
Abstract
Objective:
We aimed to map the prevalence and predictors of psychological outcomes in affected communities 3–4 years after the Black Saturday bushfires in the state of Victoria, Australia.
Methods:
Baseline assessment of a longitudinal cohort study in high-, medium-, and low-affected communities in Victoria. Participants included 1017 residents of high-, medium-, and low-affected fire communities. Participants were surveyed by means of a telephone and web-based interview between December 2011 and January 2013. The survey included measures of fire-related post-traumatic stress disorder (PTSD) and general PTSD from other traumatic events, major depressive episode, alcohol use, and general psychological distress.
Results:
The majority of respondents in the high- (77.3%), medium- (81.3%), and low-affected (84.9%) communities reported no psychological distress on the K6 screening scale. More participants in the high-affected communities (15.6%) reported probable PTSD linked to the bushfires than medium- (7.2%) and low-affected (1.0%) communities (odds ratio (OR): 4.57, 95% confidence interval (CI): 2.61–8.00, p = 0.000). Similar patterns were observed for depression (12.9%, 8.8%, 6.3%, respectively) (OR: 1.83, 95% CI: 1.17–2.85, p = 0.008) and severe psychological distress (9.8%, 5.0%, 4.9%, respectively) (OR: 2.08, 95% CI: 1.23–3.55, p = 0.007). All communities reported elevated rates of heavy drinking (24.7%, 18.7%, 19.6%, respectively); however, these were higher in the high-affected communities (OR: 1.39, 95% CI: 1.01–1.89, p = 0.04). Severe psychological distress was predicted by fear for one’s life in the bushfires, death of someone close to them in the bushfires, and subsequent stressors. One-third of those with severe psychological distress did not receive mental health assistance in the previous month.
Conclusions:
Several years following the Black Saturday bushfires the majority of affected people demonstrated resilience without indications of psychological distress. A significant minority of people in the high-affected communities reported persistent PTSD, depression, and psychological distress, indicating the need for promotion of the use of health and complementary services, community-based initiatives, and family and other informal supports, to target these persistent problems.
Introduction
In February 2009, Australia suffered one of its worst natural disasters as severe bushfires swept through most of the state of Victoria, with the worst bushfires occurring on Saturday, 7 February. Commonly referred to as the ‘Black Saturday’ bushfires, this disaster resulted in 173 fatalities, 3500 buildings damaged or destroyed, and massive adverse impact on community infrastructures (Victorian Bushfires Royal Commission, 2009). Over the recent decades, much research has attested to the effects of disasters on the psychological outcomes of those who survive them (Norris et al., 2002a, 2002b). Many studies have highlighted the onset of stress-related problems, including post-traumatic stress disorder (PTSD) and depression (Norris et al., 2002a). Australia has a long psychiatric tradition of managing natural disasters. Arguably, one of the largest disasters prior to Black Saturday were the Ash Wednesday bushfires in 1983. In the aftermath of these bushfires, two studies (McFarlane 1988; McFarlane et al., 1997) reported that 42% of affected people were distressed 1 year later relative to 23% of unaffected people. In a 20-year follow-up of children affected by these bushfires, McFarlane and Van Hooff (2009) found that children had higher rates of psychological disturbance than adults; however, this was not directly the result of exposure to the disaster. Another study screened primary school children 6 months after the bushfires and found that 12% showed severe emotional distress (McDermott and Palmer, 1999). Following the 2003 Canberra bushfires, people who had previously participated in a community-based longitudinal study were assessed; whereas poorer mental health and neuroticism prior to the bushfires predicted a poor outcome, these factors were less influential than being evacuated and being distressed by the threat of fire (Parslow et al., 2006).
One pattern following traumatic events is for people to experience distress in the period immediately after exposure to the trauma, and then experience improved psychological health as time progresses (Galea et al., 2003). The convergent finding from earlier Australian studies (McFarlane, 1988; McFarlane et al., 1997; Parslow et al., 2006), as well as international studies (Bonanno, 2004), is that the majority of people are resilient following a disaster. Underscoring the trend for most people to be resilient, studies of those affected by more prolonged hardship, such as the Australian drought, found that people typically manage despite adversity (Greenhill et al., 2009).
In contrast, there is also evidence that following natural disasters that cause massive infrastructure damage, the lingering effects of the disaster may not abate so readily. For example, following Hurricane Katrina, PTSD rates increased from 15% 5–8 months after the disaster to 20% a year later (Kessler et al., 2008). The observation that up to 25% of people with PTSD may have developed it at least 6 months after the trauma underscores the conclusion that PTSD can worsen over time (Andrews et al., 2007). The complexity of post-traumatic adjustment has also been highlighted by longitudinal assessments that have found that people experience fluctuating PTSD symptoms at various points in the course of time following trauma exposure (Bryant et al., 2013). This pattern underscores the need for longer-term follow-up assessments of natural disasters to inform policymakers concerning initiatives that may be required to promote resilience following disasters.
Accordingly, in response to the Black Saturday bushfires, we started a large-scale survey of community and individual responses to the disaster and to subsequent developments (Gibbs et al., 2013). Overall, this programme represents a multi-method, longitudinal analysis of social connectedness and individual psychological outcomes. It is particularly important to map the longer-term mental health status of affected communities following disasters because although mental health services were active in the aftermath of earlier disasters, as evidenced by activity following the Ash Wednesday bushfires in 1983 (Berah et al., 1984; Valent, 1984), service provision has considerably changed in more recent times, including the manner in which it was made available to the survivors of Black Saturday. Specifically, the state and federal governments implemented structured programmes targeting all affected areas and provided significant training to health providers to ensure they were skilled in post-traumatic mental health provision (Forbes et al., 2010). The aims of this article were to (a) report on the psychological status of the respondents 3–4 years after the bushfires, and (b) identify the key predictors of psychological outcomes at this point.
Methods
Participants
This study focused on adults (aged ≥ 18 years) living in 25 communities in 10 locations in the state of Victoria; these communities were selected because they were variably affected by the bushfires, ranging from a high level of impact in terms of lives lost and property destroyed through to communities with minimal impact. We defined communities as high-impact (operationalised as ‘many houses lost plus fatalities’; N = 630), medium-impact (operationalised as ‘upper end of range may include a small number of fatalities through to communities with no fatalities but significant amount of property damage’; N = 182), and low-impact (operationalised as ‘no evidence of fires being present’; N = 205). The 2006 census data indicated a total adult population of 7693 in the selected communities, including 702 adults in the two pilot communities. The Victorian Electoral Commission (VEC) provided contact details of both current residents and those who had relocated since the bushfires (N = 7467 adults); a letter, including a reply-paid envelope, was sent to them to invite them to participate in the study. In terms of the people who were eligible to take part in this study, 16% eventually participated and completed the survey. Relative to the available census data, the sample who participated in this study were disproportionately older, female, and better educated than the general community. Following piloting of the recruitment and data collection methods, a personalised letter of invitation to be sent to the adults in this sample was approved by the VEC. Additional community awareness activities, mailbox drops, area-based phone calls, news media and social media activities were also conducted to increase awareness of the study and the methods for registration.
Full details of respondent characteristics according to affected community status are presented in Table 1. Only respondents who were resident in the selected communities at the time of the bushfires are included in analyses.
Participant characteristics according to affected community status.
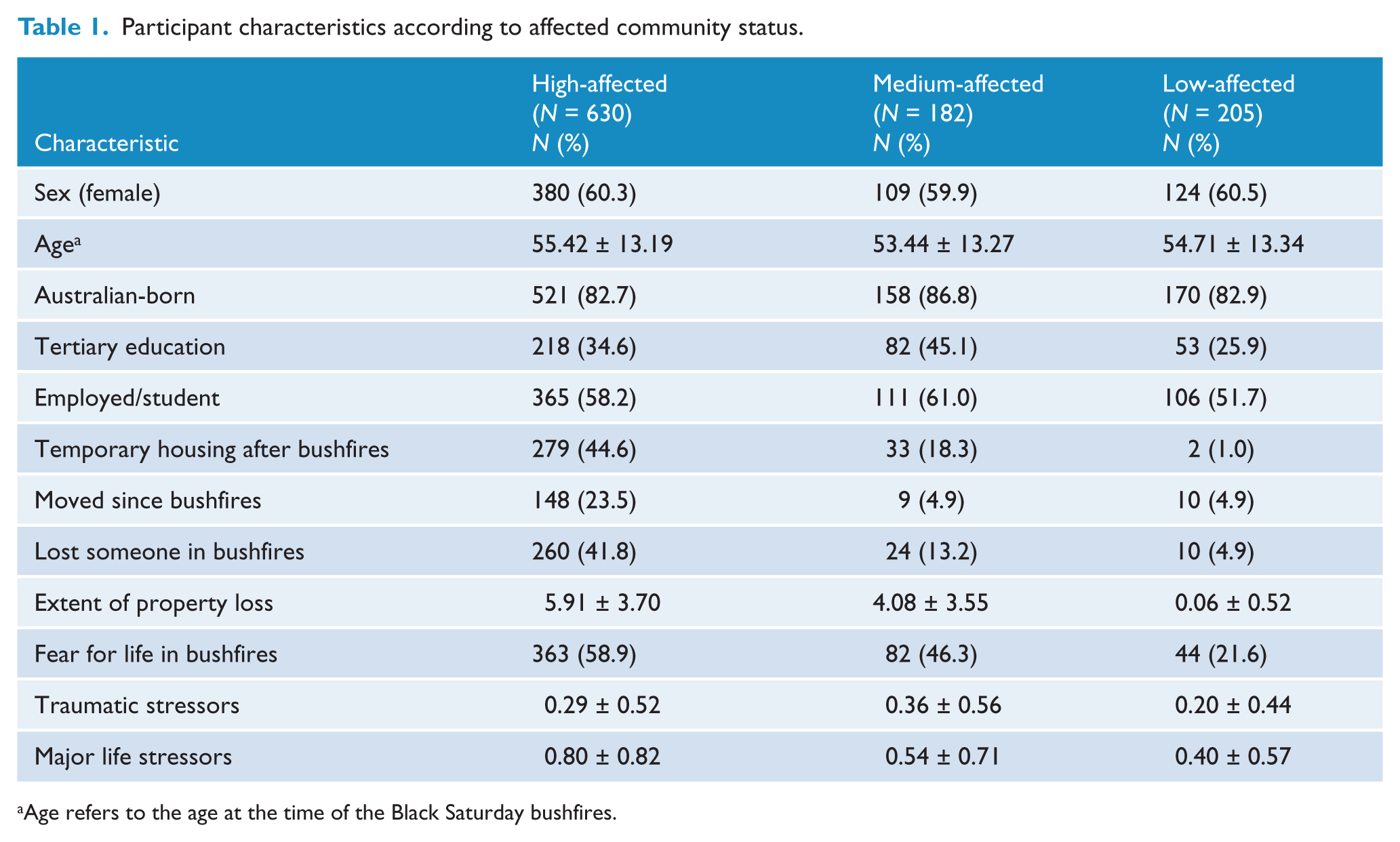
Age refers to the age at the time of the Black Saturday bushfires.
Measures
Post-traumatic stress disorder
Probable PTSD was assessed using an abbreviated version of the PTSD Checklist (PCL) (Bliese et al., 2008), which comprises four items, each scored on a 5-point severity scale, that index key symptoms of PTSD and refers to the previous 4 weeks. Adopting a cut-off score of 7 on the abbreviated PCL achieves an efficient estimation of PTSD diagnosis relative to the full version of the PCL (Bliese et al., 2008). We assessed PTSD in two ways: responses that were specific to the Black Saturday bushfires and responses to traumatic events generally.
Depression
Probable major depressive episode (MDE) was assessed using the Patient Health Questionnaire (PHQ). The PHQ-9 is the depression module of the PHQ which scores each of the nine depression criteria listed in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (Kroenke et al., 2001). Major depressive episode was diagnosed if five of the nine symptoms had been present for most days in the previous 2 weeks.
Psychological distress
The K6 scale indexes non-specific psychological distress; it assesses anxiety-mood disorders by indexing symptoms in the past month (Kessler et al., 2003). According to the Substance Abuse and Mental Health Services Administration’s definition of severe mental illness (SMI), K6 scores of 0–7 were classified as no mental illness, 8–12 as mild–moderate mental illness, and 13–24 as probable SMI (Kessler et al., 2008). In this study, psychological resilience was defined as K6 scores of 0–6, reflecting people who experienced no or minimal psychological problems. In addition, the K6 asks how often in the past 30 days the person saw a health professional about the problems reported on the K6.
Alcohol use
Heavy drinking was indexed using the alcohol consumption questions of the Alcohol Use Disorder Identification Test (AUDIT-C) (Bush et al., 1998), a 3-item self-report measure that indexes heavy drinking. This scale is an abbreviated version of the AUDIT, which is the most commonly used measure of alcohol abuse; the AUDIT-C employs the initial three questions of the AUDIT, which index the degree of alcohol consumption rather than the adverse effects of alcohol use. Using previous cut-offs recommended for identifying heavy drinking in community samples, we adopted a cut-off of 6 for men and 5 for women as the most effective detection of heavy drinking; these cut-offs have sound sensitivity (men: 0.82; women: 0.84) and specificity (men: 0.79; women: 0.88) (Aalto et al., 2009) with heavy/binge drinking as defined by the timeline followback interview for alcohol consumption (Sobell and Sobell, 1996).
Fire-related experiences
The interview indexed a wide range of events that occurred on the day of the bushfires. Relevant to this study, we indexed (a) whether the respondent had feared for their own life, (b) whether anyone close to the respondent had died in the bushfires, and (c) whether they personally lost property or buildings in the bushfires. These questions were asked to obtain an index of degree of direct exposure to the bushfires.
Post-fire traumatic events
As part of the interview, participants were asked to indicate whether they had been exposed to any of the following and potentially traumatic events: (a) natural disaster, (b) serious accident, and (c) serious assault/violence. They were also asked if they had experienced major life stressors in the form of disruptions to their (a) income, (b) accommodation, or (c) personal relationships.
Procedure
The study was approved by the University of Melbourne Human Research Ethics Committee. Baseline data collection was piloted in late 2011, and then full data collection occurred between December 2011 and January 2013. Prior to commencement of data collection, considerable engagement occurred between the research team and the community representatives and members, as well as major stakeholders in the post-disaster recovery, to establish ongoing collaborations and to support local engagement in the study, knowledge exchange, and information dissemination. The interview was conducted by a combination of telephone and web-based formats. Following an introduction to the study and after obtaining informed consent, the interviewer initially asked socio-demographic questions, followed by social connection questions, and questions on physical health, events that occurred on the day of the Black Saturday bushfires, and traumatic events that may have occurred since the bushfires. Relevant to the current analyses, the interview sequentially administered the abbreviated PCL, PHQ-9, K6, and AUDIT-C, and ended with questions about life satisfaction and community attachment.
Statistical analyses
Prevalence rates were initially calculated based on the recommended cut-offs for PTSD, MDE, heavy drinking, and SMI. To assess the predictors of psychological outcomes, separate logistic regressions were conducted to predict case cut-offs of general PTSD, fire-related PTSD, depression, SMI, and heavy drinking. In each regression, sex, age at the time of the Black Saturday bushfires, and highest level of education were entered at step 1. Factors that reflected the severity of fire exposure were entered at step 2, including whether the respondent had feared for their own life, whether someone close to the respondent had died in the bushfires, and the extent of property loss. Finally, at step 3 traumatic and major life stressors were entered to index the additional effects of subsequent adversity on psychological outcomes.
Results
Participant characteristics
Participants did not differ between the three levels of affected communities in terms of sex, age, country of birth, or employment status. Fewer participants in the low-affected communities had tertiary education than those in the medium- and high-affected communities (odds ratio (OR): 1.68, 95% confidence interval (CI): 1.20–2.38, p = 0.003). Participants in the high-affected communities were more likely to report temporary housing following the bushfires (OR: 8.02, 95% CI: 5.47–11.74, p = 0.000), having moved since the bushfires (OR: 5.95, 95% CI: 3.62–9.77, p = 0.000), fearing for the their lives during the bushfires (OR: 2.90, 95% CI: 2.22–3.79, p = 0.000), and having lost someone in the bushfires (OR: 7.42, 95% CI: 5.04–10.91, p = 0.000). Participants in the high-affected communities also reported more property loss (t (907.27) = 18.16, p = 0.000), and major life stressors (t (957.79) = 7.32, p = 0.000) since the bushfires than the other communities. Participants from the low-affected communities reported fewer traumatic stressors (t (431.96) = 7.16, p = 0.000) than the other communities.
Prevalence of psychological outcomes
Table 2 presents the frequencies of reported probable PTSD, MDE, heavy drinking, and levels of mental illness according to the level of exposure to the bushfires. In terms of PTSD linked to the Black Saturday bushfires, more participants in the high-affected communities reported probable PTSD (15.6%) than those from the medium- (7.2%) and low-affected (1.0%) communities (OR: 4.57, 95% CI: 2.61–8.00, p = 0.000). A similar pattern was observed regarding general PTSD from any traumatic event, with more participants in the high-affected communities reporting probable PTSD (21.7%) than participants in the medium- (13.8%) and low-affected (8.8%) communities (OR: 2.21, 95% CI: 1.53–3.20, p = 0.000). Similarly, participants in the high-affected communities were more likely to report MDE (12.9%) than participants in the medium- (8.8%) and low-affected communities (6.3%) (OR: 1.83, 95% CI: 1.17–2.85, p = 0.008). Consistent with these findings, participants in the high-affected communities were also more likely to report SMI (9.8%) than participants in the medium- (5.0%) and low-affected communities (4.9%) (OR: 2.08, 95% CI: 1.23–3.55, p = 0.007). Finally, more participants reported heavy drinking in the high-affected communities than in the other communities (high-affected: 24.7%; medium-affected: 18.7%; low-affected: 19.6%) (OR: 1.39, 95% CI: 1.01–1.89, p = 0.04). Overall, the rates of people suffering any disorder (including SMI) was 43.1% in the high-affected, 33.3% in the medium-affected, and 27.5% in the low-affected communities; those living in high-affected communities were more likely to have any disorder than those in the other communities (OR: 1.75, 95% CI: 1.33–2.29, p = 0.000).
Prevalence of mental health conditions across communities.
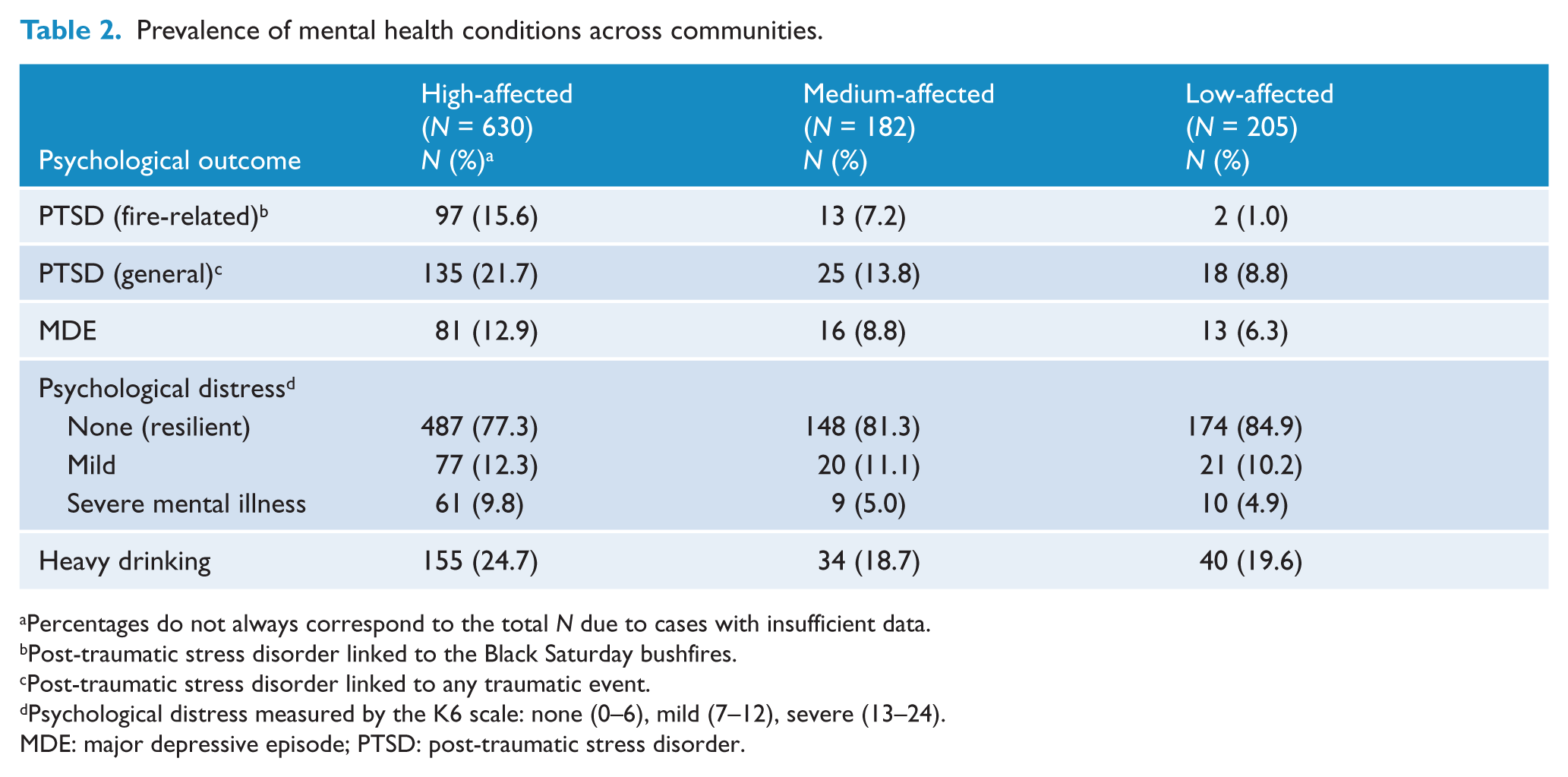
Percentages do not always correspond to the total N due to cases with insufficient data.
Post-traumatic stress disorder linked to the Black Saturday bushfires.
Post-traumatic stress disorder linked to any traumatic event.
Psychological distress measured by the K6 scale: none (0–6), mild (7–12), severe (13–24).
MDE: major depressive episode; PTSD: post-traumatic stress disorder.
Resilience rates
Consistent with prevailing definitions of resilience as the absence of persistent psychological distress (as distinct from the absence of mental disorder) (Bonanno, 2004), we operationalised resilience as scores of 0–6 on the K6 scale (Kessler et al., 2008). On this metric, fewer people in the high-affected communities reported being resilient than those in the medium and low-affected areas (OR: 0.59, 95% CI: 0.43–0.81, p = 0.001) (see Table 2). It should be noted, however, that the majority of people in each level of affected community were resilient.
Sex and psychological outcomes
Table 3 presents the rates of psychological outcomes according to sex. Women (13.0%) were significantly more likely to develop PTSD linked to the bushfires than men (8.2%) (OR: 1.68, 95% CI: 1.09–2.57, p = 0.02), and PTSD linked to general trauma (not limited to the bushfires) (20.0% vs. 14.2%) (OR: 1.51, 95% CI: 1.07–2.13, p = 0.02). In contrast, men (28.2%) were significantly more likely to experience heavy drinking than women (18.9%) (OR: 0.59, 95% CI: 0.44–0.80, p = 0.001). Men and women reported comparable level of SMI, resilience, and depression.
Prevalence of mental health conditions according to sex.
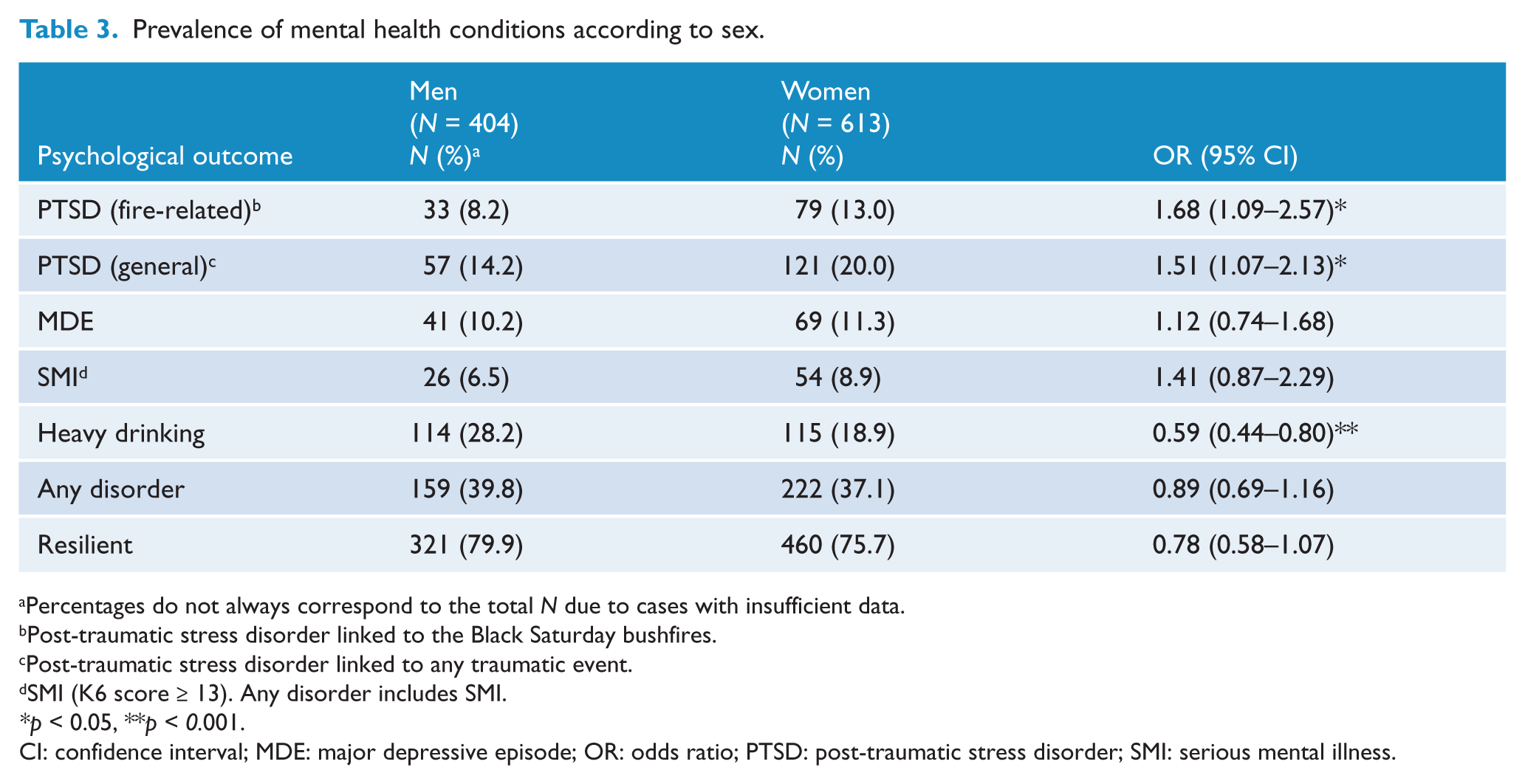
Percentages do not always correspond to the total N due to cases with insufficient data.
Post-traumatic stress disorder linked to the Black Saturday bushfires.
Post-traumatic stress disorder linked to any traumatic event.
SMI (K6 score ≥ 13). Any disorder includes SMI.
p < 0.05, **p < 0.001.
CI: confidence interval; MDE: major depressive episode; OR: odds ratio; PTSD: post-traumatic stress disorder; SMI: serious mental illness.
Help-seeking patterns
In terms of respondents who reported SMI, only 50 (63.3%) had received mental health assistance in the previous month. That is, one-third of those with very severe distress did not consult any health or related professional in this period for mental health assistance. In terms of the sex of those with SMI, there was a marginal trend for more men to attend treatment (76.9%) than women (56.6%) (OR: 0.39, 95% CI: 0.14–1.13, p = 0.08).
Predictors of psychological outcomes
Table 4 presents the adjusted ORs for PTSD (general and fire-related), MDE, heavy drinking, and psychological distress. General PTSD was predicted by fear for one’s life, death of someone in the bushfires, and subsequent major life and traumatic events since the bushfires. PTSD arising from the bushfires was predicted by female sex, lower educational level, death of someone in the bushfires, property loss, fear for one’s life, and subsequent major life stressors. Both MDE and SMI were predicted by the death of someone in the bushfires, fear for one’s life, and subsequent major life stressors. Heavy drinking was predicted by male sex and younger age.
The effects of socio-demographic factors, fire exposure, and post-fire stressors on psychological outcomes.
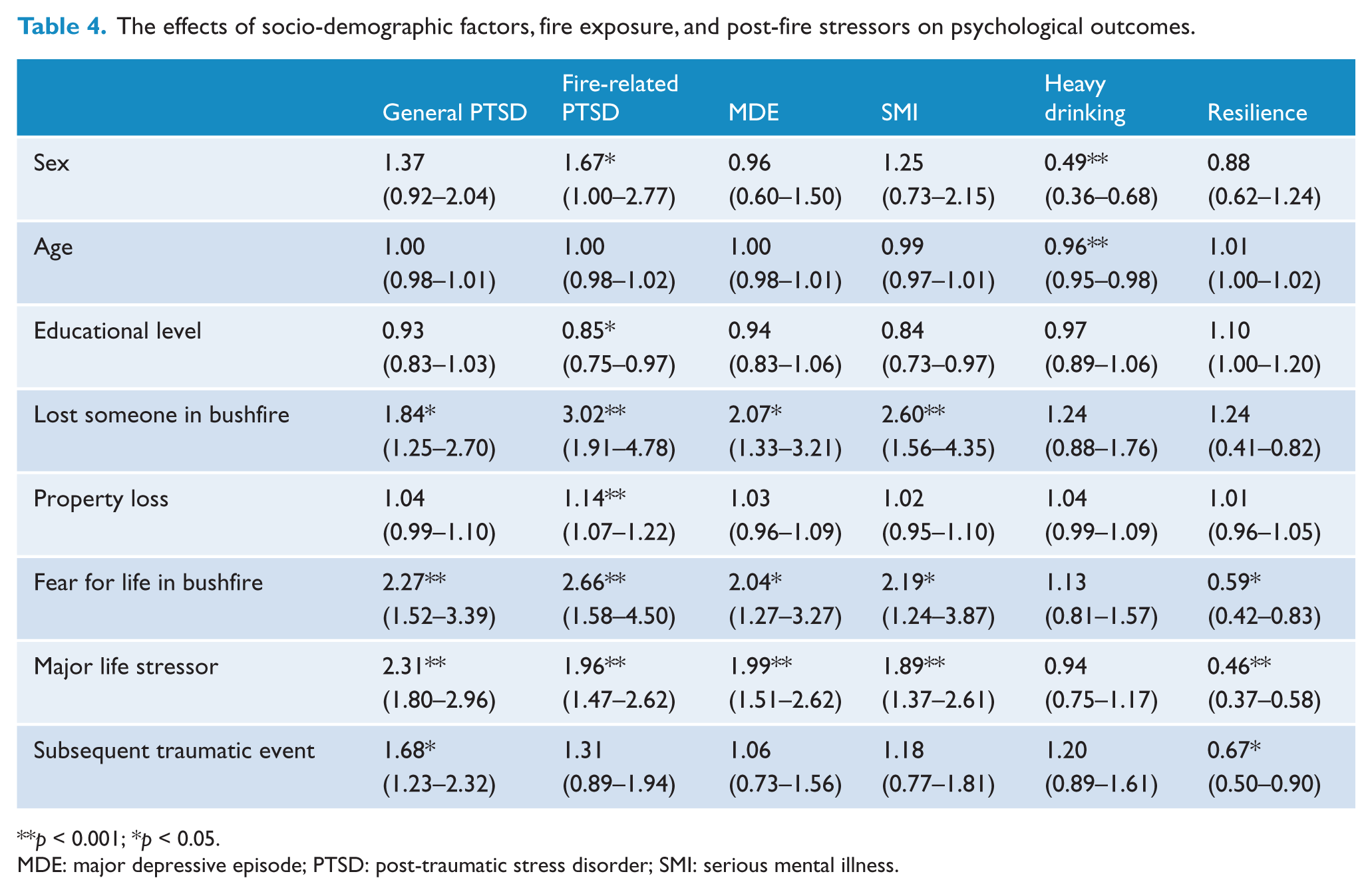
p < 0.001; *p < 0.05.
MDE: major depressive episode; PTSD: post-traumatic stress disorder; SMI: serious mental illness.
Discussion
The first point to note from these results is that the majority of respondents, including those from communities most affected by the Black Saturday bushfires were resilient 3–4 years after the bushfires. The finding that only a minority of people in the most affected regions had probable PTSD, MDE, or psychological distress accords with much previous evidence that most people eventually adapt to adverse life events (Bonanno, 2004; McFarlane et al., 1997). Our observation is particularly noteworthy in the context of previous Australian studies, dating from the Ash Wednesday bushfires up to recent natural disasters, which have all found that the majority of affected people eventually adjust capably (McFarlane and Van Hooff, 2009; McFarlane et al., 1997; Parslow et al., 2006). We defined resilience in this study as scoring less than 7 on the K6, which indicated that the significant majority of respondents in the high- (73.9%), medium- (81.3%), and low-affected (84.9%) communities reported no psychological distress. The fact that this survey was conducted 3–4 years following the bushfires suggests that this observed pattern is probably indicative of more chronic responses rather than acute reactions that are susceptible to subsequent changes. Most studies following disasters show remission of psychological problems as time progresses, with a flattening of the recovery curve by 2 years post-exposure (Norris et al., 2002a), and so this snapshot several years after the bushfires suggests these resilient profiles reflect more stable and enduring effects.
Overall, the rates of PTSD reported in the high-affected communities were at least as high, if not higher, than the rates reported in earlier Australian studies. Having said this, it is very difficult to accurately compare the current rates of psychological disturbance with those reported in previous Australian studies because of variable sampling methods, assessment tools, and interviewing methods. It is noteworthy that the rates of general PTSD were higher than PTSD linked specifically to the Black Saturday bushfires in the most affected communities, and that the rates were high in the less affected communities. This finding underscores the proposal that rural regions of Australia have been exposed to considerable adversity at different periods. Although we did not index the identified triggers for all respondents’ reported PTSD, regional parts of Australia have been affected by a range of natural disasters (fires, floods, storms), as well as extended drought, for a number of years; further, regional and rural areas can experience marked rates of economic downturn, unemployment, domestic violence, and accidents. The finding that approximately 10% of people in the medium- and low-affected communities reported PTSD, more than double the 4.4% rate reported in the Australian 2007 National Survey of Mental Health and Wellbeing (McEvoy et al., 2011), highlights that living in these communities can involve exposure to adverse events that can precipitate traumatic stress responses. This observation also accords with much evidence of the adverse effects of cumulative trauma that contributes to PTSD (Scott, 2007). Sensitisation models posit that exposure to extreme stress results in neural sensitisation, which causes the person to be susceptible to the adverse effects of subsequent stressors (Post et al., 1995). This pattern has also been noted in trauma survivors, who display a greater reactivity to later stressors (Breslau et al., 1995).
A significant minority of respondents also indicated suffering major depression. Again, this was more common in the high-affected communities, where 12.9% reported significant depression. Depression is a very common sequel of traumatic events (Norris et al., 2002a), and it has been shown to be very common in post-disaster contexts that feature infrastructure and personal loss (North et al., 2008). Increasing concern about suicidality in rural and regional parts of Australia has arisen because of the increased risk of suicidality in rural and remote populations, arguably because of sustained drought, economic hardship, and limited mental health resources (Caldwell et al., 2004). In this context, it is worth noting that in the survey questions that addressed depressive responses, more participants from the high-affected (10.5%) than medium- (4.9%) or low-affected (5.9%) communities indicated having suicidal or self-injurious thoughts (OR: 2.03, 95% CI: 1.22–3.38, p = 0.007). It is common for disasters and other traumatic events to increase suicidal risk because of the distress of the symptoms, the losses incurred during the disaster, and the demands of the post-disaster context (Kessler et al., 2008). This highlights the need to consider suicidal risk for managing those most affected by the disaster.
Not surprisingly, factors that reflect the severity of the impact of the bushfires, including the degree to which the person feared for their life on Black Saturday, predicted a range of mental health outcomes, including PTSD and severe psychological distress. Fearing for one’s safety has repeatedly been shown to predict PTSD, and clearly reflects that the extent to which one’s sense of security is directly threatened has a major impact on one’s mental health several years later (Bryant and Harvey, 1996). We also observed that the death of someone close to the respondent predicted PTSD, depression, and severe psychological distress. There is abundant evidence that the extent to which someone experiences loss and hardship secondary to a traumatic event will increase the likelihood of PTSD and other mental health conditions following a disaster (Peek-Asa et al., 2012). This accords with the pattern that there were poorer psychological outcomes in the high-affected communities. The finding that lower educational level predicted fire-related PTSD accords with evidence that intellectual capacity provides a buffer against PTSD, arguably because people may have better cognitive, social, or financial resources to manage the demands of the traumatic experience (Macklin et al., 1998).
The increased risk for women of developing PTSD (in this case, as related to the bushfires), which may be attributed to hormonal, situational, or social factors that can all contribute to this increased risk, is a very consistent finding across most studies (Olff et al., 2007). Specifically, research suggests that women may be more likely to experience greater PTSD because of acute biological responses (Felmingham et al., 2012), greater appraisals of threat (Mak et al., 2004), or distinct coping styles (Norris et al., 2001). Interestingly, and in contrast with much evidence that women are more at risk of depression (Kessler et al., 1993), men and women reported comparable levels of depression in the current study. It is worth noting that sex disparity in depression only occurs after puberty, which suggests the involvement of a hormonal component in this increased risk (Cyranowski et al., 2000) interacting with increased rates of stressful events in girls during adolescence (Ge et al., 1994). The finding that depression was predicted by major life stressors since the bushfires may explain, in part, why men and women experienced comparable levels of depression; the enduring effects of stressors may have reduced any differential vulnerability to depression. This interpretation is consistent with findings from previous disasters, such as Hurricane Katrina, that have also reported comparable levels of anxiety and mood disorder across men and women (Kessler et al., 2008).
The finding that subsequent traumatic events were predictive of general PTSD but not fire-related PTSD suggests that the psychological outcomes of respondents were also influenced by traumatic events that occurred following the bushfires. There is increasing evidence that disasters, and traumatic events generally, increase the risk of exposure to further potentially traumatic events. For example, one study found that boys not evacuated prior to Hurricane Ike were more likely to be sexually assaulted and also to perpetrate sexual violence than those who were evacuated (Temple et al., 2011). Similarly, there were higher rates of domestic violence in people displaced after Hurricane Katrina (Larrance et al., 2007). Further, this effect seems to be impacted by the level of exposure to the disaster (Harville et al., 2011), which is consistent with the current finding that participants from the high- and medium-affected communities experienced more traumatic events since the Black Saturday bushfires than participants from the low-affected communities. Interestingly, and somewhat contrary to expectations, the impact of further traumatic events appears to have been specific to PTSD, failing to predict the development of subsequent depression.
Major life stressors were also very influential, predicting fire-related and general PTSD, depression, and severe psychological distress. Much of the available evidence points to the adverse compounding effects of subsequent stressors on post-traumatic mental health (King et al., 1998). Considering the frequency of social and personal upheaval that occurs following disasters, including economic problems, employment difficulties, and family stressors, these findings highlight that alleviating these stressors can play an important role in reducing psychological problems post-disaster.
There were significant rates of heavy drinking across all communities; however, heavy drinking rates were even higher in the high-affected communities. This finding accords with evidence that substance abuse increases following disasters (Boscarino et al., 2006). Previous reports have noted the high rates of alcohol abuse in rural parts of Australia (Australian Institute of Health and Welfare, 2008), and it is probable that the elevated rates in the less affected communities can be explained by this factor. The observation that younger people and more men were more likely to be abusing alcohol is consistent with previous studies conducted in rural Australia (Inder et al., 2012), and highlights the need to address this issue in these subgroups.
A worrying trend in the responses was that one-third of respondents who indicated SMI did not receive formal assistance for their problems in the previous month. It is unlikely that this pattern can be attributed to impoverished resources in regional areas of Victoria because the pattern observed in this study is consistent with findings from a range of disasters, where significant proportions of distressed people do not seek mental health services (Boscarino et al., 2004). In this context, it is worth noting that considerable effort has gone into developing mental health resources in the affected regions of the state of Victoria following the bushfires; however, it appears that these resources are not being used optimally. Enhancing health service use appears to remain a challenge for health providers in the regions most affected by the bushfires. It is also noteworthy that two-thirds of those who were reporting SMI were receiving care at this period of time after the bushfires. This may reflect chronic distress in some individuals with difficulties prior to the bushfires, ongoing adjustment problems that have been resistant to heath interventions, or possibly suboptimal mental health interventions. It has been shown that a significant proportion of trauma survivors approach general practitioners for mental health assistance (Brewin et al., 2010), though it is unknown if this leads to eventual receipt of evidence-based interventions.
This study has a number of limitations. First, the overall recruitment rate was low, the sample was not fully representative of local communities, and there was a marginal imbalance of gender. Second, we indexed psychological outcomes with screening tools rather than structured clinical interviews; whereas the former are brief screening tools that permit estimates of prevalence in epidemiological studies, the latter ask about the full range of symptoms that are required to make definitive diagnostic decisions. Third, there was difficulty promoting the study to people who were displaced by the bushfires beyond the initial contact letter using the VEC-provided address. It is possible that these people may have a different profile than those who remained within their community; in this sense our findings may not fully reflect the effects of the bushfires on all people exposed to the disaster. Fourth, we did not index the psychological status of people prior to the bushfires and so we cannot determine the extent to which the effects are influenced by pre-existing psychological difficulties. Fifth, the nature of the interview precluded full assessment of experiential aspects of fighting the bushfires, which may have been important for subsequent adjustment. Finally, this study was conducted 3–4 years after the bushfires and there is a need for longer-term follow-up assessments to index the prolonged effects of the bushfires and other adverse events; this study will be conducting further longitudinal assessments in the coming years.
These findings point to several important outcomes. First, despite the magnitude of the disaster most people in the affected communities appear to have adjusted to the events of Black Saturday. This is consistent with the pattern observed following most disasters; however, it may also reflect the considerable effort given to rebuilding community connectedness and growth following the disaster. Second, despite the overall trend of resilience, a significant proportion of respondents did report psychological distress that included post-traumatic stress and depression. On the basis of the current findings we can speculate about possible improvements to mental health services. There is much evidence that many affected individuals following disasters do not seek mental health assistance (Boscarino et al., 2004). The approach taken by this study, which was facilitated by substantive community engagement exercises in the affected communities, allowed more personal communications with survivors and thereby a thorough assessment of functioning. Variants of this approach have been adopted in previous post-trauma settings, such as the London bombings (Brewin et al., 2010), and there may be scope for systematic screening of high-affected areas to overcome the barrier of survivors not seeking suitable care. It is worth noting, however, that although the government response, along that of many other agencies, initiated substantive psychosocial recovery projects in the wake of Black Saturday (Forbes et al., 2010), the high rate of SMI in these communities suggests this approach was not adequate. It is recognised that provision of mental health services in regional areas is difficult, but the current findings point to the need for policymakers to strategically target regions that have a high risk of persistent mental distress and ensure that adequately trained and supported health professionals can provide the services required. Further, we recognise the role of social and community support in long-term adjustment. Finally, there is a need to index more closely how community processes are impacting on adaptation after the bushfires.
Footnotes
Acknowledgements
We are grateful for the assistance of Shae Johnson in the presentation of the final results.
Funding
This study was funded by an Australian Research Council Linkage Grant (LP100200164).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.