
Abstract
The aim of the present study was to review international literature on the incidence of suicide on railway networks, describe risk factors associated with it, and examine existing prevention practices. Searches on Medline and PsycINFO for the period 1966–2007 were performed. Thirty original studies published in English on epidemiology of rail suicide were included in the review along with peer-reviewed articles on risk factors and prevention of rail suicide. Internationally, suicide by collision with a train accounted for 1–12% of all suicides, with up to 94% of all attempts resulting in death. Suicide by train seriously affects not only survivors, but also train drivers and bystanders. Correlations between density of rail network, number of passengers and number of suicides by train have been found. Conflicting data exist on gender ratio of this type of suicide, but studies are homogenous in identifying young adults (20–40year of age) as those most exposed to train suicide. Documented psychiatric diagnoses were found in up to 83% of cases. Mid-seasonal peaks were also identified, with events occurring mostly during late morning and early afternoon. Limited evidence exists for effective suicide prevention practices. Successful examples are represented by pits and sliding door systems (Singapore Mass Rapid Transit System) and responsible media reporting (Viennese Subway). Suicide by train involves emotional and financial costs to individuals and society as a whole. A combination of different strategies might significantly reduce its effect.
Suicide is among the major external causes of death in Australia, and between 1997 and 2005 the total number of suicides was higher than the number of transport-related accidents [1]. In 2005 the Australian Bureau of Statistics registered 2201 deaths by suicide, with the overall rate of 10.3 per 100 000 population [1]. Psychopathology, particularly affective and psychotic disorders, substance abuse, history of suicidal behaviour and ideation, familial history of suicide and psychopathology, demographic and socioeconomic factors (including unemployment), negative life events, low social support and psychological factors (such as hopelessness and problem solving deficits) are among the most prominent risk factors for suicide [2]. Despite decades of research, there is still limited knowledge regarding constellations of risk factors related to the choice of a particular method of suicide. Identification of factors that affect the choice and substitution of method can support development of effective suicide prevention strategies [3].
Suicide by collision with a train is one of the most lethal and violent methods of death. The first case of rail suicide was recorded in England in 1852, approximately 20 years after the commencement of the rail era [4]. Today, suicide by collision with a train is a relatively rare method, accounting for 1–12% of all suicides internationally [5], but highly lethal, with up to 94% of attempts resulting in death [6]. Rail suicide is often a public event witnessed not only by train drivers but also by onlookers on platforms and train passengers. Therefore, in addition to the psychological effect on family and friends of the deceased, traumatic consequences are experienced by railway staff and passengers. Financial and organizational costs to the railway system, including delays in services and driver absenteeism [7], [8], are also directly connected with suicide incidents. In summary, ‘the costs of railway suicide are enormous in terms of human lives lost, driver and bystander trauma, and delays to the service’ [9].
This paper reviews research on rail suicide in order to identify epidemiological and clinical factors that increase the risk of engaging in this type of behaviour, and examines approaches to prevention of suicide on rail networks and their effectiveness.
Methods
The review is based upon searches of PsycINFO and Medline databases covering the period 1966–2007. The following keywords were used for the search: ‘train suicide’, ‘railway suicide’, ‘violent suicide and railway’, and ‘fatal and railway accidents’. Lists of references of the retrieved articles were searched to identify further material.
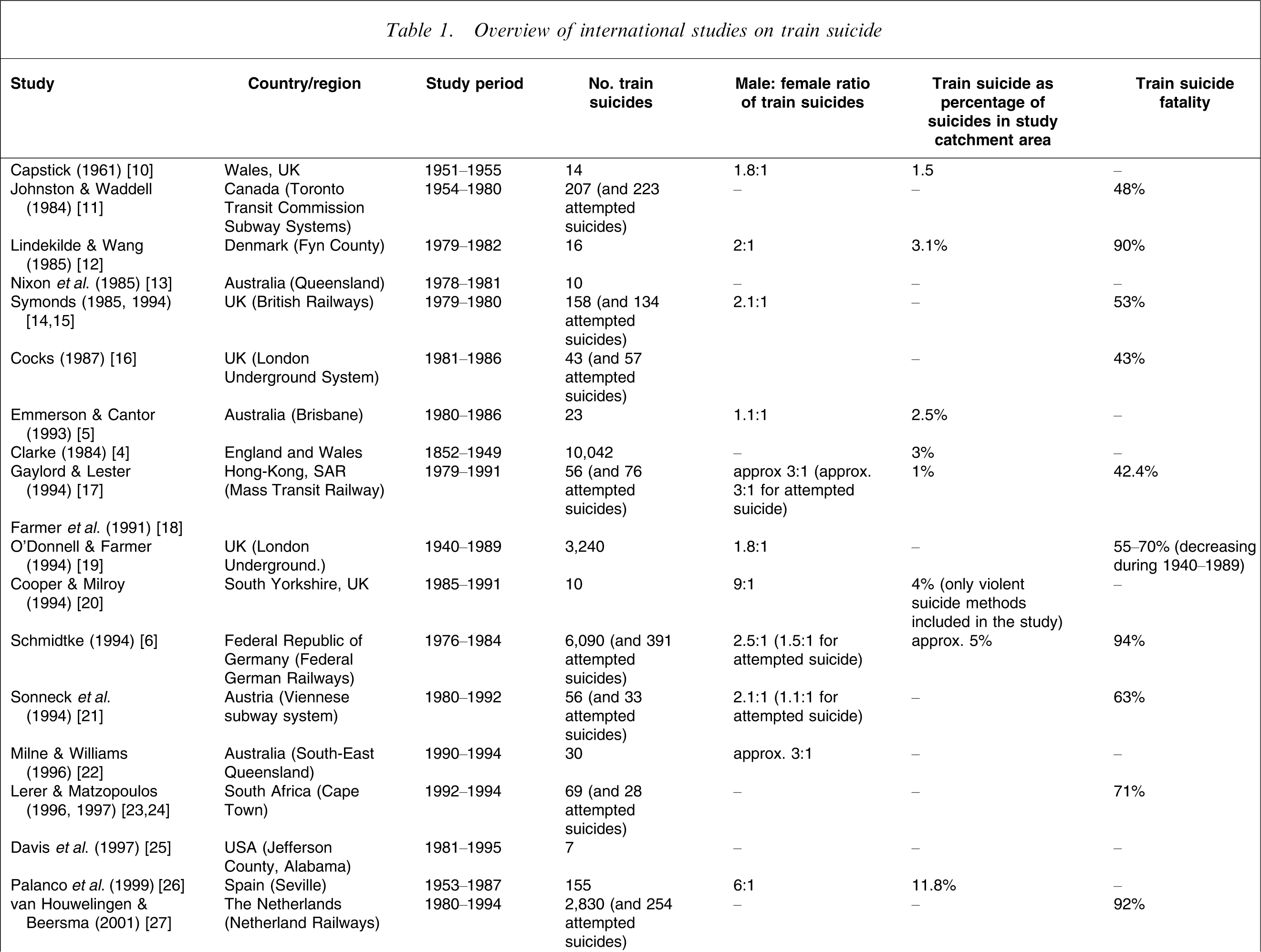
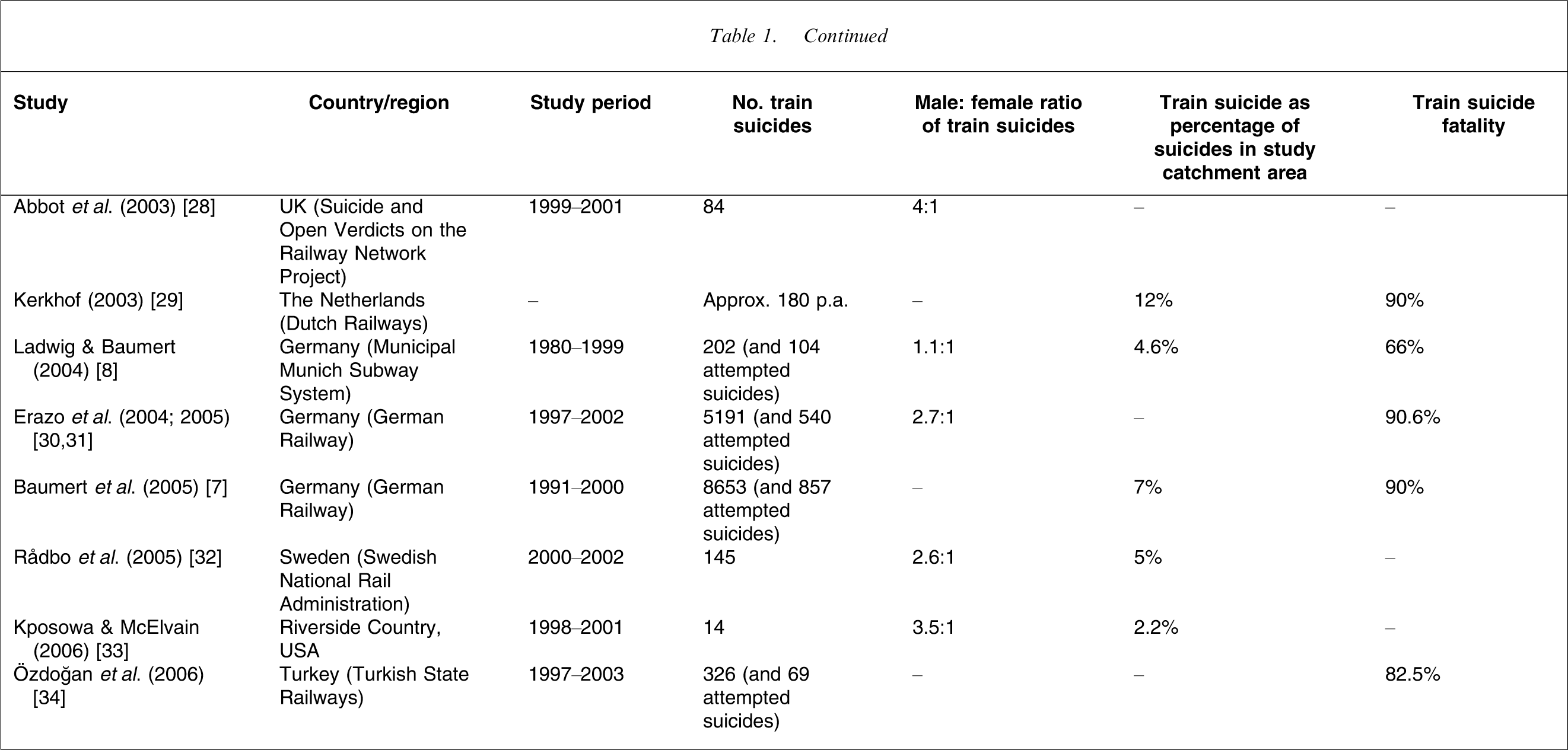
Thirty original studies on epidemiology of rail suicide published in English were included in the review (Table 1). Also, peer-reviewed articles on risk factors and prevention of rail suicide were included. Forensic pathology case studies of rail suicide deaths were excluded from the review.
Overview of international studies on train suicide
Results
Lethality and incidence of rail suicide
Rail suicide is a very lethal method with fatality rates between 43% [17] and 94% [6] (Table 1). Its incidence ranges from 1% [17] to 12% of all suicidal deaths [26], [29] (Table 1). Rising trends in rail suicide rates were reported in Canada in 1954–1980 [11], Denmark in 1979–1982 [12], England and Wales in 1852–1949 [4] and Turkey in 1997–2003 [34]. A similar increasing trend was observed on the London Underground (LU) system for 1940–1989 [18], [19] and in the Viennese underground system for 1984–1987 [21]. But rates of train suicide decreased in Spain in 1953–1987 [26] and were stable over the period 1991–2000 in Germany [7] and Queensland, Australia, for 1980–1986 [5]. There appears to be no correlation between national and rail suicide rates [35].
Risk factors for rail suicide
Sociodemographic risk factors
In comparison to the world average male: female suicide ratio of 3:1 [36], some studies show a similar or higher gender ratio of rail suicide victims (Table 1). For example, in the USA, Kposowa and McElvain found the ratio of 3.5:1 [33], and in Spain Palanco et al. reported the ratio of 6:1 [26]. Other studies indicate that the ratio is lower, with similar numbers of rail suicides in both genders [5], [8]. Although in the general population non-fatal suicidal behaviour is more frequent in female than male subjects [37], an identical male: female ratio of 3:1 for both fatal and non-fatal suicidal behaviour by train was reported in Hong Kong [17], and a ratio of 1.1:1 for non-fatal attempts was found in Vienna [21].
The majority of victims of train suicide are young adults between the age of 20 and 40 years [5], [6], [8], [17], [22], [28], [29], [32] and the incidence of train suicide decreases with age in both genders [19]. A different age pattern of rail suicide was reported in Spain, where the average age of a victim was 54 years for men and 49 years for women [26], and in Japan, where the highest incidence of rail suicide was found in the 51–60 years age group [38].
Rail suicide has also been reported in children, adolescents and young adults [39], [40]. In a comparative study of 48 cases of suicide in young people aged 13–16 years in South Australia and San Diego, Byard et al. found five cases of train suicide in the Australian sample, which accounted for 10% of suicidal deaths and included a similar number of male and female victims (i.e. three and two, respectively) [39].
Psychopathology and psychiatric hospitalization
Individuals with serious psychopathology, especially psychotic disorders, are prone to use violent and lethal means of suicide [26]. High prevalence of psychiatric disorders was found among people who died by suicide by train [5], [14], [15], [28], [29]. For example, a study of suicides on the UK railway network found that approximately 60% of victims had a psychiatric diagnosis, mostly major depressive disorder (24%) and schizophrenia (14%) [28]. A study in Queensland showed that 83% of victims had a documented psychiatric history, and schizophrenia and depression were the most frequent diagnoses (57% and 17%, respectively) [5].
Up to 81% of persons who die as a result of being hit by a train [12], [41], [42] have a history of psychiatric hospitalizations, with some psychiatric inpatients choosing this method of suicide while absconding from psychiatric wards [28]. van Houwelingen and Kerkhof reported that 53% of people who died after being hit by a train in the Netherlands were under psychiatric care at time of their death, with 49% of them being current inpatients [43].
Previous suicidal behaviour and repetition
Forty per cent of people who died by train suicide had a history of previous attempts, and 21% repeated their attempts with either a fatal or non-fatal outcome [42], sometimes switching methods, for example from self-poisoning or cutting [10]. Despite the high fatality of method, repetition of suicidal behaviour does not seem to be elevated among individuals who survived a rail suicide attempt in comparison to other attempters [44]. A 10 year follow-up study of attempters on the LU system showed that the incidence of suicidal death in that group was not higher than among individuals using other methods (i.e. 10%) [41].
Imitation and contagion
A study of survivors of attempts on the LU system showed that almost half of attempters personally knew someone who died or attempted suicide using this method, for example fellow patients at a psychiatric hospital [41]. In addition, studies show that media reports of both non-fictional and fictional cases of rail suicide lead to more frequent use of this method [6], [21], [45].
Impulsivity/premeditation
Studies show that train suicide is either impulsive or premeditated, in both cases with a high intent to die. In the Guggenheim and Weissman study some of the attempts were premeditated and planned, while other happened without preparation [46]. Almost all (90%) of survivors of the LU believed that their behaviour would have led to death, but their attempt was usually impulsive and involved little preparation [47]. Given the well-established correlation between alcohol consumption, impulsiveness and increased suicide risk [48], some studies analysed alcohol levels in victims of rail suicide as compared to victims of non-intentional deaths. Results of such studies remain inconclusive: some research shows that train suicide completers have higher levels of alcohol consumed prior to death than in other types of suicides [26]; other data did not confirm this indication [14], [23], [24].
Circadian, weekly and seasonal patterns
Train suicide appears to be more frequent around late morning and early afternoon [8], [18], [19], [30], [31] and at midday [11], [12], [17], [34]. The distribution of suicide incidents is related to availability of services during the day [41] and daylight visibility, affecting both attempters and rescuers [31], [27].
The number of incidents has been reported to peak on Monday and Tuesday, with lowest numbers during weekends [6], [8], [18], [21], [30–32]. Such fluctuations are related to volume of services over the week and factors external to the rail network, including the ‘broken promise effect’, that is, dysphoric mood resulting from a discrepancy between how one actually feels and the expected positive outcomes ‘promised’ by holidays, Spring and weekends [49], [50]. The latter explanation was questioned by O'Donnell and Farmer, who observed that although the numbers of LU trains were reduced on both weekend days, the drop in the number of suicides was exclusive for Sundays [19].
In addition to circadian and weekly fluctuations, there appear to be also Spring and/or Autumn peaks in rail suicide [11], [18], [19], [30], [32]. The seasonality effect appears more pronounced in violent suicides, including train suicide, than in deaths resulting from softer methods [51], [52].
Suicide hot spots
Train suicide incidents are not evenly distributed on the rail networks; frequently hot spots or particular areas of the network with elevated incidence of suicide are identifiable [28], with a tendency to be located in proximity to psychiatric hospitals or other places easily accessible to psychiatric patients [53]. In the Netherlands 20% of rail suicides happened near large psychiatric institutions [29], and in Australia approximately 50% of suicides were committed near mental hospitals [5], [13]. Also, stations with high levels of average annual passenger throughput, including busy transfer stations, potentially become suicide hot spots [18], [19].
Length and density of rail track
International differences in the incidence and trends of train suicide have been linked to different ease of access to the rail network, measured by length and density of rail track [7], [29]. Clarke found a significant positive correlation between numbers of people dying from suicide by train, length of railway track and number of passengers carried on the railway network [4].
Behaviour patterns
Guggenheim and Weisman distinguished four types of victims of train suicide: ‘jumpers’ (i.e. individuals jumping or leaping directly in front of an approaching train in the presence of bystanders); ‘liers’/‘prostraters’, who lie down across the tracks waiting for an oncoming train; ‘touchers’, who get electrocuted by touching the third rail; and ‘wanderers’, descending from the platform into the pit when no train is visible and walking along the tracks [42], [46]. The level of suicidal intent and willingness to be rescued influence the choice of behaviour. For example, wanderers seem to communicate their suicide intent by walking on the tracks, which allows for help and rescue more readily than in other methods [5], [42], [46].
Symonds suggested categorization of rail suicides into private (i.e. no witness; usually on track) and public (i.e. in presence of others; typically at a train station) [14], [15]. His studies showed that the majority of rail suicide victims in the UK died in public settings (64%), mostly by jumping from a crowded platform. Approximately one-third of victims died a private death: in the majority of cases in this category, the body was found on railway track between stations. Contrary to Symond's findings, Rådbo et al. reported that more than half of suicides in Sweden died in urban locations distant from station areas, with approximately one-third recorded at stations (55% and 30%, respectively) [32]. The majority (75%) of victims were standing, walking, lying or sitting on the tracks or in their proximity, and only 14% appeared suddenly in front of the train by jumping or running.
Prevention of rail suicide
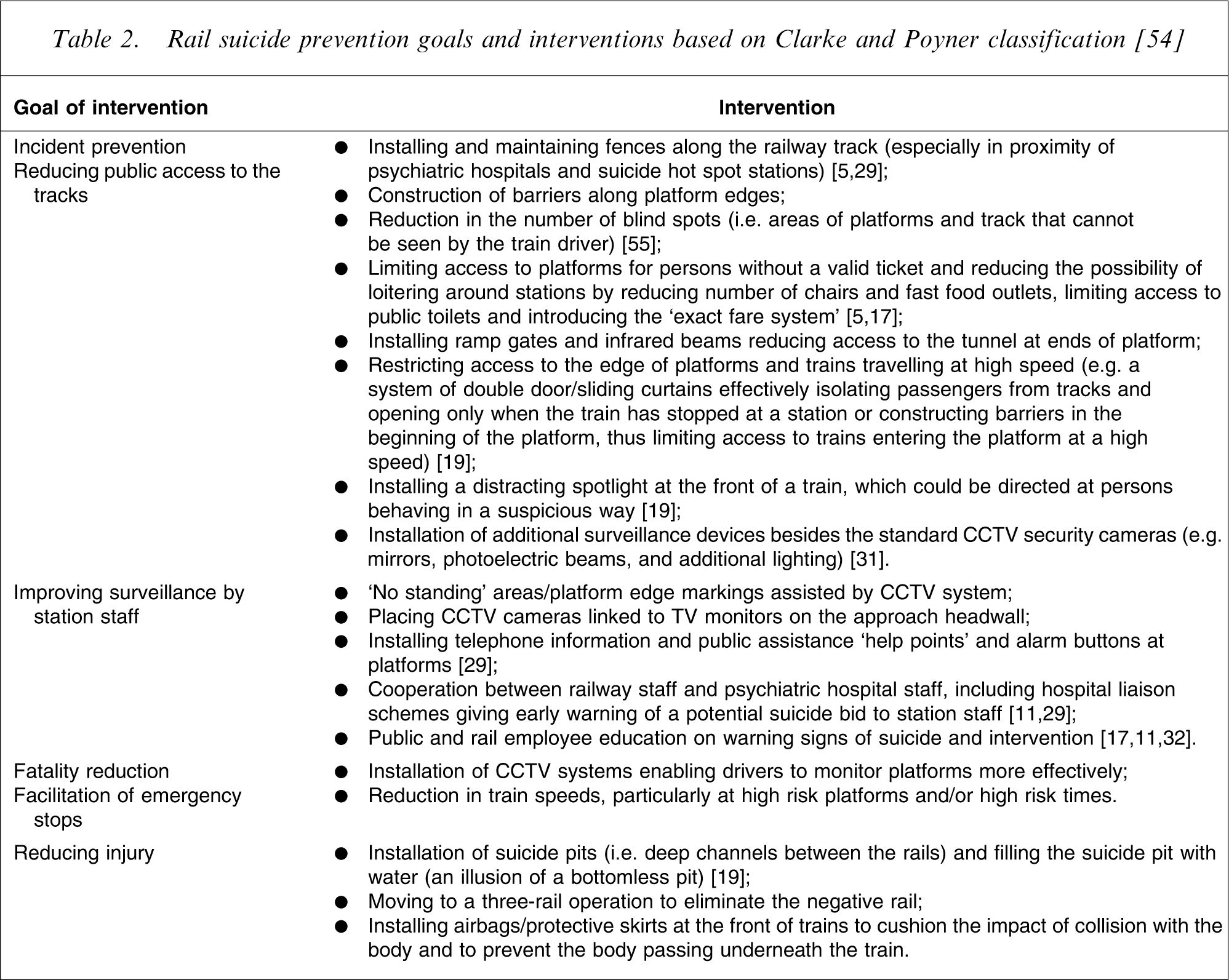
Although not an easy task, prevention of rail suicide is possible. O'Donnell et al. warn against adopting the fatalistic attitude that considers suicide on railway networks as an ‘unfortunate but unavoidable, negative consequence of railways’ [9]. There are two goals of preventing rail suicide: reducing incidence of the behaviour and reducing its mortality [19], [38], [54]. Table 2 presents an overview of rail suicide prevention measures.
Rail suicide prevention goals and interventions based on Clarke and Poyner classification [54]
Effectiveness of programmes
The evidence regarding the effect of train suicide prevention measures is limited. There are data to support the effectiveness of suicide pits, that is, deep channels between the rails [16], [18], [19], [38] and sliding doors at platforms limiting access to the track [38], and indirect evidence pointing out the potential effectiveness of airbags or skirts at fronts of trains [54]. Also, studies show that responsible reporting of suicide in the media [21], [56] and community media campaigns [57] help to reduce the number of rail suicides.
Since the mid-1930s suicide pits were installed at all deep stations of the LU network, and they have proved effective in reducing the suicide mortality [18], [19]. Based upon data for the period 1973–1990 O'Donnell and Farmer reported that the 66% of incidents happening at stations without suicide pits ended in death as compared to 45% at stations with pits: a statistically significant difference (χ2=72.1, df = 1, p < 0.001) [19].
A sliding door system on the Singapore Mass Rapid Transit System was installed in order to save energy in air-conditioned stations and there have been no incidences of suicide since the opening of the network in 1987 until the early 1990s [38].
An airbag, which inflates after the use of an emergency brake, can cushion and reduce the impact of collision between a body and a train, and a rigid skirt can prevent the body from falling underneath the train. It has been suggested that a well-designed protective skirt also has a psychological effect on people considering a train suicide by reducing the appeal of the front of a train as a tool for suicide [54]. Unfortunately, no data are available in the published literature regarding the effectiveness of airbags and skirts in preventing rail suicide and reducing the severity of injuries. Clarke and Poyner draw analogies between the potential effects of such devices and data coming from studies on car design and pedestrian fatality [54]. These studies show that the design of the front of a vehicle, for example smooth versus sharp design, padding, lowering the point of impact with the body and so on, has a significant effect on severity of injuries sustained by accident victims [58–60].
Following implementation of guidelines for responsible media reporting on suicide in Vienna in 1987, the number of suicides and suicide attempts in the local subway system dropped by 80% [21], [56]. There is also indirect evidence that community media campaigns advertising local crisis intervention centres and hotlines at railway stations are effective [15], [29]. In the UK a collaborative project between the Rail Safety and Standards Board and the Samaritans resulted in production of a booklet (Reducing suicides at railway stations), staff training and a poster campaign advertising the crisis intervention phone services [61]. No data have been published regarding the effect of the campaign on the incidence of rail suicide, although a similar initiative, that is, the posting of signs with the Samaritans’ national telephone number at a suicide hot spot car park in New Forest in England, resulted in a significant reduction in the number of suicides [57].
Limitations
This paper presents a review of the literature on incidence, risk factors and prevention of rail suicide. A systematic review of retrieved studies was not conducted due to problems with comparability of data coming from a wide range of sources across original studies, including police and coronial files [5], [20], [25], and rail network incident and death registers [7], [32].
The majority of studies focused on fatal suicidal behaviour and there is a paucity of epidemiological data and research on risk factors for suicide attempts on railway networks; consequently only limited information regarding such behaviour has been covered in the present review. Also, there is only limited evidence available regarding effectiveness of prevention strategies based on the published studies.
Where data on suicide deaths on railway networks have been presented, it should be kept in mind that variations exist regarding definition of suicidal acts by different rail and metropolitan subway networks, with some cases of suicide recorded as accidents, a problem shared with all suicide mortality statistics [36], [38]. In addition, the World Health Organization's ICD includes rail suicide in the broad category of ‘intentional self-harm by jumping and lying before the moving object’ (X81) [62]. This category also includes intentional self-harm by jumping and lying in front of other moving objects, including trams, cars and trucks. Consequently, there are problems with availability of nationwide data on the incidence of train suicide (e.g. in Australia), because national mortality statistics usually do not present disaggregated data.
Discussion
Review of the literature indicates that rail suicide is a relatively rare method of self-harm that accounts for 1–12% of all suicides [17], [26], [29]. It is a highly lethal method with fatality rates ranging between 43% [17] and 94% [6], depending on design of rail track and vehicles, and design of stations, including suicide pits [19].
Results of studies strongly converge to create the profile of a typical victim of rail suicide: a young man between the age of 20 and 40 years with a history of psychopathology (particularly schizophrenia and affective disorder) and psychiatric hospitalization [8], [32], [43]. Imitation and contagion, as well as ease of access to rail track, potentially contribute to the choice and popularity of the suicide hot spots [28]. Of special concern is the vulnerability of individuals with psychopathology and under psychiatric care, including inpatient care, to such a highly lethal method of suicide [43]. The relatively high incidence of suicide by train among adolescents under the age of 21 (with a gender ratio close to 1:1) warrants further attention [39], [40]. Recognition of typical behavioural patterns, popular locations, seasonality and timing, along with psychological factors involved (e.g. public attention seeking in the case of public suicides, and impulsivity or premeditation of attempts) can help to identify high-risk populations and locations, and thus inform development of effective approaches to prevention.
Despite the high fatality of the method, repetition of suicidal behaviour does not seem to be elevated among individuals who survived a rail suicide attempt in comparison to other attempters [44]. The relatively low incidence of repetition in this group seems unexpected in the light of follow-up studies of medically serious attempters [63], [64]. In some cases, however, surviving a nearly lethal attempt has a cathartic effect, limiting the occurrence of further self-harm [47], [65].
Although certain factors, including gender, familiarity with the method and its availability, influence the choice of suicide method, to date no comprehensive model regarding the choice of method of suicide, including rail suicide, has been developed [66]. In a psychodynamic perspective, suicide by train represents a passive submission to a destructive dominant physical force or is an expression of the wish to be overwhelmed and murdered [6], [46]. Due to the often public nature of death, which involves not only train drivers but also other witnesses, train suicide sometimes is an expression of interpersonal hostility and attention seeking [5], [6]. Collision with a train is usually perceived as a quick and foolproof method, with the speed of death overcoming concerns of pain [9], [67] or ambivalence [7], [42]. Choice of this method can be related to delusional systems in psychosis [14], although in some cases it is the only method available to absconding psychiatric patients [46], [54].
Many approaches to prevention of rail suicide have been suggested and implemented, but there is only limited evidence available regarding their effectiveness. Restricting access to lethal means of suicide is among the most effective means of suicide prevention [3], with the risk of means substitution generally considered to be low [68], [69].
The aftermath of rail suicide and the effect of death on train drivers involved in the incidents also require consideration. In the literature the term ‘person under train’ (PUT) is used to denote ‘an event caused by a person being hurt or killed by a (subway) train because he or she has fallen (incidentally or intentionally) in front of a moving train’ [70]. The detailed description of the drivers’ trauma is beyond the scope of this review, but studies looking at psychological and somatic reactions related to PUT show that some drivers experience severe adverse reactions [71]. Although these reactions usually are transient and do not have a long-tem effect on their ability to perform the job [72], they are part of the human and organizational costs of rail suicide. Trauma management programmes for train drivers are now standard procedures on many networks.
Conclusions
The extremely high lethality of collision with a train as a method of suicide, comparable to the fatality rate of firearms (>90%) [73] and hanging (>70%) [74], calls for special attention regarding its prevention and further research. Victims of rail suicide share many characteristics with individuals using other methods, including psychiatric diagnoses, impulsivity and influence of alcohol [2]. The vulnerability of individuals with serious psychopathology, however, including psychiatric inpatients, and the role of ease of access to the rail track, require close cooperation between railway companies and mental and public health services for effective prevention.
The example of Singapore Mass Rapid Transit System shows that effective prevention of rail suicide is possible. Suicidal behaviour on the railway networks results from a complex interaction of a variety of factors, including sociodemographic, psychopathological and environmental variables, and ‘preventive strategies are unlikely to work unless they are the result of concerted inter-agency action’ [28].