
Abstract
Objectives:
To map the changing prevalence and predictors of psychological outcomes in affected communities 5 years following the Black Saturday bushfires in Victoria.
Method:
Follow-up assessment of longitudinal cohort study in high, medium and non-affected communities in Victoria, Australia. Participants included 1017 respondents (Wave 1) interviewed via telephone and web-based survey between December 2011 and January 2013, and 735 (76.1%) eligible participants were retested between July and November 2014 (Wave 2). The survey included measures of fire-related and subsequent stressful events, probable posttraumatic stress disorder, major depressive episode, alcohol use and severe distress.
Results:
There were reduced rates of fire-related posttraumatic stress disorder (8.7% vs 12.1%), general posttraumatic stress disorder (14.7% vs 18.2%), major depressive episode (9.0% vs 10.9%) and serious mental illness (5.4% vs 7.8%). Rates of resilience increased over time (81.8% vs 77.1%), and problem alcohol use remained high across Wave 1 (22.1%) and Wave 2 (21.4%). The most robust predictor of later development of fire-related posttraumatic stress disorder (odds ratio: 2.11; 95% confidence interval: [1.22, 3.65]), general posttraumatic stress disorder (odds ratio: 3.15; 95% confidence interval: [1.98, 5.02]), major depressive episode (odds ratio: 2.86; 95% confidence interval: [1.74, 4.70]), serious mental illness (odds ratio: 2.67; 95% confidence interval: [0.57, 1.72]) or diminished resilience (odds ratio: 2.01; 95% confidence interval: [1.32, 3.05]) was extent of recent life stressors.
Conclusion:
Although rates of mental health problems diminished over time, they remained higher than national levels. Findings suggest that policy-makers need to recognize that the mental health consequences of disasters can persist for many years after the event and need to allocate resources towards those who are most at risk as a result of substantive losses and ongoing life stressors.
There is overwhelming evidence of the adverse mental health consequences of both man-made and natural disasters (Norris et al., 2002a, 2002b). Most research has focused on posttraumatic stress disorder (PTSD), with rates of approximately 10–20% being reported in the initial year following the disaster (North, 2007; North et al., 2008). Depression is also commonly reported after disasters, with approximately 14% of survivors reporting major depression (Norris et al., 2002a, North et al., 2012). Finally, there is also much evidence that excessive use of substances is common following disasters (Boscarino et al., 2006; Vlahov et al., 2002). These trends need to be balanced with the recognition that all large studies of disaster survivors converge on the observation that most people are resilient and do not develop psychiatric disorders (Norris et al., 2009).
Current evidence is limited by several factors. First, most studies lack comparator populations which are important to determine the relative impact of the disaster on the affected population. Second, few studies have tracked the long-term sequelae of major disasters, with most research focusing on the initial year or 2 years after the event. The longest follow-up to date was conducted after the Buffalo Creek dam disaster, which studied a sample of litigants over time; this study found that PTSD decreased from 44% at 2 years to 28% at 14 years (Grace et al., 1993). Another study of survivors of the Oklahoma Bombing found that the rate of PTSD decreased from 41% at 6 months to 26% at 7 years (North et al., 2011); this latter study found no cases of delayed onset of PTSD in which people developed the disorder if they did not present with it at the 2-year assessment.
Australia has a long tradition of dealing with natural disasters, and numerous studies have longitudinally investigated the mental health effects of bushfires and earthquakes. One study that tracked the mental health of people exposed to the Newcastle earthquake throughout the initial 2 years of the disaster found that 18% of those most exposed to the quake had probable PTSD at 2 years (Carr et al., 1997). A 20-year follow-up of children affected by a major bushfire found that although disaster-affected children had higher rates of adult psychopathology, this was not directly a result of the childhood disaster exposure (McFarlane and Van Hooff, 2009). In a rare design, a New Zealand study capitalized on a cohort study of people living in the Canterbury region, 57% of whom were exposed to the 2010–2011 earthquakes. This design allowed mental health effects of the disaster to be disentangled from other potential confounding factors; this research reported that the disaster could account for 10.8–13.3% of overall rates of mental health conditions in this cohort (Fergusson et al., 2014). There is a need for further study of long-term effects of disasters because this initial evidence suggests that people can suffer the adverse psychological effects for prolonged periods after the disaster occurs.
In February 2009, Australia experienced one of its worst disasters when severe bushfires affected most of the state of Victoria in what is known as the ‘Black Saturday’ fires. This disaster caused widespread damage, including 173 fatalities, 3500 buildings being damaged or destroyed, and massive adverse impact on community infrastructures (The 2009 Victorian Bushfires Royal Commission Final Report Summary, 2009). To study the long-term effects of the disaster, we undertook a major multi-method longitudinal study to map the mental health sequelae of the fires (Beyond Bushfires: Community, Resilience and Recovery Study (Gibbs et al., 2013). In an earlier report that identified the mental health status of survivors 3–4 years after the fires, we found that people in highly affected regions had higher rates of probable disaster-related PTSD (15.6%), probable depression (12.9%), severe distress (12.8%) and heavy alcohol use (24.7%) relative to those from less affected regions and also higher than Australian normative data (Bryant et al., 2014). The goal of this report is to outline the status of the mental health of respondents 5 years after the disaster and to map the course and predictors of mental health over time.
Method
Participants
This Wave 1 data collection occurred between April 2012 and January 2013 (approximately 3–4 years after the fires) and recruited adults aged at least 18 years of age living in 25 communities in 10 locations in Victoria; the sites were selected because they were variably affected by the Black Saturday fires, ranging from a high level of impact in terms of lives lost and property destroyed through to communities with minimal impact. Affectedness was defined as high-impact (operationalized as many houses lost plus fatalities; N = 630), medium-impact (operationalized as ranging from a small number of fatalities through to communities with no fatalities but significant amount of property damage; N = 182), and low-impact (operationalized as no evidence of burning; N = 205). The 2006 census data indicated a total adult population of 7693 in the selected communities, including 702 adults in the two pilot communities. The Victorian Electoral Commission (VEC) provided contact details of both current residents and those who relocated since the fires (N = 7467 adults), and a letter was sent to them inviting them to participate in the study with a reply-paid envelope; this step was taken to comply with ethical requirements pertaining to respondents’ privacy. Additional community awareness activities, mailbox drops, area-based phone calls, news media and social media activities were also conducted to increase awareness of the study and methods for registration. In terms of people who were eligible to participate this study, 16% of available people eventually participated and completed the survey. The sample who participated in this study were older, had a higher proportion of females and were more educated than the general community according to census data for these regions. At the completion of the Wave 1 survey, 966 participants agreed to be contacted for the Wave 2 survey. The Wave 2 data collection was conducted between July and November 2014 (5 years after the fires). In terms of retention, 736 (76.1%) eligible participants took part in Wave 2. Of these, 29 had not been living in the study communities at the time of the fires and were excluded from the final analyses. The final sample for the analyses below is based on a sample of n = 707 individuals who took part in both surveys and who lived in a selected community on the day of the bushfires.
Measures
PTSD
Probable PTSD was assessed using an abbreviated version of the Posttraumatic Stress Disorder Checklist (PCL-S) (Bliese et al., 2008), which comprises four items each scored on a 5-point severity scale that indexes key symptoms of PTSD anchored to the previous 4 weeks. Adopting a cut of 7 on the PTSD Screen achieves an efficient estimation of PTSD diagnosis relative to the full version of the PCL-S (Bliese et al., 2008). PTSD was assessed in two ways: (a) regarding responses that were specific to the Black Saturday fires and (b) in response to traumatic events generally. To disentangle general PTSD from fire-related PTSD, we followed each question about a PTSD symptom with a question of whether this symptom was related to their reactions to the fires. For example, after asking about intrusive memories, participants were asked, ‘Were these reactions about the fires?’
Depression
Probable Major Depressive Episode (MDE) was assessed using the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001). Probable occurrence of MDE was assessed if five of the nine symptoms had been present for most days in the previous 2 weeks.
Psychological distress
Generic psychological distress was assessed using the K6, which measures anxiety-mood problems in previous 30 days (Kessler et al., 2003). Classification of no distress has used K6 scores of 0–7, 8–12 as mild-moderate distress, and 13–24 as probable severe distress (Kessler et al., 2008). We defined psychological resilience as K6 scores of 0–7, reflecting people who reported no or minimal psychological problems. Additionally, the K6 asks how often in the past 30 days did the person see a health professional about problems reported on the K6.
Alcohol use
Heavy drinking was assessed using the Consumption Scale of the Alcohol Use Disorder Identification Test–Consumption (AUDIT-C) (Bush et al., 1998), a 3-item self-report measure that indexes heavy drinking. The AUDIT-C employs the initial three questions of the AUDIT, which indexes amount of alcohol consumption. We adopted recommended cut-offs of six standard drinks for males and five for females as the most effective detection of heavy drinking; these cut-offs have sound sensitivity (males: 0.82; females: 0.84) and specificity (males: 0.79; females: 0.88) (Aalto et al., 2009) with heavy/binge drinking as defined by the Timeline Followback structured interview for alcohol consumption (Sobell and Sobell, 1995).
Fire-related experiences
To index exposure to the fires, we asked (a) whether the respondent had feared for his or her own life, (b) whether anyone close to the respondents had died in the fires and (c) whether they personally lost property or buildings in the fires.
Recent traumatic events
To assess traumatic events that had occurred since the fires, participants were asked to indicate whether they had been exposed to any of the following potentially traumatic events: (a) natural disaster, (b) serious accident and (c) serious assault/violence. They were also asked whether they had experienced major life stressors in the form of disruptions to their (a) income, (b) accommodation or (c) personal relationships.
Procedure
The study was approved by the University of Melbourne Human Research Ethics Committee. Following considerable engagement in the affected communities, the survey was conducted by a combination of telephone and web-based formats. Following an introduction to the study and obtaining informed consent, the interviewer initially asked about socio-demographic factors, events that occurred on the day of the Black Saturday fires and traumatic events that may have occurred since the fires. The Wave 2 survey followed the same format, with questions about traumatic and stressful events focusing on the time period since the last survey. Relevant to the current analyses, the survey sequentially administered the PCL-S, PHQ, K6 and AUDIT-C.
Statistical analyses
All data are based on the participants retained at Wave 2. Prevalence rates were calculated based on recommended cut-offs for probable PTSD, MDE, heavy drinking and serious mental illness (SMI). To determine the patterns in which people altered their status over time, separate logistic regressions were conducted to predict changes in case cut-offs of general PTSD, fire-related PTSD, depression, SMI and heavy drinking. In each regression, sex, age at the time of the Black Saturday fires and highest level of education were entered at Step 1. Factors that reflected the severity of fire exposure were entered at Step 2, including whether the respondent had feared for their own life, whether someone close to the respondent had died in the fires and the extent of property loss. Finally, at Step 3, major life stressors experienced since the Wave 1 survey were entered to index the additional effects of subsequent adversity on psychological outcomes. Separate regressions were conducted to predict (a) delayed development of disorder (comparing participants without the disorder at Wave 1 who either did or did not have the disorder at Wave 2) and remission of disorder (comparing participants with the disorder at Wave 1 who either did or did not have the disorder at Wave 2).
Results
Participant characteristics
Table 1 presents the participant characteristics of those retained and not retained at the Wave 2 assessment. Participants who were retained at Wave 2 did not differ from those who did not participate in terms of age, gender or whether they had experienced bereavement in the fires. Relative to those who were lost at follow-up, participants at Wave 2 were more likely to have tertiary education (38.9% vs 27.6%; odds ratio [OR]: 1.67; 95% confidence interval [CI]: [1.25, 2.21], p = 0.000), and fewer participants from low-impact communities (52.7%) were retained than those from medium- and high-impact communities (73.6%) (OR: 2.50; 95% CI: [1.83, 3.43], p = 0.000). All subsequent analyses focus on those who were retained at Wave 2.
Participant characteristics by survey retention status.
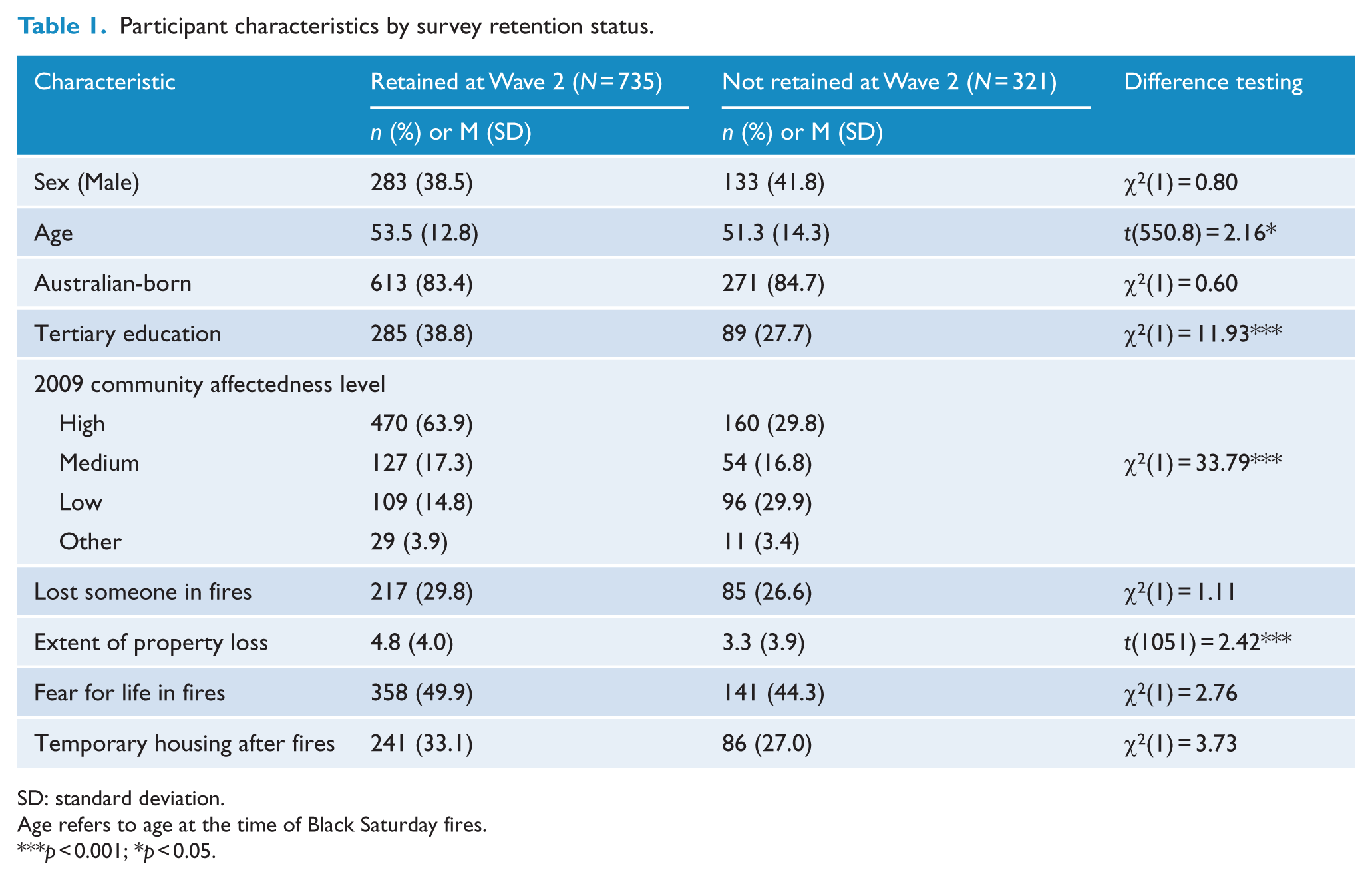
SD: standard deviation.
Age refers to age at the time of Black Saturday fires.
p < 0.001; *p < 0.05.
Prevalence of psychological outcomes
Table 2 presents the frequencies of reported probable PTSD, MDE, heavy drinking and SMI at Wave 2, according to the level of exposure to the fires. In terms of PTSD linked to the Black Saturday fires, more participants in the high-affected communities reported probable PTSD (10.9%) than those from the medium-affected (5.6%) and low-affected (1.9%) communities (OR: 3.04, 95% CI: [1.47, 6.29], p = 0.003). A similar pattern was observed regarding general PTSD from any traumatic event, with more participants in the high-affected communities reporting probable PTSD (18.7%) than medium-affected (8.7%) and low-affected (4.6%) communities (OR: 3.14, 95% CI: [1.79, 5.48], p = 0.001). Similarly, participants in the high-affected communities were more likely to report MDE (10.9%) than participants in the medium-affected (4.7%) and low-affected communities (4.6%) (OR: 2.48, 95% CI: [1.27, 4.85], p = 0.008). Participants in the high-affected communities were no more likely to report severe distress (6.2%) than participants in medium-affected (4.7%) and low-affected communities (2.8%) (OR: 1.65, 95% CI: [0.77, 3.55], p = 0.19). Finally, there were comparable proportions of participants reporting heavy drinking in each type of community (high-affected: 23.2%, medium-affected: 18.4%; low-affected: 17.0%) (OR: 1.40, 95% CI: [0.94, 2.09], p = 0.19). Overall, the rates of people suffering probable PTSD, MDE or severe distress (problem alcohol use excluded because of its high prevalence in all communities) were 21.9% in high-affected, 10.3% in medium-affected and 5.6% in low-affected regions; those living in high-affected regions were more likely to have any disorder than those in other regions (OR: 3.18, 95% CI: [1.89, 5.33], p = 0.001).
Prevalence of mental health conditions across communities.
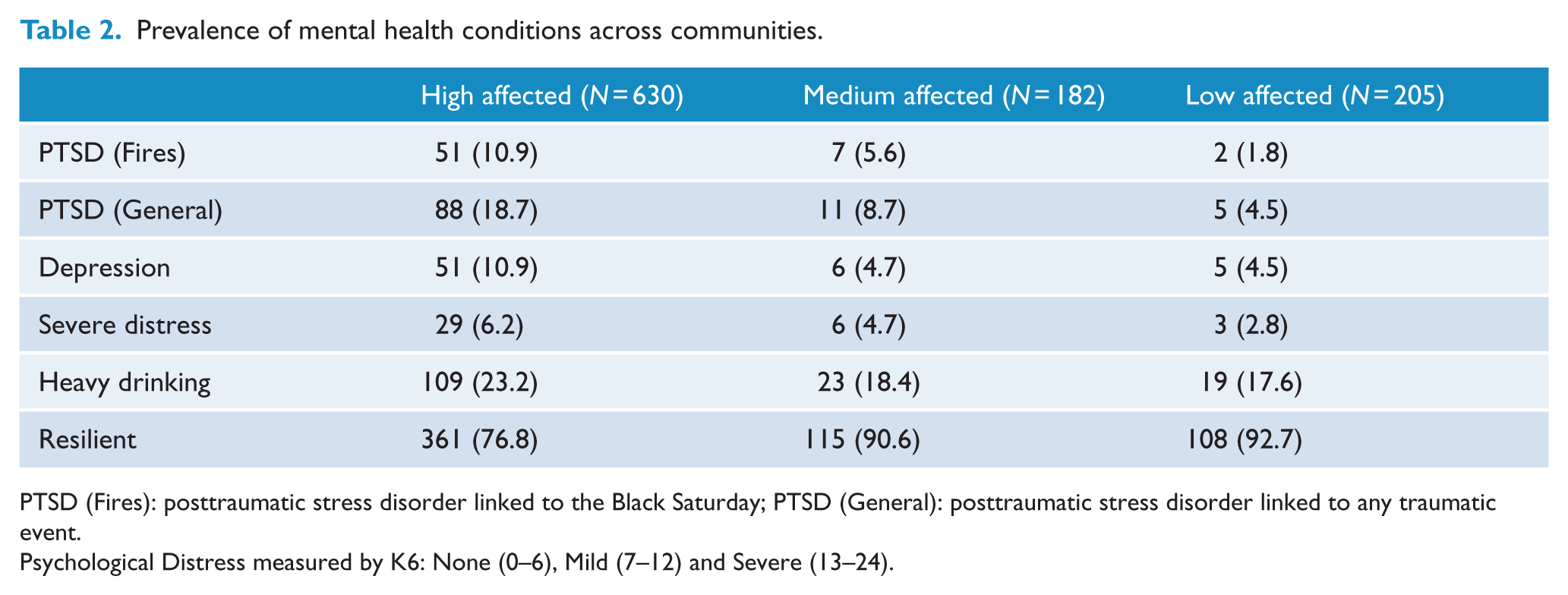
PTSD (Fires): posttraumatic stress disorder linked to the Black Saturday; PTSD (General): posttraumatic stress disorder linked to any traumatic event.
Psychological Distress measured by K6: None (0–6), Mild (7–12) and Severe (13–24).
Comorbidity
Considering the documented evidence of comorbidity between PTSD and depression and alcohol abuse (Kessler et al., 1994), the rates of comorbidity between these conditions were calculated. Relative to those without the probable diagnosis, there was stronger comorbidity of those with general PTSD (34.9% vs 14.4%; OR: 24.13; 95% CI: [13.33, 43.70], p = 0.001) and fire-related PTSD (36.5% vs 15.7%; OR: 13.30; 95% CI: [7.34, 24.12], p = 0.001) with probable depression. Similarly, relative to those without the probable diagnosis, there was stronger comorbidity of those with general PTSD (29.4% vs 20.3%; OR: 1.633; 95% CI: [1.03, 2.57], p = 0.04) and fire-related PTSD (34.9% vs 20.4%; OR: 2.09; 95% CI: 1.20, 3.63, p = 0.009) with probable severe alcohol use.
Rates of resilience
Consistent with prevailing definitions of resilience as the absence of persistent psychological distress (as distinct from the absence of mental disorder) (Bonanno et al., 2004), we operationalized resilience as scores of 0–6 on the K6 (Kessler et al., 2008). Fewer participants from the high-affected communities reported resilience (76.8%) than in the medium-affected (90.6%) and low-affected (92.6%) communities (OR: 0.46, 95% CI: [0.32, 0.65], p < 0.001).
Changes in psychological status
Table 3 reports the changing prevalence rates of psychological outcomes across the two waves of data collection. Overall, the rates of mental health problems decreased over time. A lower rate of probable fire-related PTSD was observed at Wave 2 (8.7%) compared to Wave 1 (12.1%), with an exact McNemar’s test indicating that this difference was statistically significant (χ2 = 9.19, p = 0.002). Similarly, lower rates were observed at Wave 2 for general PTSD (18.2% vs 14.7%; χ2 = 5.38, p = 0.020) and severe distress (7.8% vs 5.4%; χ2 = 5.59, p = 0.017). Consistent with this pattern, the rates of resilience increased over time (77.1 vs 81.8%; χ2 = 6.51, p = 0.011). However, the difference in MDE (11.2% vs 8.8%) was not significantly lower at Wave 2 (χ2 = 3.71, p = 0.054). Likewise, rates of problem alcohol use remained high across Wave 1 (22.1%) and Wave 2 (21.4%) (χ2 = 0.05, p = 0.826).
Prevalence of mental health conditions in Wave 1 and Wave 2.
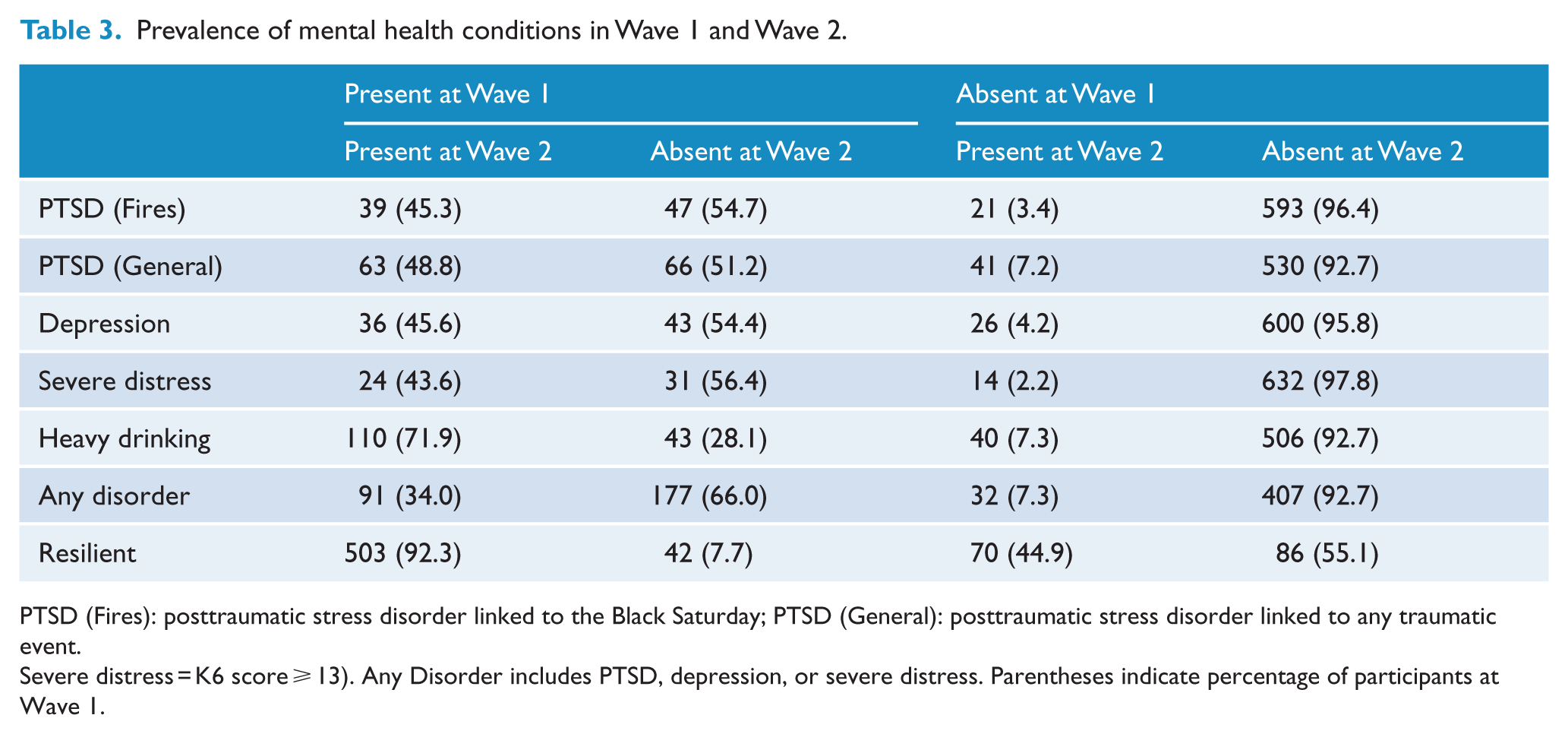
PTSD (Fires): posttraumatic stress disorder linked to the Black Saturday; PTSD (General): posttraumatic stress disorder linked to any traumatic event.
Severe distress = K6 score ⩾ 13). Any Disorder includes PTSD, depression, or severe distress. Parentheses indicate percentage of participants at Wave 1.
Table 3 indicates that there were considerable shifts in each domain over time. Approximately half of participants who displayed PTSD, MDE or severe distress at Wave 1 did not retain this status at Wave 2. In contrast, a smaller but significant proportion of participants who did not report the condition at Wave 1 did report it at Wave 2; specifically, 7.3% of participants who did not report any disorder at Wave 1 reported a disorder at Wave 2.
Predictors of changing psychological outcomes
In terms of changing mental health status across time, Table 4 presents the adjusted ORs for PTSD, MDE, heavy drinking and psychological distress for those who did not meet the cut-offs at Wave 1 but did meet them at Wave 2. The late onset of both fire-related PTSD and general PTSD was predicted by the extent of property loss in the fires and major life stressors since the fires. Late-onset MDE was predicted by major life stressors. Late-onset heavy drinking was predicted by younger age. Late-onset severe distress was predicted by the extent of property loss in the fires and recent life stressors. Delayed resilience was predicted by lower education level (less than tertiary education).
Effects of socio-demographic, fire-exposure and post-fire stressors on changing psychological outcomes.
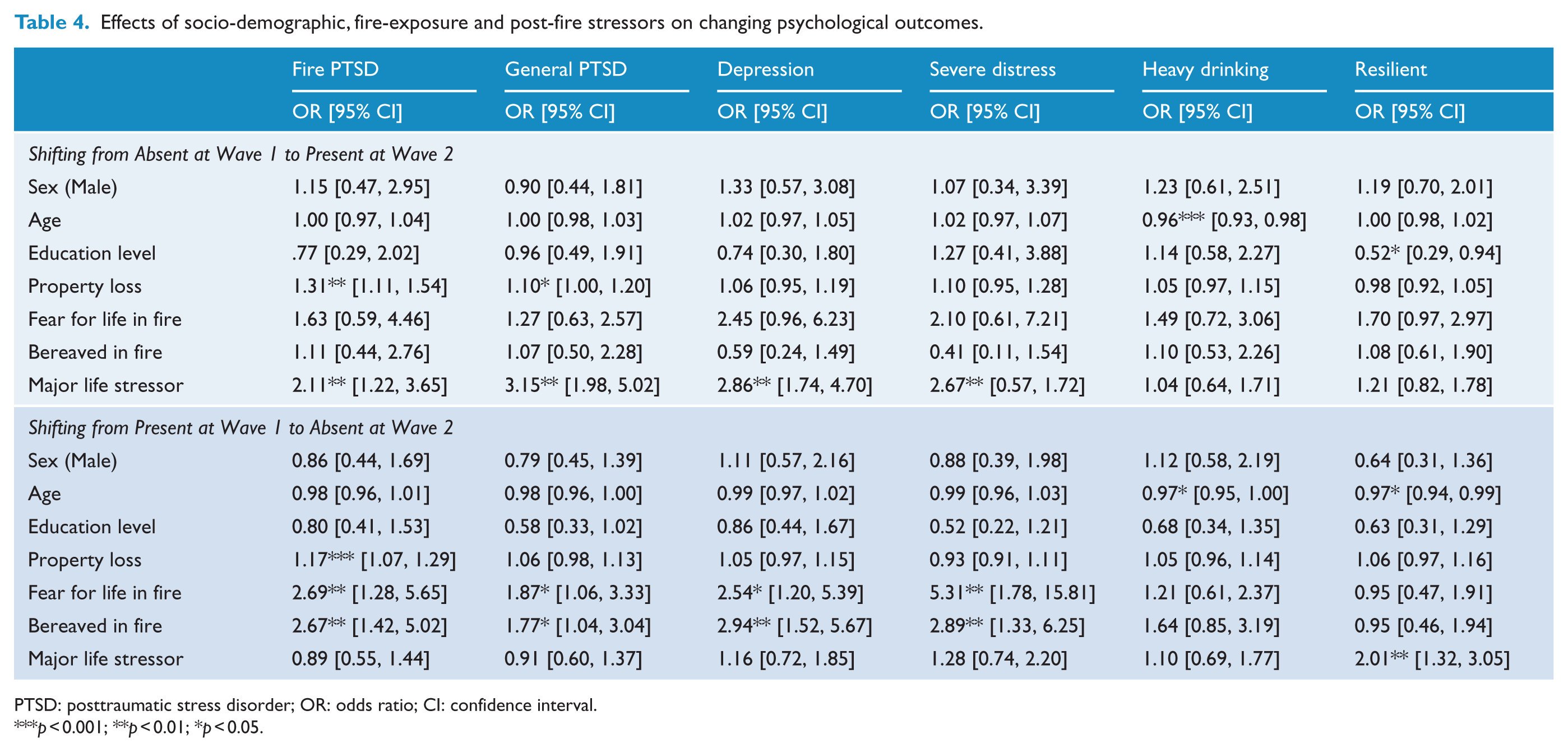
PTSD: posttraumatic stress disorder; OR: odds ratio; CI: confidence interval.
p < 0.001; **p < 0.01; *p < 0.05.
Table 4 also presents the adjusted ORs for PTSD, MDE, heavy drinking and psychological distress for those who met the cut-offs at Wave 1 but did not meet them at Wave 2. Recovery from fire-related PTSD was seen in those who had had higher property loss, higher levels of fear for life and higher rates of bereavement resulting from the fires. Similarly, recovery from general PTSD, MDE and severe distress was also seen in those who had had higher levels of fear for life and higher rates of bereavement. Those whose drinking rates fell tended to be younger individuals. Diminished resilience was predicted by younger age and recent life stressors.
Discussion
The rates of probable PTSD, depression and severe distress observed 5 years following the disasters suggest that the rates of psychological distress remained high. For example, the rate of probable PTSD was markedly higher than the nationally reported rate of 4.4% rate in the Australian 2007 National Survey of Mental Health and Wellbeing (McEvoy et al., 2011), although this comparison needs to be made tentatively because these studies used very different sampling strategies and assessment tools. The elevated rates of psychiatric disorder accord with previous reports of persisting mental distress in people directly affected by severe disaster (Grace et al., 1993; North et al., 2011). The comorbidity between PTSD and both depression and alcohol use is also consistent with much evidence of the strong overlap between these conditions (Afzali et al., 2017; Kessler et al., 1994).
The observation that rates of probable disorder fluctuated over time is consistent with evidence that posttraumatic mental health follows a dynamic and fluctuating course over time (Bryant et al., 2013). The observation that a significant proportion of people apparently had better mental health over time accords with considerable evidence that many people eventually adapt over time following trauma (Galea et al., 2003; Van Griensven et al., 2006). Conversely, the trend that many people displayed probable disorder at follow-up without reporting this level of distress at the initial assessment is consistent with reports of worsening or delayed expression of symptoms as time elapses after trauma (Bonanno et al., 2008; Bryant et al., 2015; Norris et al., 2009). This finding needs to be understood in the context of this wave of data collection occurring at least 1 year after the initial wave (at least 5 years after the fires). These timeframes underscore how the effects of disasters, and their aftermath, can impact people in different ways years after the event.
Across analyses, it was apparent that ongoing life stressors were a major factor in determining the ongoing mental health of survivors of the fires. Recent stressors contributed to worsening PTSD, depression and distress, as well as diminishing psychological resilience. Previous studies have highlighted that ongoing stressors following a traumatic event significantly impact subsequent mental health (Andrews et al., 2007; Bryant et al., 2013). Disasters are often marked by widespread societal and economic adversity, which can pervasively undermine the capacity to recover from the traumatic event. The impact of ongoing stressors has been previously noted in an Australian context in the aftermath of the Newcastle earthquake, where it was noted that disruptions occurring in the period following the disaster predicted posttraumatic psychopathology 2 years after the quake (Lewin et al., 1998). More recently, in the wake of Hurricane Katrina, it was noted that the increased rates of mental distress and suicidal risk may be attributed to the ongoing stressors in New Orleans, including inadequate housing, poor infrastructure in the worst-affected regions and the downturn in economic options (Kessler et al., 2008). Importantly, numerous studies have noted ongoing stressors contribute to worsening of mental health after disaster (Pietrzak et al., 2013) and that the relative impact of these stressors can increase as time elapses (Cerda et al., 2013). It is also worth noting that rural and regional districts of Australia can suffer a range of ongoing adversities, which can adversely impact mental health. The finding that participants across the differently affected communities experienced general PTSD and depression underscores the vulnerability of rural and regional areas of Australia to psychological difficulties.
Some of the most salient effects of the disaster, including bereavement, fear and property loss, were associated with recovery from PTSD, depression and psychological distress over time. It is possible that for individuals affected by these events, as more time elapses after the disaster, the direct adverse effects of these factors on mental health reduce. However, as noted above, life stressors – many of which may be triggered by the ongoing social and economic disruption of the bushfires – remain as a central burden on mental health of the disaster survivors.
The notion that worsening mental health was influenced by environmental stressors accords with the finding that delayed expression of PTSD was also predicted by the extent of property loss in the fires. The extent to which people suffered property damage may have resulted in ongoing and delayed difficulties in resuming prior levels of occupational or domestic functioning, which subsequently compounded their stress reactions. It is also possible that extent of property loss during the fires contributes ongoing financial stressors, arising from legal proceedings, rebuilding costs and loss of income. Prior studies of postdisaster adaptation have noted that as time elapses after the disaster, mental health is adversely affected by financial losses (Cerda et al., 2013; Galea et al., 2008). The extent of property loss in the fires may contribute to financial strain, which then impacts ongoing PTSD and depression.
It is important to note that most participants reported being resilient across time, underscoring overwhelming evidence that most people are able to cope with adversity (Bonanno and Diminich, 2013; Pietrzak et al., 2014). People who were not resilient at Wave 1 but demonstrated resilience at Wave 2 were less likely to have suffered bereavement during the fires or extensive property loss. This pattern suggests that people are more likely to adjust to the disaster as time elapses when they have suffered less exposure to events that are likely to have long-lasting effects. In other words, bereavement and severe property loss may impede resilience because they potentially continue to have an adverse impact on the survivor’s capacity to function on a daily basis.
We qualify this conclusion by recognizing that the sample at this assessment represents a minority of those affected by the fires, and hence there remain questions over the generalizability of the findings. The recruitment of only 16% of people in the affected regions tempers our conclusions and precludes definitive statements about the incidence of psychopathological conditions after the fires. The finding that participants in this study were older, more likely to be female and more educated than others in the community highlights the need for caution in generalizing these results to the broader community. We also note that the survey methodology did not use structured clinical interviews, the measures of stressful life events were not psychometrically validated measures, it is inherently difficult to disentangle PTSD related to fires from PTSD related to other events and there is a possibility that the observed rates of probable disorder may be inflated (North, 2014). In this sense, it is possible that our reported rates may be detecting subsyndromal levels of disorders (North and Pfefferbaum, 2002). This possibility is underscored by the absence of validation of the probable diagnosis cut-offs for this population, and scoring below the cut-offs may still incorporate a range of subsyndromal symptomatology that can pose risk for ongoing difficulties. Nonetheless, there is strong evidence that subsyndromal levels of disorders following traumatic events lead to comparable levels of impairment and distress as diagnostic levels, and hence the reported rates nonetheless represent a significant health issue (Pietrzak et al., 2012; Stein et al., 1997).
These findings have implications for disaster policy-makers. It is apparent that the mental health effects of large-scale disasters can persist for years after the event, and resources need to be devoted to addressing these needs. It appears that those most at risk of persistent or delayed mental health problems are those who are exposed to the more severe trauma exposure during the disaster, as well as those who suffer adverse life events in the aftermath of the event. Strategies that can minimize stressful events for those affected by disaster in the years after the initial event may carry widespread benefits in alleviating the mental health burden of survivors. The findings also suggest that monitoring of disaster survivors who are exposed to ongoing stressors (e.g. financial strain, insurance difficulties and rebuilding pressures) is warranted because these people are the ones who are most likely to experience deteriorating mental health years after the disaster, and so resources may need to be targeted towards these individuals or communities.
Footnotes
Acknowledgements
We acknowledge the late Professor Elizabeth Waters, Principal Investigator, for development and guidance of the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was funded by an Australian Research Council Linkage Grant (LP100200164).