
Abstract
Objective:
Results from studies examining associations between serum 25-hydroxyvitamin D (25(OH)D) concentrations and depressive symptoms are equivocal. We investigated the relationship between serum 25(OH)D concentrations and symptoms of depression, anxiety and stress in a cross-sectional analysis of a population-based sample of young adults participating in the Western Australian Pregnancy Cohort (Raine) Study.
Methods:
Participants provided a blood sample at the 20-year follow-up (March 2010-April 2012) for the measurement of serum 25(OH)D concentrations. Mental health symptoms were assessed using the 21-item Depression Anxiety Stress Scales (DASS-21). Associations between serum 25(OH)D concentrations and total DASS-21 scores and subscale scores of depression, anxiety and stress were explored in males and females using negative binomial regression, adjusting for age, race, body mass index (BMI) and physical activity (n=735). Models examining subscale scores were also adjusted for the other subscale scores.
Results:
After adjusting for confounders, an increase in serum 25(OH)D concentrations of 10 nmol/L decreased total DASS-21 scores in males by 9% (rate ratio (RR) 0.91; 95%CI 0.87,0.95; p<0.001) and depression subscale scores in males by 8% (RR 0.92; 95%CI 0.87,0.96; p=0.001). However, in adjusted models there were no significant associations between serum 25(OH)D concentrations and symptoms of anxiety and stress in males. There were no significant associations between serum 25(OH)D concentrations and symptoms of depression, anxiety and stress in females.
Conclusions:
We found an association between serum 25(OH)D concentrations and symptoms of depression, but not anxiety and stress, in males. Randomised controlled trials are necessary to determine any benefit of vitamin D supplementation in the prevention and treatment of depressive symptoms in young adults.
Introduction
Vitamin D may play an important role in mood disorders. Vitamin D appears to be involved in brain function and it has been suggested that it acts as a neurosteroid (Eyles et al., 2005; Garcion et al., 2002; McGrath et al., 2001). Vitamin D metabolites can cross the blood-brain barrier and vitamin D receptors (VDR) have been identified in neuronal and glial cells in the central nervous system (Eyles et al., 2005). Regions of the brain that are associated with the pathophysiology of mood disorders, such as the amygdala, hippocampus, hypothalamus and the dopaminergic neurons of the substantia nigra, carry VDR and 1α-hydroxylase – the enzyme responsible for converting 25-hydroxyvitamin D (25(OH)D) into the active form of vitamin D (Drevets et al., 2008; Eyles et al., 2005). Mice lacking VDR have substantial behavioural impairment and increased anxiety compared with VDR-replete mice (Kalueff et al., 2006; Minasyan et al., 2007). Evidence from animal studies also supports a role of vitamin D in the expression of monoamines likely to be involved in depression, including norepinephrine, serotonin and dopamine (Cass et al., 2006; Garcion et al., 2002; Smith et al., 2006).
A number of epidemiological studies have found associations between serum 25(OH)D concentrations and depression, independent of lifestyle and health factors (Ganji et al., 2010; Hoang et al., 2011; Jamilian et al., 2013; Kjaergaard et al., 2011; Lee et al., 2011; Milaneschi et al., 2010; Tolppanen et al., 2012). However, others have shown no association, including a large population-based study in the United States (Nanri et al., 2009; Pan et al., 2009; Zhao et al., 2010). Many of these studies were conducted in middle-aged to elderly adults, with limited data available in young adults. Furthermore, serum 25(OH)D concentrations have not been widely examined in relation to anxiety and stress. We investigated the relationship between serum 25(OH)D concentrations and symptoms of depression, anxiety and stress in a cross-sectional analysis of a population-based cohort of young adults. It was hypothesised that low serum 25(OH)D concentrations would be associated with elevated depressive, anxiety and stress symptoms.
Methods and materials
Participants
The Western Australian Pregnancy Cohort (Raine) Study methodology has been described previously (Newnham et al., 1993). In brief, a total of 2900 pregnant women attending the public antenatal clinic at King Edward Memorial Hospital, or nearby private practices, were recruited into the Western Australian Pregnancy Cohort (Raine) Study between May 1989 and November 1991. The criteria for enrolment were gestational age between 16 and 20 weeks, sufficient proficiency in English to understand the implications of participation, an expectation to deliver at the King Edward Memorial Hospital and an intention to remain in Western Australia in the coming years. Although 114 women delivered in hospitals other than the King Edward Memorial Hospital, their outcomes were still assessed. The vast majority (96%) gave birth at the King Edward Memorial Hospital. A total of 2868 children have undergone serial assessment at birth and at ages 1, 2, 3, 5, 8, 10, 14, 17 and 20 years. Recruitment was approved by the ethics committees of King Edward Memorial Hospital for Women and the Princess Margaret Hospital for Children, Perth, Western Australia, and ethics approval at the 20-year follow-up was obtained from the University of Western Australia Human Research Ethics Committee. Informed and written consent was obtained from the participant and/or their primary caregiver for all follow-ups.
Data collection for the 20-year follow-up occurred between March 2010 and April 2012. A total of 2125 young adults were eligible (not withdrawn or deferred) for follow-up at 20 years. Of the 1565 who participated, 75% (n=1172) provided a blood sample for measurement of serum 25(OH)D concentrations and 78% (n=1220) completed the DASS-21. Data for serum 25(OH)D concentrations and DASS-21 at 20 years were available for 945 participants.
Assessment of depression, anxiety and stress
Mental health was assessed using the 21-item self-reported Depression Anxiety Stress Scales (DASS-21), which consists of three 7-item self-report scales that assess symptoms of depression, anxiety and stress (Lovibond et al., 1996). The longer DASS-42 and short-form DASS-21 were developed using Australian data and have been validated in both clinical and non-clinical samples (Antony et al., 1998; Henry and Crawford, 2005; Ng et al., 2007). The depression scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia, and inertia; the anxiety scale assesses autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experience of anxious affect; and the stress scale assesses difficulty relaxing, nervous arousal, being easily upset/agitated, irritable/over-reactive and impatient. Participants were asked to rate the extent to which they had experienced each state over the past week on a four-point severity/frequency scale. Each item uses a four-point response scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). The DASS-21 yields separate depression, anxiety and stress subscale scores, and a total score that is the sum of the three subscales and represents a composite measure of negative emotional symptoms. Scores for each subscale can range from 0 to 21, with higher scores indicating greater depression, anxiety or stress. The total score can range from 0 to 63. Cut-off scores defining mild/moderate/severe/extremely severe scores are designed for clinical practice and are not validated for research purposes; therefore, we used DASS-21 scores as a continuous measure.
Assessment of serum 25(OH)D concentrations
Participants provided a blood sample for measurement of serum 25(OH)D concentrations within two weeks of completing the DASS-21. Venous blood samples were taken from an antecubital vein after an overnight fast and samples were stored at −80°C until analysed using isotope-dilution liquid chromatography-tandem mass spectrometry (RDDT, Victoria, Australia), according to published methodology (Maunsell et al., 2005). Of the 945 participants who provided a blood sample and completed the DASS, only 10 participants had detectable serum 25(OH)D2 concentrations, ranging from 5.24 to 7.07 nmol/L. Given that blood samples were collected year-round between March 2010 and April 2012, and that an association between vitamin D levels and mental health symptoms would take time to develop, a sinusoidal model incorporating month of blood collection was used to calculate deseasonalised serum 25(OH)D3 concentrations (van der Mei et al., 2007). Since 25(OH)D2 is obtained from food and supplements, rather than sunlight exposure, serum 25(OH)D2 concentrations were added to the deseasonalised serum 25(OH)D3 concentrations to obtain total concentrations of serum 25(OH)D. We defined vitamin D levels as being sufficient when concentrations of serum 25(OH)D were ≥75 nmol/L, insufficient when they were 50-74.9 nmol/L and deficient when they were <50 nmol/L (Holick et al., 2011). Duration of sun exposure, and vitamin D intakes from food and supplements were not available at the 20-year follow-up. However, since serum 25(OH)D concentrations are a product of sun exposure and dietary vitamin D intakes, these factors were accounted for by the measurement of serum 25(OH)D concentrations.
Potential confounding variables
Analyses were adjusted for variables that may confound the relationship between serum 25(OH)D concentrations and symptoms of depression, anxiety and stress. Participants were classified as Caucasian if both parents were Caucasian, or as non-Caucasian if one or both parents were of an alternate ethnicity. Since the age of participants at the 20-year follow-up ranged from 19 to 22 years, we included age at date of blood sample as a potential confounder. Weight was measured to the nearest 100g using Personal Precision scales UC-321 (A and D Company) and height was measured to the nearest 0.1 cm with a wall mounted Seca 202. We calculated body mass index (BMI) as weight in kilograms divided by height in metres squared. Physical activity was assessed by asking participants how many days they engaged in moderate or vigorous physical activities of at least 10 minute duration during the last seven days. Responses were collapsed into three categories: exercises less than once per week, exercises 1-3 times per week, exercises four or more times per week.
Statistical analysis
Characteristics of participants who provided a blood sample for analysis of serum 25(OH)D concentrations and completed the DASS-21 at the 20-year follow-up were compared with non-participants from the original cohort. Sex, race, family income during pregnancy, maternal age at birth, maternal education and maternal pre-pregnancy BMI were compared using Chi-square tests.
Baseline characteristics, including age, race, deseasonalised serum 25(OH)D concentrations, vitamin D status, total DASS-21 scores and subscale scores, BMI and physical activity were described for participants in the current study and stratified by sex. Chi-square tests were used to determine differences between males and females for categorical variables (race, deseasonalised serum 25(OH)D categories and physical activity). For continuous variables, skewness >1 indicated that non-parametric analysis was appropriate. We used independent-samples t-tests to determine differences between males and females in parametric data (deseasonalised serum 25(OH)D concentrations) and Mann-Whitney U tests for non-parametric data (age, total DASS-21 scores, DASS-21 subscale scores and BMI).
We performed univariate general linear models investigating the impact of potential confounding variables (age, race, BMI and physical activity) on serum 25(OH)D concentrations. Due to the highly skewed total DASS-21 scores and subscale scores, negative binomial regression with a log link was applied to investigate associations between serum 25(OH)D concentrations and DASS-21 scores (total score and depression, anxiety and stress subscale scores). Negative binomial regression reports a rate ratio (RR), which is interpreted, in this case, as the predicted proportional increase in DASS scores per 10 nmol/L change in 25(OH)D concentrations. Models were performed unadjusted and then adjusted for sex, race, age, BMI and physical activity. Models examining subscale scores were also adjusted for the other subscale scores. An interaction term between sex and serum 25(OH)D concentrations was included to determine whether effects of serum 25(OH)D concentrations were different in males and females. Analyses were performed using IBM SPSS Statistics Release Version 19.9.9.1 (IBM SPSS Inc., 2010, Chicago, IL). Statistical significance was defined as p< 0.05.
Results
Compared with those from the original cohort who did not participate in the current study (n=1923), participants in the current study (n=945) were more likely to come from families with a higher income during pregnancy and to have mothers with a higher age, higher education and healthier BMI (Table 1). There were no significant differences in sex and race between participants in the current study and non-participants from the original cohort.
Characteristics of participants (n=945) v non-participants from the original cohort (n=1923).
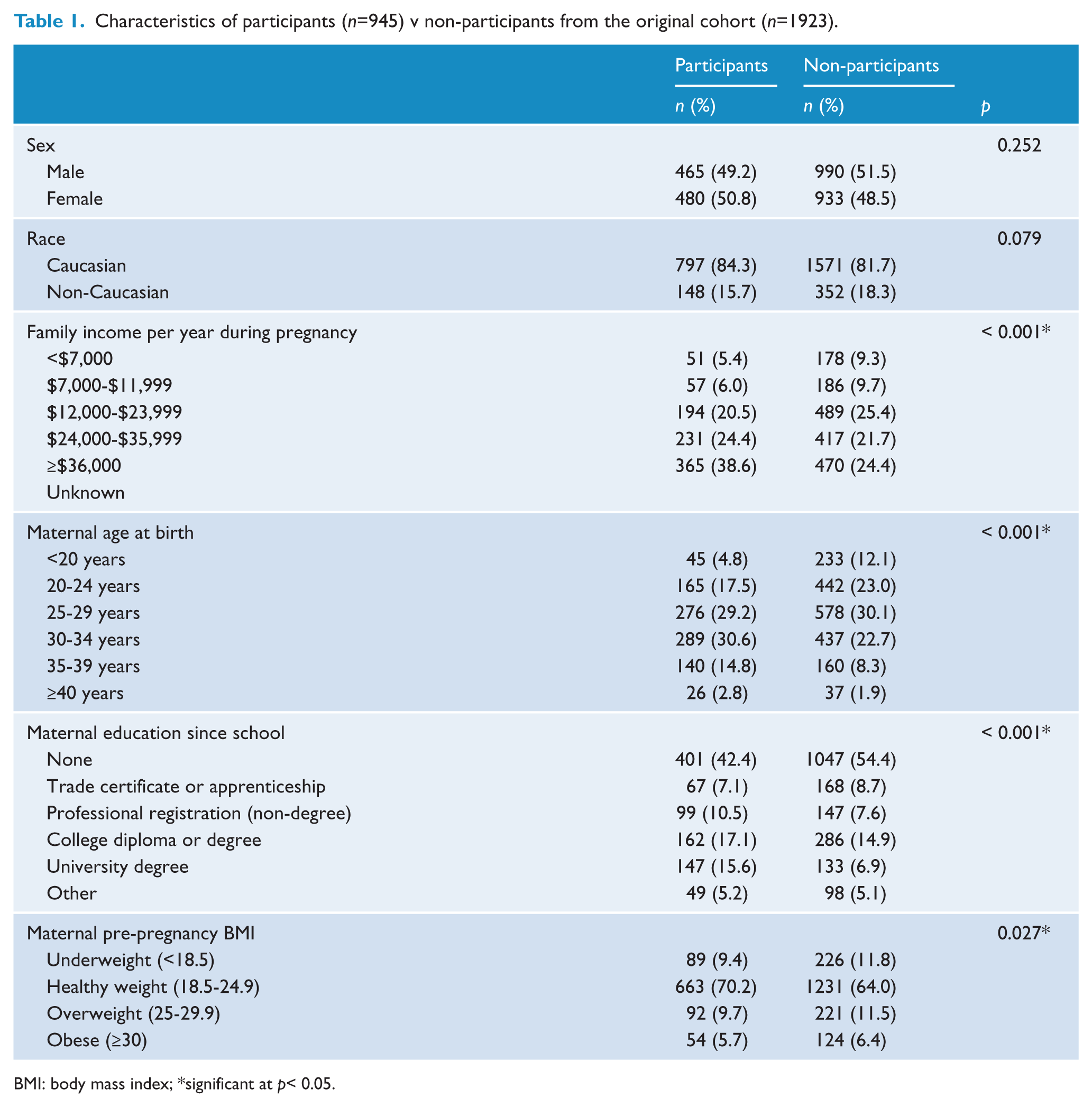
BMI: body mass index; *significant at p< 0.05.
In participants of the 20-year follow-up, the median (interquartile range (IQR)) total DASS-21 score was 12 (20) for males and 18 (24) for females (Table 2) (p <0.001). The median (IQR) scores for the depression subscale were 4 (8) for males and 4 (8) for females. For the anxiety subscale, the median (IQR) scores were 2 (6) for males and 4 (8) for females. The median (IQR) scores for the stress subscale were 6 (10) for males and 8 (10) for females. The mean (standard deviation) serum 25(OH)D concentration was 70.7 (23.0) nmol/L for males and 74.8 (24.2) for females (p=0.008). There was a significant difference in vitamin D status between males and females (p=0.039). The prevalence of vitamin D deficiency (25(OH)D <50 nmol/L) was 18% for males and 12% for females.
Characteristics of the Raine Study participants for whom serum 25(OH)D concentrations and DASS-21 scores were available (n=945).
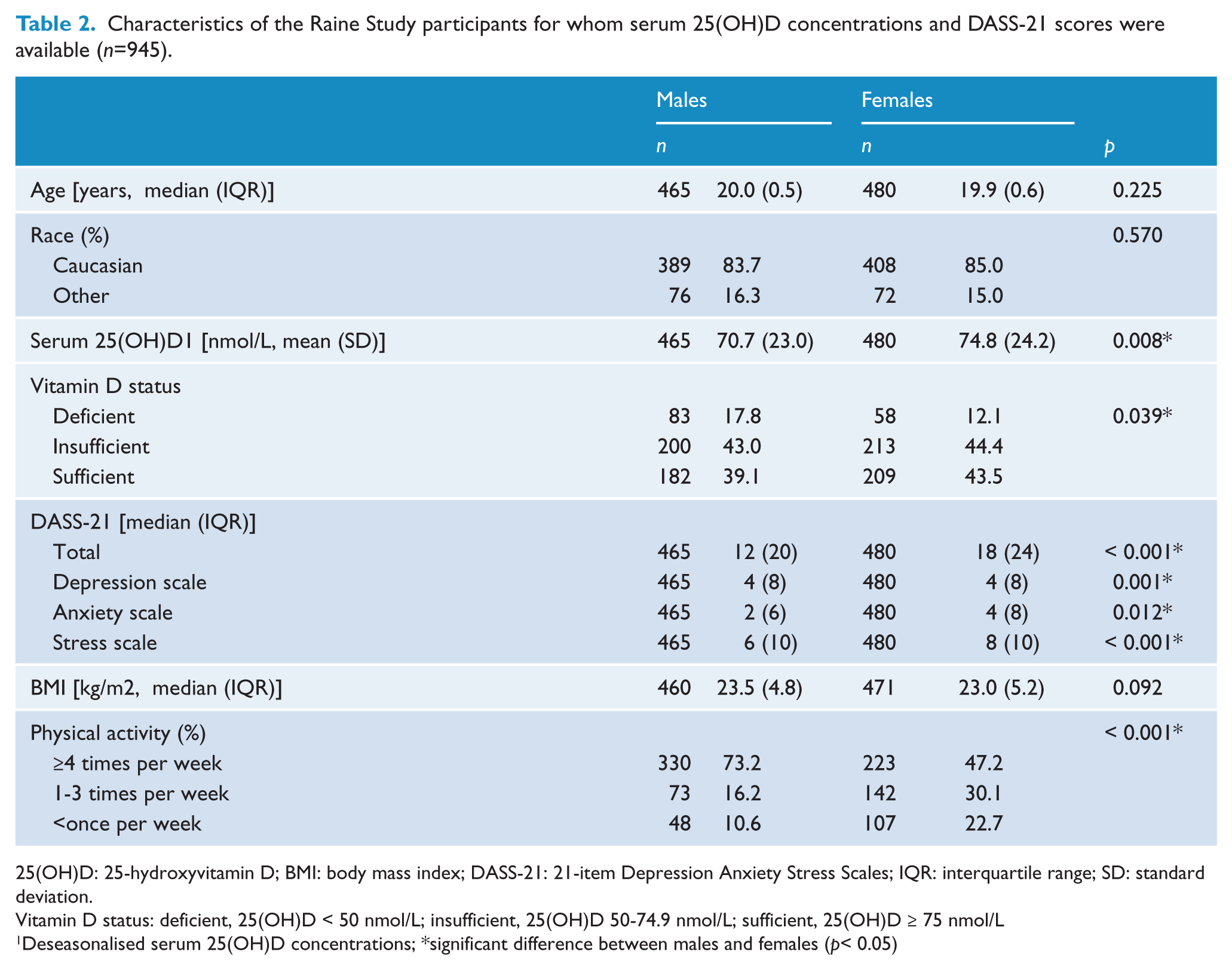
25(OH)D: 25-hydroxyvitamin D; BMI: body mass index; DASS-21: 21-item Depression Anxiety Stress Scales; IQR: interquartile range; SD: standard deviation.
Vitamin D status: deficient, 25(OH)D < 50 nmol/L; insufficient, 25(OH)D 50-74.9 nmol/L; sufficient, 25(OH)D ≥ 75 nmol/L
Deseasonalised serum 25(OH)D concentrations; *significant difference between males and females (p< 0.05)
Complete data, including all potential confounding variables, were available for 735 participants. In univariate models, age, race, BMI and physical activity were all significantly associated with serum 25(OH)D concentrations (Table 3). When investigating the effect of serum 25(OH)D concentrations on total DASS-21 scores, there was a significant interaction between sex and serum 25(OH)D concentrations (p=0.005); therefore, models were stratified by sex. In unadjusted models, higher serum 25(OH)D concentrations were significantly associated with decreased total DASS-21 scores and all three subscale scores in males (Table 4). An increase of 10 nmol/L of serum 25(OH)D in males decreased total DASS-21 scores by 9% (RR 0.91; 95% CI 0.88, 0.96; p<0.001), depression subscale scores by 12% (RR 0.88; 95% CI 0.83, 0.93; p<0.001), anxiety subscale scores by 6% (RR 0.94; 95% CI 0.90, 0.99; p=0.016) and stress subscale scores by 7% (RR 0.93; 95% CI 0.88, 0.97; p=0.003).
Unadjusted general linear models showing the effect of potential confounding factors on deseasonalised serum 25(OH)D concentrations (n=735).
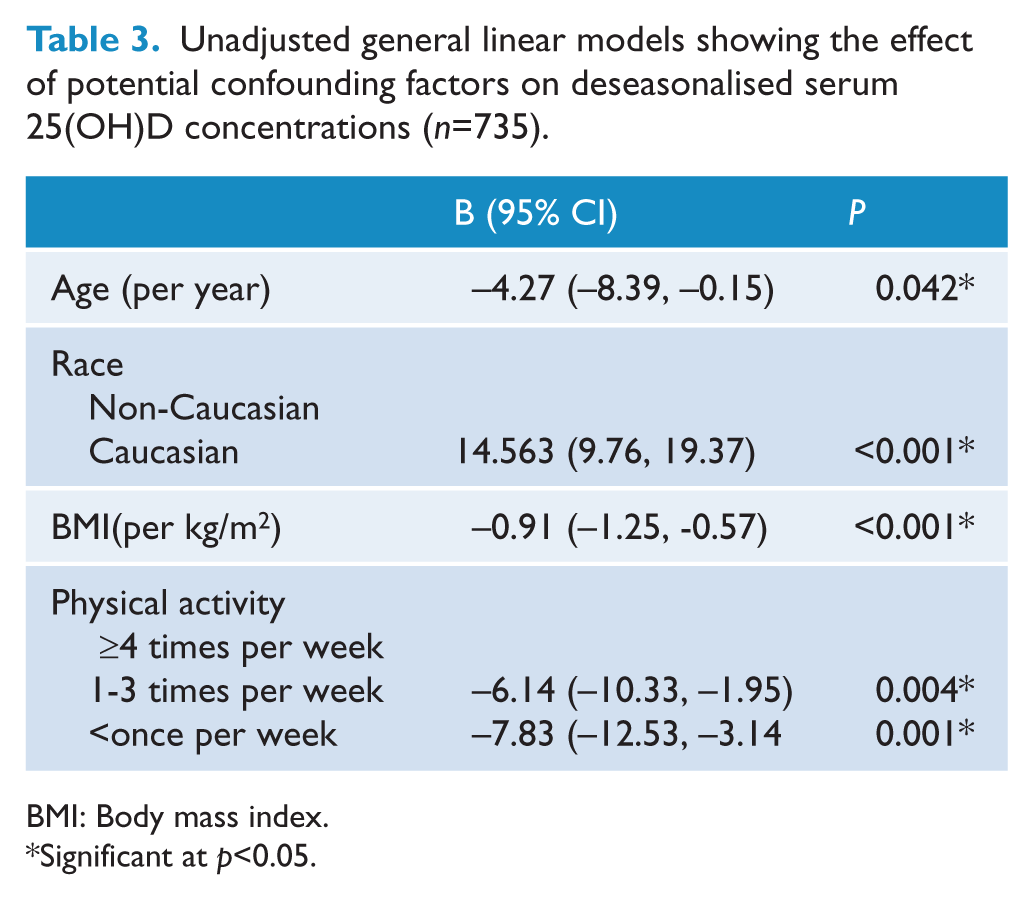
BMI: Body mass index.
Significant at p<0.05.
Unadjusted and adjusted negative binomial model coefficients for the effect of deseasonalised serum 25(OH)D concentrations (per increase of 10 nmol/L) on DASS-21 scores and subscale scores in males and females.
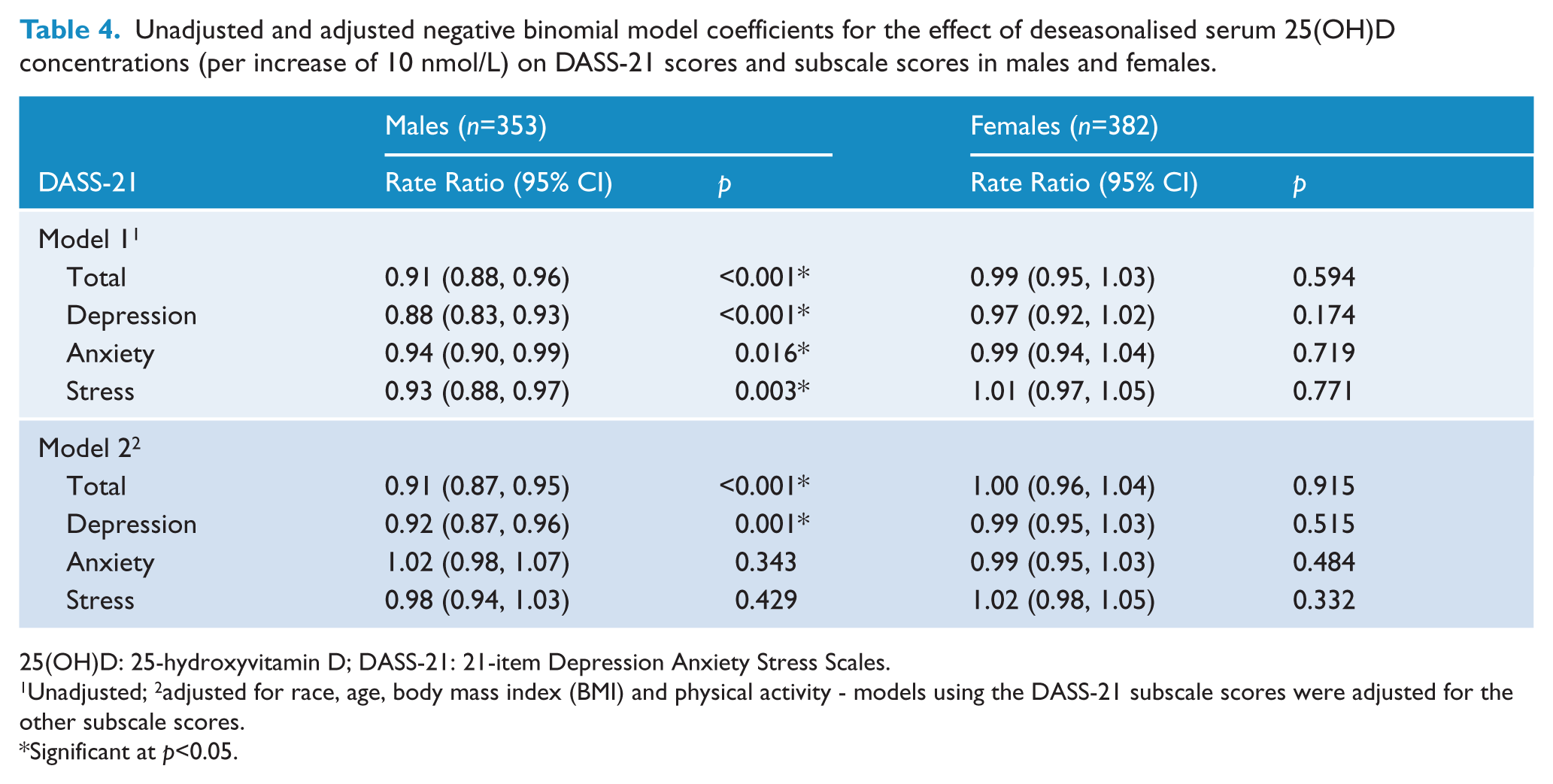
25(OH)D: 25-hydroxyvitamin D; DASS-21: 21-item Depression Anxiety Stress Scales.
Unadjusted; 2adjusted for race, age, body mass index (BMI) and physical activity - models using the DASS-21 subscale scores were adjusted for the other subscale scores.
Significant at p<0.05.
When adjusted for race, age, BMI and physical activity, the association between serum 25(OH)D concentrations and total DASS-21 scores remained significant (RR 0.91; 95% CI 0.87, 0.95; p<0.001). Similarly, when adjusted for race, age, BMI, physical activity, anxiety subscale score and stress subscale score, the association between serum 25(OH)D concentrations and the depression subscale score remained significant (RR 0.92; 95% CI 0.87, 0.96; p=0.001). After adjusting for confounders, including the depression subscale scores, there were no significant associations between serum 25(OH)D concentrations and symptoms of anxiety and stress in young adult males. In females, there were no significant associations between serum 25(OH)D concentrations and total DASS-21 scores or subscale scores in unadjusted or adjusted models.
Discussion
Higher serum 25(OH)D concentrations were significantly associated with lower total DASS-21 scores and reduced symptoms of depression in males, after adjusting for age, race, BMI, physical activity, anxiety subscale scores and stress subscale scores. An advantage of using the DASS-21 is that it distinguishes between the related symptoms of depression, anxiety and stress. Our results suggest that vitamin D is related specifically to depressive symptoms, since we found no significant association between serum 25(OH)D concentrations and symptoms of anxiety and stress in males, after adjusting for confounders. Significant associations between serum 25(OH)D concentrations and symptoms of depression, anxiety and stress were not seen in females, either in unadjusted or adjusted models. These findings are important as relatively few studies have considered associations between vitamin D levels and symptoms of depression, anxiety and stress in young adults.
Several previous population-based studies in different age groups have examined the relationship between vitamin D levels and the presence of depressive symptoms (Ganji et al., 2010; Hoang et al., 2011; Jamilian et al., 2013; Kjaergaard et al., 2011; Lee et al., 2011; Milaneschi et al., 2010; Nanri et al., 2009; Pan et al., 2009; Tolppanen et al., 2012; Zhao et al., 2010). Kjaergaard et al. (2011) showed that low serum 25(OH)D concentrations predicted depressive symptoms in a cross-sectional study of adults aged 30-87 years (n=10,086) after adjusting for multiple confounders, including chronic disease. In concordance with our findings, there were no significant associations between low 25(OH)D concentrations and anxiety. Prospective analysis using data from the Avon Longitudinal Study of Parents and Children (ALSPAC) showed that higher concentrations of 25(OH)D3 were associated with lower levels of depressive symptoms in children (Tolppanen et al., 2012).
Our findings differ from results of a large, cross-sectional, population-based study of adults aged ≥20 years in the United States (n=3916) (Zhao et al., 2010). That study found inverse associations between vitamin D levels and moderate-to-severe depression after adjusting for age and sex, but the associations were not significant after adjusting for other potential confounders. A major confounder was the presence of chronic disease. Pan et al. (2009) also found no significant associations between vitamin D levels and depressive symptoms in 3262 Chinese adults aged 50-70 years after adjusting for potential confounders.
Sex differences in the relationship between vitamin D levels and depression have been reported by Milaneschi et al. (2010) and Kjaergaard et al. (2011). In contrast to our findings, these studies reported stronger associations between serum 25(OH)D concentrations and depressive symptoms in females than males. A functional relationship between the active 1,25-dihydroxyvitamin D (1,25(OH)2D) and oestradiol has been suggested (Correale et al., 2010; Nashold et al., 2009), which may contribute to sex differences in response to low vitamin D levels. However, it is not clear why associations were evident in males and not females in the current study. The differences between males and females in response to serum 25(OH)D concentrations warrants further investigation in future studies.
It is problematic to make comparisons between studies examining vitamin D levels and mental health due to the use of different tools to measure mental health symptoms and the use of different assays to determine circulating 25(OH)D concentrations. Circulating 25(OH)D concentrations are measurable using several techniques, including competitive protein binding assay (CPBA), high performance liquid chromatography (HPLC), liquid chromatography-tandem mass spectrometry (LC-MS/MS), radioimmunoassay (RIA) and enzyme immunoassay. However, there is significant variation in 25(OH)D measurement depending on the laboratory and assay used, confounding the diagnosis of vitamin D deficiency. Furthermore, baseline serum 25(OH)D concentrations and season of blood collection differ between studies, and different confounders are used in statistical models.
Results from clinical trials investigating vitamin D supplementation and depressive symptoms are varied (Bertone-Johnson et al., 2012; Dean et al., 2011; Dumville et al., 2006; Hogberg et al., 2012; Jorde et al., 2008; Kjaergaard et al., 2012; Lansdowne et al., 1998; Sanders et al., 2011). Recently, a large, randomised, double-blinded trial in the United States, comprising 36,282 postmenopausal women, showed no relation between 400 IU/day vitamin D supplementation and depressive symptoms over a two-year period (Bertone-Johnson et al., 2012). However, serum 25(OH)D concentrations were not available so it is not known whether the dose was sufficient to improve vitamin D status. Similarly, Kjaergaard et al. (2012) showed that although low levels of serum 25(OH)D were associated with depressive symptoms in adults, a high vitamin D dose of 40 000 IU/week for six months did not improve symptoms. In contrast, a cross-sectional study of 441 adults in Norway found that a weekly vitamin D dose of 20 000 IU significantly improved Beck Depression Inventory scores after one year (Jorde et al., 2008). The equivocal results from vitamin D supplementation trials may be a reflection of differences in dose, baseline 25(OH)D concentrations, latitude, race and the outcome measure of depressive symptoms.
A strength of our study was the deseasonalisation of serum 25(OH)D concentrations, which is important since blood samples were collected year-round and vitamin D levels vary with respect to season of blood collection. A further strength was access to data that may influence both serum 25(OH)D concentrations and symptoms of depression, anxiety and stress, allowing us to adjust for potential confounders, including BMI and physical activity. This allowed us to examine the independent associations between serum 25(OH)D concentrations and the total DASS-21 scores and subscale scores. However, although we adjusted for physical activity, the measure of assessment was not based on a validated questionnaire and did not differentiate between indoor and outdoor activity.
A limitation of our study was the use of self-reported questionnaire rather than clinical diagnosis to assess symptoms of depression, anxiety and stress. While self-report assessment has been established as a valid means for assessing mental health difficulties such as depression, anxiety and stress (Antony et al., 1998; Henry and Crawford, 2005) and may lead to more truthful reporting than face-to-face assessment, we cannot rule out the possibility of under- or over-reporting. Our results suggest an association between serum 25(OH)D concentrations and self-reported depressive symptoms, rather than an association with a clinical diagnosis of depression.
A further limitation of our study was the loss to follow-up. Participants included in the current study were more likely to be from families with higher socioeconomic status relative to participants from the original cohort and care should be taken when generalising results to the wider community. Furthermore, attrition may have been higher for those participants suffering from mental health symptoms, such as depression or anxiety. However, it should be possible to observe an association between vitamin D and mental health symptoms in the remaining participants, although the power to detect this association at a significant level may be weaker.
Since the DASS-21 scores were only available at the 20-year follow-up, we conducted a cross-sectional analysis and do not infer a causative relationship between vitamin D levels and depressive symptoms in males. It is possible that males with depressive symptoms were less likely to engage in outdoor activities, leading to lower serum 25(OH)D concentrations. Future follow-ups of the Raine cohort will likely provide mental health data based on the DASS-21, providing an opportunity for investigating the longitudinal association between serum 25(OH)D concentrations and the development of depressive symptoms. Furthermore, as the cumulative incidence of depression increases in future follow-ups of the Raine cohort, it may be possible to investigate whether low vitamin D status impairs recovery from mental health disorders, including depression. This would be consistent with recent findings that daily vitamin D supplementation may prevent the deterioration of Parkinson disease (Suzuki et al., 2013).
Conclusion
We found a cross-sectional association between serum 25(OH)D concentrations and symptoms of depression, but not anxiety and stress, in young adult males. In order to investigate a potential causative relationship between vitamin D levels and depressive symptoms, longitudinal investigations are warranted. Randomised controlled trials using effective doses of vitamin D, and monitoring serum 25(OH)D concentrations, are necessary to determine any benefit of vitamin D supplementation in the prevention and treatment of depression.
Footnotes
Acknowledgements
We gratefully acknowledge the Raine Study participants and their families, and the Raine Study Team for cohort co-ordination and data collection.
Funding
Core funding for the Western Australian Pregnancy Cohort (Raine) Study is provided by the University of Western Australia; the Faculty of Medicine, Dentistry and Health Sciences at the University of Western Australia; the Telethon Institute for Child Health Research; the Women and Infants Research Foundation; Curtin University; and the Raine Medical Research Foundation. Specific data collection for the 20-year follow-up was funded by the National Health and Medical Research Council Project #1022134 (2012-2014).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.