
Abstract
Objective:
To investigate the ambulatory mental health service profile of persons with intellectual disability (ID) in a representative sample of New South Wales (NSW).
Methods:
A statistical linkage key was used to link the Disability Services Minimum Data Set (DS-MDS) and a community mental health services dataset (MH-COM) for a representative area of NSW for the period 2005–2010. Linkage was undertaken in four NSW local health districts (LHDs), covering 36.7% of the NSW population. The mental health profiles and service use characteristics of people with an ID were compared to mental health service users without an ID.
Results:
Of the 89,262 people in the MH-COM over this 6-year period, 1,459 people (1.6 %) were identified as having an ID. Compared to those without an ID, people with an ID were more likely to have psychotic disorders, developmental disorders and personality disorders, and more than twice as likely to have an ‘unknown’ diagnosis. Compared to those without an ID, people with an ID were less likely to have depressive disorders, adjustment disorders and other disorders. Service use profiles revealed that people with an ID had 1.6 times more face-to-face contacts, and a total face-to-face contact time which was 2.5 times longer than people without an ID.
Conclusions:
Ambulatory mental health data from NSW indicates that people with an ID receive care for a distinct range of mental disorders, and experience uncertainty regarding their diagnosis. People with an ID have higher service needs which require recognition and the allocation of specific resources. Such data provide a suitable baseline for future evaluation of the impact of ambulatory mental health reforms for people with an ID.
Keywords
Introduction
People with an intellectual disability (ID) are a minority group in Australia, accounting for approximately 400,000, or 1.8% of the population (Australian Institute of Health and Welfare (AIHW), 2003) and 2.2% of the NSW population (AIHW, 2008). The majority of these individuals (57%) have a psychiatric disability or mental disorder (Australian Bureau of Statistics, 2009). Compared to the general population, people with an ID experience elevated rates of common mental disorders which are approximately two to three times those experienced by the general population (Cooper et al., 2007; Einfeld et al., 2006, 2011; Emerson, 2007; Smiley et al., 2007). Predisposition to mental ill-health is apparent across the lifespan of people with an ID, including in children, younger people, adults (Einfeld et al., 2006) and older adults. Schizophrenia appears to be over-represented by two to four times and has an earlier onset in people with an ID (Borthwick-Duffy, 1994; Morgan et al., 2008). Over-representation has also been noted for common mental disorders such as affective disorders, anxiety disorders and the dementias (Cooper, 1997; Cooper et al., 2007; Strydom et al., 2007, 2009). This vulnerability to mental illness highlights the importance of timely access to psychiatry services for this group (Borthwick-Duffy, 1994; Emerson, 2003).
Vulnerability to mental disorders in people with an ID is underpinned by a variety of biological, psychological and social factors. For example, specific genetic conditions associated with ID can increase the risk of psychopathology (Cooper et al., 2007), as can developmental brain abnormalities and pharmacological treatments and their side effects (Tonge and Einfeld, 2000). People with an ID are also at increased risk of a range of physical health conditions (O’Hara et al., 2008; Scheepers et al., 2005; Wallace and Beange, 2008), a factor which increases the risk for mental ill-health.
Despite the over-representation of mental disorders in people with an ID, access to mental health services for this population is limited and falls far short of that for the general population. Australian research following a cohort of children and adolescents with ID for 14 years demonstrated that just 10% of those with a mental disorder received an intervention (Einfeld et al., 2006). This compares unfavourably with access to mental health supports for the general population, which has been estimated to be about 34.9% over a 1-year period (Slade et al., 2009). Access to mental health services for this group is influenced by a number of factors. These include: the difficulty a person with an ID may have in seeking mental health care; lack of knowledge, training and confidence of mental health professionals (Edwards et al., 2007; Jess et al., 2008; Phillips et al., 2004; Torr et al., 2008); poor understanding by carers and disability and mental health workers of the manifestations of mental disorders in people with an ID (Costello et al., 2007; Moss et al., 1997; Patel et al., 1993); and a lack of data on the interaction between, and distinct roles and responsibilities of disability and mental health services (Evans et al., 2012).
Data linkage is increasingly used as a tool to investigate health and mental health service use and outcomes (Holman et al., 1999; Morgan et al., 2000; Williams et al., 2005). It is a relatively cheap and accurate method of determining the epidemiology of mental disorders, profile of service use, and outcomes of specific sub-groups of interest. Presently, Western Australia (WA) is the only Australian jurisdiction to have linked disability and mental health datasets. Established in 1953, the WA Disability Register (now known as the Intellectual Disability Exploring Answers (IDEA) database), (Petterson et al., 2005) has been used for a number of purposes, including to provide accurate prevalence estimates of ID in children (Leonard et al., 2003) and to investigate the causes of ID (O’Leary et al., 2012) and correlates of ID (Leonard et al., 2005). Linkage between IDEA and the WA Mental Health Information System, the general psychiatric case register, has indicated that approximately 32% of people with an ID had a psychiatric comorbidity and 2% in the WA mental health system had an ID (Morgan et al., 2008). This study indicated that, compared to people without an ID, people with an ID had a higher prevalence and earlier onset of schizophrenia (Morgan et al., 2008).
We linked disability services data from the New South Wales Disability Services Minimum Data Set (DS-MDS) with ambulatory mental health services data from a community mental health services dataset (MH-COM) to examine the mental health profile and service use of people with an ID receiving an ambulatory mental health service. We hypothesised that people with an ID would be under-represented in ambulatory mental health services relative to available data on the prevalence of mental disorders in people with an ID. Further, we predicted that people with an ID being managed within ambulatory mental health services would have service use profiles which reflected the complexity of their condition and its management.
Methods
Datasets and linkage
The DS-MDS is a de-identified dataset which is routinely collected by each Australian State and Territory under the National Disability Agreement. It collates information about the services provided to persons with a disability, and the persons receiving these services. The NSW DS-MDS related to State-funded disability service provision was obtained from the NSW Department of Family & Community Services – Ageing Disability and Home Care (ADHC).
The MH-COM refers to ambulatory mental health data which is collected at the local health district (LHD) level within the NSW Mental Health Outcomes and Treatment (MHOAT) data collection system and fed into the local Health Information Exchange (HIE) system. It contains information about community mental health contacts and the patients making those contacts.
The MH-COM was provided to the research team from extractions at the local HIE level. The MH-COM represented data from the ethnically and economically diverse catchment areas of South Western Sydney, Sydney, Illawarra Shoalhaven and South Eastern Sydney LHDs.
Pre-processing was performed prior to linkage to remove those records in either dataset with missing components in the date of birth (DOB) field and those records with dubious DOB as determined by a calculated age of either <0 or >100 using a record’s DOB and a census date of 01/01/2008 (the mid-point of the study period). This resulted in the removal of 59 records from the DS-MDS and 126 records from the MH-COM as there was no way of verifying these dates.
The DS-MDS was linked to the MH-COM for the period 2005–2010. The sample area of NSW covered by the study had a total population of 2.64 million, or approximately 36.7% of the State of NSW at the time of the 2011 census. Deterministic linkage was performed using the SLK581 Statistical Linkage Key devised by the AIHW (Karmel, 2005). The SLK581 is constructed using: the 2nd, 3rd and 5th letters of the surname, the 2nd and 3rd letters of the given name, the date of birth as a character string of the form ddmmyyyy, followed by the character ‘1’ for male or ‘2’ for female. Non-alphabetic letters in names are excluded (e.g. hyphens and apostrophes), and where a name contains insufficient letters, the character ‘2’ is used as a place-marker for absent key letters. The character ‘9’ is used for any other missing data so that the linkage key always has a length of 14 characters. The SLK581 has a linkage rate of 99.8% (Karmel, 2005), maintains the integrity and privacy of the data and provides the links in a de-identified format. The SLK581 was generated onsite by local staff for each of the sites in which the MH-COM data were held for the four LHDs, and the data were extracted using an in-house algorithm which collected the required target variables.
Access to data was granted by both the data custodians at ADHC and at the Mental Health and Drug and Alcohol Office (MHDAO), NSW Ministry of Health, as well as Directors of Mental Health (and Drug and Alcohol) for the four LHDs. Ethics approval was granted from The University of New South Wales Medical and Human Research Ethics Advisory Panel (HREA) (reference number: 2011-7-18) and from the Human Research Ethics Committee (HREC) – Northern Sector (reference number: 11/165 (LNR/11/POWH/271)) representing the four LHDs. Site Specific Approvals (SSAs) were also obtained from each of South Western Sydney, Sydney, Illawarra Shoalhaven and South Eastern Sydney LHDs. Participant consent was not required as the study involved the linkage of de-identified data and researchers at no point had access to identifying information.
Ascertainment of ID and mental disorders
The MH-COM recorded community-based mental health services delivered to 89,262 people. The DS-MDS recorded 34,432 people for whom ID was coded as a primary or secondary disability. Individuals with ID within this dataset meet strict eligibility criteria which includes: intellectual functioning measured at two or more standard deviations below the mean for the full-scale score on a recognised test of intelligence; significant deficits in adaptive functioning in two or more areas, as defined by performance on domains or factors of recognised tests of adaptive functioning which is two or more standard deviations below the mean; and evidence that the deficits in cognitive and adaptive functioning are manifest prior to 18 years of age (ADHC, 2002).
Of the 34,432 people with ID in the DS-MDS, 1,159 people were also in the MH-COM. A further 300 people in the MH-COM were identified as having ID as they had an International Classification of Diseases 10 (ICD-10) (WHO, 2010) code in the range F70–79 (Mental Retardation). Therefore, a total of 1,459 individuals with ID were identified within the MH-COM. The comparison group were people without linked records and without an ICD-10 coding in the F70–79 range in the MH-COM (87,803 people).
We specified 10 mental disorder diagnostic categories of interest for this study, subsuming related individual ICD-10 diagnoses into overarching categories as described in Table 1. For each individual, each ICD-10 diagnosis recorded over the 6-year study period was assigned a binary flag, which was mapped onto the overarching diagnostic category. An ‘unknown’ diagnosis was also assigned where this was represented in the data. The prevalence of each diagnostic category was then calculated for those with an ID and those without an ID. The number and duration of direct ‘face-to-face contacts’ for each MH-COM client were then aggregated for each individual with ID and without an ID over the 6-year period.
Diagnostic categories from the MH-COM dataset.
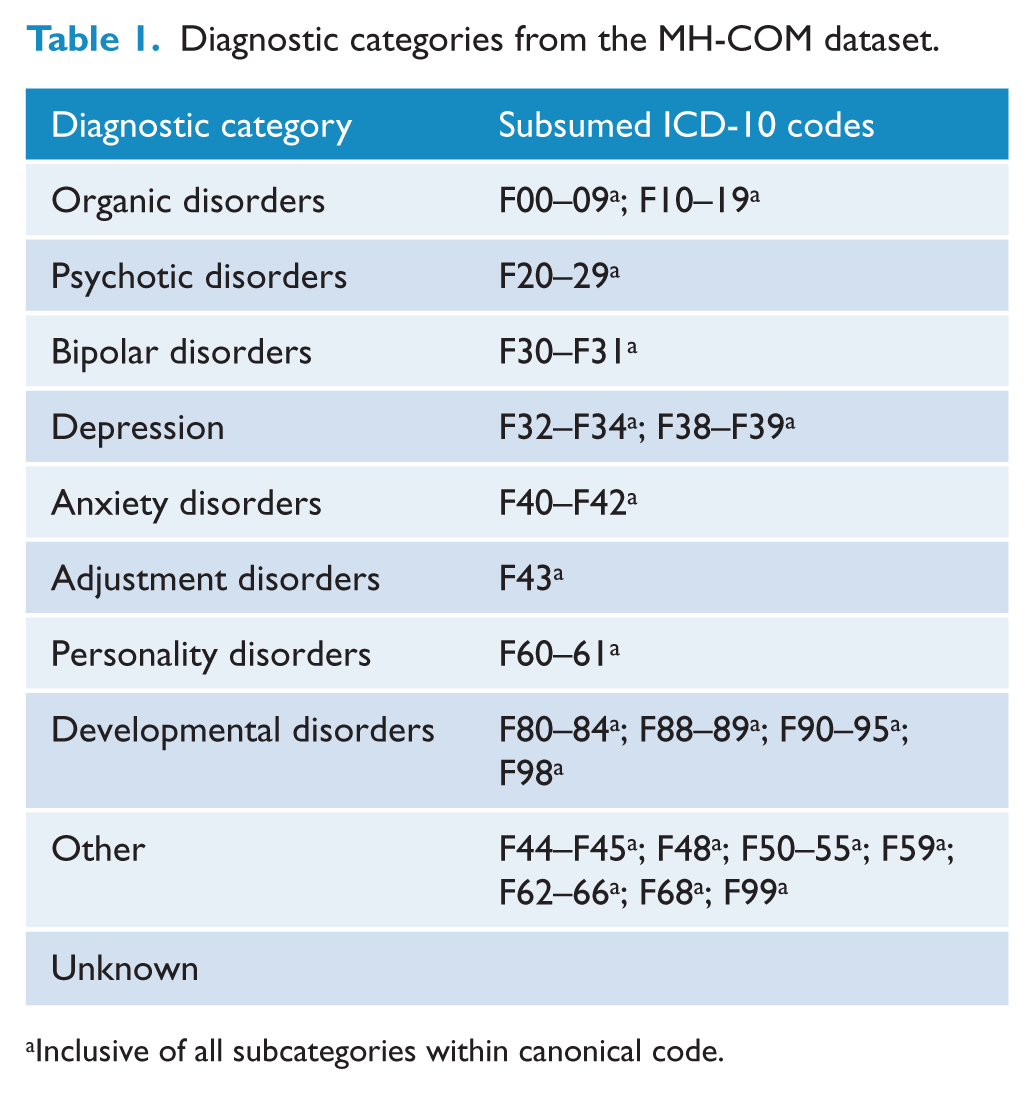
Inclusive of all subcategories within canonical code.
Statistical analyses
After excluding records with missing data for specific variables of interest, mean age differences for those with and without an ID were determined using a two-tailed Student’s t-test. Pearson’s chi-squared test of independence was performed to determine group differences in age distribution, sex and indigenous status. Logistic regressions were used to calculate the adjusted odds ratios (ORs) and examine the association between diagnostic categories (criterion variable) and demographic factors including age, sex and presence of an ID (independent variables). Natural logarithmic transformation was performed on both the number and duration of face-to-face contacts as the data were skewed. A one-tailed Student’s t-test was performed on the transformed data to determine differences in service usage between groups.
Results
There were a total of 1,318,083 direct contacts for 89,262 individuals in the MH-COM over the 6-year study period. Of these, 36,806 direct clinical contacts occurred in relation to the 1,459 people with an ID, while 1,281,277 direct clinical contacts occurred in relation to the 87,803 people without an ID. People with an ID represented 1.6% of the total study population. The demographic characteristics of people with and without an ID are shown in Table 2. People with an ID were on average 10 years younger than those without an ID (mean age of people with an ID = 28.1 (SD 15.5) years; people without an ID = 38.3 (SD 20.4) years; t(1,544) = −24.8, p<0.001). The age distribution differed between those with and without an ID (χ2 = 425.4, df = 5, p<0.001). Post-hoc standardised residual analysis showed that compared to people without an ID, there was an over-representation of people with an ID in the 5- and 24-year age range and an under-representation of those aged 65 years or more. The male to female (M:F) ratio differed between groups (χ2 = 6.7, df = 1, p=0.010). There was a predominance of males in the group with ID (57%) but a minority of males amongst those without an ID (46%). There was no significant relationship between the presence of ID and Aboriginal or Torres Strait Islander status (χ2 = 1.3, df=1, p=0.249).
Demographic profile of ambulatory mental health service users with and without an ID.
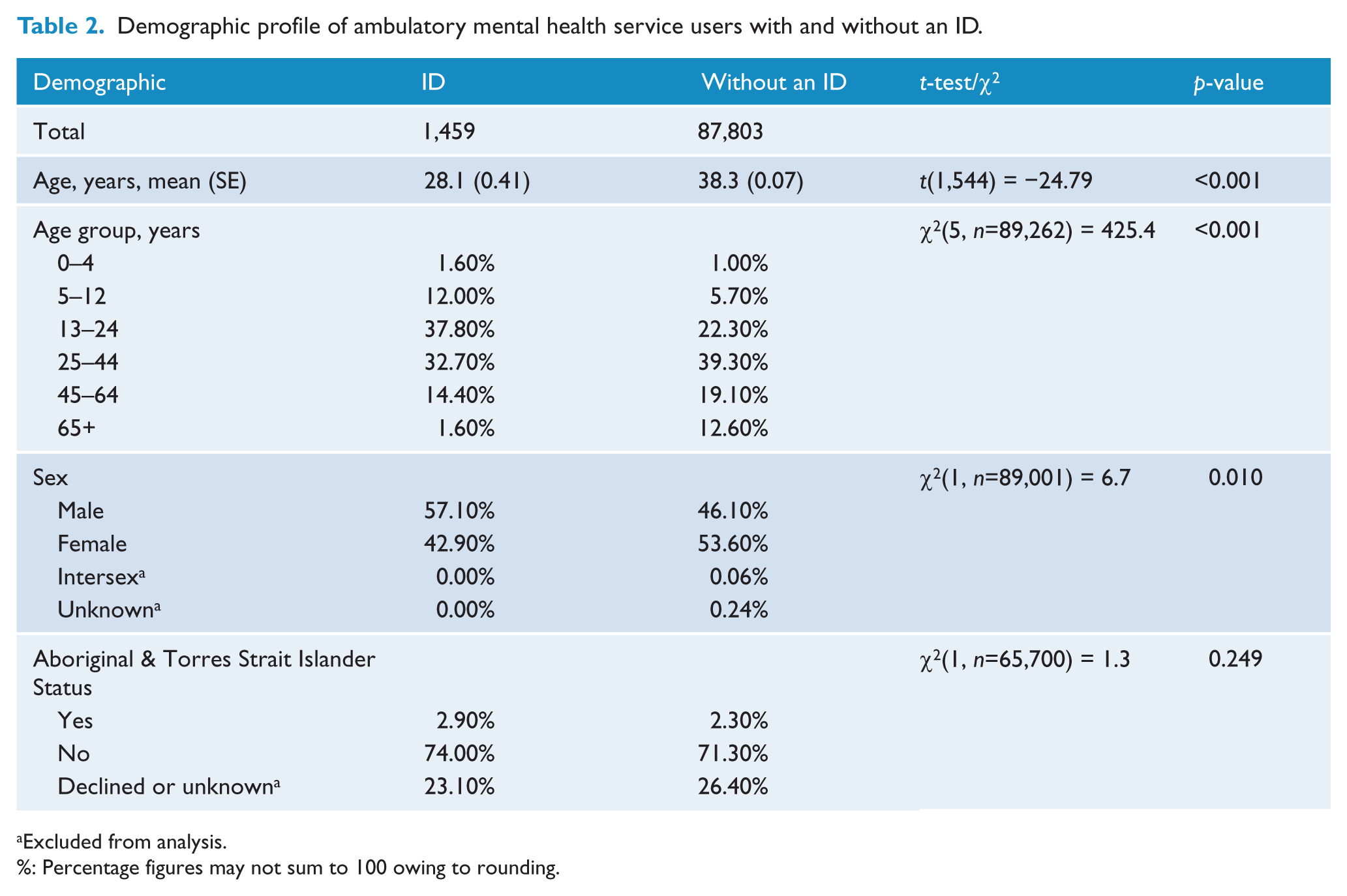
Excluded from analysis.
%: Percentage figures may not sum to 100 owing to rounding.
Marked differences in the distribution of diagnostic categories were apparent between ambulatory mental health service users with and without an ID (χ2 = 110,624, df=9, p<0.001) (Table 3). After analyses were adjusted for age and sex, compared to people without an ID, people with an ID were more likely to have psychotic disorders (OR 2.23, 95% CI 1.97, 2.51; p-value <0.001) and less likely to have depressive disorders (OR 0.71, 95% CI 0.59, 0.84; p-value <0.001), adjustment disorders (OR 0.76, 95% CI 0.60, 0.94; p-value = 0.010) and other disorders (OR 0.85, 95% CI 0.76, 0.96; p-value = 0.007). Unsurprisingly, people with an ID were more likely than those without an ID to have developmental disorders (OR 1.83, 95% CI 1.43, 2.32; p-value <0.001). People with an ID were also more likely to have personality disorders (OR 1.59, 95% CI 1.29, 1.94; p-value <0.001) and to be assigned an unknown diagnosis (OR 2.27, 95% CI 1.90, 2.70; p-value <0.001). There was no statistically significant difference between the groups in regard to the diagnostic categories of: organic disorders (OR 0.77, 95% CI 0.85, 1.24; p-value = 0.73), bipolar disorders (OR 1.12, 95% CI 0.86, 1.44; p-value = 0.37) and anxiety disorders (OR 0.80, 95% CI 0.63, 1.00; p-value = 0.06).
Ambulatory mental health diagnostic categories for people with and without an ID.
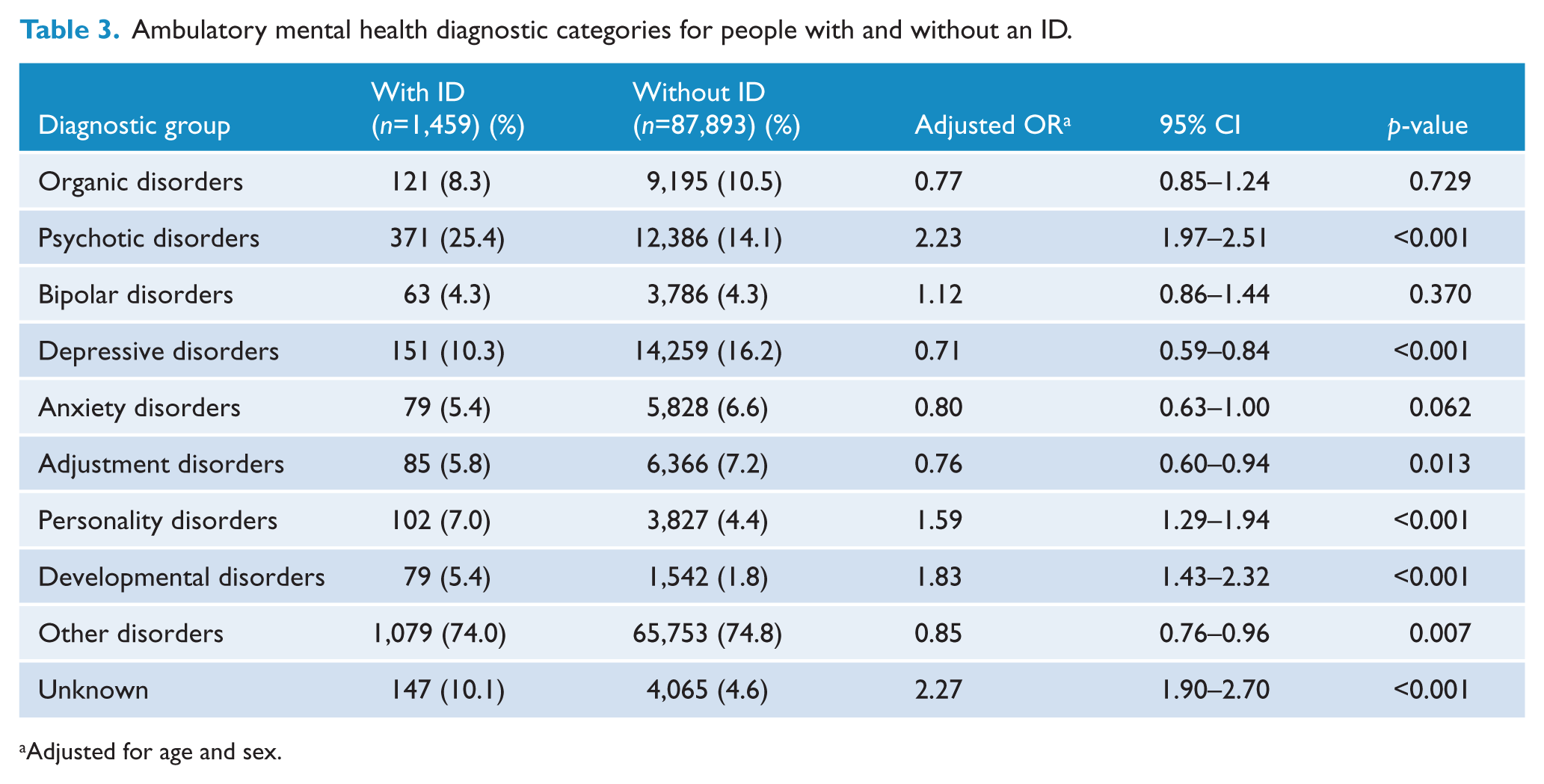
Adjusted for age and sex.
Service use profiles were different for people with and without an ID. Compared to people without an ID, using log-transformed data, people with an ID had 1.6 times as many face-to-face contacts (t(1,498) = 11.8, p-value <0.001) and used a total of 2.5 times more minutes of contact (t(1,510) = 12.6, p-value <0.001).
Discussion
This is the first data linkage study to examine the ambulatory mental health service profile of people with an ID in Australia. The key findings include: relative under-representation of people with an ID, that people with an ID are more likely to receive ambulatory mental health treatment for more severe mental health disorders such as psychosis, and that people with an ID had more service contacts and used more service time than people without an ID – demonstrating that there is an extra level of complexity in the service needs of people with an ID compared to those without an ID.
Only 1.6% of the individuals represented in the sample had an identified ID. Some people with an ID may not be receiving disability-related supports, and hence will be missed by reliance on the DS-MDS alone. Our inclusion of those individuals with ID who were additionally identified as having an ID in the MH-COM is a more inclusive approach. However, there remains a small likelihood that clinical services will not have identified or coded ID as a diagnosis. Nevertheless, the apparent under-representation of ID in the ambulatory mental health dataset is surprising, given that the prevalence of ID in the Australian population is estimated at 1.8% (AIHW, 2003) and that both Australian (AIHW, 2008; Morgan et al., 2008) and international data (Cooper and van der Speck, 2009) indicate a significant over-representation of mental disorders in people with an ID of the order of two to three times that observed in the general population. The relative under-representation of people with an ID in ambulatory mental health settings may reflect difficulty in accessing services. Previous Australian data supports this notion (Einfeld et al., 2006). Alternatively, people with an ID may be accessing alternative pathways to treatment of mental disorders. However, specific health and mental health services for people with an ID are very limited in NSW, making this an unlikely explanation. Despite being untrained and ill-equipped, disability-specific support services are often called on to provide support for mental health-related issues. The existence of this erroneous ‘care’ pathway within disability services could be one possible reason why people with an ID appear under-represented in our data. Ambulatory mental health services provide a vital pathway to treatment and provide post-discharge monitoring and coordination of mental health interventions. The failure to engage such mental health supports for people with an ID risks feeding into a cycle of adverse outcomes and the perpetuation of mental ill-health in this high-needs group.
The age distribution of the ambulatory mental health sample indicated that, compared to people without an ID, there was a lower proportion in the 65 years and over age band for people with an ID (1.6% for people with an ID versus 12.6% for people without an ID). The under-representation of elderly individuals with ID is apparent in national datasets (AIHW, 2008) and could reflect the lower life expectancy of people with an ID. Whether older persons with an ID experience greater difficulty accessing ambulatory mental health services than their younger counterparts is unclear. The highest proportion of people with an ID was observed in the 5–24-year age range, whilst for people without an ID it was in the 25–44-year age range. Assessments for childhood developmental disorders could explain this earlier peak in presentations, as may the existing supports for this age range, such as family and schools. However, there are a number of reasons that may explain under-ascertainment of ID more generally across all age ranges within these data. This may include that people with ID may be using other support services, such as GPs, private psychiatrists or even inpatient mental health admissions, which may provide a buffering effect on ascertainment rates broadly.
Our data indicate that the majority of those with ID receiving an ambulatory mental health service were male (57.1%), while males were a minority (46.1%) for those without an ID. The higher prevalence of ID in males (AIHW, 2008) may contribute to this finding, although some research on prevalence of mental illness in people with an ID has suggested a predominance of mental ill-health in females (Cooper et al., 2007). The representation of males in the MH-COM could also be affected by the help-seeking behaviour of persons with an ID or their carers. The latter could be influenced by the heightened risk encountered in males, including challenging behaviour (Borthwick-Duffy, 1994; Emerson et al., 2001).
Our finding of the over-representation of psychotic disorders in people with an ID is expected and supports previous findings of a vulnerability to psychosis in people with an ID (Morgan et al., 2008; Zammit et al., 2004). The under-representation of more common diagnostic categories (such as depressive disorders and adjustment disorders) within the ambulatory mental health dataset suggests either under-recognition of these mental disorders or a problem of access. As in the general community, psychotic disorders in people with an ID often require the most intensive support. The larger proportion of people with an ID within the psychosis category, together with an under-representation of other common mental disorders, suggests a ‘high pass’ filter effect in which only the most pressing problems are addressed in this group.
People with an ID were more than twice as likely as those without an ID to receive an ‘unknown’ diagnosis, suggesting that a clinician’s uncertainty regarding a mental health diagnosis is greater in people with an ID. There are a number of possible contributors to this including a lack of confidence of mental health professionals when working with people with an ID (Edwards et al., 2007; Torr et al., 2008), lack of training, complexity of mental health presentations, communication barriers and diagnostic overshadowing (Reiss et al., 1982).
The service use profile of people with an ID indicates the complexity of the mental health support needs of people with an ID. The greater number of contacts and the longer total duration of face-to-face contacts for those with an ID indicates either that their mental health issues are complex, or that other specific barriers to brief crisis contacts or interventions exist for people with an ID which bias the data toward longer direct contacts. The complexity of the service use supports the incorporation of ID as a specific factor in activity-based funding models for mental health with the view to improving service outcomes for service users with complex health conditions. A mechanism that provides a ‘clear price signal’ (Rosenberg and Hickie, 2013) and incentivises for timely, integrated and person-centred interventions in the treatment of people with an ID is required. Unless such adjustments are made, people with ID, who are often high-end service users, are unlikely to be afforded the appropriate intensity of clinical contact required to meet their substantial mental health needs.
The high intensity of ambulatory mental health service use by people with an ID suggests that the services may benefit from enhanced skills and resources in this area of clinical practice. Training of clinicians in ID mental health may equip mental health practitioners for the complexity and service needs of this population. Access to appropriately skilled ID mental health consultations from a specialised ID mental health team would also support the work of clinicians in the ambulatory mental health setting, and could provide a bridge to disability supports. The frequency and duration of the ambulatory health service contacts, as well as the proportion of ‘unknown’ diagnoses, could serve as useful indicators by which to monitor the impact of service enhancements in this area of clinical practice.
Notable methodological issues presented challenges during this study. Ethics approval for the study took more than half the total time allocated for the project (12 months) and was complicated by variations in parameters required for each site-specific study approval. The extraction of the data at local sites was made challenging by the outmoded hardware at the local sites which struggled to handle the computational load.
Limitations
One of the limitations of this study is the use of the DS-MDS as the main source of identification of people with an ID. However, an additional 300 people with an ID were identified from the MH-COM, and the incorporation of these individuals ensured a more complete representation of people with an ID than would otherwise have been achieved by reliance on identification from the DS-MDS alone. This methodology will have missed those individuals with ID who do not identify as having an ID and in whom ID was not recognised or coded by mental health services. Our methodology allowed for mapping of each diagnosis assigned to the person during the 6-years. As such, we have not identified the primary diagnosis, but rather the full range of diagnoses assigned for any individual during this period. This approach does not reflect the clinical nuance in which a primary diagnosis may emerge, and be complicated by various comorbidities. Another limitation of our study is that it reports only ambulatory mental health contacts thereby representing only one aspect of comprehensive mental health services and thus limiting the generalisability of the findings. We now have access to additional data which will allow us to report in the future on service use in inpatient, emergency and general practice settings. This will allow a more comprehensive picture to emerge regarding the service use and mental health needs of people with an ID. Also, our approach was unable to identify people who may have been managed by ambulatory mental health services for challenging behaviour. However, in our experience it is rare for people with an ID (or without an ID) to be managed by a public mental health service for challenging behaviour alone.
Conclusion
Linkage between the DS-MDS and the MH-COM datasets has allowed insights into the diagnostic and service use profiles of people with an ID who had contact with ambulatory mental health services over a 6-year period in an area of NSW. These profiles highlight a relative under-representation of people with an ID, a predominance of psychosis over other common diagnostic categories and a high level of diagnostic uncertainty in people with an ID. Ambulatory mental health service contacts for people with an ID consume considerable resources and would be appropriately provisioned by enhanced and targeted funding approaches and training of staff in this sector. Further data linkage across NSW, including linkage between emergency and inpatient datasets, could extend the findings to enable a more complete understanding of the diagnostic profiles and service use in other components of the mental health service system. Such an understanding will help assist the development of more comprehensive services for people with an ID, and would also assist in the monitoring of key policy and service initiatives in NSW, such as the NSW Health ‘Service Framework to Improve the Health Care of People with Intellectual Disability’ (NSW Health, 2012) and the NSW Health & ADHC ‘Memorandum of Understanding in the Provision of Services to People with an Intellectual Disability and a Mental Illness’ (NSW Health, 2011), which aim to improve health and mental health service delivery to this marginalised population.
Footnotes
Acknowledgements
The authors acknowledge the assistance, financial and otherwise, of Ageing, Disability & Home Care (ADHC) – NSW Department of Family & Community Services, and the Mental Health & Drug & Alcohol Office (MHDAO) – NSW Ministry of Health; also, InforMH – NSW Ministry of Health, for their advice on linkage.
Funding
This work has been supported by funding from Ageing, Disability & Home Care (ADHC) - NSW Department of Family & Community Services.
Declaration of interest
The authors report no conflict of interest. The authors alone are responsible for the content and writing of the paper.