majority of ADHD medications were prescribed by paediatricians (59.1%).
Conclusions:
Dispensing of psychotropic medications increased markedly from 2009 to 2012, with notable age-specific trends. General adherence to treatment guidelines is apparent, yet concerns exist regarding rapid increases in serotonin noradrenaline reuptake inhibitor (SNRI) antidepressant prescribing, the likely overmedication of persons with mild psychological distress, and the increasing use of powerful psychotropic medications in younger populations despite uncertain risk–benefit profiles.
Introduction
Psychotropic medications are among the most widely prescribed of all drugs (Britt et al., 2012; IMS Institute for Healthcare Informatics, 2012) and their use continues to increase in many countries of the world. In the last decade Australia has seen a 58.2% increase in psychotropic dispensing overall (Stephenson et al., 2013), with similar increases observed in the US (Medco, 2011) and UK (Ilyas and Moncrieff, 2012). Particularly notable are changes in the dispensing of antidepressants, antipsychotics and ADHD medications: between 2000 and 2011, antidepressant dispensing in Australia increased by 95.3%, antipsychotic dispensing by 85.2% and ADHD medications by 72.9% (Stephenson et al., 2013). In 2011, Australia had the second highest rate of antidepressant use of the 34 Organisation for Economic Co-operation and Development (OECD) nations (OECD, 2013).
This overall escalation has included upward international trends in the prescribing of psychotropic medications to children and adolescents. In the USA, prescription of antipsychotics to children more than doubled between 2001 and 2010 (Medco, 2011), while stimulant prescribing increased by over 3% per year (Zuvekas and Vitiello, 2012). Upward trends in antipsychotic and stimulant prescribing patterns have also been reported in the UK, although to a lesser extent than the USA (Rani et al., 2008). In Australia, antipsychotic dispensing to children aged below 14 was relatively stable between 2002 and 2007, although increases were apparent in those aged 10–14 years (Hollingworth et al., 2013). Antidepressant prescribing to children and adolescents has remained relatively stable in the USA following the 2004 introduction of a black box warning on all antidepressants advising of their association with suicidal ideation and behaviour in those aged under 25 (Medco, 2011). Increased antidepressant prescribing has, however, been observed in the UK (Wijlaars et al., 2012).
The widespread use of psychotropic medications in children and adolescents is a topic of considerable debate. While psychotropics have the potential to help children and adolescents with mental illness, there is often limited evidence supporting their efficacy and safety. Few clinical trials are undertaken in young people, thus much of clinical practice rests on extrapolation from adult data. However, given the well-established differences in physiology, brain development, pharmacokinetics and pharmacodynamics between children, adolescents and adults, such practice is questionable. In addition, little is known about the long-term consequences of exposure to psychotropic drugs on child and adolescent brain development. Preclinical studies suggest exposure to psychotropic drugs during adolescence may lead to atypical changes in brain structure, neurochemistry and growth, thus affecting behavioural and emotional development (Andersen and Navalta, 2011; Karanges and McGregor, 2011).
Approximately 2.5% of US children under the age of 18 are taking antidepressant medication (Medco, 2011), yet studies suggest that many antidepressants have only limited efficacy in childhood depression (Whittington et al., 2004) and confer an increased risk of adverse psychiatric side effects such as self-harm, and suicidal ideation and behaviour (Henry et al., 2012). In addition, the use of antidepressants has been proposed as a risk factor for induction of mania and cycle acceleration in bipolar disorder, particularly in young people (Joseph et al., 2009). Evidence for the efficacy of antidepressants in anxiety disorders in young people appears more robust (Strawn et al., 2012).
Antipsychotics have a lower overall rate of use in children, but are increasingly prescribed for non-psychotic disorders such as anxiety, disruptive behaviour disorders, autism spectrum disorders, ADHD and bipolar disorder (Olfson et al., 2012; Olfson et al., 2014). While providing some benefit in these disorders (Loy et al., 2012; Sharma and Shaw, 2012), atypical antipsychotics may cause significant weight gain and metabolic syndrome, particularly in children and adolescents (Correll, 2008).
Similarly, the ever-increasing diagnosis and pharmacological treatment of ADHD has been widely questioned, particularly with regard to less severe forms of the disorder (Thomas et al., 2013). While stimulants show robust efficacy in the treatment of core symptoms of ADHD (Wigal, 2009), they appear to have limited long-term efficacy and have the potential to cause cardiac adverse effects and growth retardation (Government of Western Australia, 2010; Jensen et al., 2007; Molina et al., 2009).
More generally, concerns have also been raised over the potential over-diagnosis of mental illness and the widespread use of psychotropic medications in mild cases of illness where non-pharmacological approaches may be more appropriate (Maj, 2014; Parker, 2009; Thomas et al., 2013).
To date, few studies have investigated trends in psychotropic use among Australian children and adolescents. Hollingworth et al. (2013) have reported trends in the dispensing of antipsychotic medications to children and young adults between 2002 and 2007, and there have been state-based investigations of stimulant use (e.g. Government of Western Australia, 2012; Preen et al., 2007). The current study provides a more comprehensive national examination of recent longitudinal trends in the dispensing of psychotropic medications (including antidepressants, antipsychotics and ADHD medications) to Australian children, adolescents and adults between 2009 and 2012.
Methods
This study utilised the dispensing database maintained by the Department of Human Services (DoHS) to examine changing trends in government-subsidised antidepressant, antipsychotic and ADHD medication use from January 2009 to December 2012. In Australia, community prescriptions for approved uses of a certain drug are dispensed under one of two government-subsidised schemes: the Pharmaceutical Benefits Scheme (PBS), which supplies the general community, and the Repatriation PBS (RPBS), for returned servicemen and women. The DoHS database provides data on all prescriptions subsidised under these two schemes. It does not include data on private prescriptions funded by the patient or private health insurer, or inpatient prescriptions in public hospitals. It does not include medications that are not listed on the PBS or RPBS schedule (namely agomelatine, trimipramine and thioridazine), or items dispensed for unapproved (off-label) uses. Finally, the DoHS does not include data on prescriptions where the cost is less than the co-payment threshold (where the required patient contribution covers the total cost of the prescribed medication, as occurs with many of the older and cheaper psychotropics).
In 2010, the DoHS database included 75.7% of dispensed antidepressants, 94.3% of antipsychotics, and 74.5% of ADHD medications (Department of Health and Ageing (DoHA), 2010).
Data were sub-divided on the basis of gender and age group (3–9 years, 10–14 years, 15–19 years, 20–24 years and >25 years). Data on class of prescriber (including GPs, psychiatrists, paediatricians and other specialists) were also provided for specified subclasses of drugs.
The quantity of each drug dispensed was expressed in terms of number of scripts (original and repeat). The exact number of prescriptions could not be determined in cases where the number of scripts in an individual cell was between one and five. In such instances the median was taken for the purpose of analysis. We were unable to standardise the data using the standard measure of defined daily dose per 1000 population per day (DDD/1000/day) as data on the form and strength of the drug could not be obtained. Regardless, the validity of the DDD/1000/day among children and adolescents is debatable due to the likely use of different doses in these populations.
The drugs included in the analysis were all drugs with an anatomical therapeutic chemical code in the following groups: antidepressants, antipsychotics and ADHD medications. Benzodiazepines were of lesser interest as their use has remained relatively stable over time, while mood stabilisers are often anticonvulsant drugs and current record keeping makes their use in epilepsy versus psychiatric illness difficult to discern (Stephenson et al., 2013).
Antidepressants included (by class): selective serotonin reuptake inhibitors (SSRIs) (citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline); serotonin noradrenaline reuptake inhibitors (SNRIs) (desvenlafaxine, duloxetine, venlafaxine); noradrenergic and specific serotonergic antidepressants (NaSSAs) (mianserin, mirtazapine); noradrenaline reuptake inhibitors (NRIs) (reboxetine); tricyclic antidepressants (TCAs) (amitriptyline, clomipramine, dothiepin, doxepin, imipramine, nortriptyline); and monoamine oxidase inhibitors (MAOIs)/reversible inhibitors of monoamine oxidase A (RIMAs) (moclobemide, phenelzine, tranylcypromine).
Antipsychotics included: atypical (amisulpride, aripiprazole, asenapine, clozapine, olanzapine, paliperidone, quetiapine, risperidone and ziprasidone); and typical antipsychotics (chlorpromazine, flupenthixol, fluphenazine, haloperidol, pericyazine, trifluoperazine, zuclopenthixol).
ADHD medications included the non-stimulant drug atomoxetine and the stimulants, dexamphetamine and methylphenidate (including immediate- and extended-release formulations).
All calculations were completed using Microsoft Excel 2011 and graphs were generated using GraphPad Prism 5.0c.
Results
Overview: all psychotropics
Overall trends in the dispensing of psychotropic drugs, by class and subclass, are shown in Figure 1. There was a 17.5% increase in dispensing of subsidised psychotropics (antidepressants, antipsychotics and ADHD medications) from 2009 to 2012 (from 15,526,594 to 18,247,828 prescriptions). The largest percentage increases occurred in those aged 15–19 years (33.3% increase), followed by 3–9 years (27.7%), 10–14 years (22.5%), 20–24 years (21.6%) and 25+ years (16.8%).
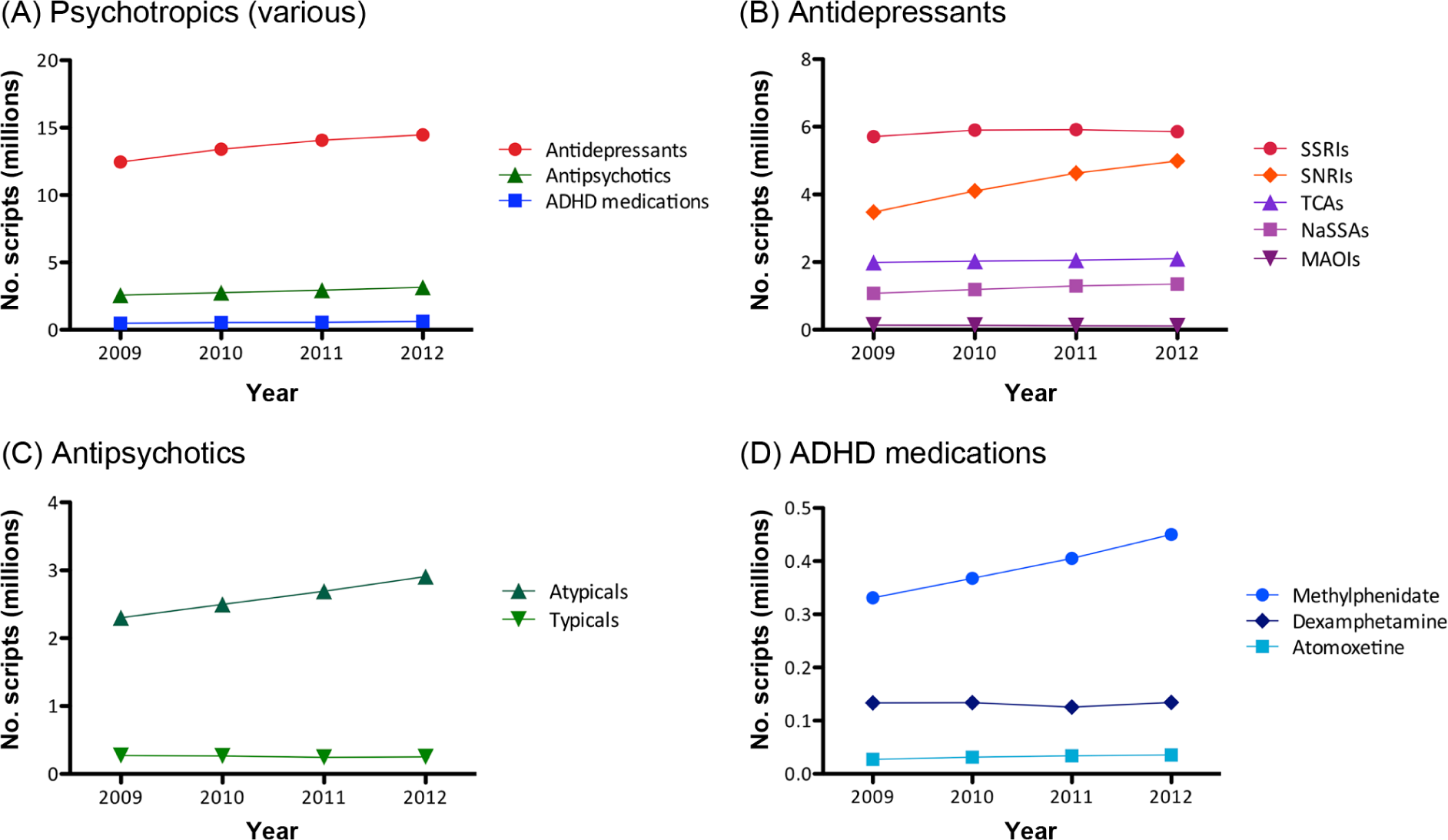
Dispensing of subsidised prescriptions, yearly, from 2009 to 2012, for (A) the three investigated classes of psychotropic medication, (B) the five main classes of antidepressant drugs, (C) typical and atypical antipsychotics, and (D) the three main ADHD medications.
In 2012, 91.5% of investigated psychotropics were dispensed to those aged over 25 years, with 5.5% to those aged 15–24 and 3.0% to those aged 3–14; these three age groups comprised 67.5%, 13.6% and 18.9% of the Australian population respectively (Australian Bureau of Statistics, 2013). The majority of psychotropics dispensed to adults (25+ years) and adolescents (15–24 years) were antidepressants, with ADHD medications the most commonly dispensed psychotropic class in children aged 3–14 years (see Figure 2).
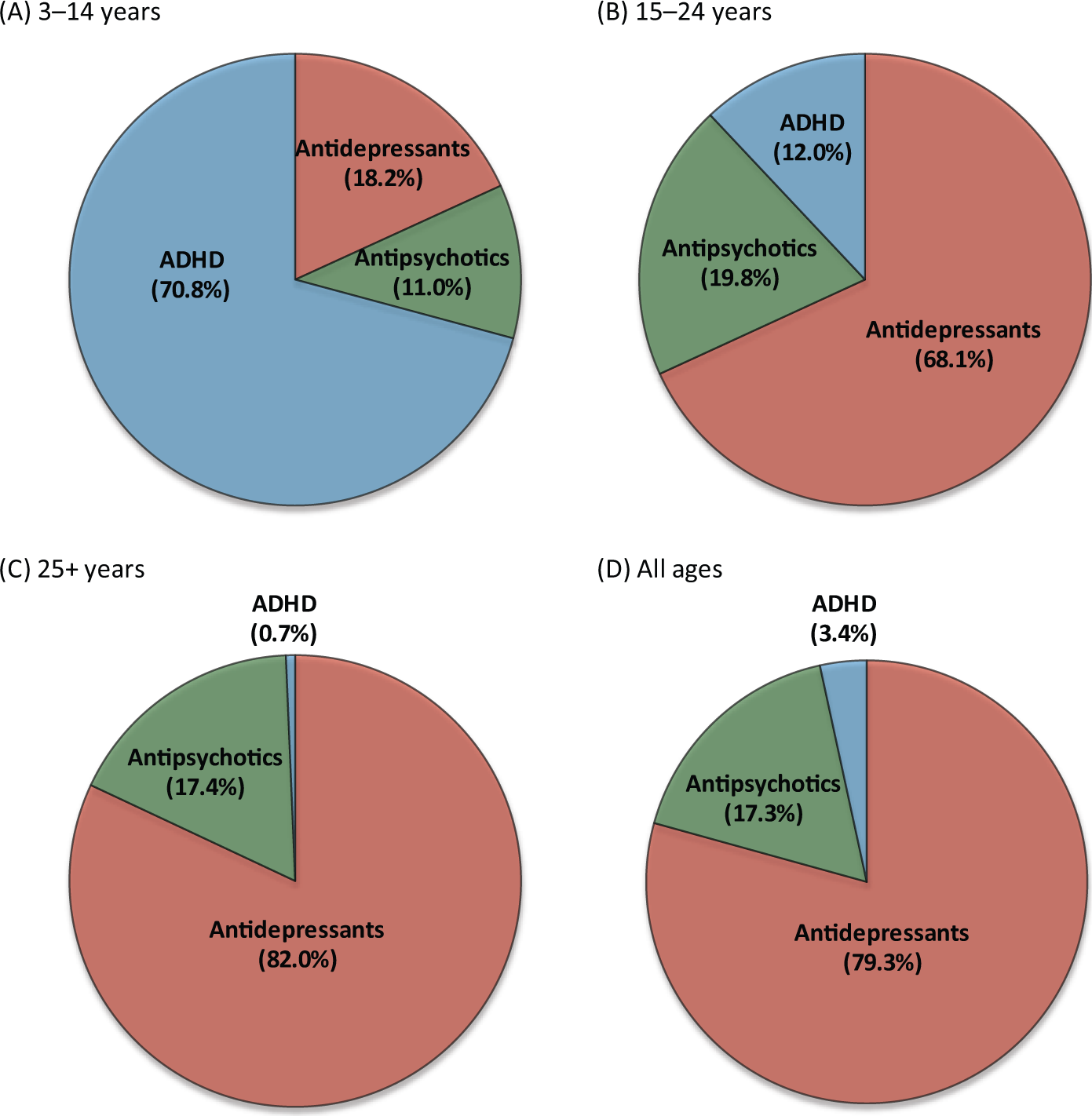
Pie charts showing the percentage share of the market (in terms of number of scripts) for each of the three psychotropic classes for ages (A) 3–14 years, (B) 15–24 years, (C) 25+ years, and (D) all ages.
The most dispensed psychotropic drugs in each age group are shown in Figure 3. In 2012, methylphenidate was the most dispensed psychotropic drug in those aged 3–14 years (61.6% of total psychotropics) and its use in this age group increased 25.3% from 2009–2012. In those aged 15–24, desvenlafaxine was the most common psychotropic (12.5% of total psychotropics), with an increase of 298.1% over the study period. Venlafaxine was the leading psychotropic drug in those aged over 25 (14.1% of total psychotropics); nonetheless, its use in this age group declined 9.5% from 2009 to 2012.
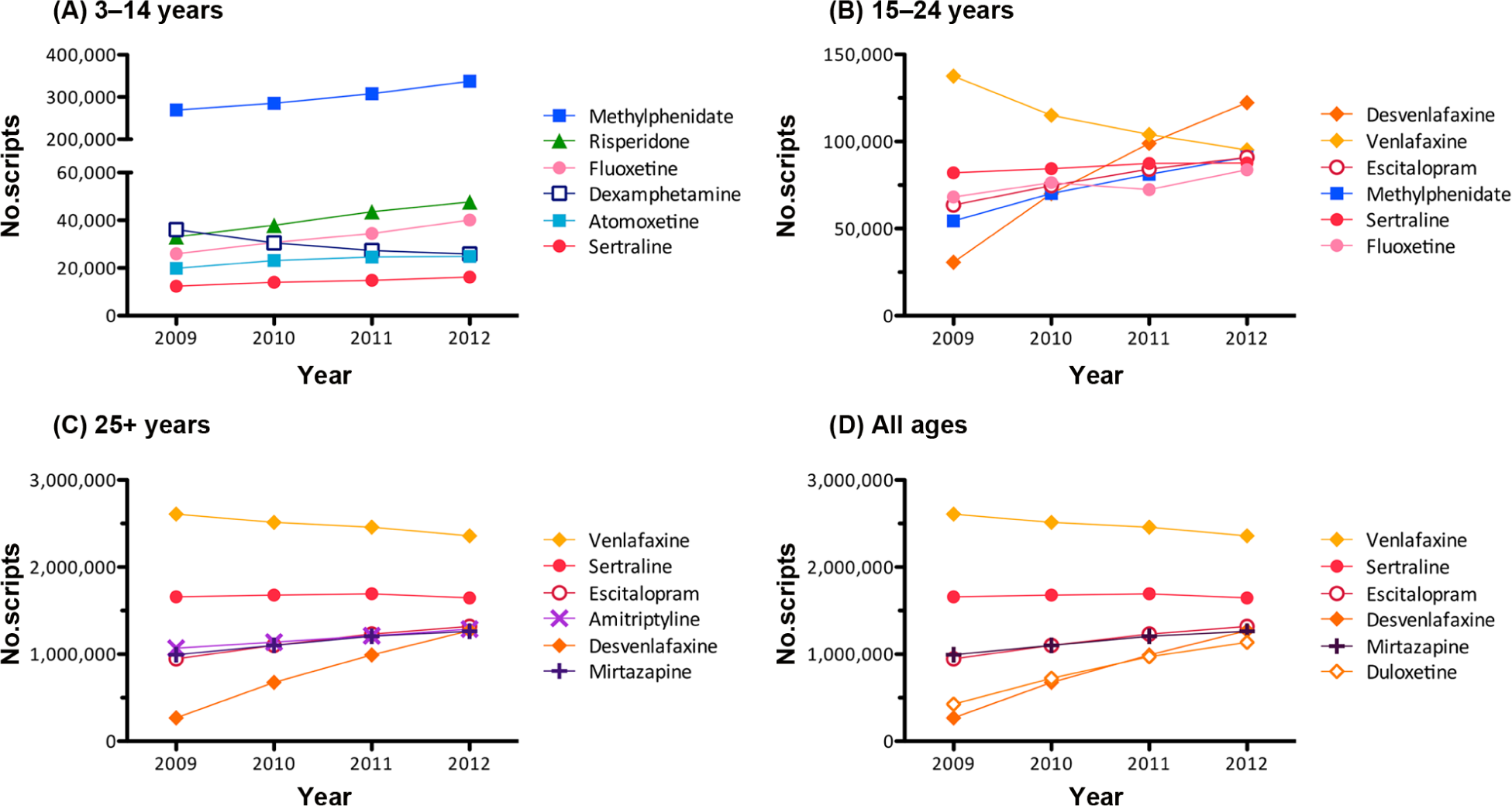
Most dispensed drugs: dispensing trends, from 2009 to 2012, for the six most prescribed drugs in each age group (2012 rankings): (A) 3–14 years, (B) 15–24 years), (C) 25+ years, (D) all ages. Note: Classes of drugs are depicted by colour and symbol as follows: Antidepressants (SSRIs: pink circles; SNRIs: orange diamonds; other antidepressants: purple crosses), antipsychotics (green triangles), and ADHD medications (blue squares).
The most rapid changes in dispensing patterns over the study period, by age, are shown in Figure 4. The fastest growing drug in the 3–14 year age group was duloxetine (210.7% increase), while desvenlafaxine was the fastest growing drug in those aged 15–24 years and 25+ (298.1% increase and 374.0% increase respectively).
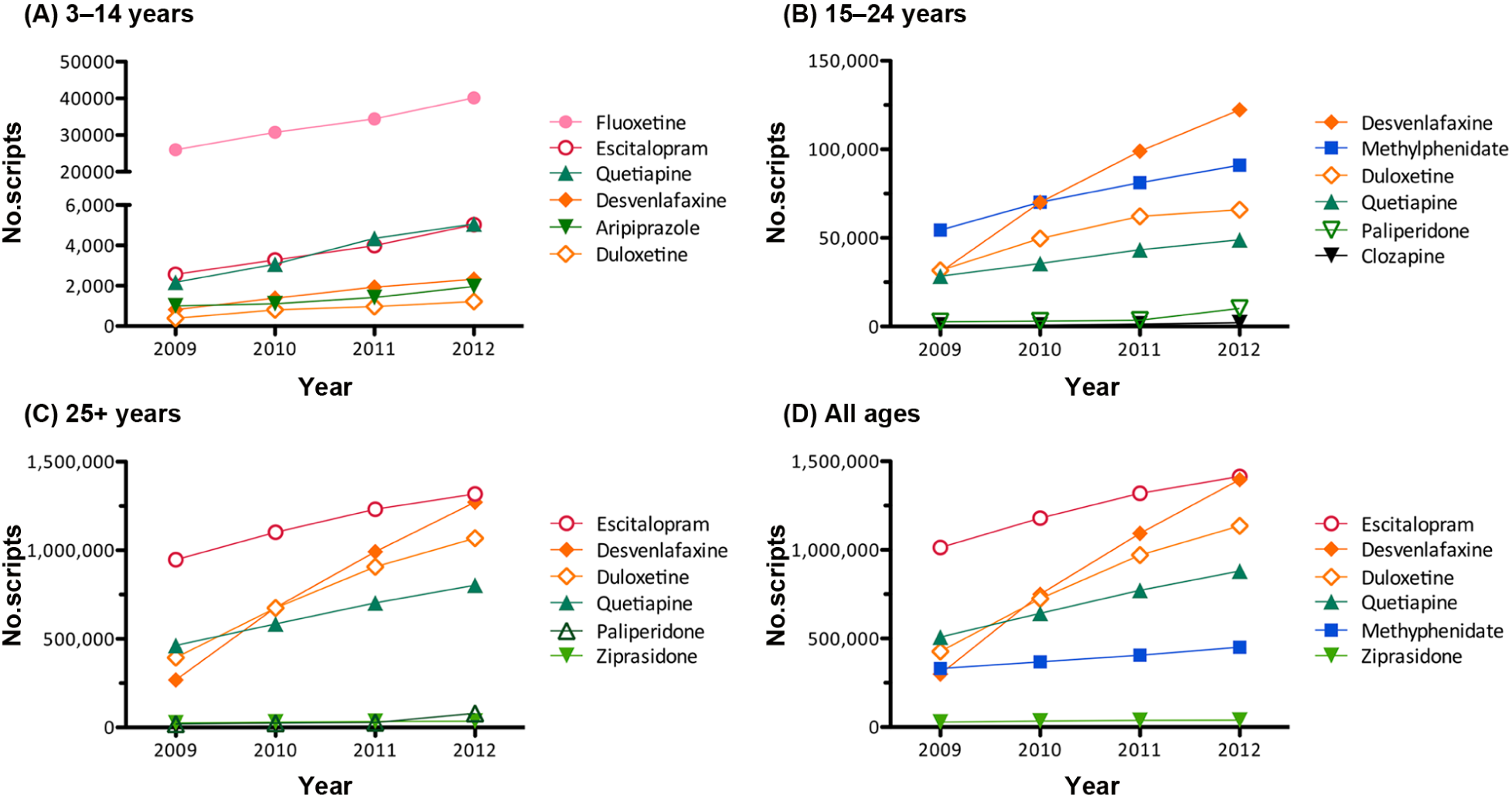
Most rapidly changing drugs: dispensing trends, from 2009 to 2012, for the six most rapidly changing drugs in each age group: (A) 3–14 years, (B) 15–24 years), (C) 25+ years, (D) all ages. Note: Drugs representing less than 0.2% of yearly age total are omitted. Classes of drugs are depicted by colour and symbol as follows: Antidepressants (SSRIs: pink circles; SNRIs: orange diamonds; other antidepressants: purple crosses), antipsychotics (green triangles), and ADHD medications (blue squares).
Antidepressants
Percentage changes in psychotropic dispensing, by age, from 2009 to 2012 are shown in Table 1, while Tables 2, 4 and 5 present key characteristics (drug subcategory, sex of patient and prescriber speciality) for antidepressant, antipsychotic and ADHD prescriptions respectively according to age of patient. Table 3 shows the leading drugs from each class by age, as a percentage of total prescriptions dispensed.
Percentage change from 2009 to 2012 for the major psychotropic classes and age divisions.
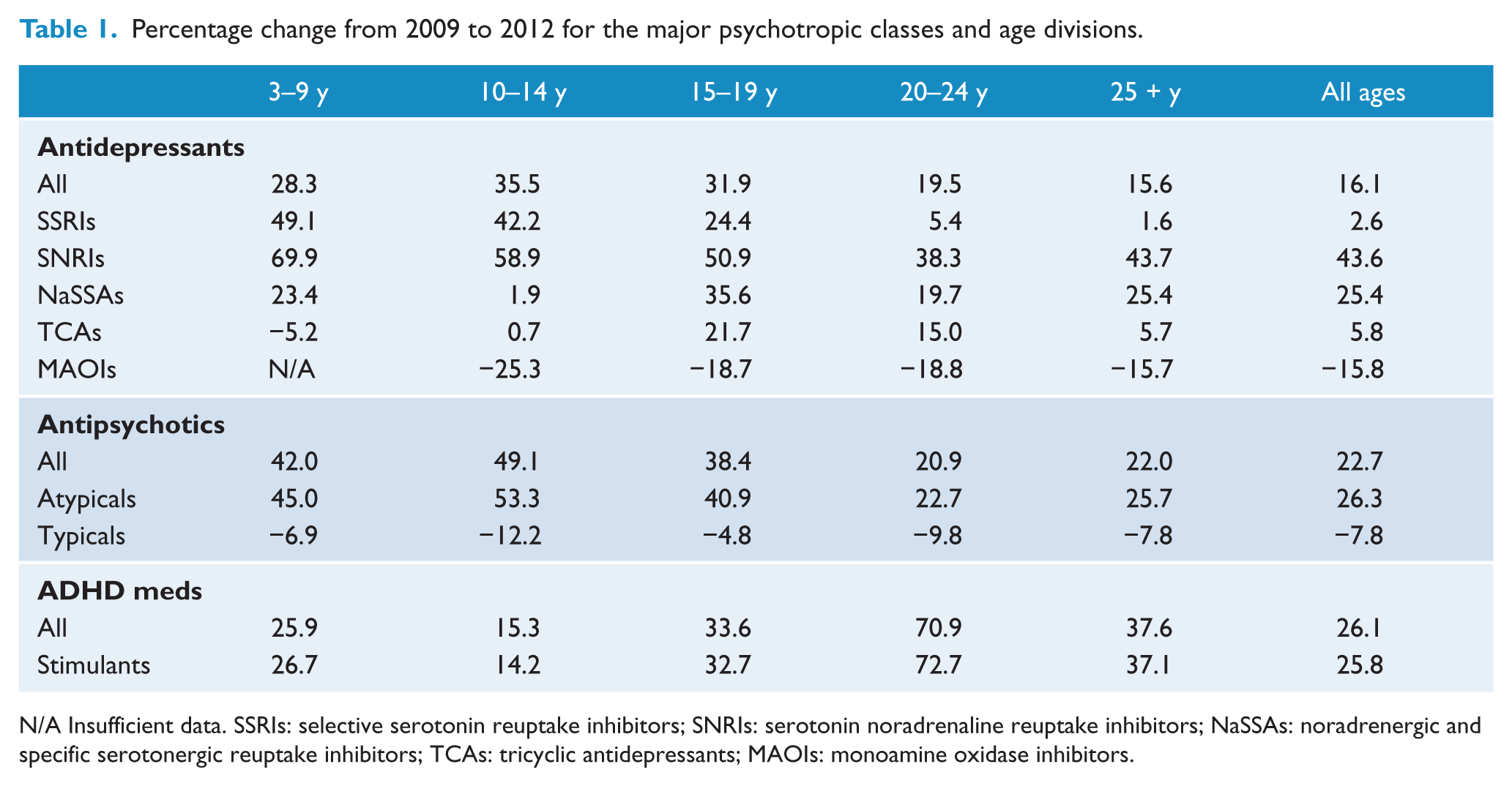
N/A Insufficient data. SSRIs: selective serotonin reuptake inhibitors; SNRIs: serotonin noradrenaline reuptake inhibitors; NaSSAs: noradrenergic and specific serotonergic reuptake inhibitors; TCAs: tricyclic antidepressants; MAOIs: monoamine oxidase inhibitors.
Characteristics of antidepressant prescriptions in 2012 as a percentage of age totals.
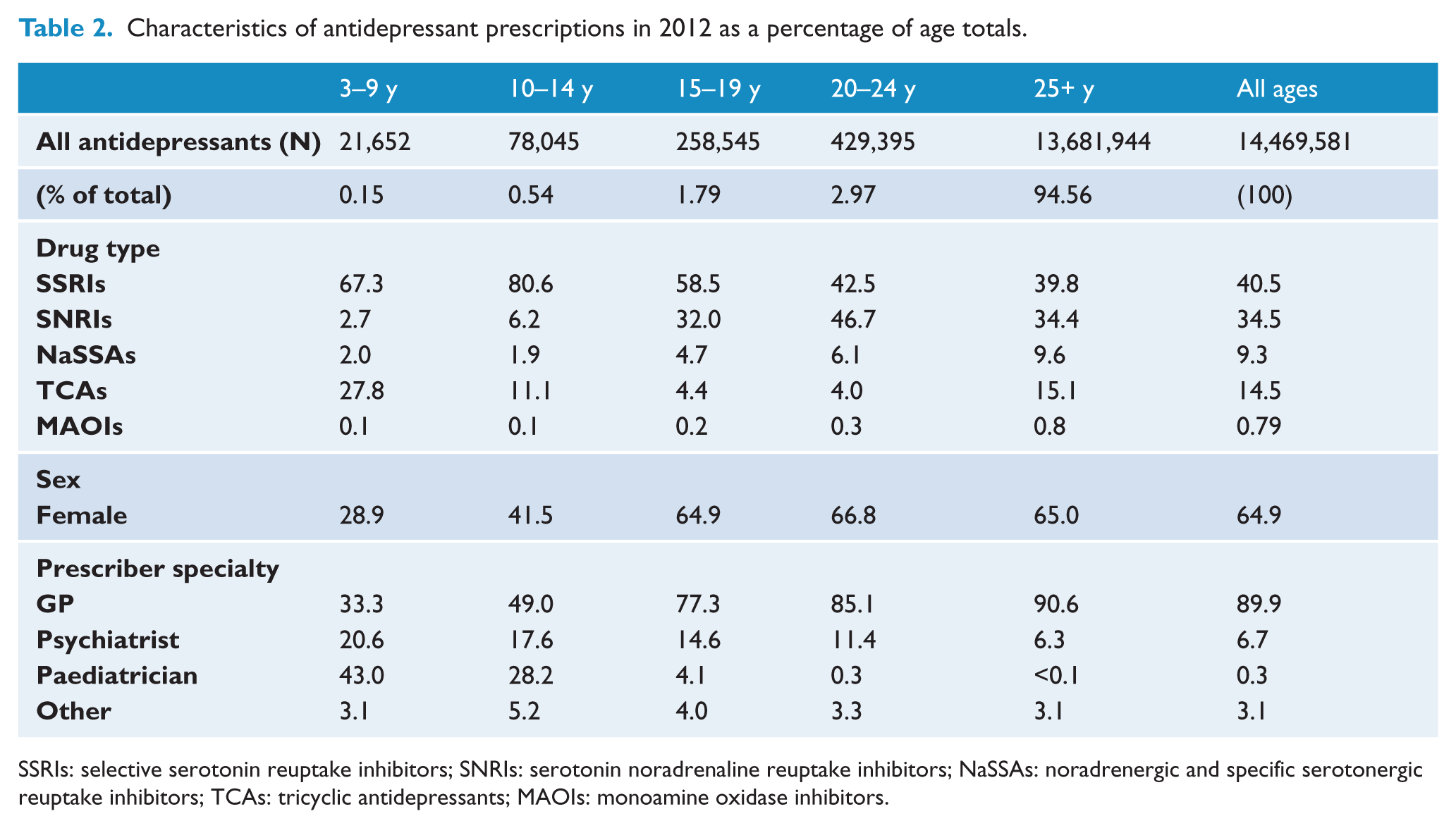
SSRIs: selective serotonin reuptake inhibitors; SNRIs: serotonin noradrenaline reuptake inhibitors; NaSSAs: noradrenergic and specific serotonergic reuptake inhibitors; TCAs: tricyclic antidepressants; MAOIs: monoamine oxidase inhibitors.
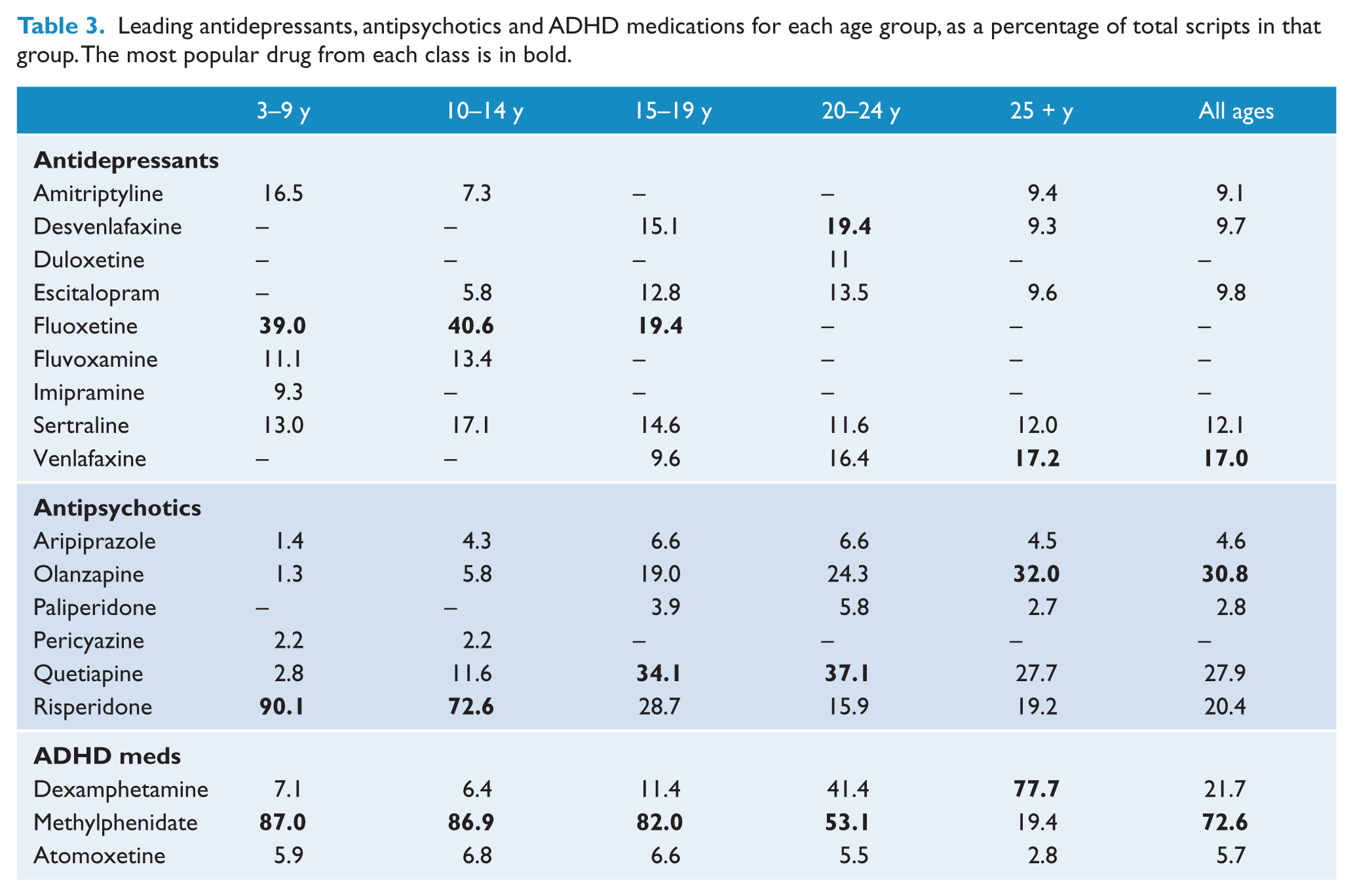
Leading antidepressants, antipsychotics and ADHD medications for each age group, as a percentage of total scripts in that group. The most popular drug from each class is in bold.
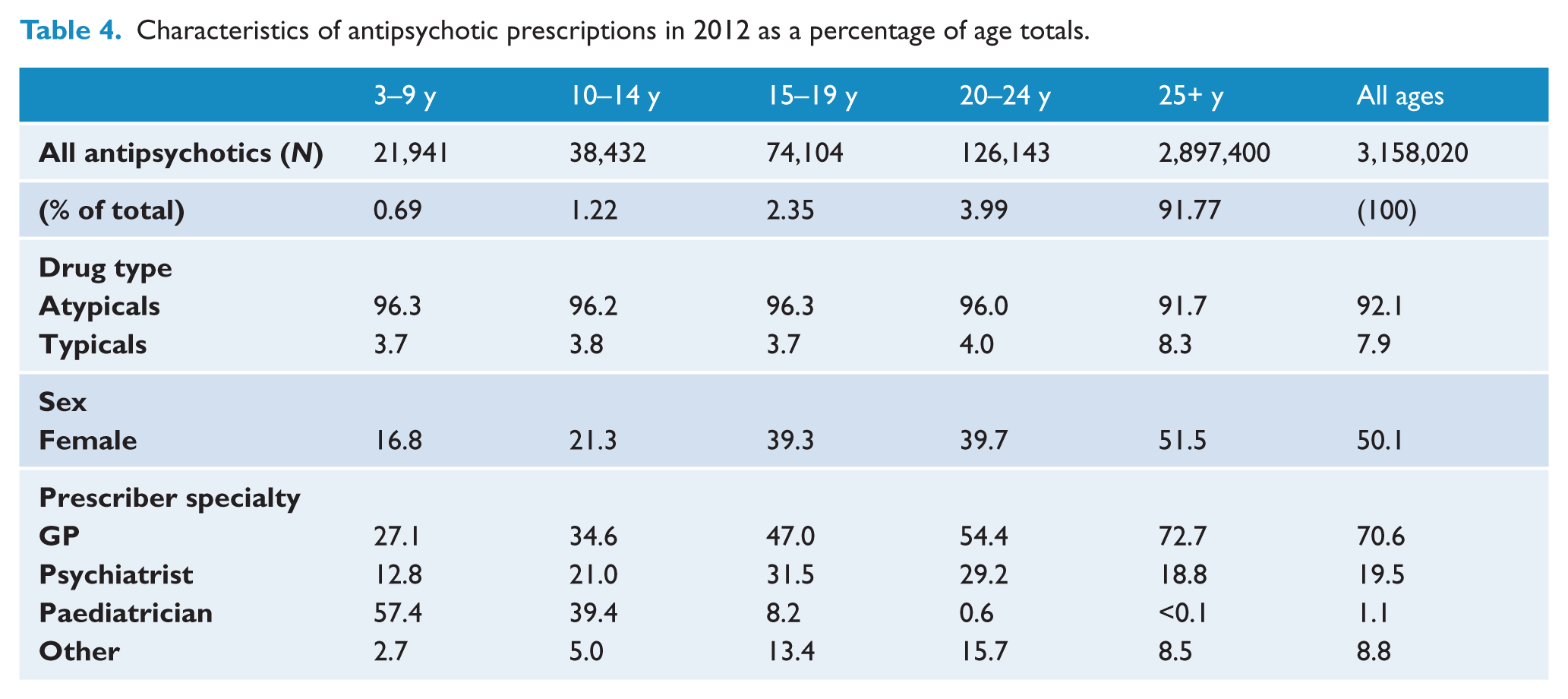
Characteristics of antipsychotic prescriptions in 2012 as a percentage of age totals.
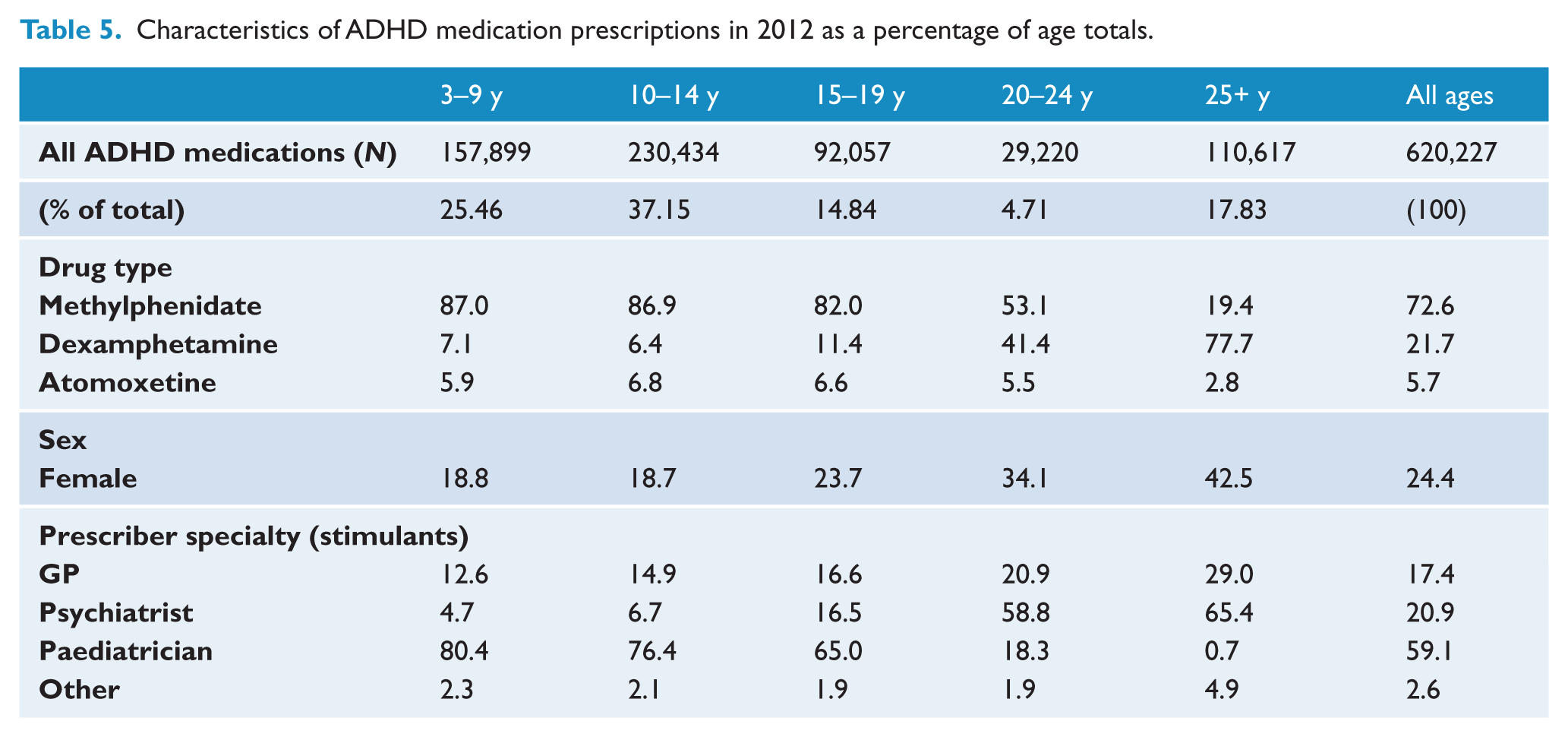
Characteristics of ADHD medication prescriptions in 2012 as a percentage of age totals.
Overall trends (all ages)
There was a 16.1% increase in the number of subsidised antidepressant prescriptions dispensed from 2009 to 2012 (from 12,460,993 to 14,469,581 prescriptions), corresponding to a 3.8% increase per year (see Figure 1A). By class, the SNRIs showed the greatest change, with a 43.6% increase (3,474,426 to 4,988,759 scripts), followed by the NaSSAs (25.4%; 1,077,007 to 1,350,079). There were only small increases in dispensing of TCAs (5.8%; 1,990,593 to 2,105,278) and SSRIs (2.6%; 5,711,934 to 5,858,150). Both MAOIs (−15.8%; 134,280 to 113,128) and NRIs (reboxetine; −25.5%; 72,753 to 54,187) declined in use (see Figure 1B).
In 2009, the majority of antidepressants dispensed were SSRIs (45.8%), followed by SNRIs (27.9%), TCAs (16.0%) and NaSSAs (8.6%). By 2012, the proportion of SNRIs had increased to 34.5%, while the proportion of SSRIs decreased to 40.5%. There was little change in the proportion of TCAs (14.5%) and NaSSAs (9.3%). In 2012, the most dispensed antidepressants were venlafaxine (17.0% of antidepressant prescriptions), sertraline (12.1%), escitalopram (9.8%), desvenlafaxine (9.7%) and amitriptyline (9.1%).
Age and sex
In 2012, 94.56% of investigated antidepressants were dispensed to those aged over 25 years, with 4.76% to those aged 15–24 and only 0.69% to those aged 3–14 (see Table 2).
There was an increase in antidepressant dispensing in all age groups from 2009 to 2012 (Table 1). Greater percentage increases were seen in children and adolescents (aged 3–24 years) than in those aged over 25 (25.0% and 13.5% respectively). The largest percentage increases were seen in the 10–14 year (35.5%), 15–19 year (31.9%), and 3–9 year age groups (28.3%).
SNRIs showed the most pronounced increases over time and these were seen across the entire age spectrum (43.6% increase on average). These increases were particularly apparent in those aged 3–9 (69.9% increase) and 10–14 (58.9%). Despite negligible change in SSRI use in the adult population between 2009 and 2012 (1.6% increase), upward trends were observed in those under 25. As with SNRIs, these trends were most pronounced in the younger age groups (3–9 years: 49.1% increase; 10–14 years: 42.2%; see Table 1).
In 2012, SSRIs were the leading class of antidepressant used in those aged under 20. Fluoxetine was the leading antidepressant in those aged 3–9 years (39.0% of antidepressant scripts dispensed; see Table 3), 10–14 years (40.6%) and 15–19 years (19.4%). SNRIs were more prescribed in older age groups (Table 2) and the most popular class in those aged 20–24 years (26.7% of antidepressants).
Desvenlafaxine was the most popular antidepressant in those aged 20–24 years (19.4%), and venlafaxine for those aged over 25 (17.2%). Tricyclic antidepressants were also prominently used in younger age groups: In children aged 3–9 years, 27.8% of prescribed antidepressants were tricyclics (Table 2).
Most children under 14 receiving antidepressants were male (3–9 years: 71.1%; 10–14 years: 58.5%), while females dominated in the older age groups (~65%; see Table 2). There were no marked differences in sex ratios between antidepressant classes, and in most instances growth in antidepressant use was similar across sexes within each age group. However, particularly marked increases were apparent in SSRIs dispensed to girls aged 3–9 years (61.2% vs. 45.0% in males) and SNRIs dispensed to 3–9 year olds of both sexes (male: 74.0%; female: 60.9%) and females aged 10–14 (70.4% vs. 42.6% in males).
Prescriber specialty
In 2012, most antidepressants were prescribed by GPs (89.9%), with psychiatrists providing only 6.7% of scripts dispensed (see Table 2). These figures were similar for all classes of antidepressant, with MAOIs slightly less likely to be prescribed by GPs (80.5%) and more likely to be prescribed by psychiatrists (17.5%) than the other classes. From 2009 to 2012 there was a 20.5% increase in dispensing of antidepressants prescribed by GPs, and a 4.2% increase in dispensing of antidepressants prescribed by psychiatrists.
Antipsychotics
Overall trends (all ages)
There was a 22.7% increase in the number of subsidised antipsychotic prescriptions dispensed from 2009 to 2012 (from 2,573,833 scripts to 3,158,020 scripts), corresponding to a 5.2% increase per year (see Figure 1A). This increase was driven by a 26.3% increase in dispensing of atypical antipsychotics (from 2,301,669 to 2,907,136 scripts) compared to a 7.8% decrease in typical antipsychotics across this period (272,164 to 250,884 scripts; Figure 1C).
Atypical antipsychotics comprised 89.4% of antipsychotic prescriptions in 2009, increasing to 92.0% in 2012. In 2012, the most dispensed atypical antipsychotics were olanzapine (34.8% of atypical antipsychotics dispensed), quetiapine (30.2%) and risperidone (21.0%), together comprising 78.9% of all antipsychotics dispensed. The leading typical antipsychotics were haloperidol (30.6% of typical antipsychotics dispensed), chlorpromazine (24.4%) and pericyazine (15.6%). However, these three drugs represented only 5.9% of antipsychotic prescriptions in 2012.
Age and sex
In 2012, the vast majority of antipsychotics were dispensed to those aged over 25 years (91.77%), with 6.34% dispensed to those aged 15–24 and 1.91% to those aged 3–14 (Table 4).
There was an increase in antipsychotic dispensing from 2009 to 2012 in all age groups, despite decreases in the use of typical antipsychotics (see Table 1). More pronounced increases were seen in those aged under 25 than those over 25 (30.9% increase compared to 22.0% increase).
With atypical antipsychotics, the greatest change was seen in the 10–14 year age group (53.3% increase), followed by 3–9 years (45.0%) and 15–19 years (40.9%). There were smaller percentage increases in the 20–24 year (22.7%) and 25+ (25.7%) age groups.
In contrast, there were modest decreases in dispensing of typical antipsychotics in all age groups. The largest decrease (12.2%) was in the 10–14 year age group, followed by the 20–24 year age group (9.8%).
In 2012, atypicals were by far the most popular class of antipsychotics used in all age groups (see Table 4) and comprised approximately 96% of dispensed subsidised antipsychotics in those under 25, with slightly more typical antipsychotics used in the adult population (91.7% atypical).
In 2012, risperidone was the most popular antipsychotic in those aged 3–9 years and 10–14 years (90.1% and 72.6% of antipsychotic scripts dispensed, respectively). Quetiapine was the most prescribed antipsychotic in those aged 15–19 years (34.1%; closely followed by risperidone, 28.7%) and 20–24 years (37.1%). In those aged over 25, olanzapine was the most dispensed antipsychotic (32.0%), closely followed by quetiapine (27.7%).
Of the typical antipsychotics, pericyazine was the most dispensed in all age groups under 25 (33.5% of typicals dispensed in under 25s), with its use declining with age (3–9 years: 58.5% of typicals dispensed; 20–24 years: 22.5%). In contrast, haloperidol was the leading typical used in those aged over 25 (15.6% of typical antipsychotics dispensed).
In 2012, males were most likely to be prescribed antipsychotics in all age groups except over 25s, with the proportion of male to female lessening with age (Table 6). This trend was similar for both atypical and typical antipsychotics. A high male to female ratio among those aged under 25 was particularly notable for risperidone, paliperidone, and to a lesser extent olanzapine. In contrast, quetiapine was dispensed at similar levels in both males and females aged 10 years and over.
2012 sex distribution (percentage female) for notable antipsychotic and ADHD medications.
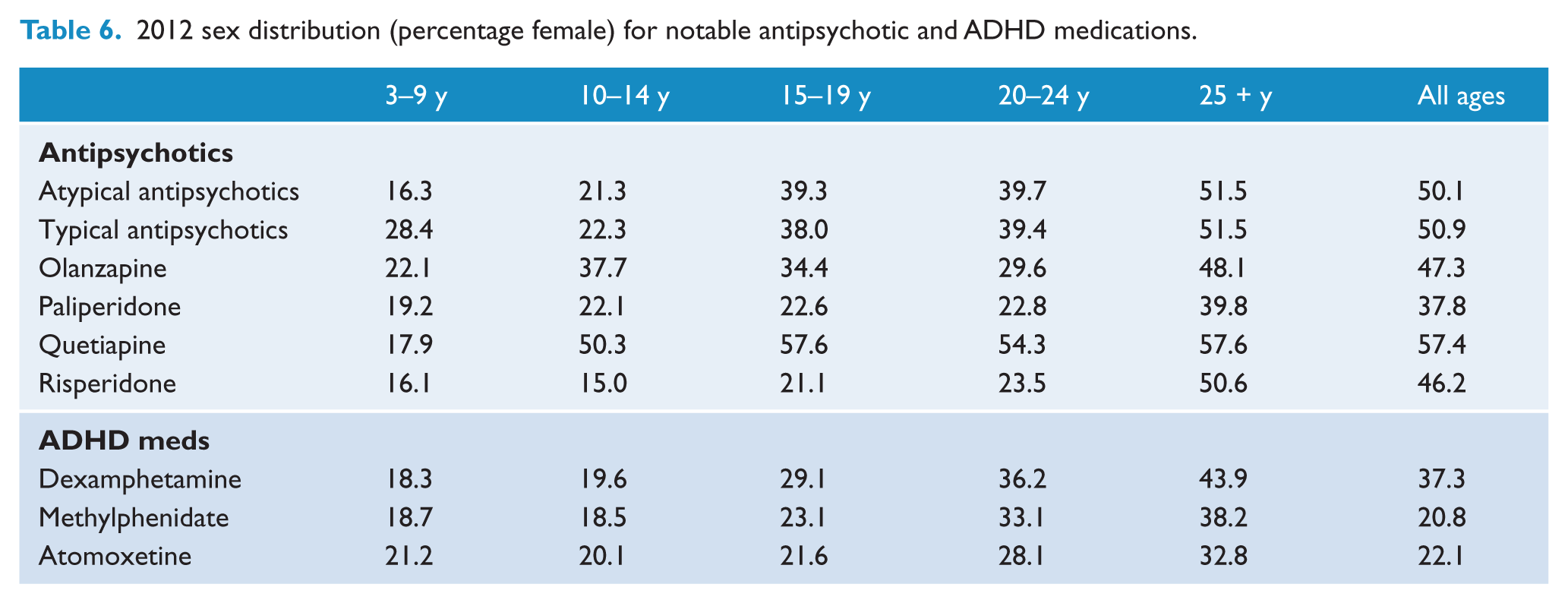
In those aged over 25, there were roughly equal numbers of each sex on antipsychotic medication (see Table 6). From 2009 to 2012, the biggest percentage increase in antipsychotic use occurred in females aged 3–9 years (176.5%), while the increase in males of this age was much lower (36.4%). In terms of individual antipsychotics, the most marked increases occurred in quetiapine use, particularly among those aged less than 14 (3–9 years: male 180.2% increase; female 117.6% increase; 10–14 years: male 97.5%; female 171.5%).
Prescriber specialty
In 2012, 70.6% of antipsychotic prescriptions were written by GPs and 19.5% by psychiatrists (Table 4). GPs wrote a greater proportion of the scripts for typical antipsychotics (77.9% for GPs versus 12.0% for psychiatrists) than for atypical antipsychotics (GPs: 70.0%; psychiatrists: 20.1%). From 2009 to 2012 there was a 30.4% increase in atypical antipsychotics prescribed by GPs and a 27.2% increase in those prescribed by psychiatrists. For typical antipsychotics, there was a 7.0% and 4.9% decrease respectively.
ADHD medications
Overall trends (all ages)
Dispensing of ADHD medications increased 26.1% over the study period, corresponding to an average yearly increase of 6.0% (See Figure 1A). From 2009 to 2012, there was a 25.8% increase in stimulant use, with this change largely driven by increased methylphenidate dispensing (up 35.9%). There was a similar percentage increase in atomoxetine dispensing (31.6%), albeit from a much lower baseline. Dispensing of dexamphetamine was relatively stable over the study period (see Figure 1D).
Methylphenidate was the most popular ADHD medication prescribed in both 2009 and 2012 (67.4% and 72.6% of ADHD medications respectively). In 2012, dexamphetamine comprised 21.7% and atomoxetine 5.7% of all subsidised ADHD medication scripts.
Age and sex
In 2012, 62.61% of ADHD medications were dispensed to children aged 3–14 years, 19.55% to those aged 15–24, and 17.83% to those aged 25 and over (Table 5).
There was a 26.1% increase in ADHD medication dispensing from 2009 to 2012, with a 23.9% increase those aged under 25, and a 37.6% increase in those aged over 25 (see Table 1). The largest increase in methylphenidate use occurred in the 20–24 year age group (456.5%), followed by the >25 age group (188.8%). Smaller increases occurred in all other age groups. Dexamphetamine use decreased in all age groups except those aged over 25.
In 2012, methylphenidate was the most popular ADHD medication dispensed in all age groups, except those aged over 25 (77.7% dexamphetamine; see Table 3). Dexamphetamine was also highly prescribed in those aged 20–24 years (dexamphetamine 41.4%; methylphenidate 53.1%).
In 2012 the majority of children on ADHD medications were male (3–9 years: 81.2%; 10–14 years: 81.3%; 15–19 years: 76.3%; see Table 5). This proportion declined in those aged 20–24 (65.9% male) and became more evenly matched in the over 25 age group (57.5% male). Overall, dexamphetamine was more likely to be prescribed to females (62.7% male) than methylphenidate (79.2%) or atomoxetine (77.9%). There were no marked sex differences in the trends observed in ADHD medication use between 2009 and 2012.
Prescriber specialty (stimulants only)
In 2012, stimulants were prescribed primarily by paediatricians (59.1% of stimulant scripts dispensed), while psychiatrists and GPs accounted for 20.9% and 17.4% of stimulant scripts respectively (Table 5). From 2009 to 2012 there was a 56.9% increase in stimulants prescribed by GPs, a 38.7% increase in stimulants prescribed by psychiatrists and a 17.7% increase in those prescribed by paediatricians.
Discussion
In line with trends in the US and UK (Ilyas and Moncrieff, 2012; Medco, 2011), the current study reveals recent significant increases in psychotropic drug use in the Australian population. Over a period of only four years, from 2009 to 2012, there was a 16.1% increase in antidepressant dispensing, a 22.7% increase in antipsychotic dispensing and a 26.1% increase in the dispensing of ADHD medications. The Australian population increased by only 4.7% (Australian Bureau of Statistics, 2013). These changes in psychotropic drug use are a continuation of trends observed for decades in Australia (Mant et al., 1987; Stephenson et al., 2013), representing an ever-increasing reliance on psychotropics for the treatment of mental health problems.
Of particular interest are some dramatic changes reported here in the use of these drugs in child and adolescent populations. We report considerable variation in the observed trends according to age and sex, with particularly large increases in antidepressant and antipsychotic use among younger children. In contrast, the most rapid growth in the use of ADHD medications was observed in young adults and those aged over 25, although substantial increases still occurred in younger populations. Such trends suggest an increased willingness to prescribe these drugs to young people, despite ongoing controversies about psychotropic use in these populations.
Antidepressants
Dispensing of antidepressants increased over the study period in children, adolescents and adults. This trend was largely driven by increases in the use of SNRIs and NaSSAs, with little overall change in the dispensing of SSRIs. Increases in SNRI use were seen across the entire age spectrum, although growth was most marked in younger children. In contrast, SSRI use was relatively stable in adults, but increased markedly in those under 25 and was particularly pronounced in children under the age of 15.
The increased prescription of antidepressant drugs to young people is of some concern given ongoing debate around the efficacy and safety of these drugs in paediatric populations. Antidepressants may have only minimal to modest efficacy in the treatment of depression in young people (Whittington et al., 2004), but their use is clearly widespread. Antidepressant use has also been associated with psychiatric and emotional side effects, many of which appear to be more common among young people, including increased risk of suicidality, aggression and emotional blunting (Goldsmith and Moncrieff, 2011; Henry et al., 2012; Read et al., 2014). Furthermore, a large proportion of antidepressant users report sexual dysfunction and interpersonal side effects such as reduced empathy (Read et al., 2014), the long-term consequences of which are unknown.
Given its superior risk–benefit profile in these populations (Whittington et al., 2004), fluoxetine is the only antidepressant approved for the use of depressive disorders in children and adolescents in both the UK and US. Fluoxetine is also recommended as the first line pharmacological treatment for childhood depression in Australia (Psychotropic Expert Group, 2008). The pre-eminence of fluoxetine use in those aged under 20 that is reported here shows some attempt to adhere to these guidelines. The significant prescription of other SSRIs such as sertraline and fluvoxamine in younger children may represent use in anxiety disorders or in depression that has not responded to fluoxetine: in Australia SSRIs, particularly sertraline and fluvoxamine, are first-line recommended treatments for many childhood anxiety disorders, and many studies support their efficacy in these conditions (Strawn et al., 2012). While tricyclic antidepressants show little, if any, efficacy in childhood depressive disorders (Hazell et al., 1995), their use is well supported in the treatment of enuresis (Glazener et al., 2003). This may explain the significant use reported here in younger children.
A notable finding is the substantial and increasing use of SNRIs in paediatric populations. In Australia, use of SNRIs in children and adolescents is not recommended due to increased risk of hostility and suicidal ideation and behaviour (Psychotropic Expert Group, 2008). It is therefore of some concern that SNRIs make up one-third of antidepressants used in those aged under 25. In addition, the most pronounced increases in SNRI use are occurring in children aged under 15. Marked increases in SNRI use are also observed in the adult population. These trends may be due to marketing practices, given that these drugs show no substantial benefit in efficacy over the SSRIs and appear to have a greater propensity to cause physical and psychiatric adverse effects, both in adult and paediatric populations (Cipriani et al., 2009; Gartlehner et al., 2011; Whittington et al., 2004). Indeed, the current data show that desvenlafaxine and duloxetine, the newer and most marketed SNRIs, are among the most rapidly growing psychotropic drugs in all age groups.
The finding that antidepressant prescription by GPs is growing particularly rapidly compared to psychiatrists may be an indication of increasing use of these drugs in mild–moderate depression and anxiety. Indeed, GPs identify ‘chronic mild depression’ as the most common indication for which they prescribe antidepressants (McManus et al., 2003). This practice goes against evidence suggesting minimal efficacy of antidepressants in mild–moderate depression (Fournier et al., 2010) and recommendations advising non-pharmacological treatments as first line options (Psychotropic Expert Group, 2008).
The observed increases in antidepressant use, both in paediatric and adult populations, likely result from a number of factors. Firstly, the greater tolerability and safety of the newer antidepressants compared to the tricyclics and MAOIs has increasingly moved prescribing of these drugs into general practice (McManus et al., 2003; Westenberg and Sandner, 2006). Indeed, the current data show that almost 90% of antidepressant prescriptions are provided by GPs. Further, growth in antidepressant use is likely driven by increased public awareness and recognition of depressive and anxiety disorders (Partridge et al., 2012), and the use of antidepressants rather than benzodiazepines as a first line pharmacological treatment for anxiety disorders (Psychotropic Expert Group, 2008). Antidepressants are also finding increasing utility in diagnoses other than depression and anxiety, including neuropathic and chronic pain, and sleep and eating disorders (Henderson et al., 2010). However, the current data is limited in its ability to pick up use of the newer antidepressants in these indications given the current lack of approval and subsidy for these conditions in Australia.
Antipsychotics
Dispensing of atypical antipsychotics in Australia increased over the study period, in line with recent reports from the US (Medco, 2011) and UK (Ilyas and Moncrieff, 2012). This increase occurred in all age groups, with the greatest changes in children under the age of 15.
Given the static prevalence of psychotic disorders over this period (Kirkbride et al., 2012), the observed increases in antipsychotic use likely result from the recent approval of antipsychotic medications for the treatment of bipolar disorder and disruptive behaviour associated with autism and dementia. Indeed, bipolar disorder accounts for approximately one-fifth of adult antipsychotic prescriptions in the US (Olfson et al., 2012), reflecting the efficacy of these drugs in the treatment and prevention of mania (Fountoulakis and Vieta, 2008; Scherk et al., 2007). Antipsychotics are also widely used in dementia, with females over 75 having the highest antipsychotic utilisation of any age group in Australia (Hollingworth et al., 2010).
As with adults, the majority of antipsychotics used in children and adolescents are for non-psychotic diagnoses (Rani et al., 2008). The recent approval of risperidone for use in behavioural disturbance in autism may in part underlie its growing popularity observed here in children. The prevalence of autism spectrum disorders has risen markedly over recent years, with a corresponding increase in their treatment using antipsychotics (Basu and Parry, 2013). While evidence suggests some efficacy of risperidone in improving behavioural disturbance in autism (Sharma and Shaw, 2012), non-pharmacological interventions are recommended first line treatments (Psychotropic Expert Group, 2008). Antipsychotics are also increasingly used in children with other diagnoses associated with disruptive behaviour including developmental disorders, ADHD, conduct disorder and oppositional defiant disorder (ODD). Indeed, disruptive behaviour disorders represent 63% of antipsychotic prescriptions in US children, with other common diagnoses including anxiety, depression, bipolar disorders, autism and developmental disorders (Olfson et al., 2012). Antipsychotics show some efficacy in improving symptoms of disruptive behaviour (Loy et al., 2012), yet, as in autism, psychological and family therapies are recommended first line treatments (Psychotropic Expert Group, 2008). While the use of antipsychotics for the treatment of disruptive behaviours in the absence of autism is not approved in Australia, the current data may partially cover such off-label uses by virtue of their similarity with approved indications. The increased diagnosis and treatment of the controversial paediatric bipolar disorder may also underlie the observed increases in antipsychotic use in children; however, this trend appears largely limited to the US (Robbins et al., 2011). Antipsychotics are also increasingly used off-label in the population for the treatment of anxiety, sleep disorders and as an adjunct in mood disorders, although the current data is limited in its ability to detect changes in these unsubsidised uses.
The finding that antipsychotic use is more common among males than females, particularly in the younger age groups, may be explained in terms of the predominance of males with autism and disruptive behaviour disorders (Centers for Disease Control and Prevention (CDC), 2010, 2012). In adults, antipsychotics are prescribed similarly to males and females due to their proportionally greater use in female-dominated illnesses such as bipolar disorder, depression and dementia (Hollingworth et al., 2010; Olfson et al., 2012).
Of interest is the high rate of antipsychotic prescription in general practice, with GPs prescribing more than 70% of antipsychotics dispensed. While GPs often write continuing prescriptions following initiation of treatment by psychiatrists, this practice is unlikely to solely account for these figures. Instead, the high level of antipsychotic prescribing by GPs likely reflects increased acceptance of the use of antipsychotics in non-psychotic diagnoses such as depression and insomnia.
The rapid increases in the use of antipsychotics in both adult and paediatric populations are a cause for concern. Atypical antipsychotics carry the risk of adverse effects including weight gain and metabolic syndrome, extrapyramidal symptoms and prolactin elevation, all of which appear more problematic in young people (Correll, 2008; Sikich et al., 2008). Furthermore, the sedative effect of these drugs may impair cognition and academic performance. The lasting impact of these adverse effects on health and development must also be considered. The extent of these effects is unknown, but may include diabetes and metabolic syndrome associated with age-inappropriate weight gain, and osteoporosis and reproductive problems related to hyperprolactinemia (Correll, 2008).
ADHD medications
There was an increase in the dispensing of ADHD medications in all age groups in Australia from 2009 to 2012, primarily driven by changes in methylphenidate and atomoxetine use. In particular, marked increases were apparent in the use of methylphenidate in those aged 20–24 and over 25, with lesser increases in other age groups. In contrast, dexamphetamine usage declined in all child and adolescent populations while its use increased somewhat in adults.
The increased use of ADHD medications in Australia reflects trends seen in the US (Zuvekas and Vitiello, 2012), UK (McCarthy et al., 2012) and globally (Scheffler et al., 2007). One of the most likely factors contributing to these trends is the ongoing rise in the diagnosis of ADHD: In the US, diagnostic rates rose from 7.4% in 2003 to 9.5% in 2007 (CDC, 2010). Further, increasing acceptance of ADHD as a lifelong disorder has seen particularly marked increases in ADHD diagnosis and medication use in older adolescents (CDC, 2010; Zuvekas and Vitiello, 2012) and adults (McCarthy et al., 2012), in line with the current data. These increases in diagnosis, and accordant effects on medication usage, are likely to continue with the further broadening of diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (Thomas et al., 2013). While increased diagnoses are considered by some to be a reflection of legitimate cases, others have raised concerns about over-diagnosis and subsequent medicating of sub-threshold symptoms and mild cases (Thomas et al., 2013). Indeed, ADHD is widely recognised as a difficult disorder to accurately diagnose given the high overlap between symptoms and normal behaviour.
As approximately 86% of those diagnosed with ADHD in the US are considered to have a mild–moderate form of the disorder (CDC, 2010), the potential for overmedication is considerable. Indeed, guidelines recommend against drug treatment for mild and moderate ADHD (National Institute for Health and Care Excellence (NICE), 2008, 2013). In addition, ADHD has considerable symptomatic overlap with other disorders such as ODD and paediatric bipolar disorder (Turgay, 2009), potentially increasing rates of misdiagnosis. To minimise the chance of misdiagnosis, Australian guidelines recommend that GPs refer patients on to specialists where a diagnosis of ADHD is suspected. Most states and territories in Australia also restrict stimulant prescribing to certain specialties, particularly paediatricians, psychiatrists and neurologists. As such, paediatricians prescribe the majority of ADHD medications to children and adolescents, as reported here; however, prescription by GPs substantially increased over the study period.
Untreated ADHD has a variety of negative consequences, being associated with poor academic and vocational performance; social difficulties; increased risk of substance use, criminal behaviour and accidents; and psychiatric comorbidity (Thomas et al., 2013). As such, adequate treatment is vital. Randomised controlled trials have demonstrated robust efficacy of methylphenidate, dexamphetamine and atomoxetine in reducing symptoms of impulsivity and hyperactivity and improving short-term educational and social outcomes (Faraone and Buitelaar, 2010). However, there is little evidence that treatment with ADHD medications improves long-term outcomes (Government of Western Australia, Department of Health, 2010; Jensen et al., 2007; Molina et al., 2009). ADHD medications have also been associated with a range of adverse effects that must be balanced against the benefits of the drug, including: loss of appetite; weight and growth retardation; insomnia; increased heart rate and blood pressure; psychiatric side effects such as psychosis, self-harm, suicidal ideation and mania (Wigal, 2009); and potential effects on neural development. ADHD medications also carry an increased risk of sudden death, myocardial infarction and stroke in those with pre-existing cardiac conditions and in adults with certain risk factors (Wigal, 2009).
Australian guidelines for the treatment of ADHD recommend the stimulants methylphenidate and dexamphetamine as first line pharmacological treatments, in line with the superior efficacy of these drugs over the non-stimulant alternative, atomoxetine (Faraone et al., 2006). In accordance with these guidelines, the current data demonstrate that the stimulants comprise over 90% of ADHD medication usage in all age groups. A significant preference, however, is observed for methylphenidate over dexamphetamine in child and adolescent populations, with methylphenidate comprising over 80% of ADHD medication prescriptions. The availability and subsidy of an extended-release form of methylphenidate may underlie this preference. Extended-release formulations allow for once-daily dosage and are widely believed to have the advantage of maintaining drug efficacy through the latter part of the day, while evening rebound effects may occur with short-release formulations (Wigal, 2009). Although the current dataset did not permit distinction between different forms of methylphenidate, previous analyses suggest a 3:1 preference for extended-release over immediate release forms in the Australian population (Stephenson et al., 2013).
In contrast to the pre-eminence of methylphenidate in child and adolescent populations, dexamphetamine comprises 78% of ADHD medications dispensed to adults. The reason for this is unknown, but may stem from its abuse potential. Indeed, recent studies suggest that up to 35% of college age individuals abuse psychostimulants, primarily immediate release formulations (Wilens et al., 2008).
In addition to their use in the treatment of ADHD, ADHD medications are often utilised in disruptive behaviour disorders such as ODD. As such, an additional factor contributing to the increase in ADHD medication use may be the increasing diagnosis of ODD and the recognition of the efficacy of stimulants in short-term symptomatic control (Turgay, 2009). However, long-term benefits have not been established. The use of stimulants in ODD and other disruptive behaviour disorders is not currently subsidised in Australia, limiting the utility of the current data in identifying such usage.
The high preponderance of ADHD and disruptive behaviour disorders diagnoses in children medicated with ADHD medications accounts for the high male to female ratio observed in those under 25: Approximately three-quarters of those diagnosed with ADHD are male (Government of Western Australia, 2010).
Although ADHD medications are also approved in Australia for use in narcolepsy, the low incidence of this disorder (25–50 per 100,000) suggests minimal contribution of this use to the present data (Longstreth et al., 2007).
Limitations
As previously mentioned, the DoHS dispensing database only includes data on prescriptions dispensed under the PBS/RPBS, thereby omitting data on prescriptions costing less than the general co-payment, private scripts and inpatient prescriptions in public hospitals. As such, the use of the PBS database limits the detection of prescription of drugs for off-label uses. This is of particular relevance to the SNRI and tricyclic antidepressants, which are widely used for the treatment of pain, and the antipsychotics, which are often used off-label for anxiety, sleep and bipolar II disorder. However, we cannot exclude the possibility that the current data does include some off-label use, given the likelihood that doctors write subsidised scripts for unsubsidised indications.
The limitations of the PBS database particularly influence the interpretation of certain results. In 2010, the PBS covered only 67.1% of SSRI dispensing, with the cost of many of these drugs falling below the general co-payment threshold, thus the reported results would underestimate use. This is particularly notable in the case of escitalopram (59.3% covered) and fluoxetine (68.1% covered). Of the antipsychotics, clozapine use is dramatically underestimated, with 77.8% of use not accounted for. In addition, the use of dexamphetamine (59.7% covered) is underestimated (DoHA, 2010).
Conclusions
In conclusion, the current study shows ongoing increases in antidepressant, antipsychotic and ADHD medication prescribing in the Australian population, similar to other countries such as the US and UK. The increases in antidepressant and antipsychotic use were particularly salient in children and adolescents, with use of ADHD medications growing most rapidly in young adults. These trends reflect an increasing acceptance and reliance on medication for the treatment of mental illness, despite ongoing controversies.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
Iain McGregor is currently a National Health and Medical Research Council Principal Research Fellow and Emily Karanges is supported by an Australian Postgraduate Award and University of Sydney Vice Chancellor’s Scholarship. We acknowledge support from the Australian Research Council for research on antidepressants and adolescent brain development [grant number DP0988609].