
Abstract
Background:
Although antipsychotic monotherapy is recommended as the main treatment for schizophrenia, antipsychotic polypharmacy is not rare in practice. However, longitudinal data on antipsychotic polypharmacy in schizophrenia treatment are limited.
Methods:
This longitudinal database study described antipsychotic polypharmacy in the treatment of schizophrenia in real-world settings in China and Japan. We retrieved information about antipsychotic treatment for schizophrenia from January 2010 to December 2014 from two hospital Electronic Medical Records databases in China and one claims database, Japan Medical Data Centre in Japan. Eligible patients had a diagnosis of schizophrenia (International Classification of Diseases, Tenth Revision F20.x) and at least one prescription for first or second generation antipsychotics. Antipsychotic polypharmacy was defined as having more than one antipsychotic medication overlapping for ⩾60 days. The Japan Medical Data Centre study cohort was further stratified by employees (insurance beneficiaries) and their dependents.
Results:
The study cohorts comprised 11,961 patients from China and 25,034 (10,661 employee sub-cohort and 14,373 dependent sub-cohort) from 14 days Japan Medical Data Centre in Japan. Most patients were prescribed monotherapy (87.3% in China and 80.1% in Japan), of which oral second-generation antipsychotics were the majority (78.9% in China and 65.8% in Japan). The prevalence rate of antipsychotic polypharmacy was 12.7% in China and 19.9% in Japan (13.7% in employees vs 24.5% in dependents). The most common combinations were two oral antipsychotics. Combinations of more than two drugs were uncommon in China (0.3%) but were prescribed for 5.3% of patients in Japan. Among patients treated with monotherapy, 12.6/100 person-years (11.8%) in China and 9.6/100 person-years (11.0%) in Japan switched to antipsychotic polypharmacy during follow-up. Younger patients were more likely to switch to antipsychotic polypharmacy than older patents in all study cohorts.
Conclusion:
The observed rates of antipsychotic polypharmacy ranged from 12.7% in China to 19.9% in Japan. Switching from monotherapy to antipsychotic polypharmacy was most likely to occur in younger patients with schizophrenia.
Introduction
Antipsychotic polypharmacy (APP) refers to the concurrent use of more than one antipsychotic medication. Although antipsychotic monotherapy is consistently recommended as the preferred treatment for schizophrenia in numerous treatment guidelines (Buchanan et al., 2010; Lehman et al., 2004; Moore et al., 2007), APP is common practice in modern psychiatry worldwide. APP is used clinically in patients with severe schizophrenia, particularly those with mania or with violent or aggressive behaviours, or to avoid side-effects resulting from high doses of a single drug (Jeon and Kim, 2017). APP may also be used in treatment-resistant schizophrenia as a combination of clozapine with an atypical antipsychotic, or as a combination of atypical antipsychotics in patients with clozapine resistance; although strong evidence supporting the effectiveness of these regimens is currently lacking (Galling et al., 2017).
Studies performed in multiple countries in various settings illustrate inconsistent patterns of APP over the past decades. Several database studies utilising health claims data in the United States reported APP prevalence rates from 4.6% to 23% (Ganguly et al., 2004; Kreyenbuhl et al., 2006; Leslie and Rosenheck, 2001; Morrato et al., 2007). APP prevalence rates reported from Asia were often higher, ranging from 17.8% to 51.7% (Chong et al., 2004; Hou et al., 2016; Ito et al., 2012; Kochi et al., 2017; Li et al., 2014; Sim et al., 2004a; Tsutsumi et al., 2011; Xiang et al., 2012). Most studies conducted in Asia were patient surveys or chart reviews. Only one study was conducted using community-based pharmacy data and reported the APP rate as 17.8% in Japan (Kochi et al., 2017). However, patient diagnoses were lacking in that database, making the rate non-specific for schizophrenia treatment. Systematic reviews of APP across multiple geographic regions between 1970 and 2009 showed a global median prevalence rate of 19.6% of patients receiving APP, with the highest rate in Asia (32%), where the rate of APP with three or more antipsychotics was also highest, followed by Europe (23%), while the lowest was in North America (16%) and Oceania (16.4%) (Gallego et al., 2012). This pattern has been consistent for the last four decades. A large-scale cross-sectional survey in East Asia showed variations in APP across countries, with the highest rate in Singapore (74%), followed by Japan (51.3%), Korea (40.6%) and mainland China (36.8%) (Ito et al., 2012).
Most of the publications to date reported cross-sectional approaches in which the design could not distinguish cross-tapering of different antipsychotics from actual combination therapy or patient interviews which might have been influenced by observational or recall biases. Only a few studies employed a longitudinal approach using large health claims databases and defined APP as concurrent overlapping of multiple antipsychotic agents for a specific duration (e.g. from 14 to 90 days) (Ganguly et al., 2004; Jaffe and Levine, 2003; Kreyenbuhl et al., 2006; Morrato et al., 2007; Tapp et al., 2003). None of these longitudinal studies were conducted in Asia. Longitudinal studies using large healthcare databases are becoming increasingly important in describing treatment patterns for many diseases, including schizophrenia. With promotion and implementation of the digitised development of healthcare information in Asia in recent decades, electronic medical record (EMR) and insurance claims databases provide rich resources for such longitudinal studies.
Objectives
We utilised three large electronic healthcare databases to estimate the prevalence and incidence rates of APP in schizophrenia treatment in China and Japan. We also described the occurrence of APP in different age groups, by gender and by calendar year. By using a longitudinal approach, we provide more precise estimates of APP occurrence compared to cross-sectional approaches used in previous publications.
Research design and methods
Data sources
This retrospective study used two independent EMR databases in China, and the Japan Medical Data Centre (JMDC) health insurance claims database in Japan. The Chinese databases were from two university-affiliated tertiary hospitals; one was a major mental health centre in Beijing, and the other was a major general hospital in Xi’an. Both hospitals provide open healthcare (no referral needed), including comprehensive inpatient care, outpatient visits, pharmacy, procedural and laboratory services for patients all over the country. The hospitals established their Hospital Information Systems (HIS) more than 10 years ago. Major clinical information was transferred from the HIS into an integrated EMR research database in each of these hospitals. The databases mainly consisted of patient ID, birth date, gender, visit date, diagnosis (inpatient and outpatient) with ICD-10 (International Classification of Diseases, Tenth Revision) coding, drug names with hospital coding, dispensing date, dispensing quantity and procedures. Patient information was de-identified independently by the hospital Information Technology departments. The study was approved by the independent review board in each of these hospitals.
JMDC offers a comprehensive database comprising claims data from people employed by middle-to-large size companies, and their dependents, up to 75 years of age, in the Japanese union-managed health insurance system. The JMDC database currently includes more than 3.7 million unique individuals and represents approximately 2.5% of the total population of Japan. Data elements captured by JMDC are similar to those in US claims databases. The JMDC data consist of health-insurance claims category, family ID, subscriber ID, year and month of visit, year and month of birth, gender, visit date, diagnosis with ICD-10 coding, drug ATC code, brand name and dispensing date. All data were anonymised and deidentified. Epidemiology research on anonymised data was exempted from the Ethical Guidelines from Epidemiology Research (Davis et al., 2015; Nakano and Shiosakai, 2014).
Study cohort
The base populations of this study were patients who had at least one diagnosis of schizophrenia (ICD-10 F20.x) within the study period, which was from January 2010 to December 2014. The study cohorts comprised patients with schizophrenia who had received continuous healthcare, and who had at least one full prescription (with at least a 30-day supply) of an antipsychotic medication within the study period. Continuous care was defined as patients having had at least three consecutive visits with at least 14 days in-between visits, and with no gap longer than 45 days. Each unique outpatient care date, a single hospitalisation or a pharmacy dispensing was considered as a visit. A single hospitalisation was counted from the admission date until the last discharge date with no gap of more than 3 days between a discharge date and the next admission date. Since the two study hospitals provide tertiary-level healthcare to large geographic areas in China, a sizable number of patients seek consultations or second opinions in these hospitals, but received major care from their local healthcare facilities. The ‘continuous care’ criterion was used to ensure that only those patients who intended to receive ongoing medical care from the same hospital were included, thereby allowing longitudinal follow-up information to be captured. In addition, an antipsychotic new-user sub-cohort was created within each study cohort for sensitivity analysis. New users were defined as patients who received healthcare services without evidence of use of an antipsychotic in the databases at least 60 days prior to the earliest identified antipsychotic medication.
Patients were followed up from the earliest visit date of the continuous care until a visit gap of more than 90 days occurred, until the last visit date or until the last hospital discharge date in the database, whichever was the latest.
Since JMDC is an employer-based claims database, insurance beneficiaries and their dependents may represent populations with different health status; the JMDC study cohort was further stratified by employee/dependent status.
Medications
Prescriptions of first generation and second generation antipsychotics (FGA and SGA, respectively) were retrieved from pharmacy records and coded using the hospital drug dictionaries in the Chinese EMR databases, or the ATC classification in the JMDC. The index date was the date of the first identified dispensing of an antipsychotic medication. Patients who switched to, or added, a new antipsychotic medication during follow-up were captured. APP was defined as having more than one antipsychotic medication overlapping for at least 60 days, as calculated from the drug dispensing dates. The APP definition of ⩾60 days was based on treatment guidelines (‘The Expert Consensus Guideline Series’, 1999). Other prescriptions for treatments for mental disorders categorised as antidepressants, mood stabilisers and antianxiety medications were also retrieved from the pharmacy records.
Statistical analyses
All analyses were conducted independently within each database, without pooling the three databases together. Patient demographic information, including gender and age at the index date, as well as diagnosis of mental disorders (ICD-10 code Fxx) at, or prior to, the index date, were described. Patterns of prescribing of SGA and FGA medications and their combinations were summarised. Prevalence rates of APP, which was defined as having begun with the earliest identified treatment, were estimated. Among patients who were on antipsychotic monotherapy, both cumulative incidence and incidence density rates of switching to APP were estimated and stratified by age and gender. Kaplan–Meier curves by age group were drawn to describe the occurrence of new APP, and log-rank tests were conducted to test for statistical differences and trends among age groups. Patients who had monotherapy throughout the follow-up were censored at the last visit date. Cumulative incidence and incidence density rates of switching to APP were also estimated in the new-user sub-cohorts as sensitivity analyses. All analyses were conducted using SAS 9.2 (SAS Institute Inc., Cary, North Carolina, USA).
Results
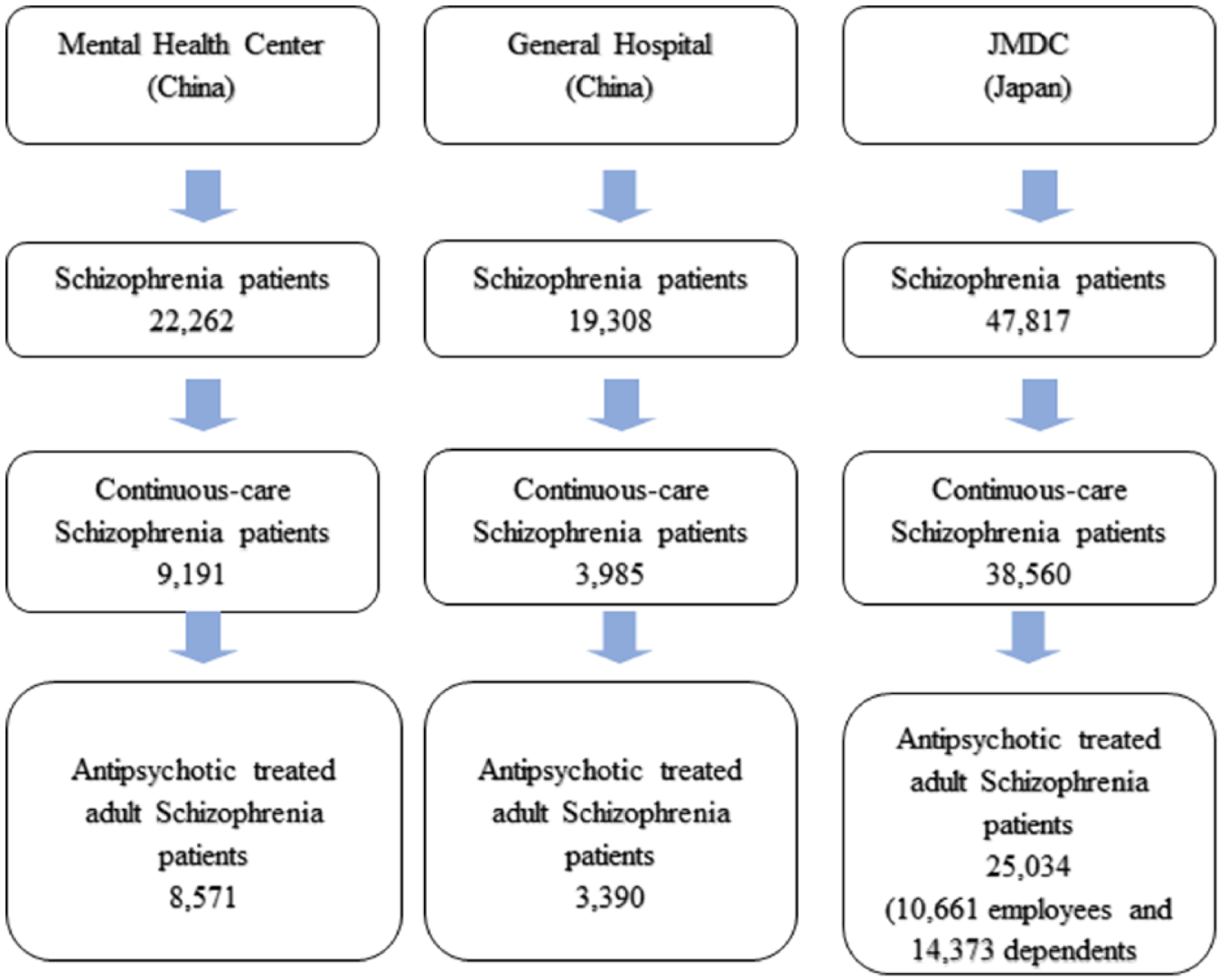
The flowchart of the study cohort generation is detailed in Figure 1. There were totals of 22,262 and 19,308 patients who had a diagnosis of schizophrenia in the mental health centre and the general hospital in China, respectively. Among these populations, 9191 and 3985 patients, respectively, were continuously seeking care at the study sites, of which 8571 and 3390 antipsychotic-treated patients were aged 15 years and older, comprising the main study cohorts from China. In JMDC, there were 47,817 schizophrenia patients identified, of whom 38,560 were patients with continuous care, and 25,034 of whom were 15 years and older, comprising the main study cohort from Japan. This cohort was further stratified by insurance beneficiary status as 10,661 (42.6%) employees and 14,373 (57.4%) dependents as sub-cohorts.
Study cohorts.
Demographic and clinical characteristics of patients included in the study cohorts are summarised in Table 1. The mean age of patients from the mental health centre in China was 38.6 (±17.4) years, and more than half (57.6%) were 15 to <40 years of age, while 10% were ⩾65 years of age. The cohort from the general hospital was younger, with mean age 28.6 (±12.5) years, of whom 82.8% were aged 15–<40 years, while 1.7% were ⩾65 years of age. The distribution between men and women was similar in both cohorts in China. The mean age of patients in the JMDC database was 39.0 (±13.5) years, and dependents (37.4 ± 14.9 years) were younger than employees (41.0 ± 10.9 years). Most (80.0%) of the patients in Japan were aged 25–<65 years and 3.5% were ⩾65 years of age. Although gender was evenly distributed overall in the JMDC cohort, the employee sub-cohort was composed of more men (78.0%) than women, whereas the dependent sub-cohort comprised more women (76.7%).
Demographic and cohort characteristics of patients with schizophrenia.
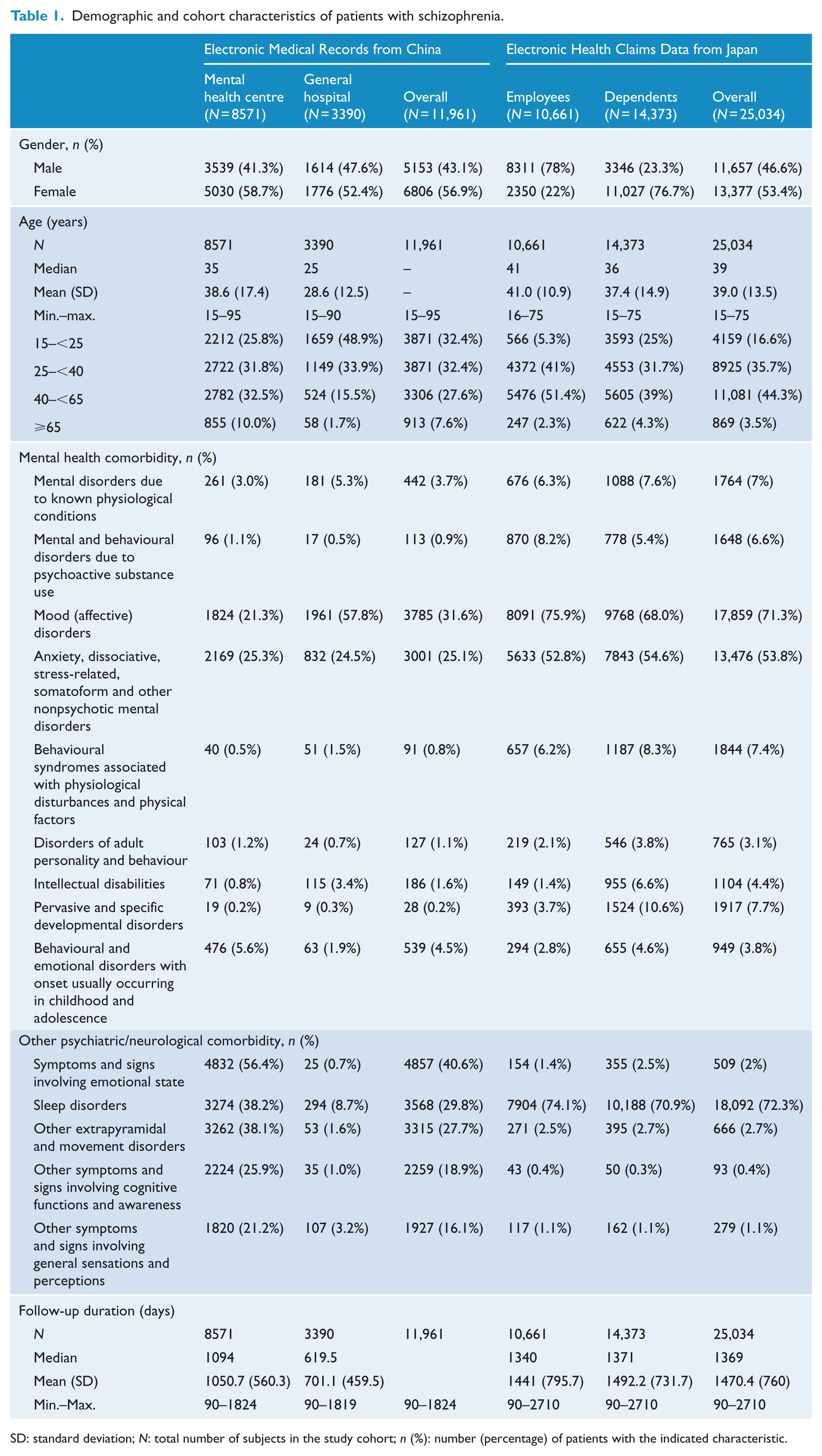
SD: standard deviation; N: total number of subjects in the study cohort; n (%): number (percentage) of patients with the indicated characteristic.
Psychiatric comorbidities most common in the Chinese mental health centre were emotional and mood disorders (56.4% with symptoms and signs involving emotional state and 21.3% with mood disorders), followed by sleep disorders (38.2%), other extrapyramidal and movement disorders (38.1%) and anxiety-related disorders (25.3%). In the Chinese general hospital, mood disorders were also common (57.8%), followed by anxiety-related disorders (24.5%), with only 8.7% having sleep disorders. In Japan, the most common psychiatric comorbidities were sleep disorders (72.3%) and mood disorders (71.3%), followed by anxiety-related disorders (53.8%). The study cohorts were followed up for an average of 1050.7 days (median: 1094 days), 701.1 days (median: 619.5 days) and 1470.4 days (median: 760 days) in the mental health centre, the general hospital and JMDC, respectively.
Table 2 describes the earliest identified antipsychotic treatment in each study cohort. Most patients were prescribed monotherapy (87.3% in China and 80.1% in Japan), of which oral SGA made up the majority (78.9% in China and 65.8% in Japan). Patients rarely initiated antipsychotic treatment with long-acting injectable (LAI) antipsychotics in either country. The prevalence rate of APP was 12.7% in China and 19.9% in Japan. In Japan, the APP rate was 13.7% in employees vs 24.5% in dependents. The most common combinations of antipsychotics in both countries were two oral SGA medications, or a combination of one oral SGA plus one oral FGA (Table 2). Combinations of more than two drugs were uncommon in China (0.3%), but were prescribed for 5.3% of patients in Japan (2.6% among employees and 7.3% among dependents). When stratifying the antipsychotic treatment by calendar year, the APP rates stayed stable across the 5-year span of the study in China. However, the rate of APP decreased in Japan from 25.1% in 2010 to 12.3% in 2014, with decreases observed in both the employee and dependent sub-cohorts.
Antipsychotic treatment regimen.
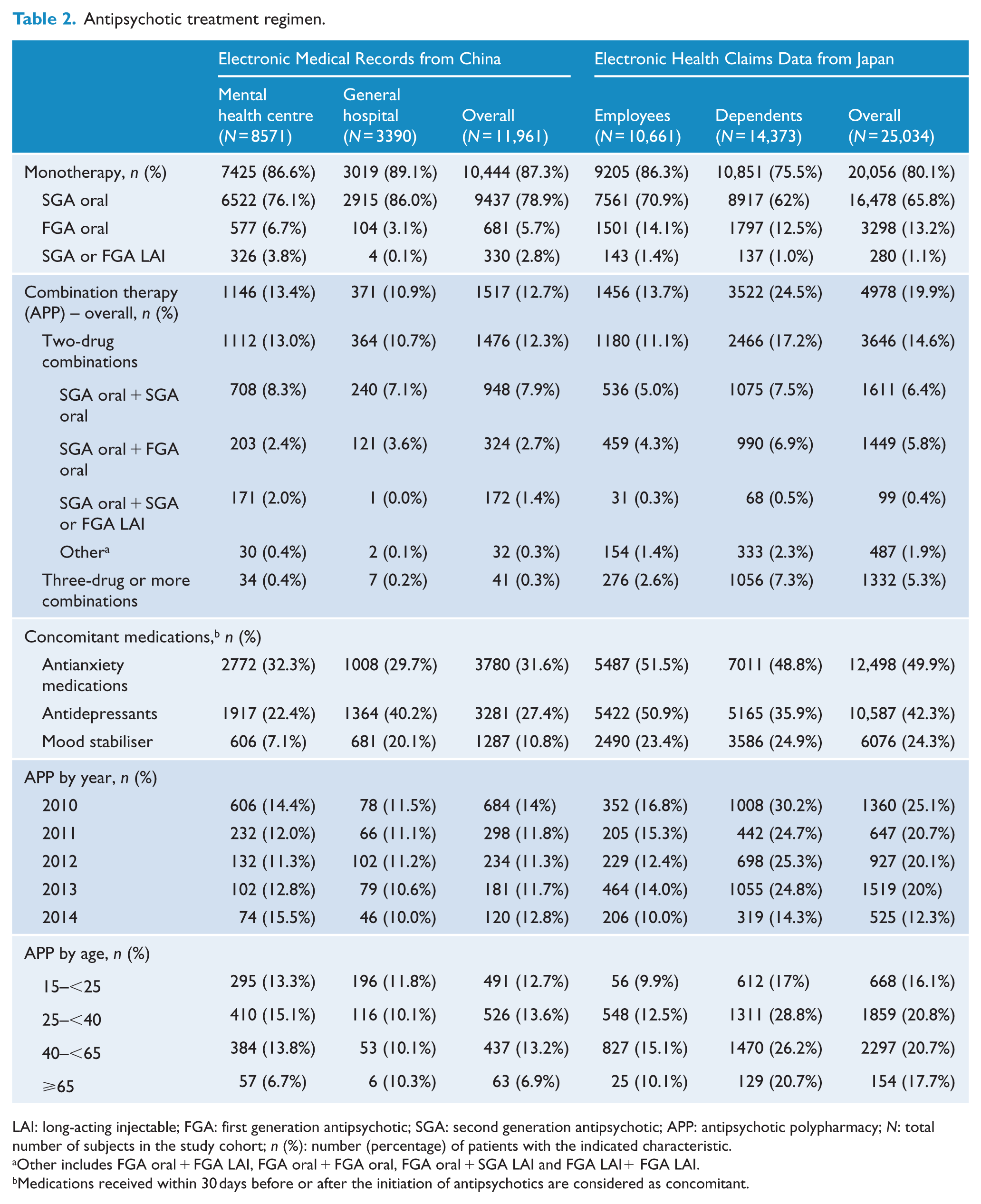
LAI: long-acting injectable; FGA: first generation antipsychotic; SGA: second generation antipsychotic; APP: antipsychotic polypharmacy; N: total number of subjects in the study cohort; n (%): number (percentage) of patients with the indicated characteristic.
Other includes FGA oral + FGA LAI, FGA oral + FGA oral, FGA oral + SGA LAI and FGA LAI+ FGA LAI.
Medications received within 30 days before or after the initiation of antipsychotics are considered as concomitant.
Among patients with antipsychotic monotherapy, 12.6/100 person-years (11.8%) in China and 9.6/100 person-years (11.0%) in Japan switched to APP during the study follow-up period (Table 3). Although the rate of switching to APP was higher in the general hospital (9.3%, 17.2/100 person-years) than in the mental health centre (12.8%, 11.7/100 person-years) in China, these rates in the two hospitals were almost identical within each age category while stratified by age. In Japan, the rate was higher in the dependents sub-cohort (13.2%, 11.3/100 person-years) than in the employee sub-cohort (8.4%, 7.7/100 person-years), even stratified by age. In both countries, the APP switching rates were similar in men and women, but appeared to depend significantly on age, with younger patients more likely to switch to APP than older patents in all study cohorts. Figure 2 shows Kaplan–Meier curves for each cohort of the time from the first identified monotherapy date, to switching to APP, stratified by age group. Log-rank tests yielded statistically significant differences and trends across age groups, with younger age groups switching to APP significantly more frequently than older age groups. Table 4 shows the sensitivity analyses of rates of switching to APP among antipsychotic new users. Within the much smaller sample sizes in these sub-cohorts, the estimated switching rates were not considerably changed and the inversed age dependence trends remained the same.
Cumulative incidence and incidence rate of patients on antipsychotic monotherapy who switched to antipsychotic polypharmacy.
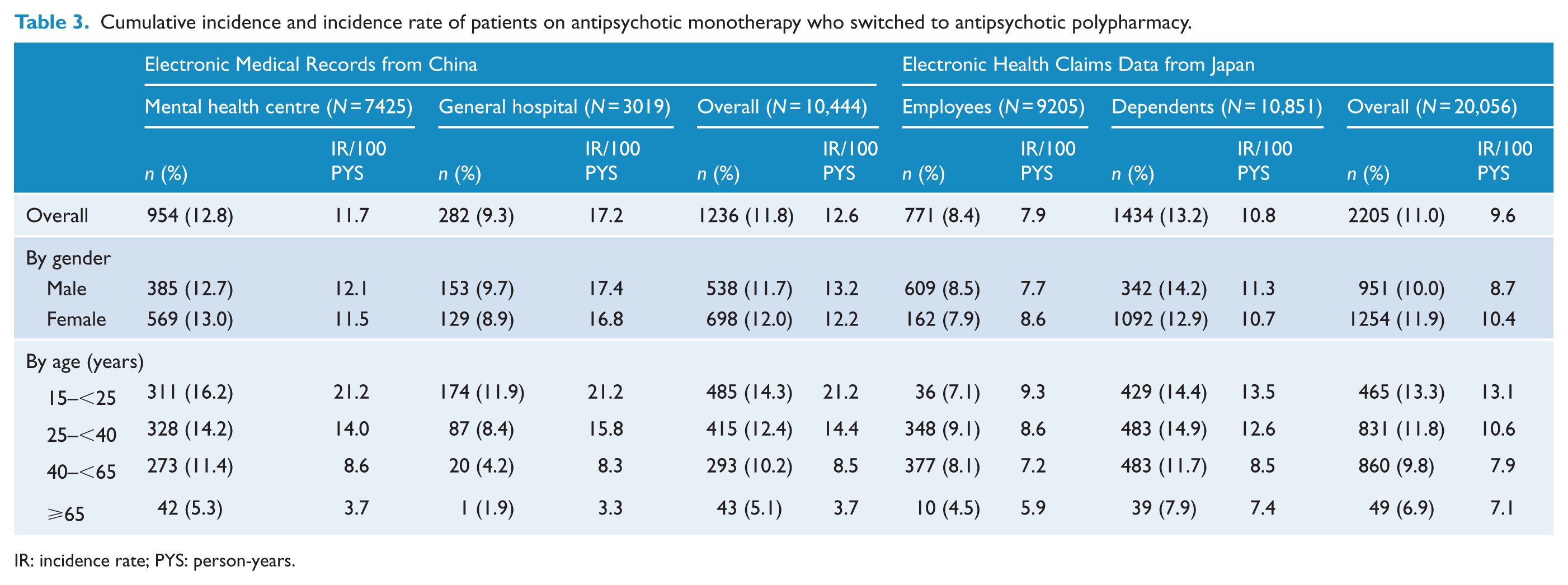
IR: incidence rate; PYS: person-years.
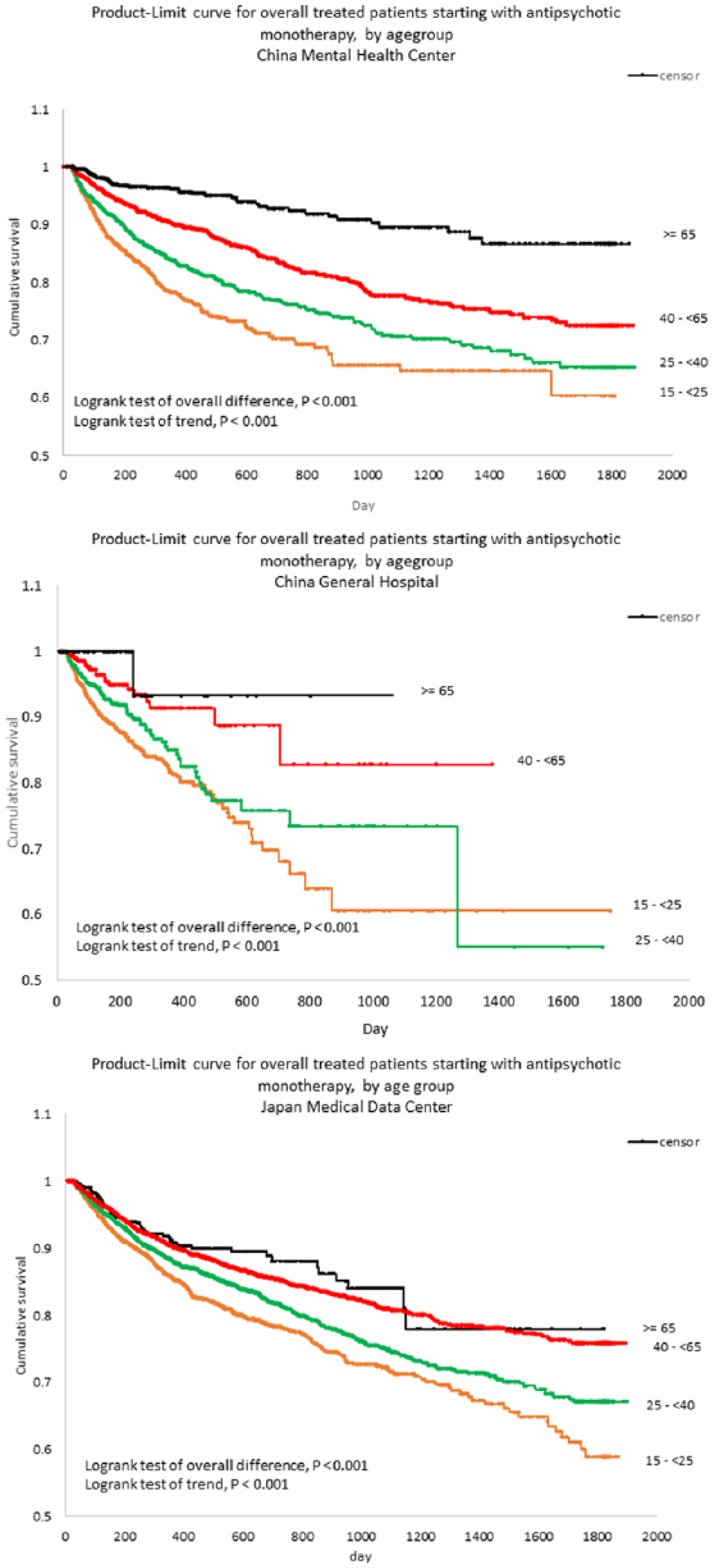
Time-to-switch to antipsychotic polypharmacy by age group.
Sensitivity analyses of cumulative incidence and incidence rate of patients on antipsychotic monotherapy who switched to antipsychotic polypharmacy – new-user sub-cohort.
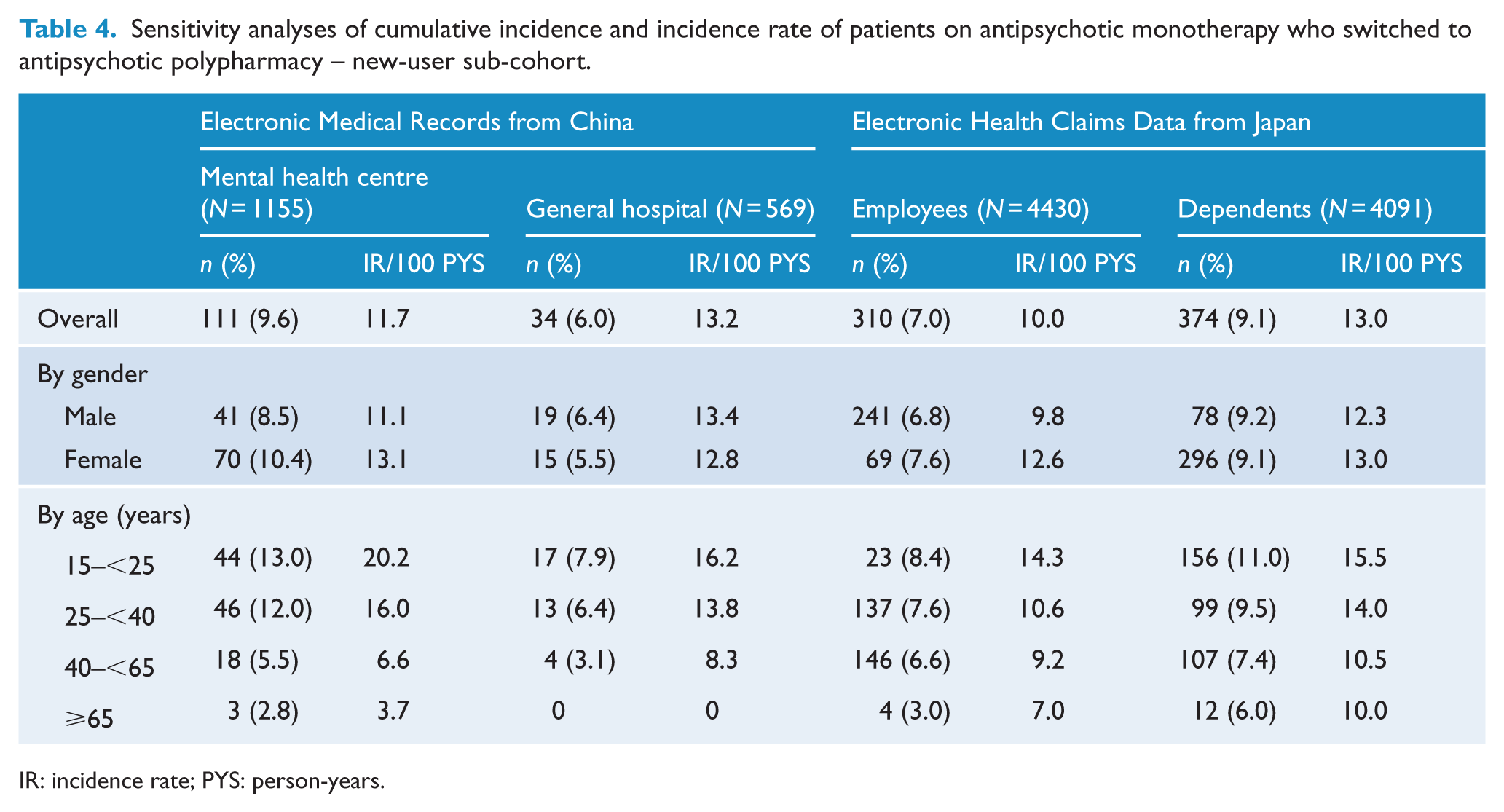
IR: incidence rate; PYS: person-years.
Discussion
To our knowledge, this is the first study to longitudinally assess APP rates and switching from antipsychotic monotherapy to APP among patients with schizophrenia in Asia. The overall prevalence rate of APP (mostly SGA + SGA or SGA + FGA) was 12.7% in China and 19.9% in Japan. Almost all (97.3%) patients with APP in China took combinations of two antipsychotic medications, whereas up to 5.3% of patients in Japan received three or more medications. We found that 12.6/100 person-years (11.8%) of patients in China and 9.6/100 person-years (11.0%) in Japan switched from monotherapy to APP. There was no difference in APP occurrence rates between men and women in any cohort. However, we observed significant association and trends between age and APP occurrence with more APP among younger than in older adults. Oral SGA medications were the dominant form of treatment among patients with schizophrenia in both countries. These findings of the age association with APP and the oral SGA dominant patterns of antipsychotic treatment are consistent with the results from recent publications from Asia (Kochi et al., 2017; Xiang et al., 2012).
In the 5-year study period, APP rates were the highest in the earliest year (2010) in both countries while remaining stable in China over the following years. The rate dropped to the lowest in the most recent year (2014) in Japan. The observed reduction in APP in Japan may have resulted from modifications to care in Japan following publications that reported high APP rates in Japan compared with other countries (Ito et al., 2012). The difference of APP switching rates between the mental health centre and the general hospital in China was confounded by the age of the cohorts. While stratified by age category, these rates were almost identical between the two hospitals within each stratum. Differences between employees and dependents in the JMDC database were evident; dependents had a higher prevalence of APP (24.5%) compared to employees (13.7%) and were more likely to be prescribed combinations of more than two antipsychotics (7.3%) than employees (2.6%). These differences might be explained by different severity and management of the underlying mental illness, given that employees with schizophrenia remained in the workforce, and were therefore more likely to have milder disease and better mental function.
APP prevalence rates from our study are lower than those reported previously from Asia (31%–51.6%) (Chong et al., 2004; Hou et al., 2016; Ito et al., 2012; Li et al., 2014; Sim et al., 2004a; Tsutsumi et al., 2011; Xiang et al., 2012). Most of the published studies were patient surveys or chart reviews with cross-sectional measurement of antipsychotic medication usage, in which APP rates might have been overestimated because transiently overlapping or cross-tapering medications were counted as APP. By contrast, our approach required a specified period (at least 60 days) of overlapping usage of multiple medications, which is more likely to capture true APP. To our knowledge, there has only been one recent publication in Asia where antipsychotic use was measured longitudinally. This study used a large pharmacy database in Japan with a cohort of 152,592 patients from 2006 to 2012 (Kochi et al., 2017). In this study, the prevalence rate of APP was 17.8% in adults (18–64 years of age) and 6.4% in older adults (⩾65 years), which is similar to our results. Within limited publications of longitudinal measurement from the United States, reported APP rates ranged from 9.5% to 23% (Ganguly et al., 2004; Kreyenbuhl et al., 2006; Morrato et al., 2007; Tapp et al., 2003), which encompasses the range of our results. Data from Australia indicate higher rates of APP than we observed. A national survey of psychosis in Australia identified APP in 28.1% of patients with schizophrenia (Waterreus et al., 2012). A study of hospitalised patients with schizophrenia found the prevalence of APP was 43.2% (John et al., 2014). This study found no association between APP use and age, gender, diagnosis or treating physician. Patients with schizophrenia on APP were taking similar doses of individual antipsychotics to patients receiving the same drug as monotherapy, suggesting that dose reduction of individual antipsychotics was not a common reason for introducing APP (John and Dragovic, 2015).
As antipsychotic treatment guidelines recognise that short-term (cross-tapering) and as needed (p.r.n.) use for symptom control are valid reasons for polypharmacy (Galletly et al., 2016; ‘The Expert Consensus Guideline Series’, 1999), only prolonged APP (recommended as ⩾60 days) raises concerns in actual practice due to the risk of adverse events. A longitudinal approach is therefore critical in studying APP practice in psychiatric care.
Among those patients prescribed antipsychotic monotherapy, younger age was statistically significantly associated with a switch to APP. This relationship with age is likely due to the different characteristics of schizophrenia at different ages. Younger patients are more likely to be newly diagnosed and may be more likely to have their antipsychotic treatments adjusted to achieve early symptom control. By contrast, older patients may be more likely to be clinically stable and on a longer term maintenance therapy. Switching to APP in older patients might be due to additional events or treatment resistance/intolerability which are quite different from early symptom control for younger patients. The inverse relationship between age and APP was also reported in several US studies (Jaffe and Levine, 2003; Kreyenbuhl et al., 2006; Morrato et al., 2007).
Contrary to global trends, there were more women than men with schizophrenia in the China databases. This is consistent with previous studies in China showing a higher prevalence of schizophrenia among women than men, particularly in rural areas (Liu et al., 2015; Phillips, 2001). The cause of this reversal among men and women is not fully understood, but could be related to differences in the social and economic outlook for women living in rural China (Liu et al., 2015; Pearson, 1995; Phillips, 2001).
We observed a low rate of depot usage, but high rates of prescribing of other drugs in both China and Japan. Previous studies have shown depot prescribing rates between 5.9% and 6.5% in both countries (Si et al., 2011; Sim et al., 2004b). In one study, the authors noted that depot usage was likely to be strongly influenced by local traditions and prescription culture (Sim et al., 2004b), which could have influenced prescribing rates in our study.
We observed prescribing rates of mood stabilisers and anti-anxiety medications that were within the range reported previously for hospitalised patients with schizophrenia in Asia (Sim et al., 2011; Tor et al., 2011). However, the prescribing rate of antidepressant prescriptions, although similar in Japan and China, was higher in our study than previously reported (Li et al., 2017; Xiang et al., 2013). A study conducted between 2002 and 2012 in China noted a significant increase in antidepressant prescribing between 2006 and 2012 (Li et al., 2017). Thus, while we have no clear explanation why the rate of antidepressant prescribing in our study is substantially higher than reported previously, it may reflect a decade of increasing use.
The strengths of this study include the use of three large electronic healthcare databases from China and Japan and has high internal validity due to the large sample sizes and long duration of follow-up, which enabled longitudinal analysis of antipsychotic medication use among patients with schizophrenia. In China, integrated services within the hospital setting allowed for data links between outpatient, inpatient, pharmacy and other healthcare services within each hospital. The insurance claims data from Japan captured overall healthcare encounters for patients enrolled in the insurance plan. All of the data were collected through routine practice, which was not biased by any specific research protocol. These strengths of the study ensure that the results reasonably reflect the real-world treatment patterns of patients with schizophrenia in these countries.
Potential limitations of the study are that the main analysis cohorts included both prevalent users and incident users of antipsychotic medications; thus, treatment patterns might be left truncated for certain patients with a long history of disease. However, the similar person-time analyses results from the sensitivity analyses in the new-user sub-cohorts showed that this bias may not be significant, although the limited sample sizes in these sub-cohorts prevented further comparative analyses among age groups. The study only included a small population of the patients with schizophrenia in China and Japan. The results from China could reflect local practices at the study hospitals, which are tertiary medical school–affiliated hospitals with high standards of care. However, consistent results from two different settings (a mental health specialty hospital and a general hospital psychiatric department) in different geographic areas (first tier city and second tier city) provide confidence in the external validity of the results. The JMDC data cover employees from medium to large size companies and their dependents in Japan. Patients with schizophrenia remaining in the workforce can be assumed to have less severe disease than the general schizophrenia population. The dependents with schizophrenia, who were covered by the employee’s insurance benefit, might be under better care (family and social support) with better function than the general schizophrenia population. The generalizability of the results needs to be examined through replication analyses in other settings and using other data sources. Finally, coding of the diagnosis of psychosis may not exactly reflect clinically and systematically verified definitions. However, schizophrenia is a severe and lifelong disease. Registration of schizophrenia is required in China and it thus unlikely to be miscoded in the system. An additional potential limitation is the differences in databases (EMR vs claims) and completeness and standardisation of data capture.
APP is in common practice worldwide, including Asia. Further research to describe the most common antipsychotic drug combinations, the rationale for their use and associated benefits and adverse events could provide important insights into real-world practice in managing patients with schizophrenia. Such data could inform high-quality studies to evaluate the benefits vs risks of specific drug combinations in patients with schizophrenia.
This retrospective database study showed that contrary to previous conclusions, APP rates in China and Japan were not higher than those in the United States. Although no other longitudinal measurements are available from China to confirm our findings, the only database study recently published from Japan showed similar APP rates to our results (Kochi et al., 2017). Switching from monotherapy to APP was most likely to occur in younger patients.
Footnotes
Acknowledgements
The authors thank Joanne Wolter for English language polishing of the submitted work.
Declaration of Conflicting Interests
H.Q., Y.Z. and M.H, are employees of Janssen Research & Development LLC which manufactures and markets risperidone and paliperidone. H.Q., Y.Z. and M.H also report stock ownership in Johnson & Johnson Pte Ltd. Other authors declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Beijing Municipal Science and Technology Commission (D171100007017002) and was based on research collaboration among Peking University Sixth Hospital (Beijing, China), Xijing Hospital (Xi’an, China) and Janssen Research and Development (Titusville, New Jersey, USA).