
Abstract
There have been many attempts to understand the issues that affect access to health services. Goldberg and Huxley's Pathways to Care (PTC) model [1] was one of the first models in the mental health field to provide a coherent framework for understanding how people move into and through the health-care system. In its broadest sense, the model aimed to describe the selection processes that determine which individuals will seek care, and in which sector of care they will receive treatment. The model proposes that the health-care system can be conceptualized in terms of five discrete sectors of care, from the community, to primary care, to primary care for mental health problems, outpatient mental health care and inpatient care. Each sector represents a more specialized level of care within the spectrum of health service delivery. Individuals reach these sectors of care via a series of selectively permeable filters that reflect consultation, diagnostic, referral and admission decisions. Examination of the factors associated with passage through these filters can highlight areas of need and provide a framework for exploring the performance of each sector of care within the context of the health system as a whole.
The PTC model has been applied across a number of different health system settings in several countries [2]. Most commonly studies have examined rates of psychiatric morbidity at some or all of the model's five levels, to thereby comment on the relative permeability of the filters [3–5]. The framework has also been used to determine the contribution of various factors to the permeability of the filters [6–8] with studies finding support for the role of clinical as well as sociodemographic factors. Pathways to Care studies have been used to evaluate access to care for specific disorders [8], to examine intervals along the pathway [9–11] and to examine international differences in health systems [12, 13]. Although themodel is not without its criticisms [2, 14], it provides a coherent framework to examine health service use and remains one of the most widely applied models of access to care in psychiatry.
The Australian National Survey of Mental Health and Wellbeing (NSMHWB) [15] has provided a rich resource to examine service use for mental health problems in Australia. Previous analyses of the NSMHWB have focused on service utilization for mental disorders in general [16, 17], service use for particular diagnostic groups [18], the types of interventions received [19], met and unmet need [20–23] and service use patterns in individual sectors of care such as the primary care sector [24]. These analyses have been useful in profiling service use for mental health problems in Australia as well as highlighting specific areas of need. In particular, these studies have highlighted the importance of the primary care sector in the delivery ofmental health care, the association of particular sociodemographic characteristics such as sex, education and marital status with help-seeking, the importance of perceived need in the decision to seek help as well as low coverage for some of the common and treatable mental disorders.
Few previous analyses have focused on the health-care system as a whole and none have examined the characteristics of those treated in each sector of care from the community to inpatient care. In particular, no previous analysis of the NSMWHB has presented comprehensive data on inpatient care and no study has examined the factors associated with use of private and public sector outpatient services for mental health problems. Previous analyses of private psychiatric care have been limited to surveys of practicing psychiatrists [25, 26] or to examination of Medicare data [27–29]. Australian data on private psychiatric care from a representative population survey have not previously been available.
The present paper steps off the framework provided by Goldberg and Huxley's PTC model to examine the health system as a whole. Specifically, it addresses the question: what are the factors associated with use of each sector of care in Australia? It draws on data from the Australian NSMHWB to examine the factors associated with reaching the primary care, outpatient and inpatient sectors, as well as those associated with accessing private versus public mental health services. It examines sociodemographic and clinical factors in an attempt to examine the way each sector of care performs within the mental health-care system as a whole.
Method
Survey design and sample
The NSMHWB was a nationwide household survey of adults conducted in 1997 to determine the prevalence of both ICD-10 and DSM-IV mental disorders in the community and their associated disability and service utilization [15]. The sample consisted of 10 641 people over the age of 18 years, a response rate of 78.1% and was weighted to match the age and sex distribution of the Australian population and to account for probability of selection.
Measurement of service utilization
Respondents were asked about service utilization in the 12 months before interview, with a focus on the type of professional consulted, the number of consultations made and whether those consultations were for ‘mental problems such as stress, anxiety, depression or dependence on drugs or alcohol’, referred to in this paper as ‘mental health consultations’. The five levels of care in the PTCmodel were defined as follows: Level 1: Community – all respondents in the survey (n = 10 641); Level 2: Primary Care – at least one consultation for any reason with a general practitioner (GP; n = 8682); Level 3: Primary Mental Health Care – at least one mental health consultation with a GP (n = 981); Level 4: Outpatient Care – at least one mental health consultation with another health provider (n = 804); Level 5: Inpatient Care – at least one admission to hospital for mental health problems (admissions included general hospitals, private and public psychiatric hospitals and drug and alcohol units; n = 47). Figure 1 illustrates each of these levels as they fit within Goldberg and Huxley's [1] PTC model.
Goldberg and Huxley's Pathways to Care model (adapted from [1]).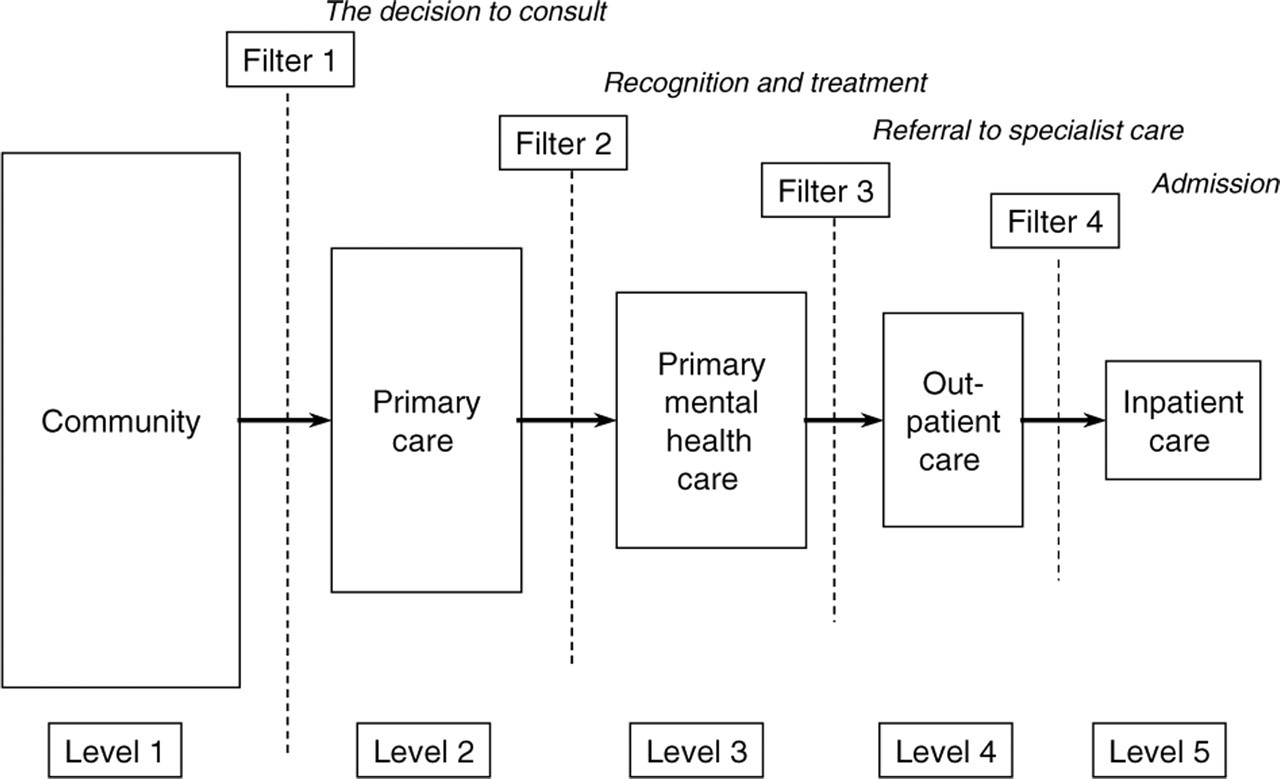
Outpatient Care (Level 4) was further examined to determine the type of provider seen in this sector. Providers were divided into four groups: (i) psychiatrists; (ii) allied health professionals (psychologists, social workers, counsellors, drug and alcohol workers, mental health team); (iii) non-psychiatric medical specialists; and (iv) ‘other’ health professionals. Respondents in the survey who reported mental health consultations were asked to indicate where the consultation/s with each type of professional took place. Respondents were coded as having seen a health professional privately if they reported at least one mental health consultation with that professional ‘in their rooms (surgery, clinic or shop)’.
Clinical characteristics
Diagnosis
The Composite International Diagnostic Interview (CIDI, version 2.1) [30] was used to determine the presence of DSM-IV and ICD-10 diagnoses of anxiety, affective and substance use disorders in the past 12 months and screening questionnaires were used for neurasthenia [31], psychosis [32] and personality disorders [33]. For this analysis, ICD-10 diagnoses were used. Note that because of the sampling strategy used in the NSMHWB, it is likely that people with chronic psychosis were under-represented.
Disability and distress
Disability was measured using the Medical Outcomes Study Short Form 12 (SF-12) [34], a measure of disablement or health status. It has two regression-weighted scales, a mental health (MCS-12) and a physical health summary scale (PCS-12). Higher scores indicate less disability. Disability days were defined as the number of days in the previous 4weeks where the respondent had to ‘cut down’ or was ‘completely unable to carry out’ their normal activities [35]. Psychological distress was measured using the Kessler 10 (K10) [36]. Higher scores indicate more severe distress.
Sociodemographic characteristics
Respondents' age, sex, marital and employment status, highest level of education attained, primary source of income and whether the residence was located in a metropolitan or rural region were collected as part of the survey.
Analysis
Four multivariate logistic regression analyses were conducted with sector of care (defined earlier) as the dependent variable. In each analysis, the comparison group comprised those who did not reach that sector of care, that is, those who did not pass through that particular filter: Model 1 – Primary Care (Level 2) versus Community only (those who did not consult a health professional for any reason); Model 2 – PrimaryMental Health Care (Level 3) versus Primary Care only; Model 3 – Outpatient Care (Level 4) versus Primary Mental Health Care only; Model 4 – Inpatient Care (Level 5) versus Outpatient Care only. Note that although the PCT model is conceptualized as a progression through Levels 1 to 5, it is possible to be treated at any level of care in the model without having passed through previous levels. Thus, although the majority of respondents treated in each sector will be a subset of those treated at levels lower in the pathway, there will be some who do not follow this pattern, and these respondents are included in this analysis. Two further logistic regressions were conducted to examine the factors associated with private sector use among those receiving outpatient care: Model 5 – at least one mental health consultation with a private psychiatrist versus public sector outpatient care only; Model 6 – at least one mental health consultation with a private allied health professional versus public sector outpatient care only. Private psychiatrists were examined separately to other health professionals as Medicare arrangements in 1997 (the year the NSMHWB data were collected) included reimbursement for consultations with psychiatrists but not other health professionals.
All models were screened for adequacy of expected frequencies and for the presence of multicollinearity [37]. To facilitate consistency across the models, independent variables were coded uniformly which meant reducing the number of categories for certain variables (e.g. rurality, age). The contribution of individual variables was assessed using the Wald χ 2 statistic, and odds ratios (OR) were derived from multivariate models where all variables in the analysis were controlled. The only exceptionwas themodel examining inpatient versus outpatient care. Small cell sizes precluded multivariate modelling for this analysis. Thus, ORs presented are from univariate models only. Univariate ORs for other models were examined for screening purposes and are available on request. Standard errors around proportions and confidence intervals around ORs were calculated using jackknife repeated replication [38] to account for the sampling design. The SUDAAN software packagewas used for all analyses [39] which were conducted using the 2001 version of the Confidentialised Unit Record File (CURF).
Results
Clinical characteristics of those treated in each sector of care
The proportion of the population treated in each sector of care and their clinical characteristics are presented in Table 1. The majority of the population reported GP consultations and one in 10 of these respondents, or 8.2% of the population reported mental health consultations with a GP. Approximately one in 15 people reported outpatient mental health care, most of whom also reported contacts in the primary care sector, either for mental health problems (56.4%; SE = 1.7) or for other reasons (90.9%; SE = 1.0). Only 0.4% of the population, or one in 20 of those who reported a mental health consultation reached the inpatient sector.
Clinical characteristics of those seen in each sector in the Pathways to Care model
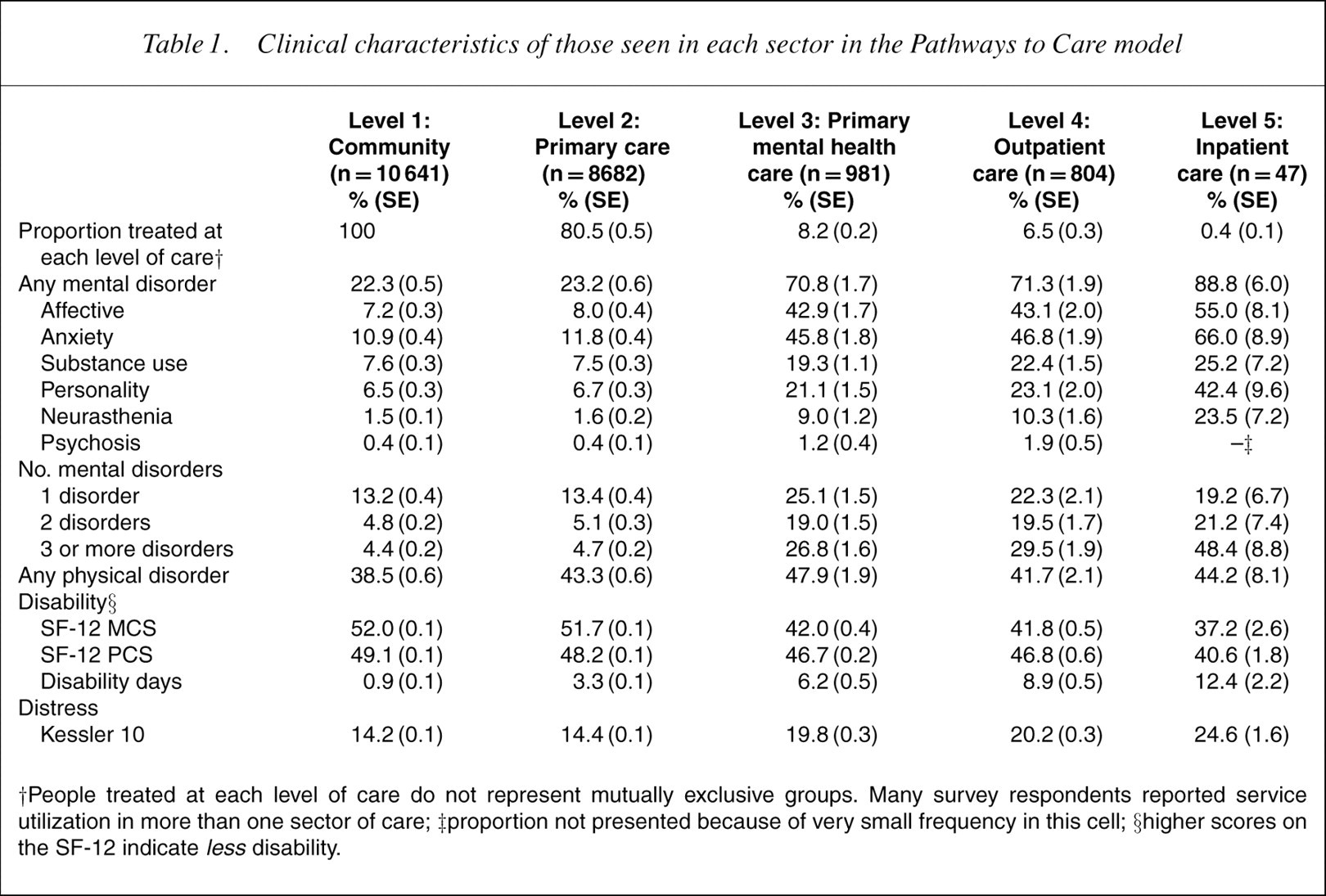
†People treated at each level of care do not represent mutually exclusive groups. Many survey respondents reported service utilization in more than one sector of care; ‡proportion not presented because of very small frequency in this cell; §higher scores on the SF-12 indicate lessdisability.
Although only 22% of the population met criteria for a mental disorder, 71% of those who reached primary mental health or outpatient care and 89% of those who reached inpatient care met the CIDI diagnostic criteria for a mental disorder. Comorbidity, disability and distress also increased across these sectors. Although only 9% of the community report comorbid mental disorders, almost 80% of those who reached inpatient care sometime during the previous year met criteria for more than one mental disorder, and almost half met criteria for more than two disorders. This inpatient group reported high levels of distress and disability (<1 SD below the normal population mean) and almost one in two disability days in the previous 4weeks, even though none were presently in hospital.
The groups in Table 1 represent the entire group of people treated in each sector of care and as such, do not represent mutually exclusive groups. Figure 2 presents key clinical indicators coded against the most specialized sector of care reached. These groups, therefore, represent mutually exclusive groups, allowing the pattern of increasing severity observed in Table 1 to emerge more clearly. In Fig. 2, we show that having one of the 12 chronic physical disorders was a strong determinant of attending a GP, but not understandably of seeking help for a mental disorder. Conversely, the probability of meeting criteria for a mental disorder rose steadily – from 18% to 90% as specialization of care increased. Even so, those who only consulted a GP for a mental problem reported significant mental health problems: 62.6% (SE = 2.9) met criteria for a mental disorder, 34.8% (SE = 2.7) for more than one, and on average they reported 6.2 (SE = 0.5) disability days in the previous 4weeks.
The presence of any mental or physical disorder among all survey respondents coded against the most specialized level of care accessed.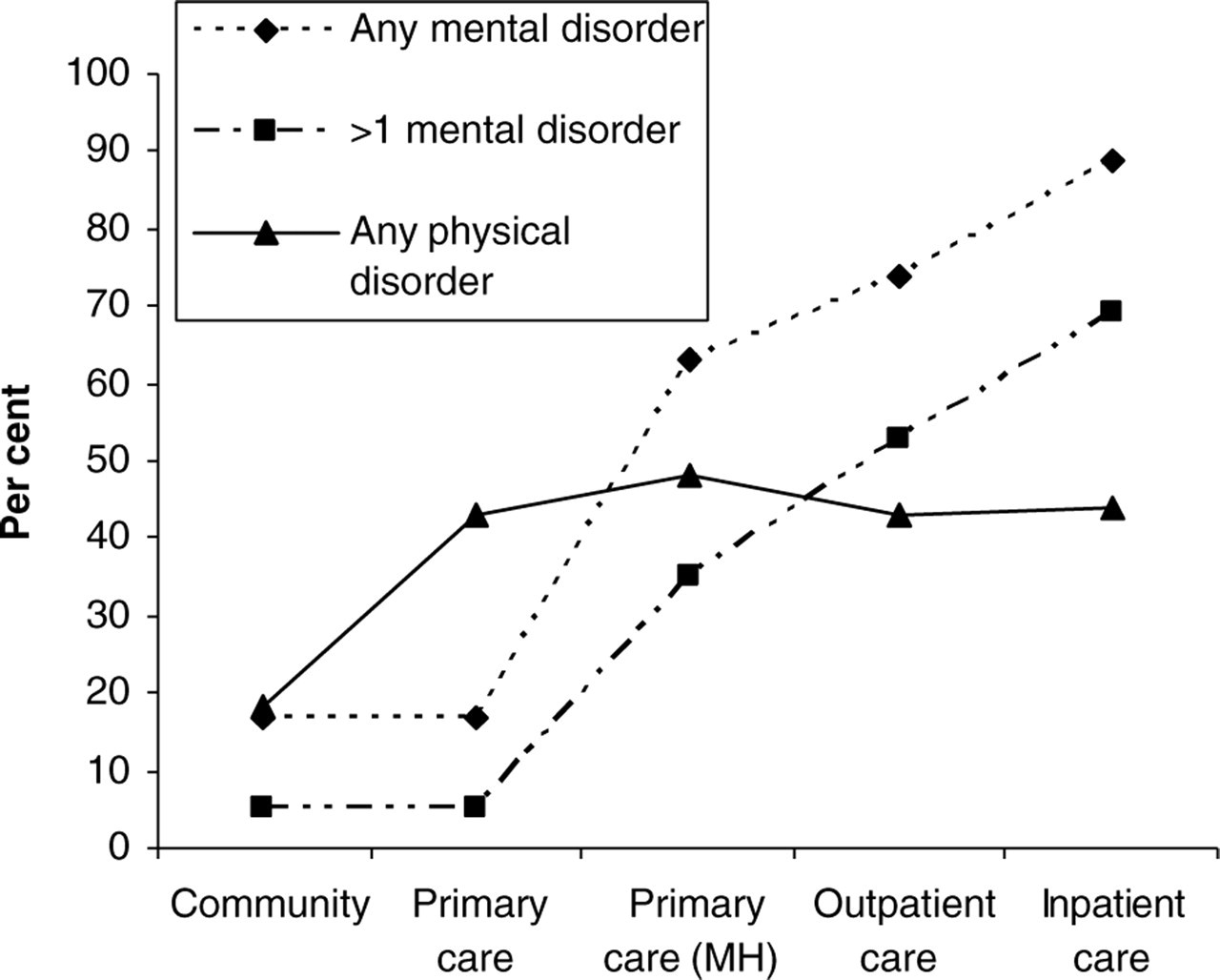
Sociodemographic characteristics of those treated in each sector of care
Table 2 presents sociodemographic characteristics of those treated in each sector, again with each group being the entire sample treated in that sector. Females represented almost two-thirds of thosewho reported primary mental health or outpatient care. Those aged over 55 years represented a quarter of those in the community, but only one in 10 of those treated in the outpatient sector. Indicators of socioeconomic disadvantage, whether antecedent or consequence, such as unemployment (60%) and lack of tertiary qualifications (60%) or presence of pension (40%) were features of those treated in the inpatient sector.
Sociodemographic characteristics of people treated in each sector in the Pathways to Care model
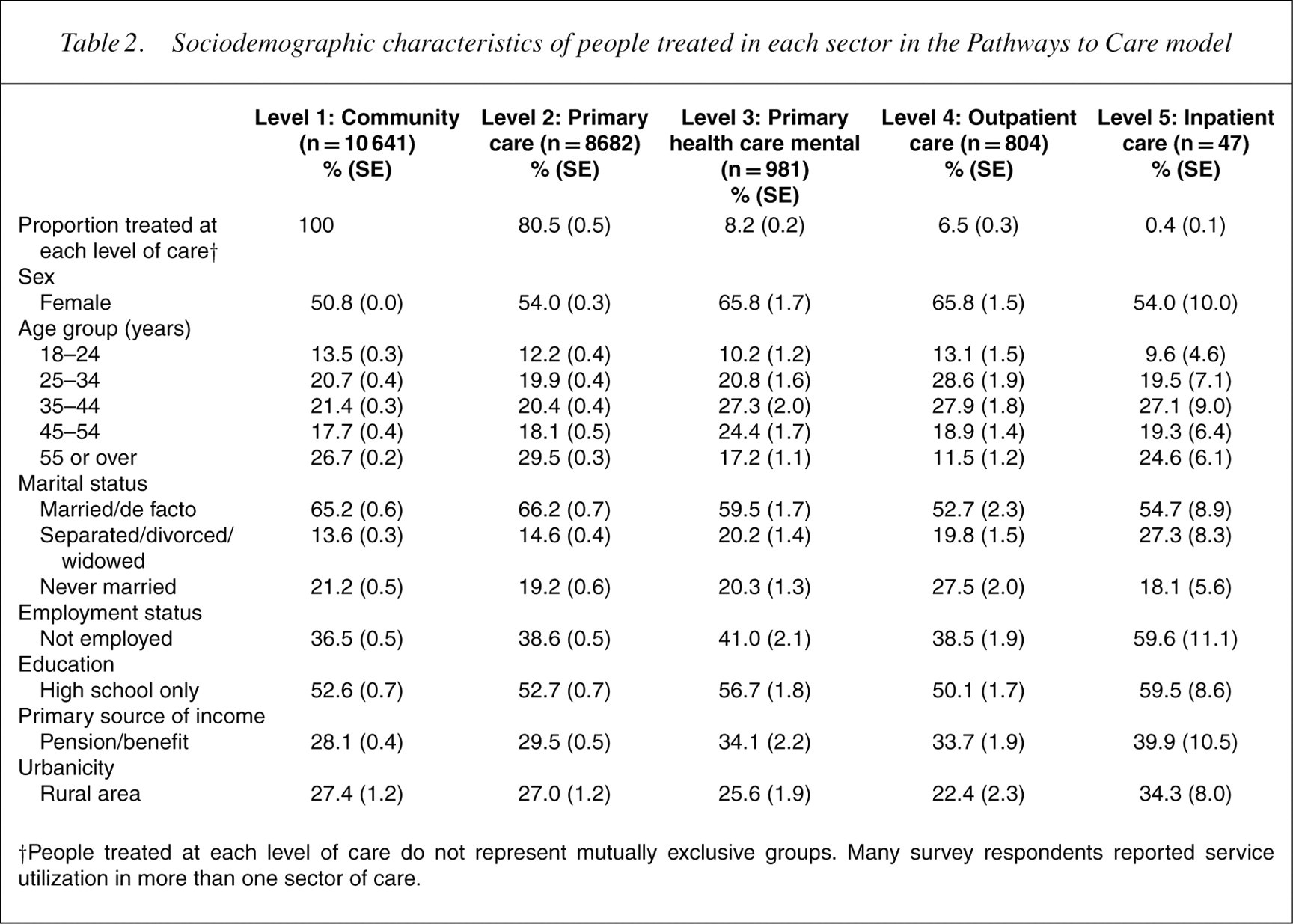
†People treated at each level of care do not represent mutually exclusive groups. Many survey respondents reported service utilization in more than one sector of care.
Factors associated with treatment in each sector of care
Table 3 presents the results of the logistic regression modelling that assessed which clinical and sociodemographic characteristics were significantly associated with access to each sector of care.
Factors associated with reaching each sector of care in the Pathways to Care model†
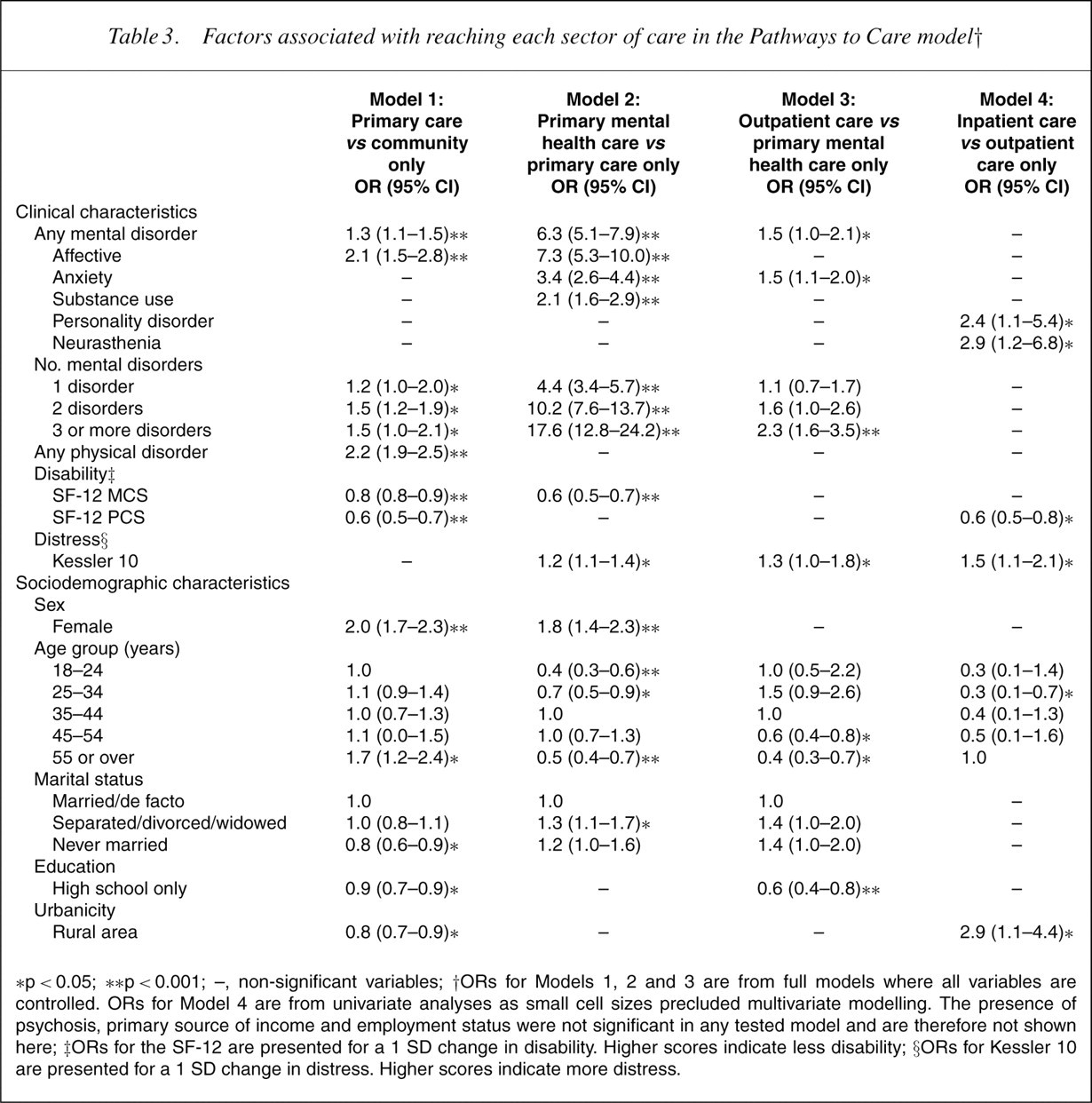
∗p<0.05; ∗∗p<0.001; –, non-significant variables; †ORs for Models 1, 2 and 3 are from full models where all variables are controlled. ORs for Model 4 are from univariate analyses as small cell sizes precluded multivariate modelling. The presence of psychosis, primary source of income and employment status were not significant in any tested model and are therefore not shown here; ‡ORs for the SF-12 are presented for a 1 SD change in disability. Higher scores indicate less disability; §ORs for Kessler 10 are presented for a 1 SD change in distress. Higher scores indicate more distress.
Clinical characteristics
Considering Model 1 first, several clinical variables were significantly associated with access to primary care. Although mental health indicators (presence of mental disorders, MCS-12) were significant in this model, the most important clinical predictors of primary care sector use were the presence of a physical disorder (χ 2 = 136.0, p<0.001) and physical disability (χ 2 = 86.6, p<0.001). In Model 2, this pattern was reversed. Access to GPs for mental health problems was most strongly associated with the presence of a mental disorder (χ 2 = 294.8, p<0.001), comorbid mental disorders (χ 2 = 553.9, p<0.001) or mental health-related disability (χ 2 = 71.3, p<0.001). Although the presence of affective, anxiety and substance use disorders was associated with access to primary mental health care, the affective (χ 2 = 160.2, p<0.001) and anxiety disorders (χ 2 = 88.3, p<0.001) were the most important of those examined.
Models 3 and 4 examined the factors associated with access to specialist mental health care. The presence of a mental disorder (χ 2 = 5.2, p<0.05),more than two disorders (χ 2 = 20.7, p<0.001) and increased levels of distress (χ 2 = 3.9, p<0.05) were significantly related to use of the outpatient as opposed to primary care sector. Those with anxiety disorders, in particular, were more likely to access specialist outpatient care (χ 2 = 6.3, p<0.05), although the presence of an affective disorder was significant when the K10 and the SF-12 were not in the model (χ 2 = 4.8, p<0.05). Because of small cell sizes, access to inpatient care was examined with univariate models only. Diagnoses of neurasthenia (χ 2 = 6.4, p<0.05) and personality disorders (χ 2 = 5.0, p<0.05) were significantly associated with inpatient care as were higher levels of physical disability (χ 2 = 10.4, p<0.05) and psychological distress (χ 2 = 7.8, p<0.05). It should be remembered that because of small cell sizes, psychosis was not included in this model.
Sociodemographic characteristics
Controlling for clinical variables, several sociodemographic characteristics were associated with access to different sectors of care. Sex (χ 2 = 106.2, p<0.001), age (χ 2 = 32.6, p<0.001), marital status (χ 2 = 7.7, p<0.05), education (χ 2 = 6.4, p<0.05) and urbanicity (χ 2 = 7.7, p<0.05) were all significantly associated with access to primary care. Specifically, being female, aged 55 years or over, being in a married or de facto relationship, educated or living in ametropolitan area were associated with increased access to primary care. In Model 2, being female was also significantly associated with access to primary mental health care (χ 2 = 27.3, p<0.001) but age (χ 2 = 47.1, p<0.001) and marital status (χ 2 = 6.5, p<0.05), although both significant showed a different pattern of association. Those in both younger (18–24 and 25–34 years) and older age groups (<55 years) were significantly less likely to report GP consultations for mental health problems than those aged 35–44 years, who reported the highest use of this sector (27.3%; SE=2.0). Those who were separated widowed or divorced were more likely than those in married or de facto relationships to report access to primary care for mental health problems.
In Model 3, three sociodemographic variables were associated with access to specialist outpatient care (age: χ 2 = 35.0, p<0.001; education: χ 2 = 12.4, p<0.001; and marital status: χ 2 = 6.6, p<0.05). Age and education were the most significant of all variables in the model. Those in older age groups (45–54 and <55 years) were significantly less likely to report outpatient care than those aged 35–44 years and those with a high school only education were significantly less likely to report outpatient care than those with a higher qualification. Although ORs for individual marital status comparisons just failed to reach significance, univariate analyses indicated that being never married was significantly associated with outpatient mental health care (OR=2.1, CI=1.4–3.0). In Model 4, age was also significantly associated with access to inpatient care (χ 2 = 10.1, p<0.05). Those over 55 years were more likely to report inpatient as opposed to outpatient care than the other age groups, although this was only significant compared to those aged 25–34 years, and in a model controlling for both age and physical disability, neither variable was significant (χ 2 = 4.4, p=0.35; χ 2 = 1.5, p=0.22). Living in a rural area was significantly associated with an inpatient episode as opposed to outpatient care (χ 2 = 4.8, p<0.05), and this effect remained significant in a model that controlled for the presence of anymental disorder (χ 2 = 4.0, p<0.05).
Outpatient care for mental health problems
Figure 3 presents the 6.5% of the population who reported outpatient care by provider type. One in six people who reached outpatient mental health care consulted a private psychiatrist, one in three a private allied health professional and one in 12 a combination of these two professional groups. This means that 1.6% (SE=0.2) of the population saw a private psychiatrist and 2.7% (SE=0.2) a private allied health professional (most commonly a psychologist: 50.1%, SE=3.3). A smaller group, 0.9% (SE=0.1), reported public sector outpatient care only. One in four of those who reported outpatient care saw a medical specialist or ‘other’ health professional for mental health problems but did not see a mental health specialist. This group represents 1.7% (SE=0.2) of the population. Those who consulted ‘other’ health professionals most commonly saw a naturopath (29%), or an alternative medicine therapist such as an acupuncturist, hypnotherapist, or spiritual healer (42%).
Respondents accessing outpatient care for mental health problems (n = 804; 6.5%) by provider type.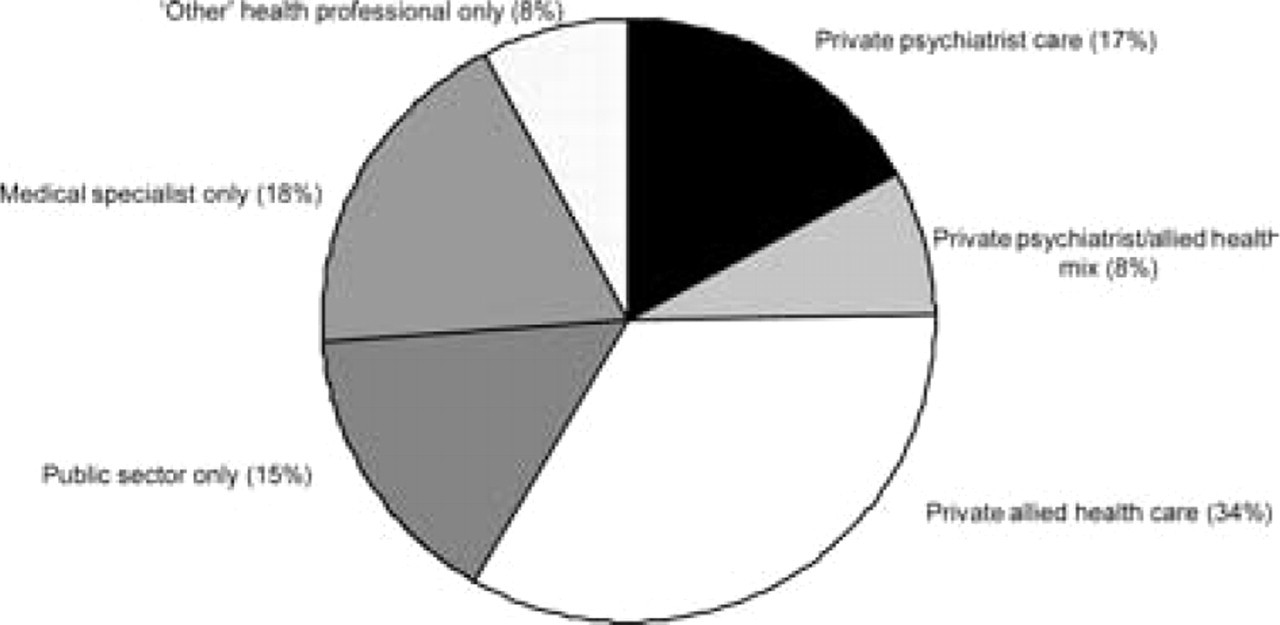
Clinical characteristics of those accessing private and public sector outpatient care
Table 4 presents the characteristics of those accessing private and public sector outpatient care. Eighty per cent of those who consulted private psychiatrists met criteria for a mental disorder, more than half for more than one disorder, and this group reported significant levels of disability and distress. They reported 13 disability days in the previous 4weeks. With the exception of higher rates of neurasthenia among the private psychiatrist group, the clinical characteristics of the other two groups (private allied health professional care and public sector care only) were very similar. Those who saw medical specialists or ‘other’ health professionals only (1.7%) are not included in this table: 61.4% (SE=4.7) of this group met criteria for a mental disorder, 42.8% (SE=3.5) for more than one; mean MCS-12 was 44.0 (SE=1.0), K10 was 18.4 (SE=0.5) and they reported an average of 5.6 (SE=0.6) disability days in the previous four weeks.
Clinical characteristics of people receiving public and private outpatient care by provider type
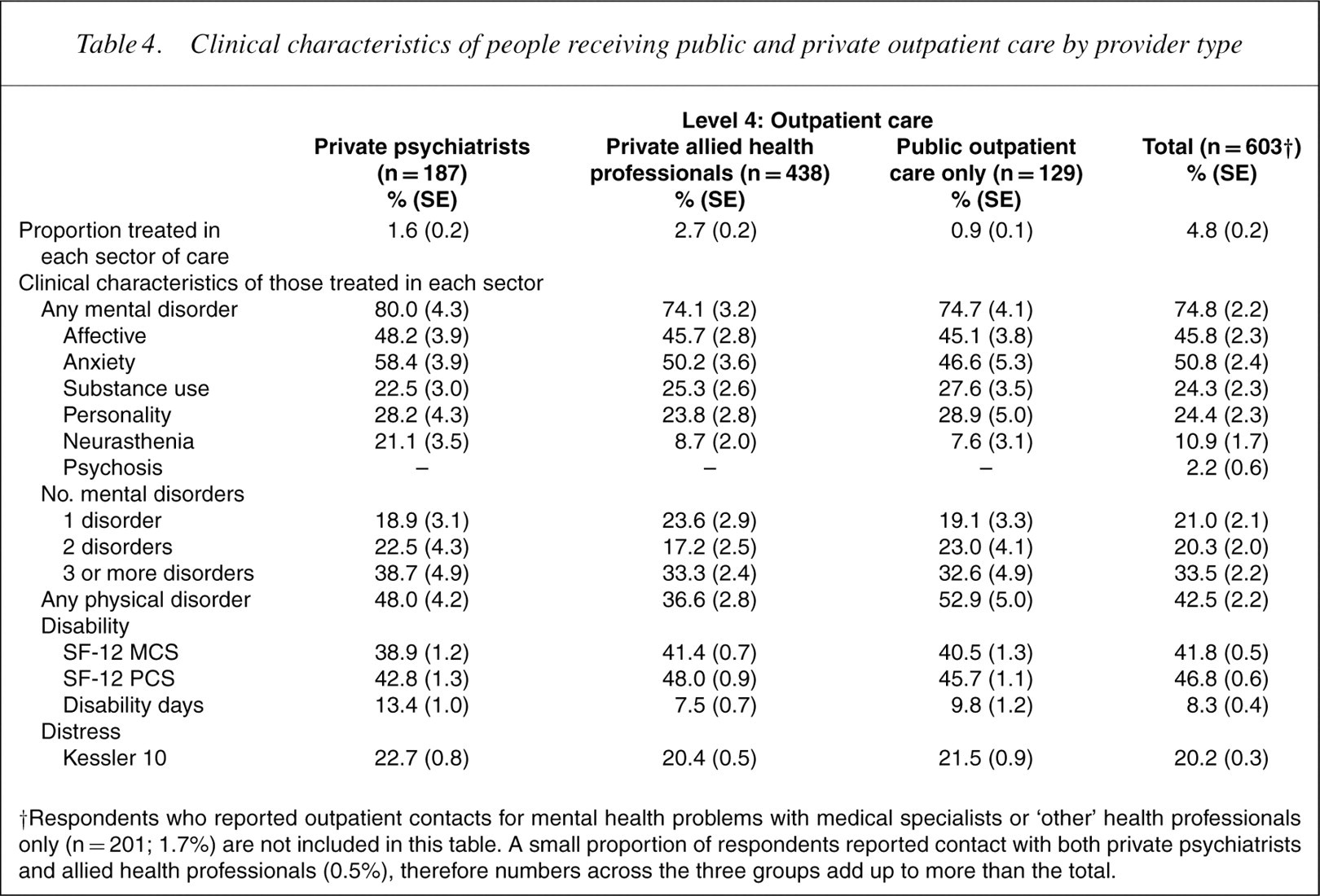
†Respondents who reported outpatient contacts for mental health problems with medical specialists or ‘other’ health professionals only (n = 201; 1.7%) are not included in this table. A small proportion of respondents reported contact with both private psychiatrists and allied health professionals (0.5%), therefore numbers across the three groups add up to more than the total.
The number of consultations with private psychiatrists and private allied health professionals was also examined. One in six of those who saw private psychiatrists consulted once in the previous 12 months (15.6%; SE=2.8) and the median number of consultations was 5. One in four reported more than 10 consultations over the 12-month period (26.0%; SE=3.5). The number of consultations among those reporting contact with private allied health professionals was similar. Those consulting psychologists privately (the largest group of private allied health professionals consulted) reported a median of 4 consultations, 15.4% (SE=3.1) consulted once and 20.7% (SE=2.7) more than 10 times over the 12-month period.
Sociodemographic characteristics of those accessing private and public sector outpatient care
The data in Table 5 indicate that half of those reporting public sector care only received a pension or benefit such as the primary source of income and 60.9% were unemployed. Both of these indicators of socioeconomic disadvantage were lower but still considerable among the groups accessing private mental health care whether Medicare subsidized or not.
Sociodemographic characteristics of people receiving public and private outpatient care by provider type
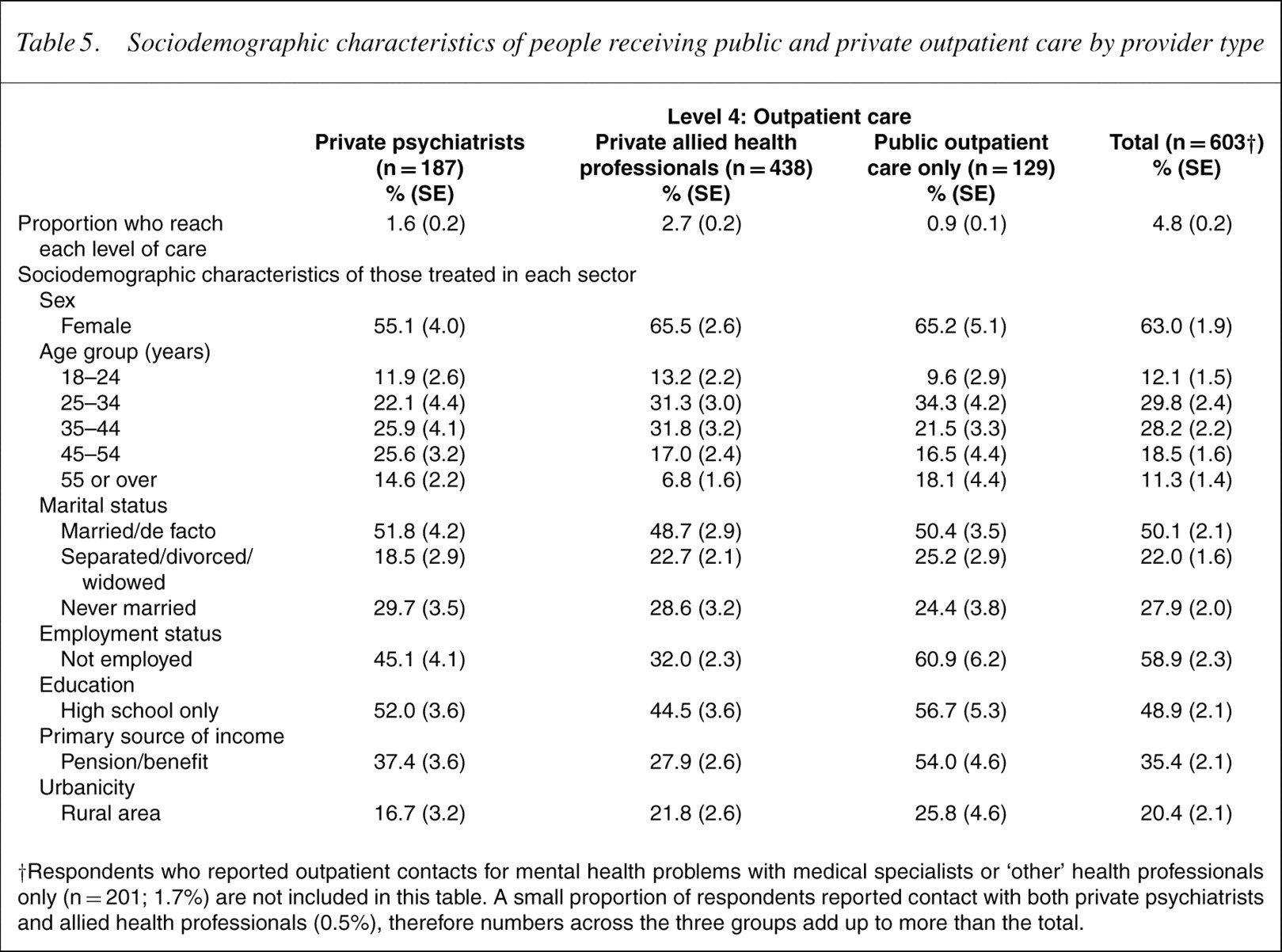
†Respondents who reported outpatient contacts for mental health problems with medical specialists or ‘other’ health professionals only (n = 201; 1.7%) are not included in this table. A small proportion of respondents reported contact with both private psychiatrists and allied health professionals (0.5%), therefore numbers across the three groups add up to more than the total.
Factors associated with use of private sector outpatient care
Models 4 and 5 assessed which factors were significantly associated with use of private sector as opposed to public sector care. Although a diagnosis of neurasthenia was associated with private psychiatrist care in a univariate model (χ 2 = 4.5, p<0.05), it was not significant in a multivariate model. No other clinical variables were significantly associated with private sector care for either professional group. Controlling for clinical variables, both employment status (χ 2 = 6.0, p<0.05, OR=2.5, CI=1.2–5.5) and source of income (χ 2 = 4.4, p<0.05, OR=2.0, CI=1.1–4.0) were significantly associated with access to private psychiatrist care (because of their strong relationship, they were tested in separate multivariate models). Both employment status and income showed even stronger association with access to private allied health professional care (χ 2 = 16.4, p<0.001, OR=2.9, CI=1.7–5.0; χ2=17.8, p<0.001, OR=2.8, CI=1.7–4.6). Living in a rural area was associated with less use of private psychiatrists (χ 2 = 4.0, p<0.05, OR=0.5, CI=0.2–1.0).
Discussion
Summary of results
The present study indicated that while most people consulted their GPs during the year fewer than would be expected reported mental health consultations either in the primary or specialist sectors. Of the total population 0.4%, or one in 20 of those who consulted for mental health problems, reported an inpatient admission during the year. Clinical severity increased as specialization of care increased, with those who reported inpatient care representing a highly disabled group. Clinical factors were strongly associated with use of different sectors of care, with physical health indicators important determinants of access to general primary care, and mental health indicators important determinants of access to mental health care in the primary and specialist sectors. Despite this, several sociodemographic characteristics were significantly associated with access to various sectors of care. Most notably, those over 55 years of age were more likely to access the general primary care sector and the inpatient mental health sector, but less likely to report mental health consultations in the primary care or outpatient sectors than those in younger age groups. Those in rural areas were less likely than those in metropolitan areas to report access to the primary care sector, but among those accessing specialist mental health care were more likely to report inpatient as opposed to outpatient care.
One in four of those who reported mental health outpatient consultations did not see a mental health professional, consulting instead with medical specialists and alternative health practitioners. Private psychiatrists and private allied health professionals were consulted by 1.6% and 2.7% of the population, respectively. Although those accessing private and public outpatient care were clinically similar groups, those accessing private care were more likely to be employed and receive an independent income than those reporting public sector care only, and this effect was strongest among those who consulted private allied health professionals. There was evidence of lower consultation rates with private psychiatrists among those living in rural areas. Those who saw psychiatrists or allied health professionals privately most commonly consulted between four and five times, and between one in four and one in five reported more than 10 consultations over 12months.
Limitations
There are a number of limitations. First, the PTC framework is a simplistic model of access to health services [2, 14]. It does not focus explicitly on complex passages through the health-care system, passages back through the model, or the bypassing of various levels and filters, and several filters can be interpreted in a number of ways [1, 2, 14, 23]. The filter between primary care and primary care for mental health problems, for example, is defined by Goldberg and Huxley as the recognition of mental disorders by GPs. It could equally be defined as the decision to consult for mental health problems by consumers [40] and may in reality reflect both these behaviours. Several studies have stepped off the PTC framework to examine these complexities [11, 12], and as Huxley [2] points out, in most countries themodel accounts for more people that not. Moreover, regardless of how one defines the filters in the model, decisions about consultation, diagnosis and referral are still subject to similar principles and can be evaluated empirically [2, 7, 12].
The second limitation worthy of discussion arises from the use of retrospective self-report for health service consultations and, in particular, for the measurement of consultation in the private sector. Like most major epidemiological surveys, no corroborative information on service use was available. A previous analysis of the congruence of reports from epidemiological data and other sources suggests that although there may be considerable consistency across parallel sources of information, self-report estimates may be lower than those from other sources [41]. However, the most substantial threat to the validity of these data probably relates to measurement of consultation in the private outpatient sector. Reports of private consultations were based on respondents' selfreport of the location of consultation and there is no way of verifying these data. However, the congruence across these data and those based on Medicare rebates for private psychiatrists for the same period: 1.6% versus 1.5–1.6% of the population; ref. [42] lends some support to their validity, as does the relationship between sociodemographic characteristics and private practitioner access, discussed below.
The third limitation relates to the sample used for the present analysis. The fact that the sample was drawn from a population epidemiological sample rather than from clinical samples has many advantages. The most important of these relates to the representativeness of the sample and, therefore, the conclusions that can be drawn about the use of each sector of care. However, it should be noted that because of few numbers of the population reporting inpatient care (0.4%; n = 47), it was not possible to differentiate between groups admitted to private or public hospitals where one would expect differences in demographics and mental disorder diagnoses [43]. Similarly, the low rates of psychosis in the general community meant that the number of people in the inpatient group with a diagnosis of psychosis was very small. Data from both Australian inpatient samples [43] and the Australian Low Prevalence Disorders Survey [44] indicate that inpatient service use among this group is high, predominantly in the public sector.
Discussion of major findings
With these caveats inmind, the study offers a number of points of interest. Four out of five Australians consulted a GP for some reason in the 12-month period, indicating that the filter between the community and primary care – the decision to consult a GP – is by far themost permeable in the PTC model. Although previous analyses of the NSMHWB have typically concentrated on consultation among those with mental disorders, rather than the whole community, they have similarly indicated that most people with mental disorders are seen by GPs [16, 17]. Our results also indicated that consultation with a GP for any reason was far more common than consultation with a GP for mental health problems, a finding that has also been reported in previous PTC studies [3, 4]. Consultation with GPs in Australia has been explored in some detail within the context of met and unmet need [24] and the types of interventions received [19, 45], and it is not the intention of the present discussion to repeat the arguments put forward in these reports. The usefulness of the PTC model lies in the fact that it facilitates examination of each sector of care within the context of the broader health system and it is this on which the bulk of the discussion focuses.
The analysis showed a clear progression in clinical severity across the five sectors of care and this was confirmed in the regression modelling that showed the importance of clinical variables in predicting use of each sector of care. As one would expect, those accessing inpatient care reported the highest levels of disability, distress and comorbidity of any group within the mental health system. Furthermore, although variables related to physical health were the most important clinical predictors of access to general primary care services, they were not associated with mental health care in the primary care sector. In this model, variables related to mental health were far more important. Both of these findings indicate that at the broadest level, each sector of care is performing as one would expect.
However, several findings qualify this statement. The first relates to the role of sociodemographic characteristics, the second to the use of the private sector and the third to the types of professionals consulted in the outpatient sector. Controlling for clinical characteristics, several sociodemographic characteristics were significantly associated with access to various sectors of care. The relationship between gender, marital status and education with mental health consultation in both primary and specialist sectors is well-documented [16, 40]. In this analysis, many of the same variables predicted consultation with GPs for any reason among the general community, suggesting that these relationships may reflect general consulting behaviour, rather than behaviours specific to mental health [46].
Age was the only sociodemographic variable significant across all analyses within the PTC model. Older adults were more likely to report consultation in the general primary care sector but less likely to report mental health consultations in the primary and specialist sectors than those in the younger to middle age groups. Among those who reached specialist mental health care, there was also some evidence that those over 55 years were more likely to receive inpatient as opposed to outpatient care – although the analysis suggested this effect was driven by physical disability. In an earlier analysis, we determined that consultation rates among those in older age groups were not significantly different from those in younger age groups [16]. However, the previous analysis focused on consultation for mental health problems only. The present study suggested that although older adults consult GPs for general health problems, they are less likely to reach primary mental health care and specialist care. There is some suggestion that perceived need for care may be lower among older adults [21, 47], which in turn may influence consulting behaviour and reporting of symptoms [48]. However, there is also evidence from the NSMHWB that older adults who consult for mental health problems do not receive the range of treatments offered to younger people [19], suggesting that clinician behaviour may also play a role. Although the NSMHWB determined that prevalence of mental disorders declines in older age groups [15], others have argued that the sampling strategy may have under-represented those with greater mental health problems in older age groups [49], and in this analysis, the effect of age persisted, controlling for the presence of mental disorders and related disability. Taken together the findings suggest that although older adults frequently access general primary health care, they may not receive equitable access to mental health care in the primary and specialist outpatient sectors and this may be a reflection of both consumer and clinician behaviours.
Those living in rural areas as opposed to metropolitan areas were less likely to report consultation with GPs for any reason, but no more likely to report GP consultations for mental health problems. Those accessing specialist mental health services were more likely to report inpatient as opposed to outpatient mental health care. Two previous analyses of service utilization in the NSMHWB similarly determined that living in a remote area was not associated with lower rates of GPconsultations formental health problems [17, 23], but neither analysis examined GP consultations in general, among the whole community. A third recent analysis [50] using data from the Bettering the Evaluation and Care of Health (BEACH) program determined that living in a rural or remote area as opposed to metropolitan area was associated with less use of GPs in general and for mental health problems. Given that the distribution of GPs in Australia is not uniform [51], it is reasonable to suggest a lower per capita number of GPs in rural areas may influence access to primary care for those living in rural areas, and the results of the present study would support this. More curious is the relationship of rural location to inpatient care. It is possible that in the context of restricted outpatient mental health resources, as well as the difficulties in providing community-based care in remote areas, the threshold for referral to an inpatient unit is lowered. Although difficult to directly verify, studies of hospital admission decisions have determined that the availability of alternatives to hospitalization has a significant impact on the decision to admit [52].
Sociodemographics also played a key role in the use of private practitioners in the outpatient mental health sector. Of the total population, 1.6% reported at least one consultation with a private psychiatrist, 2.7% with a private allied health professional. Across all outpatient groups, the number of people with psychosis was small, reflective of the population-based sample used in the present study. Those with neurasthenia represented a fifth of people seen by private psychiatrists. The public and private groups were clinically similar, reporting high rates of comorbidity, disability and distress. Although the age distribution is fairly consistent with that based on data from other sources [25, 27, 53], the proportion of females in the private psychiatrist group was slightly lower than expected, although rates were not significantly different from the other two groups. Indicators of socioeconomic disadvantage (unemployment, receipt of a pension) were higher among those accessing public care only. This is likely to reflect both enabling factors such as ability to pay for services as well as access issues such as greater distribution of private practitioners in higher socioeconomic areas [28]. The relationship between employment and income and private consultations was strongest for those consulting private allied health professionals which might be expected given different arrangements under Medicare across professional groups. The study also determined that those living in rural areas accessing outpatient care were less likely to report private psychiatrist consultations than those inmetropolitan areas and this too is likely to reflect distribution of resources across rural and metropolitan areas [23, 28, 42]. It should be noted that the present study did not examine socioeconomic status within different parts of the metropolitan area and it is certainly possible that access to the private outpatient or other sectorsmay be influenced by greater or lesser levels of deprivation within cities [23].
A final issue for discussion relates to the use of different types of health professionals in the outpatient sector. Of the total population, 1.7% reported a mental health consultation with a medical specialist or alternative health practitioner but not a mental health specialist – the same number of people in fact who reported seeing a private psychiatrist. A significant proportion of this group met criteria for amental disorder. Use of non-psychiatricmedical services among those with mental disorders is fairly common and has substantial cost implications [54], given that it is unlikely that this group is having their mental health needs met. Those consulting alternative health providers represent a smaller group, but one that is not frequently discussed in the mental health literature. Although it is not possible to determine from these data whether this group is consulting appropriately, there is a growing interest among consumers in Australia about alternative medicine and it is arguably an area about which too little is known [55].
Conclusions
The present study suggests that at a broad level the health system is performing as we would expect. Clinical severity increases as specialization of care increases from the community through primary, outpatient and inpatient care and clinical variables are important determinants of access to each of these sectors. However, the study also emphasized the role of sociodemographic characteristics and access to care across every sector of care examined. In particular, the study indicated that those living in rural areas and those in older age groups do not have access to the same range of resources as those who are younger or living in metropolitan areas. Similarly, the findings suggest that those in lower socioeconomic groups do not have access to the same range of resources as those in higher socioeconomic groups, despite the attempts to redress this issue through the use of Medicare rebates for private psychiatrists. Whether or not the government's more recent initiatives to extend health insurance coverage to certain allied health professionals will improve this disparity is yet to be evaluated. It is also possible that the recent move to limit the number of reimbursed ‘per patient’ private psychiatrist consultations will increase access to these resources, but similarly, this is yet to be evaluated. The study also emphasizes the importance of understanding the ‘forgotten groups’ in the matrix of mental health care – those who access alternative practitioners or who consult medical but not mental health specialists. At a wider level, the analysis indicates that examining the health-care system from a broad perspective such as that offered by the PTC model can provide useful insights into the way in which each sector of care operates within the broader health-care matrix.
Footnotes
Acknowledgements
This study was supported by a contract from the Commonwealth Department of Health and Ageing, Australian Government, Canberra.