
Abstract
Objectives:
To profile the long-term mental health outcomes of those affected by the 2009 Black Saturday bushfires and to document the course of mental health since the disaster.
Method:
The longitudinal Beyond Bushfires study included 1017 respondents (Wave 1; 3–4 years after the fires), 736 (76.1%) at Wave 2 (5 years after the fires) and 525 (51.6%) at Wave 3 (10 years after the fires). The survey indexed fire-related and subsequent stressful events, probable posttraumatic stress disorder, major depressive disorder, alcohol use, severe distress and receipt of health services for mental health problems.
Results:
Relative to their status 3–4 years after the fires, there were reduced rates of fire-related posttraumatic stress disorder (6.2% vs 12.2%), general posttraumatic stress disorder (14.9% vs 18.7%) and severe distress (4.4% vs 7.5%) at 10 years. There were comparable rates between Wave 1 and Wave 3 for depression (10.9% vs 8.3%) and alcohol abuse (21.8% vs 18.5%). Of people in high-affected regions, 22.1% had posttraumatic stress disorder, depression or severe distress at Wave 3. One-third to one-half of participants who reported probable posttraumatic stress disorder or depression at any assessment did not display the disorder at the next assessment. Worsening of mental health at Wave 3 was associated with the extent of property loss, exposure to recent traumatic events or recent stressful life events. Only 24.6% of those with a probable disorder had sought professional help for this in the previous 6 months.
Conclusion:
Approximately one-fifth of people from high-affected areas have a probable psychological disorder a decade after the fires. Mental health appears to fluctuate for those who are not consistently resilient, apparently as a result of ongoing stressors. The observation that most people with probable disorder are not receiving care highlights the need for further planning about managing long-term mental health needs of disaster-affected communities.
Introduction
Natural and human-made disasters have highlighted the regular threats that disasters can have on a community’s mental health. A recent meta-analysis that included 27 studies that compared mental health of people after disaster exposure with their status health prior to the disaster or with disaster non-exposed people found that people exposed to disasters were significantly more likely to develop a psychiatric disorder, with posttraumatic stress disorder (PTSD) and depression being the most increased disorders (Beaglehole et al., 2018). In terms of prevalence, the rates vary considerably but PTSD is observed in 10–20% of people affected by disasters and depression in approximately 14% (Norris et al., 2002; North et al., 2012).
There is now an increasing body of evidence that has tracked the mental health of people affected by disasters over time. Using latent growth mixture modelling, a range of studies have documented different trajectories of mental health response. Studies tend to observe between three and six trajectories of response, but most include a majority class of resilient people, and smaller classes of affected people who display a chronic distress trajectory, a gradual recovery trajectory and a worsening trajectory (for a review, see Galatzer-Levy et al., 2018). One limitation of the current literature is the relatively short-term follow-up assessments of people affected by disasters. Although a number of studies have followed disaster survivors up to 6 years after the event (Chan et al., 2015; Johannesson et al., 2015; Wahlström et al., 2013), there is a need to understand long-term effects. One of the longest follow-up assessments was conducted after the Ash Wednesday bushfires that assessed children affected by the fires 20 years after the disaster and found that although these children were more at risk of subsequent psychiatric disorder than controls, this effect was not attributed to exposure to the fires (McFarlane and Van Hooff, 2009); this study did not longitudinally assess psychological responses of the children in relation to adult mental health. Following the Buffalo Creek dam disaster, a sample of litigants found that PTSD decreased from 44% at 2 years to 28% at 14 years (Grace et al., 1993, 441–449). While this literature identifies declining prevalence of disorder over the long term, questions still remain about those whose trajectories do not follow a declining path, and what factors influence worsening mental health outcomes.
The 2009 Black Saturday fires in Victoria, Australia represented one of Australia’s worst natural disasters in that they resulted in 173 deaths, 3500 buildings being damaged or destroyed and huge disruption on many communities (Government Printer for the State of Victoria, 2009). The Beyond Bushfires study aimed to study the psychological and community effects of the fires in regions variably affected by the fires (Gibbs et al., 2013). Rates of psychological disorder in the short- and medium-term post bushfire were high, although rates were influenced by the degree to which the participant’s region was impacted by the fires. For example, Wave 1 of this study conducted 3–4 years after the fires found that people in highly affected regions had higher rates of probable disaster-related PTSD (15.6%), probable depression (12.9%), severe distress (12.8%) and heavy alcohol use (24.7%) relative to those from less affected regions, and also higher than Australian normative data (Bryant et al., 2014). Wave 2 of the study was conducted 5 years after the disaster and found that over time there were decreased rates of disaster-related PTSD (8.7%), probable depression (9.0%) and severe distress (5.4%), although heavy alcohol use remained high (22.1%) (Bryant et al., 2017).
The primary aim of this study was to assess the long-term mental health of the 2009 Black Saturday fires in Victoria, Australia. Specifically, this study reports the outcomes of the 10 years Beyond Bushfires study (Wave 3), which profiles the prevalence of mental health outcomes 10 years after the fires. Second, we investigated the factors that increased risk to worsening mental health over time with a particular focus on the degree to which ongoing stressors impact on mental health.
Method
Participants
Wave 1 data were collected between April 2012 and January 2013 (3–4 years after the fires), and it recruited adults aged at least 18 years of age living in 25 communities in 10 locations in Victoria. The communities were selected because they were variably affected by the Black Saturday fires, ranging from a high level of impact in terms of lives lost and property destroyed through to communities with minimal impact. The level of disaster affectedness was operationalized as high impact (many houses lost plus fatalities; N = 630), medium impact (ranging from a small number of fatalities through to communities with no fatalities but significant property damage; N = 182) and low impact (no evidence of burning; N = 205). The 2006 census data indicated a total adult population of 7693 in the selected communities, including 702 adults in the two pilot communities. Recruitment was conducted for Wave 1 with the following procedure: details of current residents and those who relocated since the fires were provided by the Victorian Electoral Commission (VEC) (N = 7467 adults), and to comply with local privacy laws a letter was sent to each resident inviting them to participate in the study with a reply-paid envelope. A range of community and media-based activities were also conducted to raise awareness of the research and provide an opportunity for eligible people to self-register. Of those who were eligible to participate, 1017 (14%) of available people responded to this invitation and completed the survey. Participants were older, more likely to be female and more educated than the general community according to census data for these regions. At the completion of the Wave 1 survey, 966 participants agreed to be contacted for the Wave 2 survey. Wave 2 data collection was conducted between July and November 2014 (5 years after the fires), and 736 (76.1%) people participated. Given the amount of time that had passed, the VEC also assisted recruitment for Wave 3 by providing the current addresses of those of our previous participants who had agreed to be recontacted. Wave 3 data were conducted between April and August 2019 (10 years after the fires), and 525 (51.6% of those who initially participated at Wave 1) people participated.
Measures
PTSD: Probable PTSD was assessed using the Primary Care Posttraumatic Stress Disorder Checklist Screen (PCL) (Bliese et al., 2008); this scale comprises four items each scored on a 5-point scale that index DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th ed.) PTSD symptoms of PTSD in the previous 4 weeks. A cut-off 7 on this scale provides an estimation of probable PTSD diagnosis relative to the full version of the Posttraumatic Stress Disorder Checklist (Bliese et al., 2008). After each item was asked, the interviewer enquired whether the symptom comprised fire-related memories, behaviour or triggers (e.g. Did these reactions happen after reminders of the fires?). They were additionally asked if they experienced these reactions in relation to one of the traumatic events enquired about earlier in the interview (e.g. Did these happen after reminders of ...).
As was done in Waves 1 and 2, PTSD was assessed in two ways: (a) in relation to symptoms that were specific to the Black Saturday fires and (b) in relation to traumatic events generally.
Depression: Probable major depressive disorder (MDD) was assessed using the Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001). Probable occurrence of MDD was assessed if five of the nine symptoms had been present for most days in the previous 2 weeks.
Psychological distress: Psychological distress was assessed using the K6, which measures anxiety and mood problems in the previous 30 days (Kessler et al., 2003). This study followed the guidelines of the Substance Abuse and Mental Health Services Administration’s definition of probable severe mental illness (SMI) of K6 scores of 13–24 (Substance Abuse and Mental Health Administration Service [SAMHSA], 1993). Psychological resilience was defined as K6 scores of 0–6, reflecting people who enjoyed no or minimal psychological problems (Kessler et al., 2008).
Alcohol use: Alcohol use was assessed using the Consumption Scale of the Alcohol Use Disorder Identification Test (AUDIT-C) (Bush et al., 1998), a three-item self-report measure that indexes heavy drinking. This measure asks three questions regarding alcohol use, and for the purpose of this study adopted recommended cut-offs of six standard drinks for males per day and five for females were used as detection of heavy drinking; these cut-offs have sound sensitivity (males: 0.82; females: 0.84) and specificity (males: 0.79; females: 0.88) (Aalto et al., 2009).
Fire-related experiences: Participants were asked at Wave 1 (a) whether the respondent had feared for his or her own life, (b) whether anyone close to the respondents had died in the fires and (c) whether they personally lost property or buildings in the fires.
Recent traumatic events: Participants were asked to indicate whether they had been exposed to any of the following traumatic events since their last assessment (or last 5 years): (a) another fire, (b) natural disaster, (c) serious accident or (d) sudden bereavement.
Recent stressors: Participants were also asked to indicate whether they had been exposed to any of the following stressful events since their last assessment (or last 5 years): disruptions to (a) one’s income, (b) one’s accommodation or (c) one’s personal relationships.
Help-seeking: Participants were also asked if they had consulted a health professional in the past 6 months for assistance with any psychological problems.
Procedure
The University of Melbourne Human Research Ethics Committee approved the procedure. Following recontact and recruitment of previous Beyond Bushfires participants, the survey was conducted by use of telephone and web-based formats. The survey captured sociodemographic factors, experiences of the Black Saturday fires and major stressors that may have occurred since the fires. The Wave 2 and Wave 3 surveys followed the same format, with questions about stressful events focusing on the time period since the last survey. A range of questions about social connections, recovery experiences and attitudes were also included in each Wave but were not included in this analysis. The survey sequentially administered the PCL, PHQ, K6 and AUDIT-C.
Prevalence rates were calculated based on recommended cut-offs for probable PTSD, MDD, heavy drinking and SMI. To assess the extent to which people altered their status from Wave 1 to Wave 3, separate logistic regressions were conducted to predict changes in case cut-offs of general PTSD, fire-related PTSD, depression, SMI, heavy drinking and resilience. Sex, age at the time of the Black Saturday fires and highest level of education at the time of Black Saturday were entered at Step 1. Severity of fire exposure variables were entered at Step 2, including whether the respondent had feared for their own life, whether someone close to the respondent had died in the fires and the extent of property loss. At Step 3, recent life stressors experienced since the Wave 2 survey were entered to index the additional effects of subsequent adversity on Wave 3 psychological outcomes. The focus of these regressions was on delayed development of disorder (comparing participants without the disorder at Wave 1 who either did or did not have the disorder at Wave 3).
Results
Participant characteristics
Table 1 presents the participant characteristics of those retained and not retained at the Wave 3 assessment. Participants who were retained at Wave 3 did not differ from those who did not participate in terms of age, gender or whether they had experienced bereavement in the fires. Relative to those who were retained at follow-up, participants at Wave 3 were more likely to have tertiary education, more likely to have temporary housing after the fires, were more likely to fear for their life in the fires, had greater property loss in the fires and there were more participants from high-impact communities. Notably, those who were retained and those lost to follow-up did not differ in rates of fire-related PTSD (odds ratio [OR]: 1.30, 95% confidence interval [CI]: [0.88, 1.92]), general PTSD (OR: 1.16, 95% CI: [0.84, 1.59]) or depression (OR: 1.09, 95% CI: [0.74, 1.61]).
Participant characteristics by survey retention status.
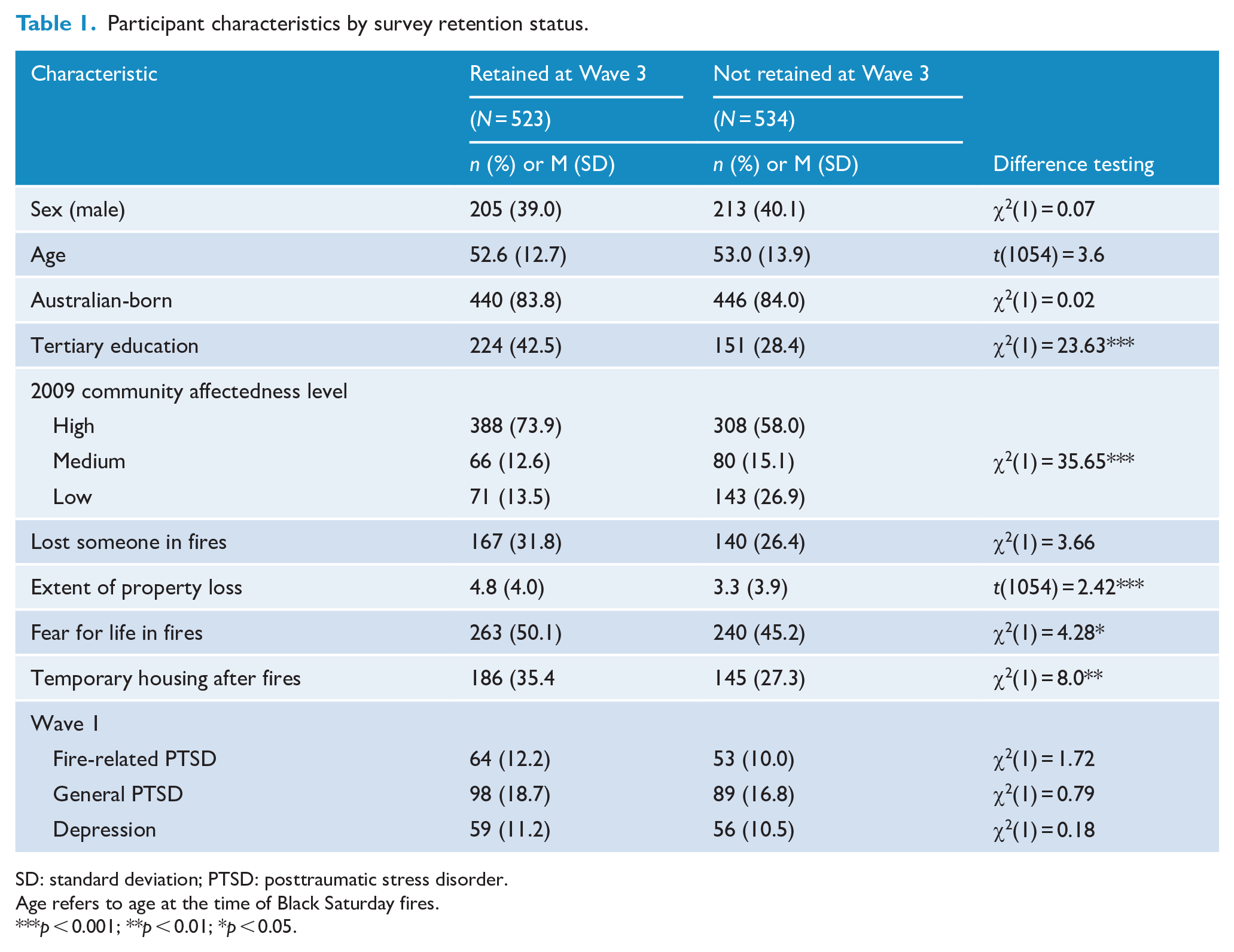
SD: standard deviation; PTSD: posttraumatic stress disorder.
Age refers to age at the time of Black Saturday fires.
p < 0.001; **p < 0.01; *p < 0.05.
Prevalence of psychological outcomes
Table 2 presents the frequencies of reported probable PTSD, MDD, heavy drinking, SMI and resilience at Wave 3, according to the level of exposure to the fires. Additionally, we report the rates of having any disorder, defined as having PTSD, MDD or SMI (we do not include heavy drinking because AUDIT-C scores do not index substance abuse disorder). In terms of PTSD linked to the Black Saturday fires, more participants in the high-affected communities reported probable general PTSD (16.8%) than those from the medium-affected (5.0%) and low-affected (7.5%) communities (OR: 1.85, 95% CI: [1.14, 3.00], p = 0.012). Similarly, participants in the high-affected communities were more likely to report MDD (9.8%) than participants in the medium-affected (3.3%) and low-affected communities (1.5%) (OR: 2.83, 95% CI: [1.20, 6.70], p = 0.017). Participants in the high-affected communities were less likely to report resilience (80.4%) than participants in medium-affected (88.3%) and low-affected communities (94.0%) (OR: 0.52, 95% CI: [0.33, 0.81], p = 0.004). Participants did not differ across affected areas in terms of fire-related PTSD, SMI or alcohol use. Overall, the rates of people suffering any psychological disorder (defined as probable PTSD, MDD or severe distress) were higher in high-affected (22.1%) than both medium-affected (6.7%) and low-affected (9.0%) regions (OR: 1.67, 95% CI: [1.16, 2.41], p = 0.006). The likelihood of developing any disorder was higher in those with heavy drinking (29.2%) than those who were not in the heavy drinking category (17.3%) (OR: 1.97, 95% CI: [1.19, 3.28], p = 0.009). In terms of those with any psychological disorder, only 24.6% had consulted a professional for assistance with this problem in the previous 6 months and 58.8% had consulted a professional since the fires occurred 10 years earlier.
Prevalence of mental health conditions and means of psychopathology measures across communities at 10 years post Bushfire disaster.
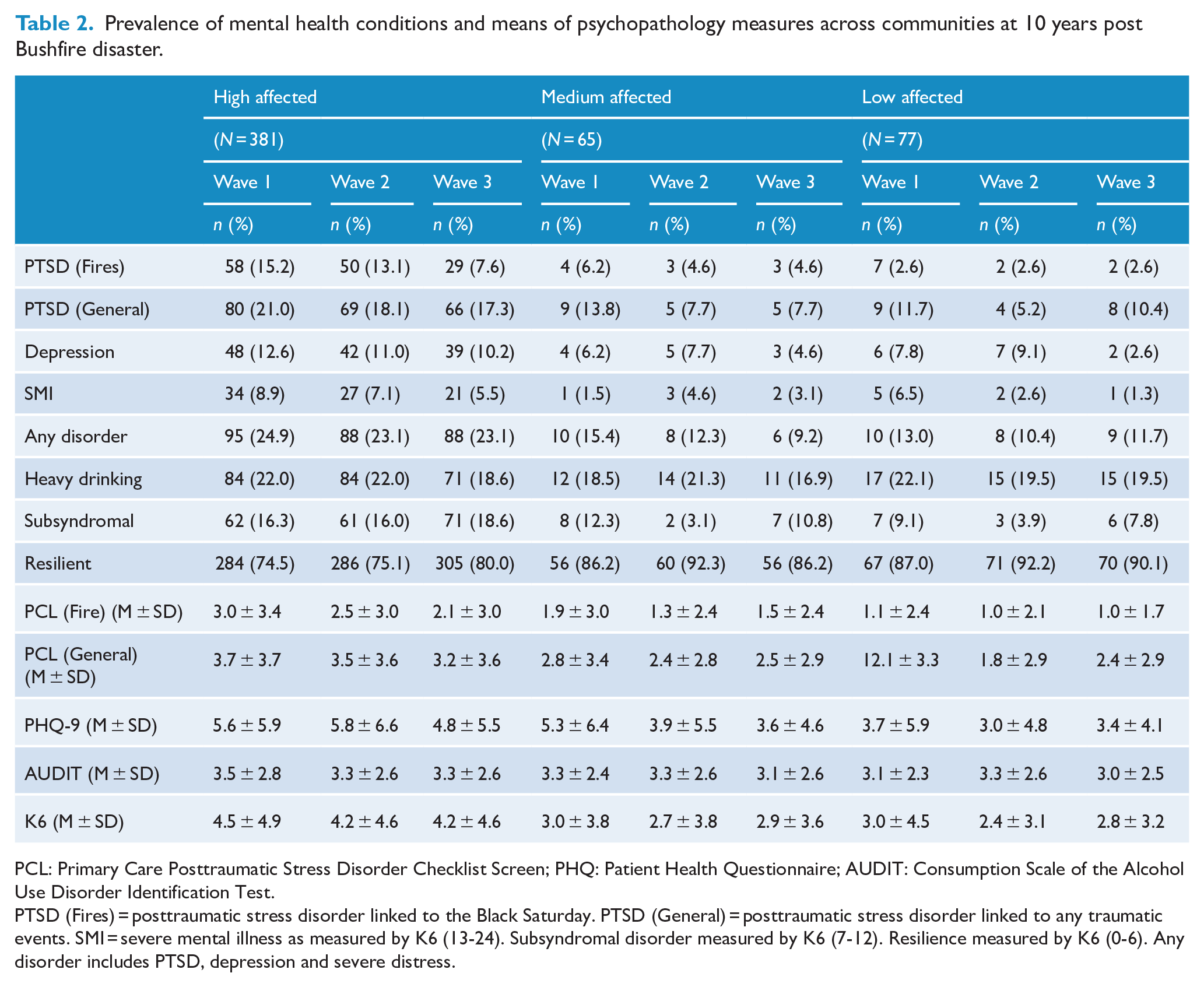
PCL: Primary Care Posttraumatic Stress Disorder Checklist Screen; PHQ: Patient Health Questionnaire; AUDIT: Consumption Scale of the Alcohol Use Disorder Identification Test.
PTSD (Fires) = posttraumatic stress disorder linked to the Black Saturday. PTSD (General) = posttraumatic stress disorder linked to any traumatic events. SMI = severe mental illness as measured by K6 (13-24). Subsyndromal disorder measured by K6 (7-12). Resilience measured by K6 (0-6). Any disorder includes PTSD, depression and severe distress.
Changes in psychological status
Table 3 reports the changing prevalence rates of psychological outcomes from Wave 1 to Wave 3. Overall, although the rates of mental health problems decreased over time, there was a consistent pattern across outcomes that people either remained being a case over time (‘Chronic’), improved from being a case at Wave 1 to not being a case at Wave 3 (Recovering), not being a case at Wave 1 but being a case at Wave 3 (Worsening) and never being a case (No caseness). Lower rates were observed at Wave 3 compared to Wave 1 for probable fire-related PTSD (6.2% vs 12.2%, χ2 = 91.25, p < 0.001), general PTSD (14.9% vs 18.7%; p = 0.03) and severe distress (4.4% vs 7.5%, p = 0.01). Consistent with this pattern, the rates of resilience increased over time (77.8% vs 82.4%, p = 0.02). In contrast, rates were comparable over time for MDD (8.3% vs 10.9%, p = 0.09) and severe alcohol use (18.5% vs 21.8%, p = 0.06).
Prevalence of mental health conditions in Wave 1 and Wave 3 (n = 523).
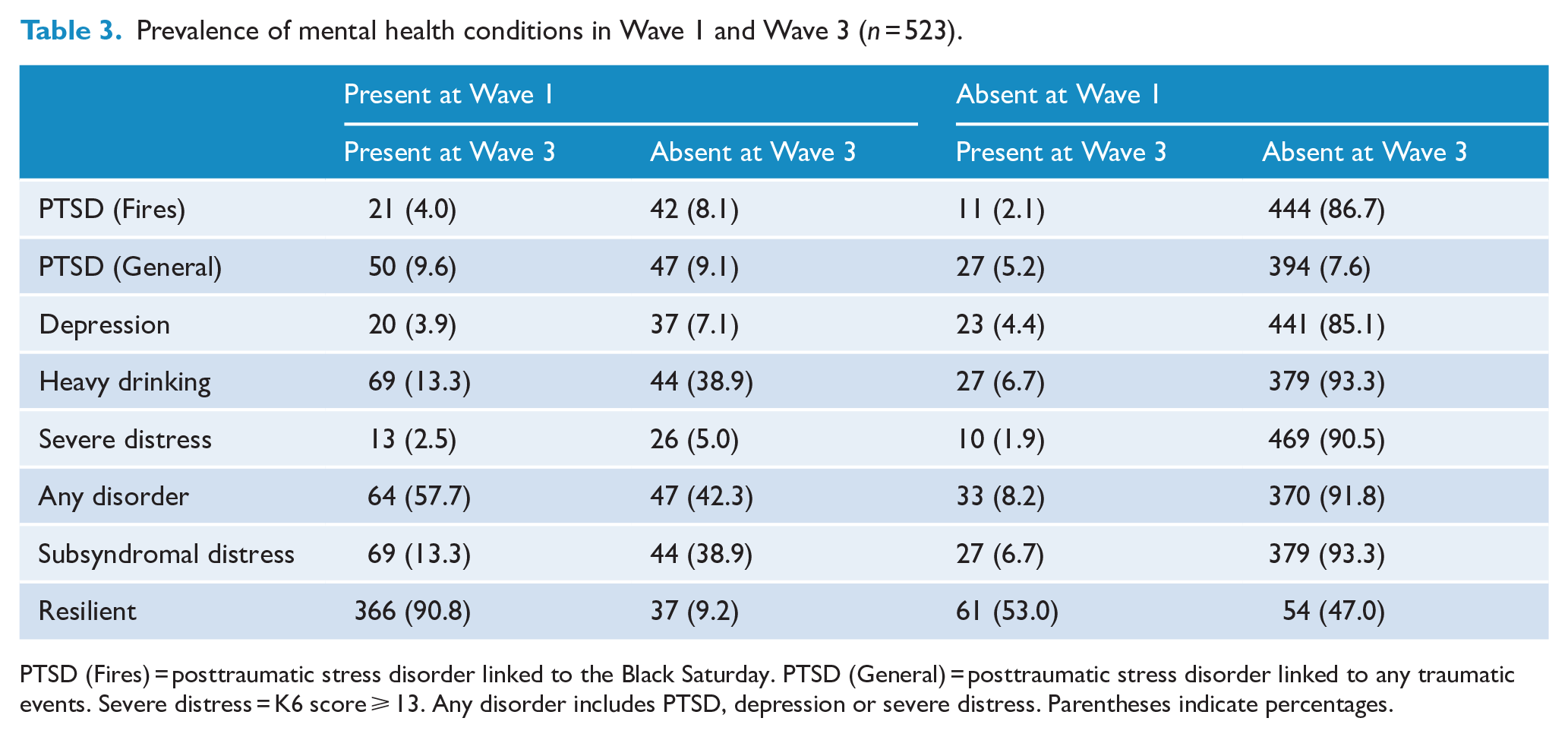
PTSD (Fires) = posttraumatic stress disorder linked to the Black Saturday. PTSD (General) = posttraumatic stress disorder linked to any traumatic events. Severe distress = K6 score ⩾ 13. Any disorder includes PTSD, depression or severe distress. Parentheses indicate percentages.
The effects of socio-demographic, fire-exposure and post-fire stressors on worsening and improving psychological outcomes from Wave 1 to Wave 3.
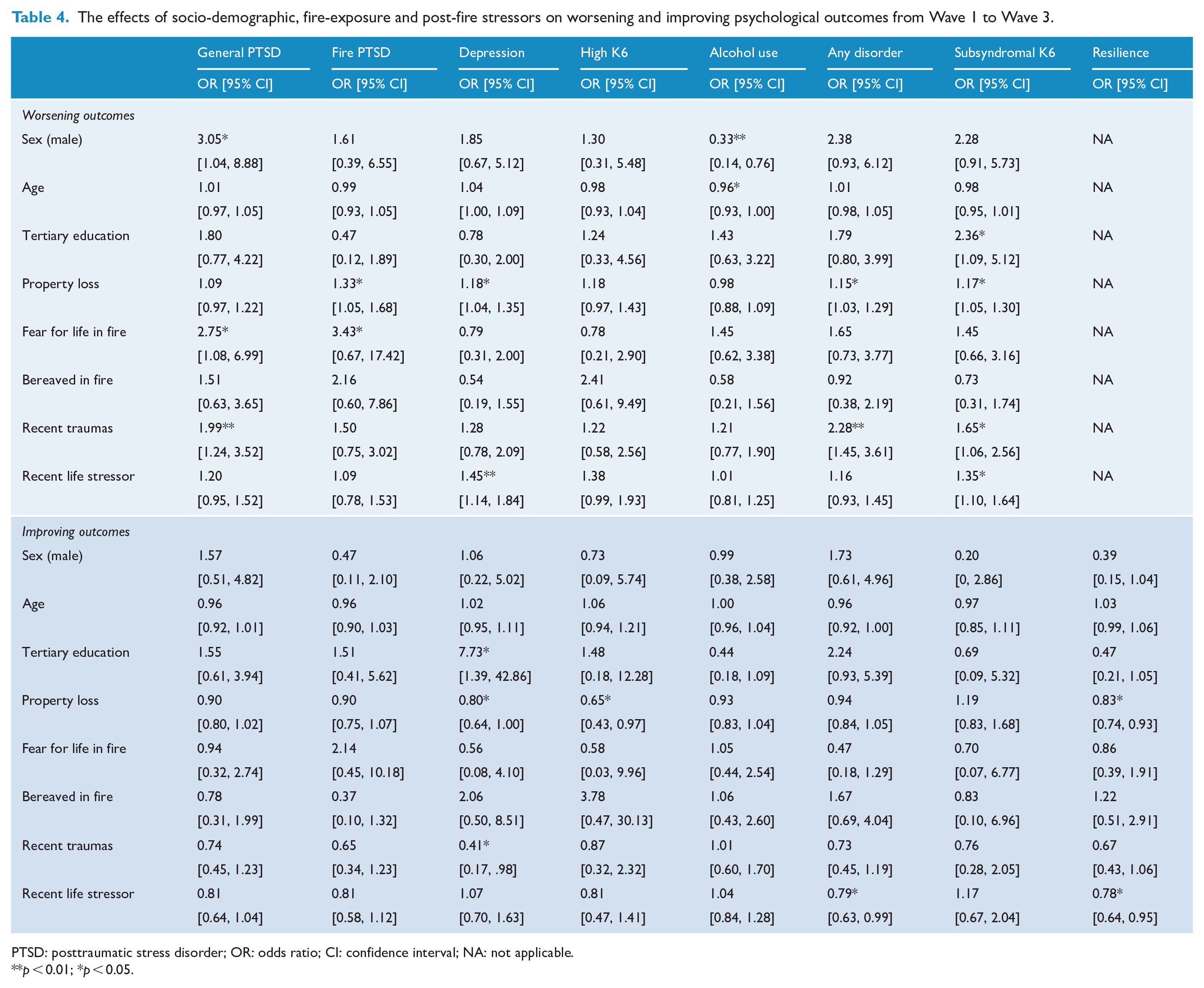
PTSD: posttraumatic stress disorder; OR: odds ratio; CI: confidence interval; NA: not applicable.
p < 0.01; *p < 0.05.
To demonstrate the course of PTSD over time, Figure 1 shows the rates of general PTSD, fire-related PTSD and depression at Waves 1, 2 and 3, including the changing status of participants over time for those participants with three waves of data. This figure demonstrates that there was considerable fluctuation over time in terms of participants’ PTSD status. Approximately 50% of those with either of the disorders at Wave 2 did not have the disorder at Wave 1, and similarly half of those with the disorder at Wave 3 did not have the disorder at Wave 2. In contrast, most people who did not have the disorder maintained this status over the following assessments, with less than 10% of people who did not have PTSD displaying PTSD at the subsequent assessment.
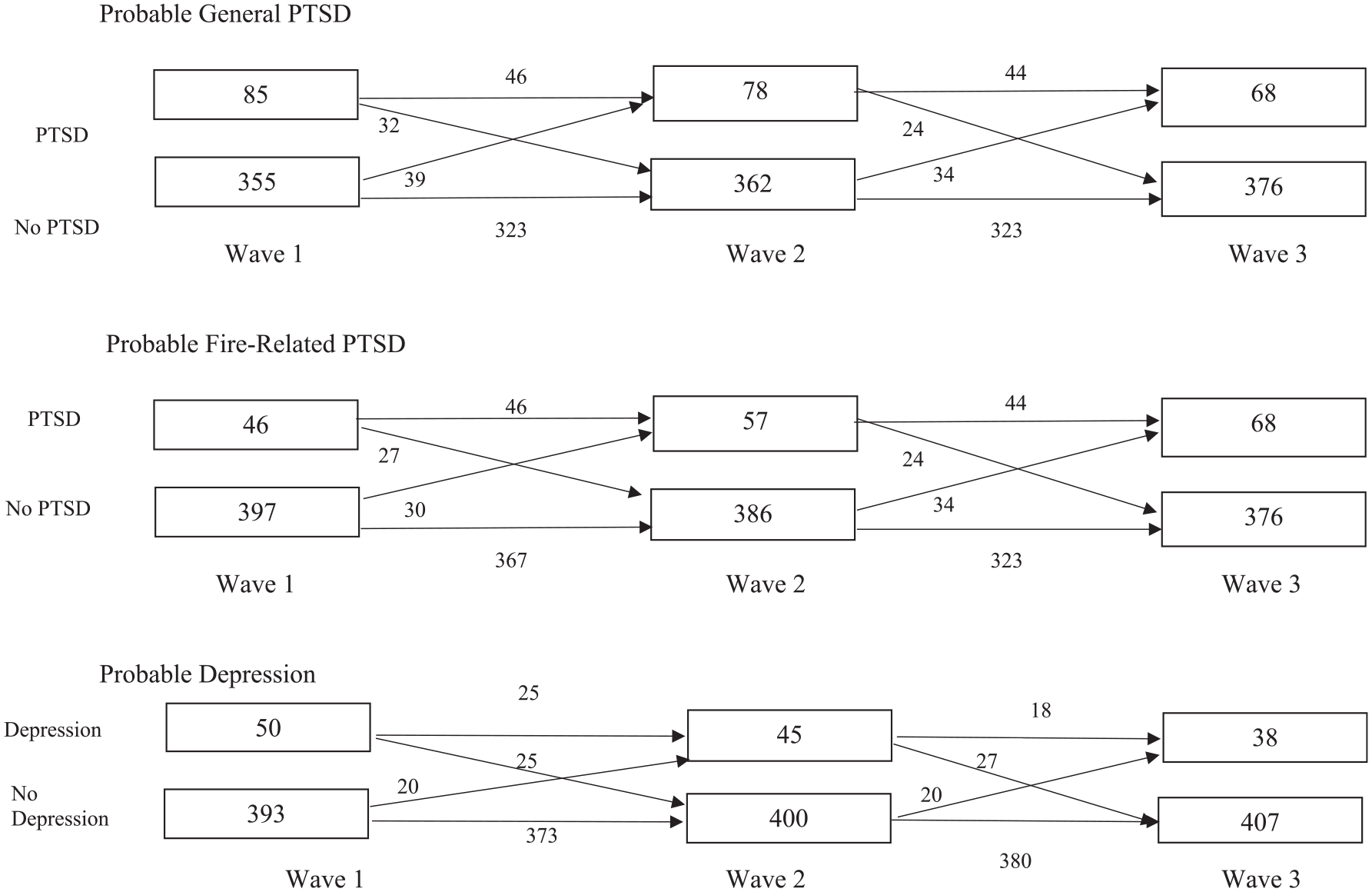
Course of general PTSD, fire-related PTSD and depression over Wave 1, Wave 2 and Wave 3.
Predictors of changing psychological outcomes
In terms of changing mental health status across time, we calculated the adjusted ORs for PTSD, MDD, heavy drinking, psychological distress and resilience for the Chronic, Recovering, Worsening and No Caseness categories. Specifically, we calculated ORs for those (a) who did not meet the cut-offs at Wave 1 but did meet them at Wave 3 and (b) who did meet the cut-offs at Wave 1 but did not meet them at Wave 3 (see Table for Worsening and Recovering categories; Chronic and No Caseness categories are presented in Table S1, Supplementary Materials). In terms of fire-related PTSD, worsened outcome was predicted by worse property loss. In terms of general PTSD, worsened outcome was predicted by female gender, greater fear for one’s life during the fires and more frequent subsequent traumatic events. Worsening depression was predicted by worse property loss and more subsequent stressful life events. Younger age predicted worsening alcohol use. There were no significant predictors of improving fire-related or general PTSD. Improving depression was predicted by better education, less property loss and few subsequent traumatic events; reduced severe distress was predicted by less property loss; and reduced resilience was predicted by more property loss and more stressful life events. There were no predictors of maintaining fire-related or general PTSD over time. Maintenance of depression was predicted by less education, more property loss and more recent traumatic events, and maintaining severe distress was predicted by more property loss. Maintenance of resilience was predicted by less property loss and fewer stressful life events.
Discussion
The first point to note in these findings is that most people affected by the Black Saturday fires, including those from high-impact regions, were displaying resilience at each assessment. This accords with much evidence that following traumatic events most people adapt and do not experience marked psychological problems (Galatzer-Levy et al., 2018). Despite this pattern, the rates of probable PTSD, depression and severe distress observed 10 years following the fires indicate that the rates of psychological problems in the highly affected regions remain higher than would be expected for an Australian community. The 2007 Australian National Survey of Mental Health and Wellbeing observed a rate of probable PTSD of 4.4% (McEvoy et al., 2011), which is markedly lower than observed in the high-affected communities in this survey; we note, however, that the rate reported in this study is based on 4-week point prevalence whereas the national survey obtained 12-month prevalence rates. These findings are consistent with prior reports of long-term mental health consequences of disasters (North et al., 2011). It is also interesting to note that the rate of general PTSD was higher in fire-affected areas than medium-affected areas; this observation accords with evidence that people severely affected by trauma, and who develop PTSD, are more likely to be subsequently exposed to traumatic events and develop PTSD (Breslau et al., 2008). This pattern may be explained by sensitization models that propose that exposure to a stressful event triggers sensitization of neural circuitry to be more reactive to subsequent traumatic events (McFarlane, 2010). This proposal accords with evidence that prior trauma is associated with more reactive responses to subsequent stressors (Breslau et al., 1995).
Although rates of PTSD 10 years after the fires had declined related to rates 5 years earlier, they were still higher than rates reported in Australian epidemiological community studies (McEvoy et al., 2011). This pattern accords with many reports that PTSD rates in the initial period after a disaster are higher than follow-up periods (Galea et al., 2003; van Griensven et al., 2006). Whereas these studies typically observe a decline in PTSD after the initial months of a disaster, this study documented a decline in PTSD between 5 and 10 years after the fires. In the Australian context, an early longitudinal study of firefighters after the Ash Wednesday fires found that rates of acute PTSD were lower relative to rates of subsequent delayed-onset PTSD (McFarlane, 1988); this study differs markedly from the current cohort, however, because firefighters tend to have a distinct trauma history, organizational culture and exposure to ongoing stressors. This pattern indicates that even after a prolonged period, the rate of PTSD tends to abate over time. In contrast, depression and substance abuse rates remained stable. Problematic alcohol use levels were not different between affected regions, and so the possibility exists that these rates reflect alcohol use rates that are independent of the fires; this observation accords with numerous previous studies that observed no change in substance abuse following disasters (Bravo et al., 1990; Fergusson et al., 2014). The observation that depression did not decline in the manner that PTSD did highlights that depressive responses followed a different pattern than PTSD; prior studies have shown that depression can persist or even increase after a disaster (Geng et al., 2018; Goenjian et al., 2011). Persistent depression after disaster is associated with negative life events (Geng et al., 2018), and it is possible that stressors in the aftermath of the fires have contributed to elevated levels of depression; this interpretation is supported by the observation that increased depression over time was associated with number of recent life stressors.
Although we observed these rates of probable disorder over time, it is important to note that people’s mental health fluctuated over time. Approximately half of people shifted from having PTSD or depression at each assessment to not having the condition at the following assessment; similarly, significant proportions of those who did not have these probable disorders at an assessment reported having the disorder at the subsequent assessment. The fluctuating nature of PTSD has been previously reported in longitudinal studies of PTSD after traumatic injury (Bryant et al., 2013; Steinert et al., 2015; Wang et al., 2013). One important implication of this finding is that commonly reported prevalence rates of psychological disorders after disasters should be considered cautiously because the people that are identified as experiencing psychological difficulties may not be the same people as those identified at a different time point.
From a public health perspective, one of the concerning findings in this study is that a proportion of those affected by the fires developed a deterioration in their mental health over time. Worsened fire-related PTSD was associated with the extent of property loss in the fires, which also predicted worsening and maintenance of depression, and maintenance of severe distress. The role of property loss may be attributed to long-term effects of difficulties in rebuilding, insurance issues and financial problems, which occurs commonly after disasters and may be a key factor in poor mental health (Kessler et al., 2003). Subgroup analyses of those who relocated away from their community could not be conducted because of insufficient numbers; however, it is noteworthy that a finding from a prior wave of this cohort found that property loss was associated with greater likelihood of relocation but an associated cost of this move was reduced connection with one’s community (Gibbs et al., 2016). That is, it is possible that property loss was associated with poorer subsequent mental health because of reduced social support. An interesting pattern emerged regarding recent stressors in that whereas worsened general PTSD was associated with recent traumatic events; deterioration in depression was associated with recent life stressors. This distinction suggests that the nature of stressful events can impact the nature of one’s post-disaster mental health, with traumatic exposures contributing to PTSD reactions. The pattern of post-trauma stressors impacting on one’s subsequent mental health accords with evidence from studies of delayed-onset PTSD that have shown that the worsening of PTSD is associated with significant stressors occurring in the wake of trauma (Andrews et al., 2007; Bryant and Harvey, 2002). It should be noted, however, that traumatic events can also impact depression, as reflected in the findings that recent traumatic events predicted maintenance of depression and few traumatic events was associated with improved depression. This pattern accords with meta-analytic evidence that negative life events are a major risk factor for depression (Liu et al., 2019). In the context of disasters, numerous studies have found that the stressors that occur in the aftermath of a disaster contribute to the long-term mental health of those affected (Kessler et al., 2008; Lewin et al., 1998; Pietrzak et al., 2013). Of particular relevance to the long-term effects of recent stressors on mental health, there is also evidence that the adverse effects of major stressors can intensify as time progresses (Cerda et al., 2013). In this context, it is worth noting that many people affected by disasters, including those of the Black Saturday fires, deal with many long-term stressors such as economic downturn, unemployment, rebuilding and insurance difficulties, and social disruption to communities. This interpretation is supported by the finding that worsening of fire-affected PTSD and depression were also predicted by the extent of property loss, which may have compounded subsequent financial, insurance and re-settlement stressors. Other post-disaster studies have reported that poor mental health is influenced by the extent of financial stressors experienced by those who are fire affected (Cerda et al., 2013; Galea et al., 2008).
A decade after the fires only one-quarter of those with probable PTSD, depression or severe distress had consulted a health professional for their condition in the previous 6 months. This pattern has been documented frequently in prior disaster research (Boscarino et al., 2004a, 2004b). This is a worrying statistic in the wake of the Black Saturday fires because government services were targeted in the affected regions to provide mental health services. It is possible that people affected by disasters have persistent disorders because they have not accessed sufficient mental health assistance. The lack of mental health assistance may be attributed to stigma about accessing mental health services, logistical barriers such as distance or cost, or the inability to detect when a person is suffering a mental health condition. We also note that the possibility that those with persistent problems 10 years after the fires may have not responded positively to prior treatments and subsequently tolerate poor mental health.
Several methodological issues need to be acknowledged. First, privacy laws required a recruitment strategy that resulted in only 16% of people in the targeted regions participating in the study. We have previously reported that participants were older, more likely to be female and more educated than other community residents (Bryant et al., 2014), thereby raising questions over the generalizability of the current findings. We also note that we do not have representative data from comparable population groups using measures employed in this study, and so we cannot estimate the extent to which our sampling resulted in a biased cohort. Relatedly, only 52.6% of the original sample was recruited at Wave 3, and these people had more tertiary education, and were more likely to have temporary housing after the fires, to have feared for their life in the fires, had greater property loss in the fires and come from high-impacted communities than those who were not retained. Greater retention at Wave 3 would also have allowed a larger sample that could provide examination of movement between diagnostic categories across time. Second, we emphasize that the survey instruments used in this study were not structured clinical interviews, and so it is probable that the observed rates of probable disorder may inflate actual incidence of mental health problems (North, 2014). Third, brevity of the survey precluded detailed assessment of exposure to a range of traumatic events, such as interpersonal trauma, which is a strong risk factor for PTSD (Forbes et al., 2012). Fourth, we recognize that the time frame between Waves and 1 and 3 spanned 7 years, and it is possible that people fluctuated in their psychological status on numerous occasions in this period. Fifth, the survey was unable to include the impact of treatment, or type of treatment, on subsequent mental health. Sixth, Wave 1 did not occur till 3 years after the fires and so this study is not able to map the psychological sequelae occurring in the initial months and years after the fires; our focus on chronic reactions needs to recognize much evidence that the acute period is marked by considerable fluctuation in psychological disorders, with a tendency to remission of initial PTSD reactions (Galea et al., 2003; van Griensven et al., 2006). Our design also did not allow for assessment of pre-existing psychological disorders, and so the extent that disorders were directly a function of the fires is uncertain; this possibility is mitigated by the relative lower rates in low-affected regions.
In summary, these findings indicate that there is a significant proportion of people affected by the Black Saturday fires who experience persistent mental health issues 10 years after the fires. It appears that apart from the lingering effects of sustaining extensive property damage in the fires, worsening mental health is linked to ongoing life stressors that have persisted since the fires. This pattern highlights the need for government to recognize that planning for mental health responses after natural disasters should not be focused exclusively on the initial year after a disaster but that mental health will need to be addressed for years after the event. In the context of recent natural disasters in Australia, and the ongoing threat of climate-related disasters in the future, there is a need for long-term and strategic planning on how to optimally support the mental health of those affected by natural disasters.
Supplemental Material
Supplementary_Table_S1 – Supplemental material for The dynamic course of psychological outcomes following the Victorian Black Saturday bushfires
Supplemental material, Supplementary_Table_S1 for The dynamic course of psychological outcomes following the Victorian Black Saturday bushfires by Richard A Bryant, Lisa Gibbs, H Colin Gallagher, Phillipa Pattison, Dean Lusher, Colin MacDougall, Louise Harms, Karen Block, Greg Ireton, John Richardson, David Forbes, Robyn Molyneaux and Meaghan O’Donnell in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The original Beyond Bushfires study was funded by an Australian Research Council Linkage Grant (LP100200164) including financial and in-kind contributions from Linkage partners Victorian Department of Health, Australian Red Cross, Australian Rotary Health, Australian Government Department of Human Services (Centrelink), Phoenix Australia: Centre for Posttraumatic Mental Health, and six Primary Care Partnerships: Central Hume, Bendigo Loddon, North East, Outer East, Central West Gippsland, Lower Hume. Additional salary support from the Jack Brockhoff Foundation is also acknowledged. The 10 years Beyond Bushfires study (Wave 3) was funded by Emergency Management Victoria, Victorian Department of Health and Human Services and Australian Red Cross.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.