
Abstract
Objective:
The objective of this study was to identify factors associated with poor dietary intake (less than four servings of fruit and vegetables daily) in a large nationally representative sample of adults with psychotic disorders.
Methods:
The sample comprised 1286 adults aged 18–64 years who took part in the second Australian national survey of psychosis. Dietary information was obtained using a standardised questionnaire; all participants provided fasting blood samples. Variables that may be related to diet and nutritional intake were investigated; these included demographics, physical health outcomes, physical activity, substance use, symptom severity and financial difficulty. Dietary status was explored by sex, age and body mass index using univariate analyses, while a multivariate analysis was performed to identify predictors of low nutritional intake.
Results:
Approximately 74% of participants ate less than four servings of fruit and vegetables daily. This was associated with a lower body mass index (p<0.05), lower levels of physical activity (p<0.05), sedentary behaviour (p<0.05), substance use (p<0.001), more negative symptoms (p<0.05), eating less frequently (p<0.001), consuming whole fat milk compared to low fat milk (p<0.05), adding salt to food (p<0.05) and financial difficulty (p<0.05). Male sex and younger age (18–34 years) were also associated with lower fruit and vegetable intake (p<0.001). A multivariate regression analysis showed that current smoking (p<0.001) and alcohol (p<0.01) and cannabis abuse (p<0.05) were risk factors for lower fruit and vegetable intake.
Conclusion:
The findings suggest that poor diet in people with psychosis, as reflected by less than four servings of fruit and vegetables daily, is accompanied by other unhealthy behaviours, which has important implications for the development of effective interventions. Importantly, current smoking is a significant predictor of dietary inadequacy.
Introduction
Dietary intake and health outcomes among people with psychosis are poor compared to people in the general population (John et al., 2009; Wysokinski et al., 2012). High caloric diets with low nutritional value are often prioritised over healthier meals (Simonelli-Munoz et al., 2012), contributing to a higher prevalence of obesity and metabolic syndrome which is almost double that of the general population (John et al., 2009). People with schizophrenia or bipolar disorder die 12–19 years earlier than the general population (Laurson, 2011) and cardiovascular illness contributes most to their poor health outcomes. Apart from antipsychotic medication, dietary intake is amongst other factors (smoking, physical inactivity, hazardous alcohol use, and obesity) that are modifiable through behavioural changes.
According to the World Health Organization (WHO) dietary guidelines, eating at least five servings (80 grams per serve) of fruit or vegetables per day is important to maintain good health (WHO, 2009). The Australian definition of a serving size for vegetable intake is slightly lower than WHO recommendations (75 grams versus 80 grams) but is higher for a serving size of fruit intake (150 grams versus 80 grams) (Australian Bureau of Statistics (ABS), 2011; WHO, 2009). On average, the general population in Australia and in Europe fail to meet WHO guidelines, consuming approximately three to four servings of fruit or vegetables daily (Daly et al., 2011; Leenders et al., 2013). Younger age (18–34 years) and male sex have previously been associated with lower consumption of fruit and vegetables (ABS, 2011).
The very few studies investigating fruit and vegetable intake in people with psychosis have been conducted in Italy and Spain where approximately two to three servings of fruit and vegetables were being consumed daily (Fusar-Poli et al., 2009; Simonelli-Munoz et al., 2012). Research suggests that predictors of an inadequate diet may be different in people with psychosis compared to the general population. Psychosis-specific factors such as the effects of antipsychotic drugs (weight gain and increased fatigue) (Nasrallah, 2003), negative symptoms and depression may contribute to poor diet and its relationship to obesity, suggesting that programs designed to improve dietary practices may not apply to those with psychosis. However, lower socio-economic status (lower education, lower income and unemployment) and substance use create potential barriers towards healthy eating in people with psychosis (Hahn et al., 2014) and in the general community (Barosh et al., 2014). People with psychosis who are current smokers consume fewer portions of fruit and vegetables weekly compared to non-smokers with psychosis (McCreadie, 2003). Similarly, smokers in the general population are more likely to drink alcohol, be physically inactive and eat less than five servings of fruit and vegetables daily compared to non-smokers (Strine et al., 2005).
Low fruit and vegetable intake in people with psychosis has previously been shown to be associated with male sex (Roick et al., 2007) and higher body mass index (BMI) (Smith et al., 2007). Unlike the general population, where increased fruit and vegetable consumption is linked to a lower risk of depression (McMartin et al., 2013), McCreadie (2003) reported no differences in depression or positive and negative symptoms in association with fruit and vegetable intake in people with schizophrenia.
Prior research has been limited to small sample sizes (n=72–194), conducted in other counties, and limited to schizophrenia diagnoses; thus, a broader analysis of dietary behaviour in people with psychosis living in Australia is warranted. To our knowledge, this is the first study to examine health outcomes, substance use, symptom severity and financial difficulty in relation to fruit and vegetable intake. Thus, based on prior research, the aims of this study were: (1) to explore the prevalence of an inadequate diet; (2) to explore univariate predictors that may be related to dietary inadequacy; and (3) to examine multivariate predictors of diet inadequacy adjusting for age, sex, BMI, education, marital status and employment.
Methods
Study design and participants
Participants in the study took part in the 2010 second Australian national survey of people living with psychotic illness. A detailed description of the method has been published elsewhere (Morgan et al., 2012, 2014). The study consisted of a two-phase sampling design. In phase 1, people aged 18–64 years and in contact with public mental health services and non-government organisations funded to support people with mental illness in the previous 12 months were screened for psychosis. People who screened positive for psychosis in phase 1 (n=7955) were randomly selected during phase 2 for interview and assessment, resulting in 1825 interviews. Of these, 1286 participants provided fasting blood samples (fasted overnight of a minimum of 8 hours) to provide bio-medical data. Diagnosis according to the International Classification of Diseases, 10th Revision (ICD-10) (WHO, 1992) was determined using the Diagnostic Interview for Psychosis (DIP) (Castle et al., 2006). The study was approved by institutional human research ethics committees at each of the seven study sites. Written informed consent was provided by all participants.
Measures
Demographic factors included participants’ sex, age, marital status (single/never married, married/de facto, separated/divorced, widowed), employment status, highest level of education obtained (did not complete high school, completed high school, trade qualification, postgraduate qualification) and migrant status (migrated to Australia, native born). Socio-economic indexes for areas (SEIFA) were obtained using a mean decile score, ranging from 1 to 10 (1 reflecting the lowest scoring 10% of areas, i.e. most disadvantaged). The main source of income was also assessed.
The survey consisted of a semi-structured interview where food intake and difficulty purchasing food was assessed, based on items from the 2001 Australian Health Survey (ABS, 2001), the 1995 National Nutrition Survey (ABS, 1995) and the 2007 second National Survey of Mental Health and Wellbeing (Slade et al., 2009). Participants were asked: ‘in the last 4 weeks how many serves of vegetables do you usually eat each day including fresh, frozen and tinned vegetables?’ (1 serve = ½ cup of cooked vegetables or 1 cup of salad vegetables = 75 grams). The same question was repeated for fruit intake (1 serve = 1 medium piece or 2 small pieces of fruit or 1 cup of diced pieces = 150 grams). The average serving size for fruit or vegetables according to WHO (2009) corresponds to 80 grams. For the purpose of this study, consuming less than four daily servings of fruit or vegetables (or a combination of both) was defined as failing to meet WHO dietary guidelines, as this was the closest estimate we could achieve in the current study.
Participants were asked about the type of milk they had consumed in the last 4 weeks (whole milk, low fat/skim/soy, other) and whether they had added salt to their food after it was cooked in the last 4 weeks (never/rarely, sometimes, usually). Further items included the number of times they ate during the day in the past 4 weeks (including snacks), how many days during the week they ate breakfast and whether they had gone without meals due to a shortage of money (last 12 months) or if they had run out of food and could not afford to buy more (last 12 months).
Metabolic syndrome was determined using the harmonised criteria (Alberti et al., 2009). The methods for the assessment of metabolic syndrome have been reported elsewhere (Galletly et al., 2012). Physical activity was determined using the International Physical Activity Questionnaire (short form) (Craig et al., 2003). The total time spent in various activities over the previous 7 days was classified according to criteria from the National Survey of Mental Health and Wellbeing (ABS, 2008), which consisted of four levels of activity: very low, low, moderate and high. Sedentary behaviour was measured in hours per day (Craig et al., 2003).
Participants were classified as current smokers if they had smoked tobacco in the previous 4 weeks. The Alcohol Use Disorders Identification Test (AUDIT) (Saunders et al., 1993) was used to measure risk and alcohol dependence, which consisted of four categories: low risk – consuming less than four standard drinks per day; hazardous drinking; harmful drinking; dependent drinking. Respondents were asked if they had used cannabis or amphetamines in the past year.
The presence of negative symptoms in the previous 12 months was assessed, which included a person’s interest in leisure activities, overall socialising, diminished emotional range, restricted affect, poverty of speech and diminished sense of purpose. This was derived from the World Health Organization Schedules for Clinical Assessment in Neuropsychiatry (WHO, 1999). Binary responses were summed to produce a score ranging between 6 and 0, with a higher score reflecting increased symptom severity.
Statistical analyses
Analyses were performed using SPSS (version 19; IBM Corp., 2010). To explore the differences between respondents who met or did not meet dietary guidelines for fruit and vegetable intake, independent t-tests or Mann–Whitney U-tests were used for continuous variables and chi-squared tests or Fisher’s exact test for categorical variables. A binary logistic regression analysis was conducted to explore potential predictors of dietary behaviour. Variables were divided into four categories (substance use, physical activity, symptom severity and financial difficulty). These variables were entered into the model to estimate multivariate associations, with and without adjusting for age, sex, BMI, marital status and employment (because poorer nutritional intake is usually associated with younger age, male sex, obesity, single marital status and unemployment; Dibsdall et al., 2003; Drewnowski, 2009) and, in our cohort, the age range varied between 18 and 64 years and there was an unequal male:female ratio.
Results
The mean age of participants was 39 years. They were most commonly diagnosed with schizophrenia or schizoaffective disorder (62%), were single or never married, unemployed, left high school without obtaining a leaving certificate, or completed a trade qualification (Table 1). Approximately 74% of participants failed to meet WHO dietary guidelines. Failure to meet the guidelines was associated with lower rates of obesity, lower levels of physical activity, and sedentary behaviour (Table 2). They were more likely to smoke tobacco, drink alcohol and use cannabis and amphetamines. They had a higher negative syndrome score but no differences were found for depressive symptoms (Table 2).
Demographic characteristics of total participants and clinical characteristics of participants.
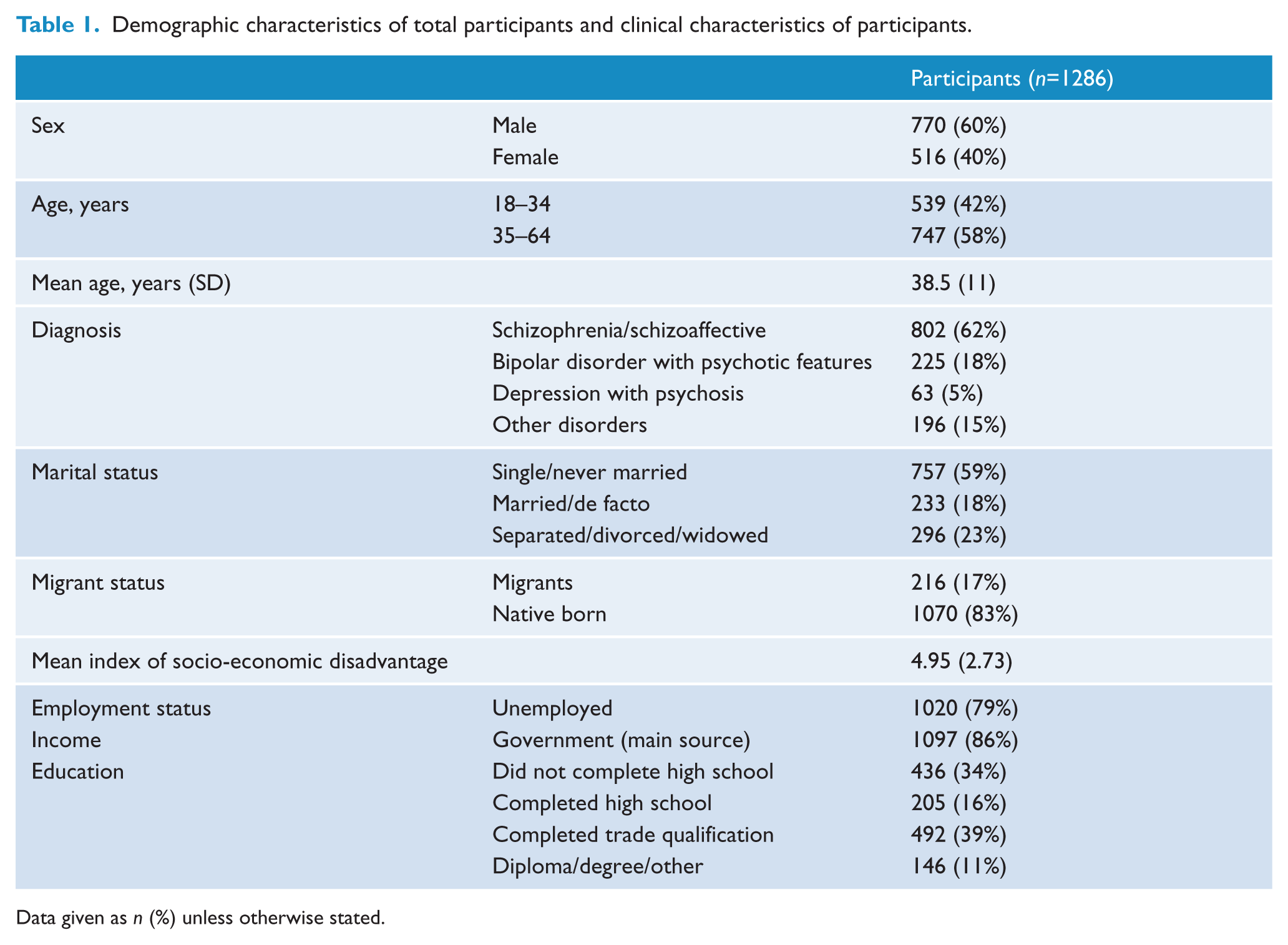
Data given as n (%) unless otherwise stated.
Association between adequacy of fruit and vegetable intake and cardiometabolic indices, BMI, physical activity, substance use and symptoms.
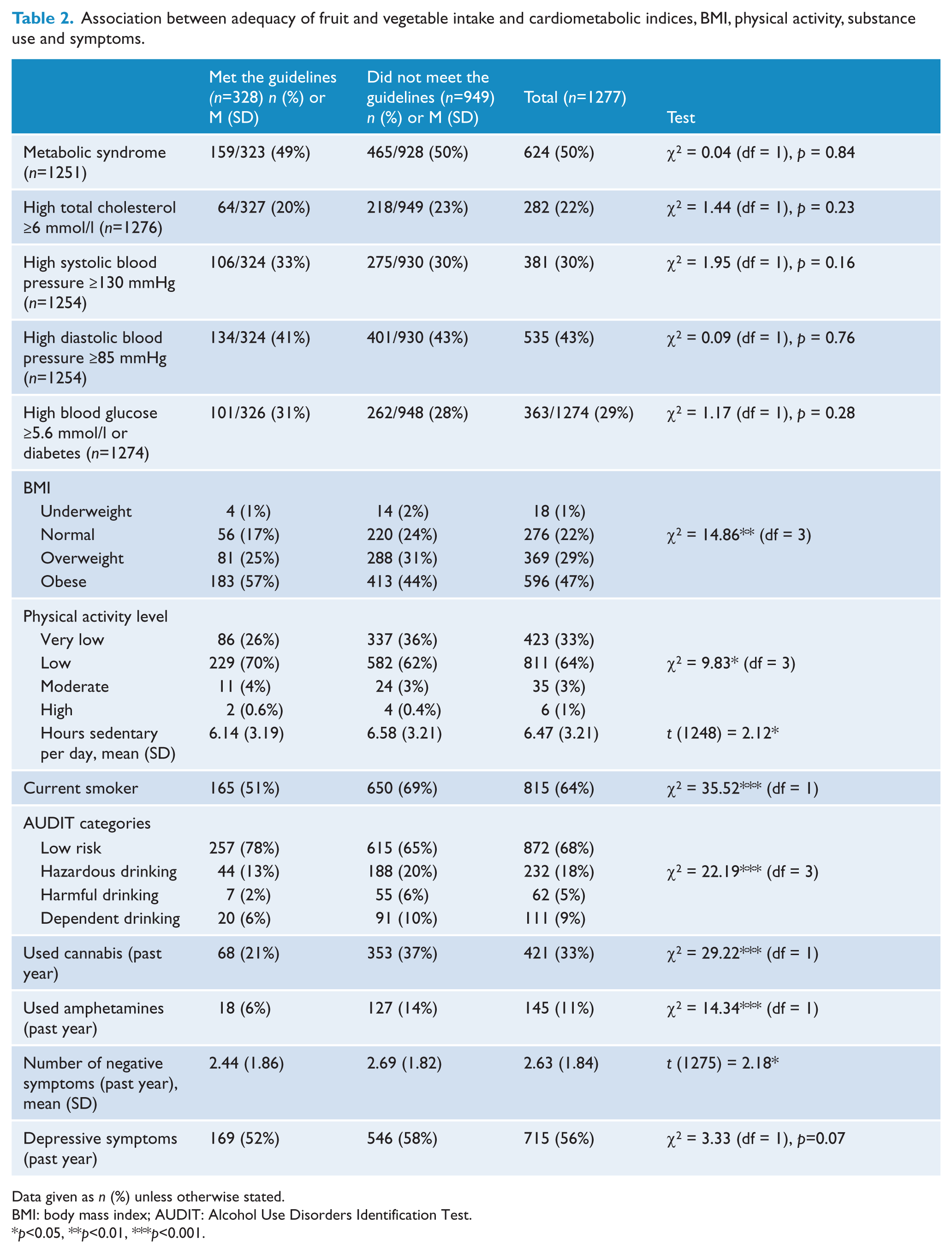
Data given as n (%) unless otherwise stated.
BMI: body mass index; AUDIT: Alcohol Use Disorders Identification Test.
p<0.05, **p<0.01, ***p<0.001.
After disaggregating the sample by sex, age, BMI and dietary behaviour (Table 3), we found that men were less likely to eat sufficient fruit and vegetables daily compared to women and were more inclined to drink whole fat milk rather than low fat milk, and more likely to add salt to their food. Participants aged 18–34 years were less likely to eat sufficient daily servings of fruit or to eat breakfast during the week and were more inclined to add salt to their food compared to people aged 35–64 years. Those participants with a BMI >25 consumed more daily servings of fruit, ate more meals (including snacks) and ate breakfast on more days of the week in comparison to people with a lower BMI; however, they were more likely to drink low fat milk opposed to whole milk. Factors associated with failure to meet dietary guidelines included financial difficulty, running out of food and not being able to buy more, eating meals (including snacks) less frequently during the day and eating breakfast less often during the week. Those not meeting dietary guidelines were also more likely to drink whole milk instead of low fat milk and to add salt to their food.
Food consumption by sex, age and BMI; nutrient intake and financial difficulty by adequacy of fruit and vegetable intake.
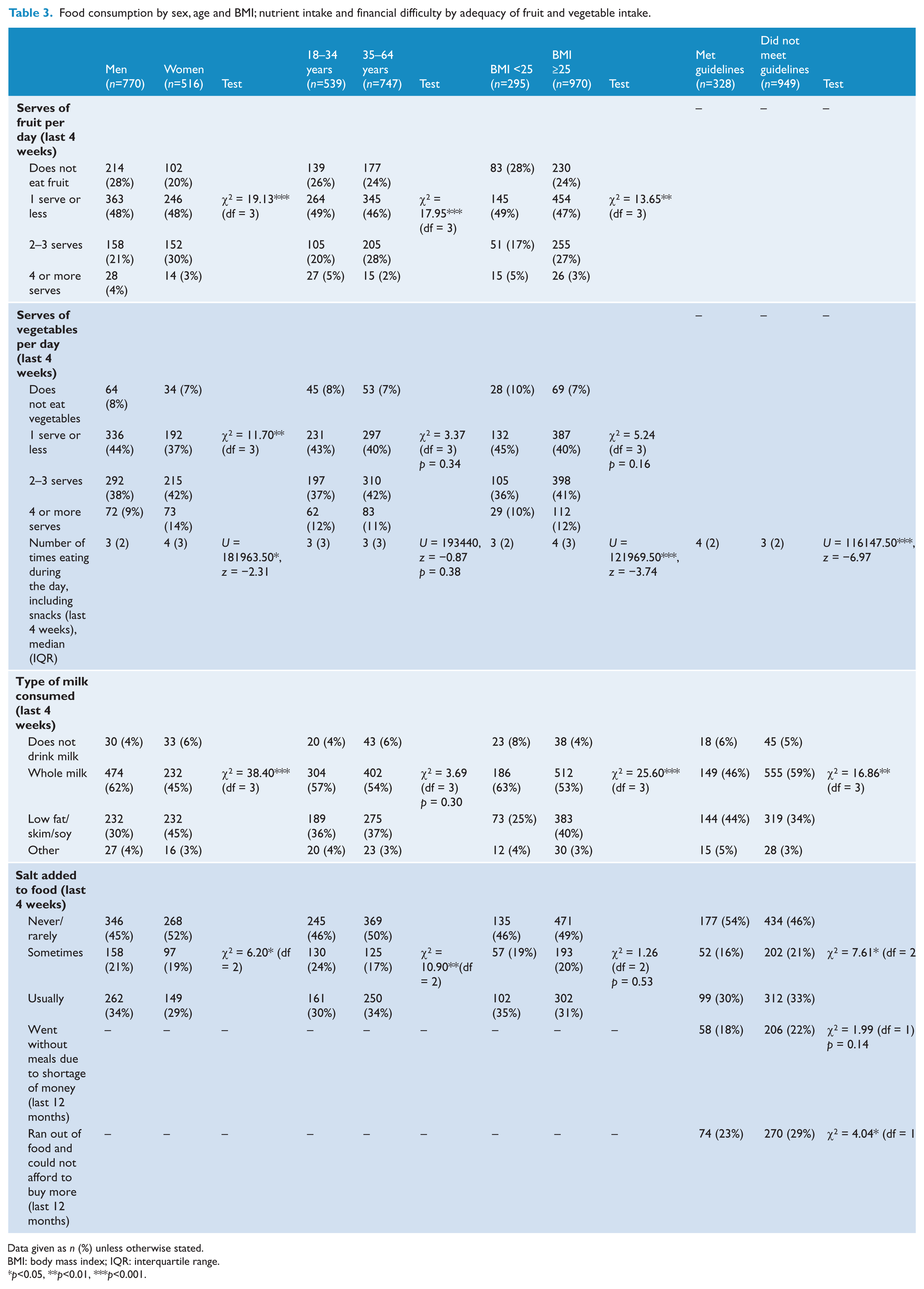
Data given as n (%) unless otherwise stated.
BMI: body mass index; IQR: interquartile range.
p<0.05, **p<0.01, ***p<0.001.
The logistic regression analysis (table 4) showed that people who were current smokers, at risk of hazardous, harmful or dependent drinking and who used cannabis in the past year were less likely to meet WHO dietary guidelines. Alcohol risk had the greatest impact (OR 3.05, 95% CI: 1.61–5.8) followed by current smoking (OR 2.05, 95% CI: 1.50–2.80) and cannabis use (OR 1.51, 95% CI: 1.05–2.16) . However, when the model was adjusted for sex, age, BMI, education, marital status and employment, only current smoking remained significant.
Unadjusted and adjusted odd ratios and confidence intervals of not eating adequate amounts of fruit and vegetables in people with psychosis.
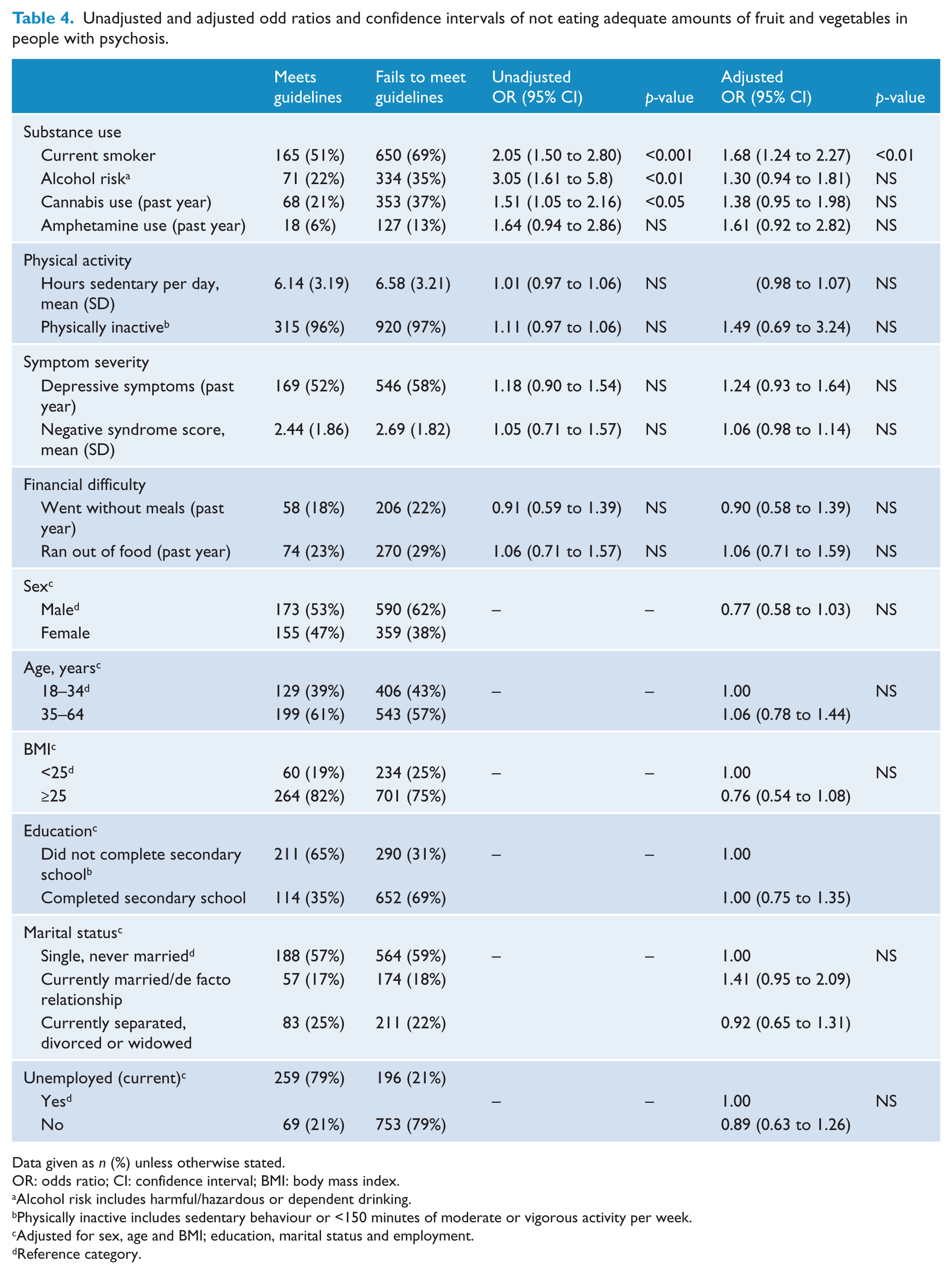
Data given as n (%) unless otherwise stated.
OR: odds ratio; CI: confidence interval; BMI: body mass index.
Alcohol risk includes harmful/hazardous or dependent drinking.
Physically inactive includes sedentary behaviour or <150 minutes of moderate or vigorous activity per week.
Adjusted for sex, age and BMI; education, marital status and employment.
Reference category.
Discussion
This national study revealed that 74% of people with psychosis did not eat adequate amounts fruit and vegetables. Simonelli-Munoz and colleagues (2012) found that in a sample of people with schizophrenia living in Spain, 91% consumed less than four servings of fruit or vegetables daily. This suggests that Australians with psychosis are, perhaps, doing better in terms of nutritional intake.
Accurate dietary comparisons based on meeting dietary guidelines were difficult to achieve between the current sample and the general population. However, if we view fruit and vegetable intake separately, a higher proportion of adults in the current study did not eat fruit (25%) or vegetables (8%) compared to Australian adults in the general population (6% and 0.8%), respectively (ABS, 2011). People in the present study were less likely to consume four or more servings of fruit compared to the Australian population (3% versus 6%) and were less inclined to consume four or more servings of vegetables than the general population (11% versus 20%) (ABS, 2011). According to Australian dietary guidelines, only 5.6% of adults in the general population meet the recommendations for fruit and vegetable intake (2 serves of fruit and 5 serves of vegetables daily), which is slightly lower than Australian adults with psychosis (6.2%) (Foley et al., 2014). This suggests that people with severe mental illness and people in the general population both have an inadequate intake of fruit and vegetables, increasing the risk of elevated blood pressure and cholesterol (Obarzanek et al., 2001).
The results of the current were mostly congruent with our hypotheses. An important finding was the higher rates of substance use (alcohol, tobacco, cannabis and amphetamines) among people who did not meet dietary requirements. This is consistent with past research (Strine et al., 2005) and may in part be explained by appetite suppressant effects that certain substances can have on the body (Jessen et al., 2005). People who followed nutritional guidelines had fewer negative symptoms, suggesting that functioning individuals with psychosis may be making dietary choices. Symptoms including avolition may also contribute to poorer eating patterns and, in addition, foods lacking nutritional value may have an effect on symptom severity (Stokes and Peet, 2004).
In the general population there is a negative correlation between nutritional intake and depression (McMartin et al., 2013), but this was not observed in the present study. Participants in the current study who ate less than four servings of fruit and vegetables per day were more sedentary and were less likely to exercise. The majority of the current sample were unemployed, did not complete high school or obtained a trade certificate. Research shows that lower educational attainment is associated with poor health behaviours in psychosis (Roick et al., 2007) and in the general population (Lee and Cubbin, 2002), but we did not find any association between education and diet. However, usually, better education is associated with a higher income, whereas most of our sample received government benefits. From the current study, we already know that people who failed to meet the fruit and vegetable intake guidelines were more likely to use substances; therefore, this may explain why people who did not meet the guidelines also reported that they ran out of food and were unable to purchase more. Supporting nicotine addiction is costly, especially among people with schizophrenia who spend the majority of their income on tobacco products (Steinberg et al., 2004). This may support why people in this study who failed to meet the nutritional requirements also ate less frequently during the day. Although people who met the guidelines had a tendency to eat more often, they remained conscious of lowering their intake of whole milk and salt.
Men consumed fewer servings of fruit and vegetables compared to women, supporting prior research (McCreadie, 2003) and this may be explained by the higher prevalence of co-morbid drug use including tobacco (Johnson et al., 2010), cannabis (Koskinen et al., 2010) and alcohol (Cruce et al., 2007) among men. Compared to men, women were more likely to eat more during the day, drink less whole milk and refrain from adding salt to their food. This discrepancy may be reflected in women being more conscious of their body image and having a stronger desire for behaviour change (Strassnig et al., 2005). We found that people aged 18–34 years were less likely to eat two to three servings of fruit (20% versus 28%), were less likely to eat breakfast during the week, but were more likely to add salt to food compared to people aged 35–64 years. People of younger age in the general population tend to eat foods high in fat and sugar, this then gradually improves with age (Peet, 2004) and we may be observing a similar trend in the current study.
People who had a BMI greater than 25 were more likely to meet dietary guidelines for fruit and vegetable intake. This finding may appear counter-intuitive as people who have a healthier diet generally have a lower risk of obesity (Simonelli-Munoz et al., 2012) but people who have a healthier diet also have lower rates of substance use. Previously, a greater BMI has been linked with poorer consumption of nutritious foods (Smith et al., 2007); therefore, the hypothesis that failure to meet dietary guidelines will be associated with higher BMI was not supported in this current study. People who had a greater BMI were more likely to eat extra meals during the day (including snacks) and eat breakfast on more days during the week. Taken together, this suggests that people who have a higher BMI may have an increased nutritional intake as they are eating more foods, though we were unable to measure the overall dietary intake, including energy (caloric intake). People with a higher BMI were more health conscious of the type of milk they consumed, choosing low fat milk as opposed to whole milk, compared to people with a BMI <25. However, this needs to be considered carefully, as while people with a greater BMI are eating more nutritious foods, they remain at greater risk of cardiovascular disease and other health complications. A total of 47% of adults in this study were obese and 50% had metabolic syndrome, which is much higher than the rates of obesity and metabolic syndrome in the Australian population (28% and 13–31%, respectively) (ABS, 2011; Cameron et al., 2007).
Of particular interest were the results from the regression analysis as being a current smoker and using cannabis and alcohol predicted failure to meet WHO dietary guidelines. Similarly, people in the general population are less likely to eat nutritious foods if they are a smoker and drink alcohol (Strine et al., 2005). Alcohol and cannabis use no longer remained significant after adjusting for sex, age, BMI, education, employment and marital status, but current smoking still retained its significance. This illustrates the importance of substances, in particular nicotine, and poorer socio-economic status in determining dietary behaviour. Drug use can cause changes in appetite (Jessen et al., 2005), which may explain this finding.
There are several limitations to this study. First, this study relied on self-reports; thus, questions relating to the frequency of food intake were retrospective, which may decrease the reliability of responses. WHO dietary guidelines state that eating less than five servings of fruit and vegetables per day is the threshold for failing to meet nutritional requirements, but only an intake of less than four servings of fruit and vegetables could be estimated in the current study. Questions relating to fruit intake also included any consumption of tinned fruit, which can contain high amounts of sugar. This may explain the increased BMI among people who met the dietary recommendations in the current study. While this study formed part of a large national cohort of 1825 participants, we only included people who provided fasting blood samples, resulting in a total of 1286 respondents. Previous studies have been limited by small sample sizes, people diagnosed with schizophrenia and the use of different dietary measures, thus limiting the reliability of comparisons.
Overall, this study showed that people with psychosis are falling well below dietary recommendations. Substances including alcohol, cannabis and, in particular, tobacco appear to be important factors that may be deterring healthy eating. In addition to addressing drug use and targeting physical activity, intervention programs may need to promote more education regarding financial budgeting and ways of accessing healthy foods so people with psychosis can meet the daily nutritional requirements for fruit and vegetable intake.
Footnotes
Acknowledgements
This paper is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V Morgan (National Project Director), A Jablensky (Chief Scientific Advisor), A Waterreus (National Project Coordinator), R Bush, V Carr, D Castle, M Cohen, C Galletly, C Harvey, B Hocking, A Mackinnon, P McGorry, J McGrath, A Neil, S Saw and H Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The authors acknowledge, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.