
Abstract
Over 400,000 Australians have an intellectual disability (ID) (Australian Bureau of Statistics, 2009) and the majority of these individuals (57%) have a psychiatric disability or mental disorder (Australian Bureau of Statistics, 2010). Compared to the general population, people with an ID experience very poor health, characterised by higher mortality (Bittles et al., 2002), and elevated rates of common mental disorders (Einfeld et al., 2011; Smiley et al., 2007) including schizophrenia and the dementias. Serious mental illnesses such as schizophrenia appear to have an earlier onset in people with an ID, pointing towards a specific developmental vulnerability to mental illness and the importance of timely access to psychiatric services for this group (Morgan et al., 2008).
These statistics make people with an ID among the most important of minority groups for mental health service providers. However, current service provision to people with an ID in Australia lags behind internationally accepted practice. This has a substantial impact on families, carers and consumers, who report that mainstream mental health services do not readily accommodate their needs, and that in some instances these services exclude individuals on the basis of ID.
Barriers to accessible mental health services for people with an ID
Potential barriers to accessing effective mental health care for people with an ID in an Australian context include: lack of knowledge regarding the substantial epidemiological data on the prevalence of mental illness in people with an ID; lack of data on the interaction between, and distinct roles and responsibilities of, disability and mental health services; lack of training and confidence of mental health professionals (Edwards et al., 2007); poor understanding by carers (Moss et al., 1997) and disability and mental health workers of the manifestations of mental disorders in people with an ID (Costello et al., 2007); lack of coherent service models and funding for ID mental health services; lack of coordination between services and treating agencies (Cohen, 2010); and lack of specific inclusion of people with an ID in mental health policy.
Australian research demonstrates the impact of these barriers. A cohort of children and adolescents with ID followed for 14 years demonstrated that just 10% of those with a mental disorder received appropriate intervention (Einfeld et al., 2006). This compares unfavourably with access to mental health support for those in the general population with mental illness, which has been estimated to be about 35% over a 1-year period (Slade et al., 2009). Unless affirmative action is taken, successive generations of people with an ID will continue to manifest high levels of mental disorders which will further erode the opportunity for a ‘contributing life’.
Understanding the high rates of mental disorders
Vulnerability to mental disorders in people with an ID is conferred by a variety of biological, psychological and social risk factors, which are readily understood by mental health professionals. Specific genetic conditions associated with ID can increase the risk of psychopathology, as can developmental brain abnormalities and pharmacological treatments and their side effects. People with an ID are also at increased risk of a range of physical health conditions that may increase the risk of mental ill health. The presence of an ID usually affects a person’s coping skills and autonomy, creating greater susceptibility to stress, and thereby increasing psychological vulnerability. Further risk arises from the reduced opportunities to engage in a range of life choices as well as restricted social networks that people with an ID often experience. Other social factors that impact mental health include poverty, a higher likelihood of contact with the criminal justice system, negative experiences during schooling, and financial and emotional strain within the family. Furthermore, people with an ID experience higher rates of physical and sexual abuse, which can further magnify their vulnerability to mental ill health. This complex set of vulnerabilities provides a quintessential challenge, which transcends disability and health service systems and demands a comprehensive inter-agency program of research and interventions.
Is there an imperative for change?
International human rights and national policy developments strongly support a case for addressing the mental health inequities affecting people with an ID. The United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) (United Nations, 2006), which was ratified by Australia in 2008, states that ‘persons with disabilities have the right to the enjoyment of the highest attainable standard of health’, and have a right to equal access to health services (Article 25) (United Nations, 2006: 18). Furthermore, under the UNCRPD there is an obligation for States Parties to ‘undertake to collect appropriate information, including statistical and research data, to enable them to formulate and implement policies to give effect to the present Convention … and to identify and address the barriers faced by persons with disabilities in exercising their rights’ (Article 31) (United Nations, 2006: 19). The National Disability Strategy (Commonwealth of Australia, 2011) commits government to action by including a key outcome related to the highest attainable health and well-being outcomes for people living with disability. The Strategy further specifies that all health services should be able to meet the needs of people with disabilities and that universal reforms, including in mental health services, should be undertaken to address the needs of people with disabilities, their families and carers.
Recent directions in disability and mental health policy assist in framing a process of change. The National Disability Insurance Scheme (Productivity Commission, 2011) provides a new approach to disability service provision for people with an ID. As highlighted by Williams and Smith in this edition of the Journal (Williams and Smith, 2014), the potential for enhanced support for those with a disability arising from a psychiatric condition has drawn the attention of the mental health sector and highlights the strong complementarity between health and disability systems. The renewed focus by mental health on the disability service system may bring side benefits, including a willingness for renewed engagement in the mental health service provision for people with an ID. The National Standards for Mental Health Services (Commonwealth of Australia, 2010), which sits under Australia’s National Metal Health Strategy, stipulates that services should be diversity responsive, including to people with an ID (Standard 4), and should ensure equity of access. Services are called on to consider the needs of carers, including specifically the carers of people with an ID (Standard 7). Further, The Roadmap for National Mental Health Reform (Council of Australian Governments, 2012) specifies action to address the prevention of mental illness in people with an ID and to reduce barriers to access to mental health services for people with disabilities. Such robust imperatives open the way for initiatives that enable mental health services and providers to meet these fundamental obligations.
What are the key elements of an effective system for people with an ID?
The key elements of mental health reform that will improve access to quality mental health services for people with an ID have been recently identified. The Australian Government Department of Health funded a National Roundtable on the Mental Health of People with Intellectual Disability (NSW Council for Intellectual Disability, 2013), which was held in May 2013 at the Australian National University. This initiative was led by the NSW Council for Intellectual Disability in collaboration with the Department of Developmental Disability Neuropsychiatry (The University of New South Wales), the Queensland Centre for Intellectual and Developmental Disability (The University of Queensland) and the Australian Association of Developmental Disability Medicine. The Roundtable brought together 95 opinion leaders from around Australia, including the Chair and CEO of the National Mental Health Commission; the Disability Discrimination Commissioner; presidents of the Royal Australian and New Zealand College of Psychiatrists (RANZCP), the Royal Australian College of General Practitioners, and the Paediatric and Child Health Division of the Royal Australasian College of Physicians; senior public servants from mental health, disability and schools; chief psychiatrists; parents and advocates of people with an ID, and senior clinicians from different professional groups.
Roundtable participants completed surveys and focus groups which generated eight key elements of an effective mental health system for people with an ID. These eight elements were detailed in a communiqué (NSW Council for Intellectual Disability, 2013) as: (1) the inclusion of ID mental health in all mental health initiatives; (2) prevention and timely intervention; (3) equitable access to and skilled treatment by mental health services; (4) specialist intellectual disability mental health services to support mainstream services; (5) collaboration between disability, schools, mental health and other agencies; (6) workforce education and training; (7) enhanced data collection; and (8) the addressing of contributors to multiple disadvantage. Priorities for action were established under each of these domains and immediate priorities that build on existing initiatives were defined. This initiative serves as a template to promote the development of a mental health service system, which meets the needs of people with an ID. Key to progress is the universal incorporation of the needs of people with an ID in mental health policy frameworks and in service enhancements.
A practical framework for mental health service providers
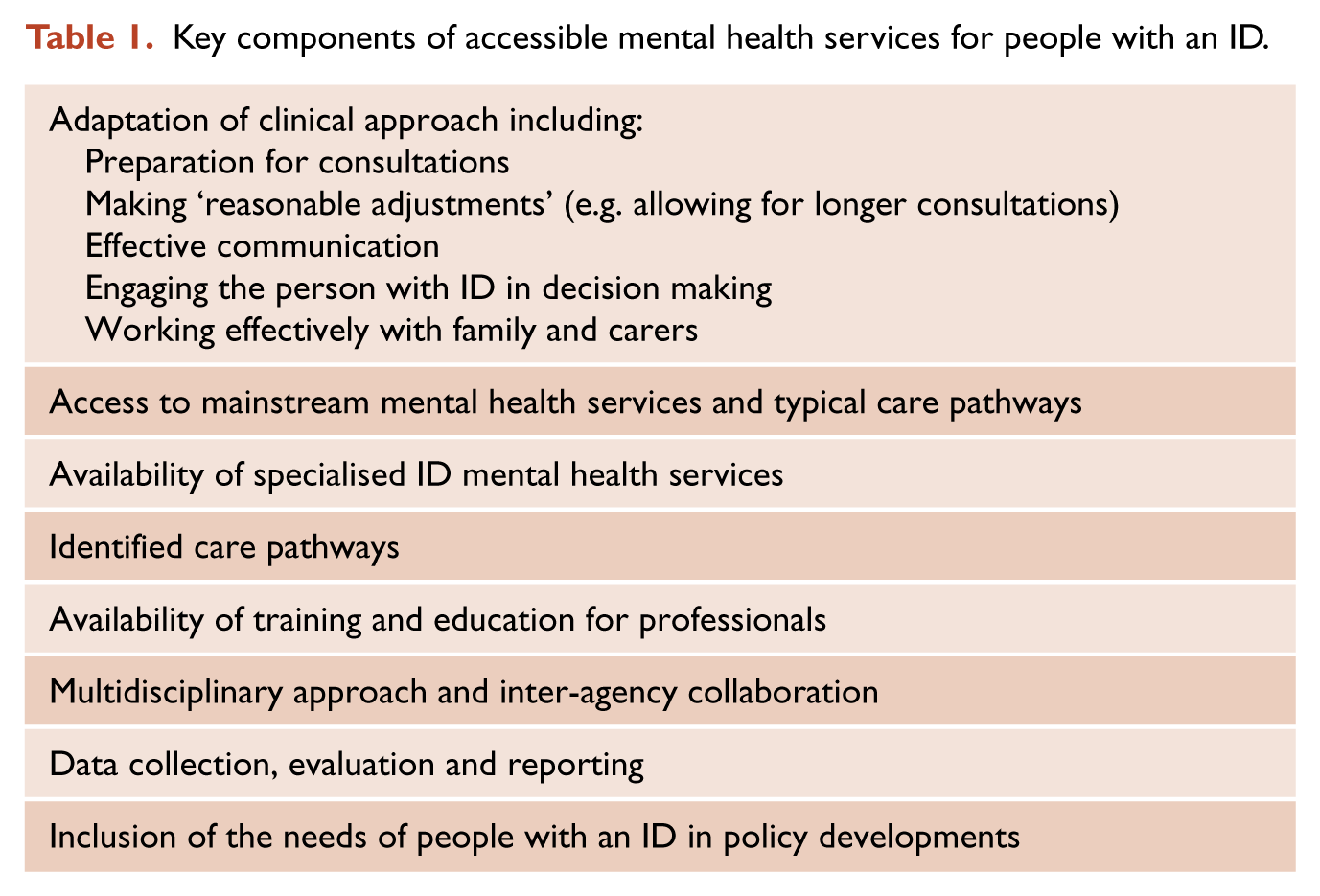
In addition to the Roundtable, the Australian Government Department of Health funded the development of Accessible Mental Health Services for People with an Intellectual Disability: A Guide for Providers (The Guide) (Department of Developmental Disability Neuropsychiatry, 2014), which will be formally launched at the RANZCP 2014 Congress by the RANZCP President. The Guide is a practical framework that will assist mental health professionals to improve access to, and quality of mental health care for, people with an ID. The Guide is underpinned by a set of principles which include human rights, inclusion, person-centred approaches, promotion of independence and recovery-oriented and evidence-based practice. Key components of accessible mental health services are outlined in Table 1. The Guide further specifies practical implications for both mental health service organisations and for individual mental health professionals. This document will provide a template that can guide mental health services and professionals in their approach to enhancing the accessibility of mental health services for people with an ID. It has been designed as the first in a series of resources which includes an as yet unfunded implementation toolkit, as well as a self-audit tool and a resource to inform carers, families and consumers of the obligations of mental health service providers.
Key components of accessible mental health services for people with an ID.
The roles and responsibilities of the RANZCP
RANZCP has an opportunity to play a key role in improving access to quality mental health care for people with an ID. Significant progress to date includes the establishment by the General Council of the RANZCP Special Interest Group in Psychiatry of Intellectual and Developmental Disabilities (SIGPIDD) in late 2010. Despite its recent formation, the SIGPIDD binational committee and SIGPIDD members have already made substantial contributions to College life, including to the annual congress program, the competency base fellowship program, and to the development of key policies. Support by the RANZCP of future initiatives, such as the establishment of a Section, formal training and subspecialty recognition of the Psychiatry of Intellectual and Developmental Disability, will be pivotal to enhancing the accessibility of specialist mental health services for people with an ID. Further, the RANZCP has a key advocacy role to ensure that the interests of people with an ID and mental illness are fully recognised under the National Disability Insurance Scheme, and that mental health and disability systems work in complementary ways rather than in traditional silos. This will be particularly important for those at the margins, including those with multiple and complex disabilities, those with additional psychosocial disadvantage, aboriginal Australians with ID, and people with an ID at risk of engaging in offending behaviours.
Conclusions
People with an ID have a disproportionate mental health burden but experience significant barriers to accessing services and appropriately trained practitioners. People with an ID have the right to the highest attainable standard of mental health care, but current Australian mental health policy, service systems and practice fail to meet these fundamental human rights obligations. A number of recent developments suggest substantial scope for reform in this area. The Roundtable communiqué features high-level endorsement of key elements of an effective mental health system for people with an ID, and sets priorities for action which can be monitored. The Guide is seen as one of the first steps in this longer process of incremental reform. It will provide practical assistance for services and practitioners who are willing to make adjustments to systems and practice to benefit people with an ID. High-level support for reform in this area has been a feature of the RANZCP response and suggests willingness for re-engagement by psychiatry in this area. Concerted action by government, policymakers, services and practitioners is required if equity of access to mental health services is to be achieved for people with an ID.
Footnotes
Acknowledgements
The author gratefully acknowledges the work of Andrea Ching on the development of Accessible Mental Health Services for People with an Intellectual Disability: A Guide for Providers.
Funding
The development of Accessible Mental Health Services for People with an Intellectual Disability: A Guide for Providers (The Guide) was supported by funding from the Australian Government Department of Health.
Declaration of interest
The author was a co-convener of the National Roundtable on the Mental Health of People with Intellectual Disability, is an executive member of the RANZCP Special Interest Group in Psychiatry of Intellectual and Developmental Disabilities, and is Vice-President of the Australian Association of Developmental Disability Medicine.