
Abstract
Objectives:
To assess differences in costs of psychosis between the first and second Australian national surveys of psychosis and examine them in light of policy developments.
Method:
Cost differences due to changes in resource use and/or real price rises were assessed by minimizing differences in recruitment and costing methodologies between the two surveys. For each survey, average annual societal costs of persons recruited through public specialized mental health services in the census month were assessed through prevalence-based, bottom-up cost-of-illness analyses. The first survey costing methodology was employed as the reference approach. Unit costs were specific to each time period (2000, 2010) and expressed in 2010 Australian dollars.
Results:
There was minimal change in the average annual costs of psychosis between the surveys, although newly included resources in the second survey’s analysis cost AUD$3183 per person. Among resources common to each analysis were significant increases in the average annual cost per person for ambulatory care of AUD$7380, non-government services AUD$2488 and pharmaceuticals AUD$1892, and an upward trend in supported accommodation costs. These increases were offset by over a halving of mental health inpatient costs of AUD$11,790 per person and a 84.6% (AUD$604) decrease in crisis accommodation costs. Productivity losses, the greatest component cost, changed minimally, reflecting the magnitude and constancy of reduced employment levels of individuals with psychosis across the surveys.
Conclusions:
Between 2000 and 2010 there was little change in total average annual costs of psychosis for individuals receiving treatment at public specialized mental health services. However, there was a significant redistribution of costs within and away from the health sector in line with government initiatives arising from the Second and Third National Mental Health Plans. Non-health sector costs are now a critical component of cost-of-illness analyses of mental illnesses reflecting, at least in part, a whole-of-government approach to care.
Introduction
Costs of illness (COI) can be assessed using a number of approaches, and different analyses can incorporate quite disparate arrays of data and resource usage. Methodological inconsistencies are considered the major impediment to the usefulness of COI analyses for decision-makers (Bloom et al., 2001). Such differences are common in the COI literature for schizophrenia and psychosis. McEvoy (2007) has called for new COI studies of schizophrenia employing comparable methodologies so that changing patterns of costs can be reliably determined. The importance of this information stems from the significant and ongoing change in the treatment and care of individuals with psychosis since the mid to late 20th century, including deinstitutionalization, development of community mental health services and the introduction of drug therapies, most recently the atypical antipsychotics (Thara et al., 2010: 350).
In Australia, policy developments and restructuring of mental health service provision has occurred under the auspices of the National Mental Health Strategy (Australian Health Ministers’ Advisory Council, 1992; Australian Health Ministers, 2009). The Strategy, endorsed in April 1992, initially focused on the ‘mainstreaming’ of acute care and expansion of community-based non-acute care for the severely mentally ill. It has since evolved to encompass a whole-of-government approach to care, within a paradigm of ‘wrap around care’ (Lee et al., 2010), including provision of support and care by non-government organizations (NGOs) for all persons with mental illness.
Over the course of the Strategy, two surveys have examined the prevalence, demographic and clinical characteristics of Australians living with psychotic illness. The first Australian national survey of psychosis – the Low Prevalence (Psychotic) Disorders Study (LPDS) – was undertaken in 1997/1998 (Jablensky et al., 1999, 2000). In the LPDS, 980 screen-positive participants were interviewed: 687 (70.1%) were identified through public specialized mental health services (PSMHS), 173 (17.7%) through private medical services and 120 (12.2%) through marginal accommodation, all in the census month. Data from the first survey were employed in a bottom-up assessment of the disorder-specific costs of psychosis in 2000 (Carr et al., 2002, 2003).
In 2010, the second Australian national survey of psychosis, the Study of High Impact Psychosis (SHIP) took place (Morgan et al., 2011, 2012). In this study, 1825 of 7955 screen-positive people were interviewed: 1211 were identified through contact with PSMHS within the census month, 409 through contact with PSMHS in the previous 11 months and 205 through contact with NGOs funded to support people with mental illness during the census month. Data from the second survey were similarly used in a bottom-up assessment of the disorder-specific costs of psychosis (Neil et al., 2014), in which costs were found to be dependent upon primary service provider and recency of contact.
SHIP was a legatee of the LPDS and this relationship resulted in a high level of commonality between the surveys including study design, diagnostic assessment and classification, and survey instrumentation. Further, the costing methodology employed in the COI analysis of the second survey was based on that of the first survey. The commonality of the surveys and their respective COI analyses provides a unique opportunity to undertake a robust comparison of the costs of psychosis over a 10-year interval, a comparison that has the capacity to inform policy-makers and health care providers alike.
In this paper, the differences in the costs of psychosis between 2000 and 2010 are assessed by minimizing known differences in recruitment and costing methodologies between the first and second surveys of psychosis. Comparison of the costs obtained provides direct insight into changes in cost profiles over time (i.e. the distribution of costs between and within sectors) and further investigation enables change due to variation in average resource use and/or real prices to be ascertained. Finally, the comparative results are considered in light of policy developments.
Methods
Costs of psychosis encompassing health sector and other sector costs, and productivity losses/time-loss costs were assessed for 2000 and 2010. Costs were assessed from a societal perspective using prevalence-based, bottom-up approaches based on the data collected in the first and second national surveys of psychosis, respectively (Jablensky et al., 1999, 2000; Morgan et al., 2011, 2012). For each survey, the comparative analysis was limited to persons identified through PSMHS in the census month.
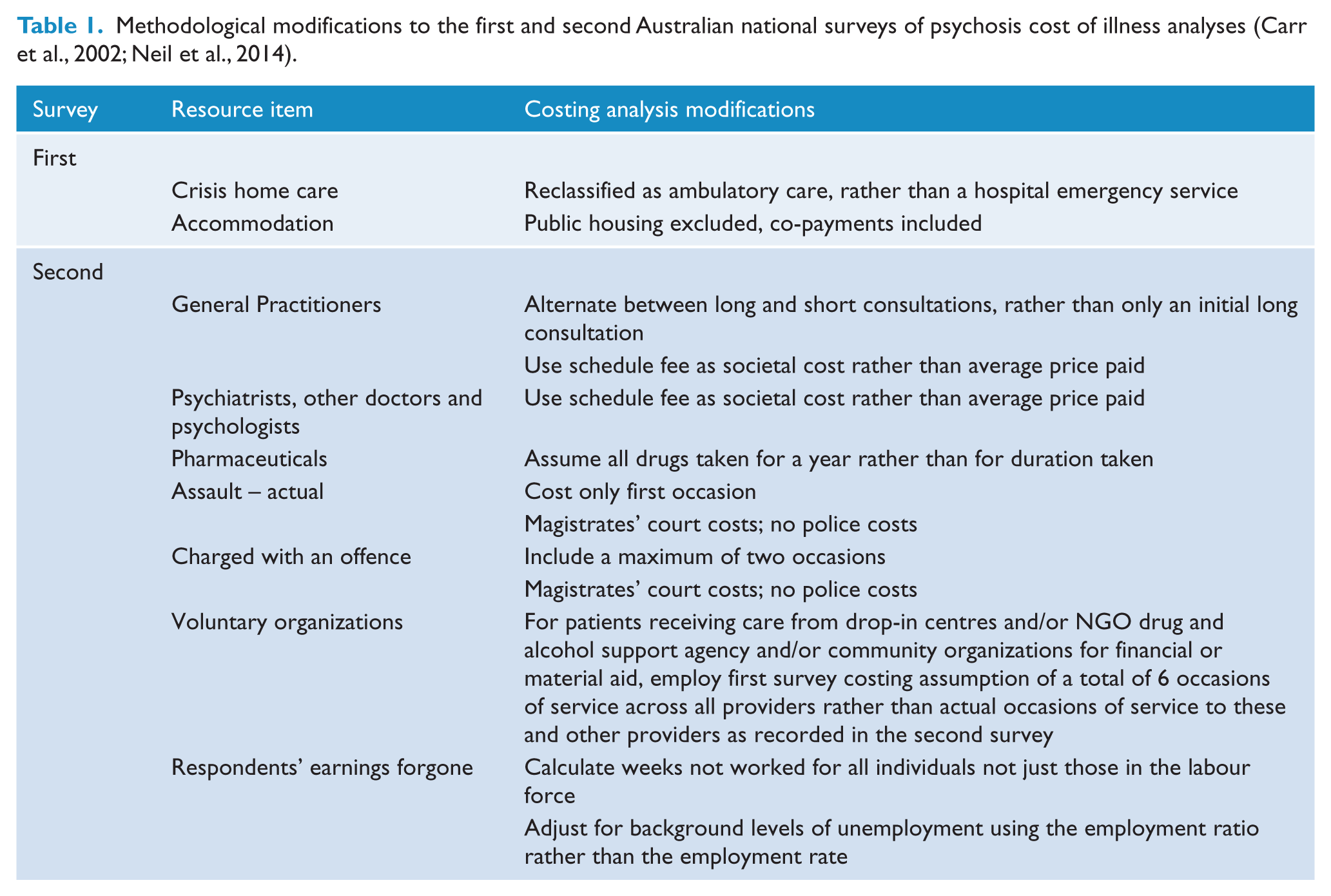
The methodology employed for the first survey’s COI analysis (Carr et al., 2002) was used as the reference approach, subject to a small number of refinements (Table 1). Given changes to the structured interview between the first and second surveys and policy developments over the intervening decade, several modifications were required to the costing methodology of the second survey’s COI analysis (Neil et al., 2014), as outlined in Table 1. All resource items newly captured and/or costed in the second survey analysis were retained in the current analysis, but separately identified to ensure exact comparability between individual line items across the two time periods. A complete listing of line items and whether they were newly included in the 2010 analysis is provided in Table 2.
Methodological modifications to the first and second Australian national surveys of psychosis cost of illness analyses (Carr et al., 2002; Neil et al., 2014).
Line items by commonality across first and second survey cost analyses, by cost category.
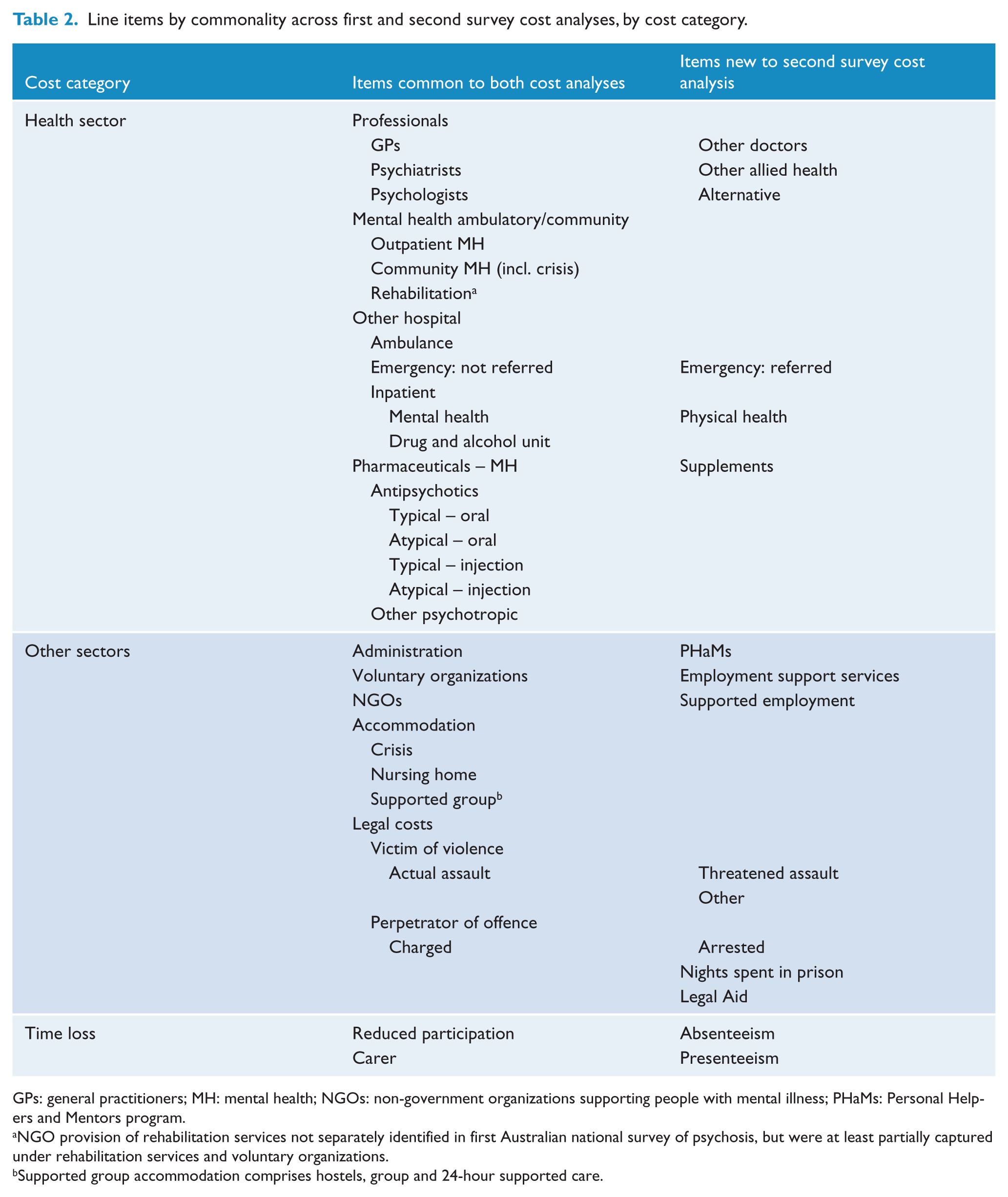
GPs: general practitioners; MH: mental health; NGOs: non-government organizations supporting people with mental illness; PHaMs: Personal Helpers and Mentors program.
NGO provision of rehabilitation services not separately identified in first Australian national survey of psychosis, but were at least partially captured under rehabilitation services and voluntary organizations.
Supported group accommodation comprises hostels, group and 24-hour supported care.
For each survey, psychosis-related data on resources used and morbidity-related impairments in productivity over the preceding 12 months were extracted from the respective survey database (see Appendix 1). When the assessment period was less than 12 months, extrapolation was employed. Where information was missing, resource usage was conservatively assumed to be nil.
Costs per respondent were calculated by multiplying the specified or estimated resource usage or losses over the preceding 12-month period by a set of standard unit costs specific to each analysis, as detailed in the original studies (Carr et al., 2002; Neil et al., 2014), and expressed in constant 2010 Australian dollars. The assessment of productivity losses employed a modified human capital approach in which lost production was valued as expected earnings forgone, calculated as the product of the number of weeks not worked by average weekly earnings by age and sex, adjusted for the prevailing employment ratio.
Within the health sector, costs of ambulatory and hospital-related care were inflated using data from the government final consumption expenditure (GFCE) for hospitals and nursing homes; for pharmaceuticals the Pharmaceutical Benefits Scheme (PBS) implicit price deflator; and for professional services the Medicare medical service fees charged deflator (Australian Institute of Health and Welfare, 2011b) were employed. For other sectors, costs were inflated using the non-farm sector gross domestic product (GDP) implicit price deflator (Australian Bureau of Statistics, 2011).
From the individual costs, the average cost per person with treated psychosis was calculated. Data from both samples were weighted to accurately reflect the structure of each study’s first-phase census. Weighting in both surveys was undertaken according to the service from which the participant was recruited. Weighting in the second survey also encompassed two age strata (18–34, 35–64).
Statistical analysis
The analysis was undertaken using the Statistical Package for Social Sciences (SPSS) (version 20; SPSS Inc., Chicago, USA), Complex Samples and Excel 2008 for Mac.
In the absence of accepted methods to bootstrap weighted data, preference was given to weighting the interviewed sample data to produce accurate cost estimates across the screen-positive sample of persons identified through PSMHS in the census month. The normal theory confidence intervals reported (±1.96*SEM) are likely to be conservative. Comparisons are considered statistically significant where 95% confidence intervals do not overlap. This is a conservative approach as some overlapping confidence intervals may be significant also (Julious, 2004).
Results
The average annual costs per person with psychosis receiving care through PSMHS during the census month in the first and second surveys are given in Tables 3 and 4, with 95% confidence intervals provided in Appendix 2. From the first to the second surveys, total costs are estimated to have risen from $75,193 to $79,537, an average of $4344 per person (5.8%) in real terms.
Average annual costs of persons with psychosis treated in public specialized mental health services, Australia, 2000 and 2010; constant 2010 prices (AUD$/person). a
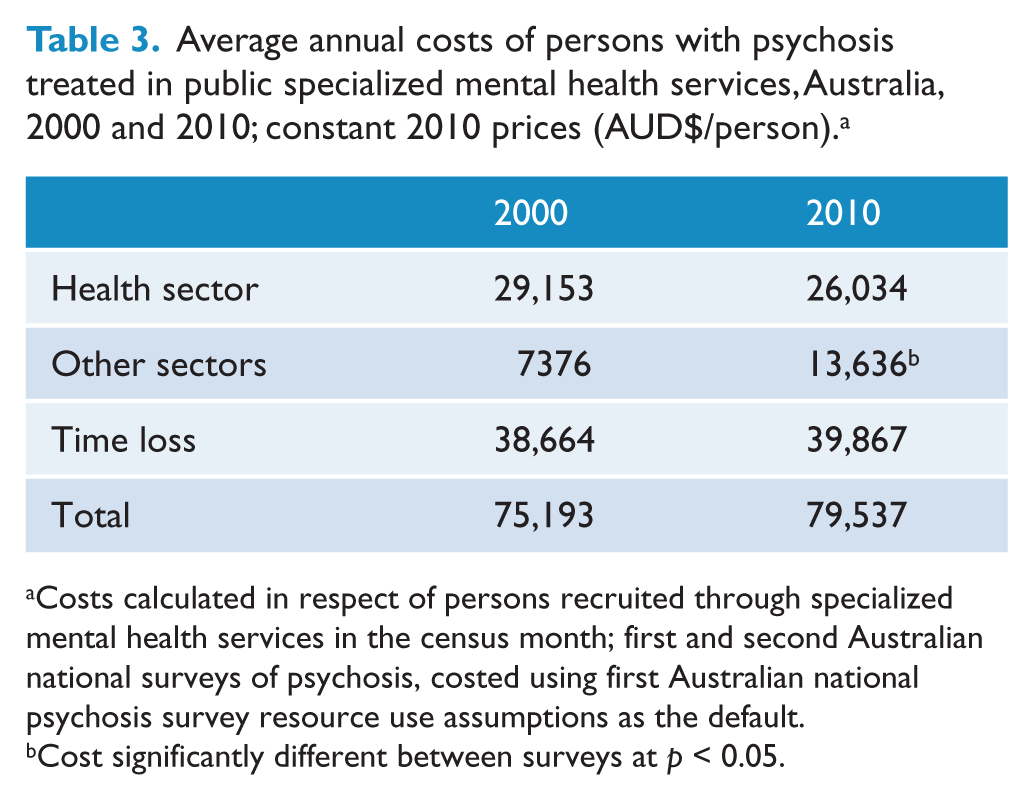
Costs calculated in respect of persons recruited through specialized mental health services in the census month; first and second Australian national surveys of psychosis, costed using first Australian national psychosis survey resource use assumptions as the default.
Cost significantly different between surveys at p < 0.05.
Average annual line-item costs of persons with psychosis treated in public specialized mental health services, Australia, 2000 and 2010; constant 2010 prices (AUD$/person). a
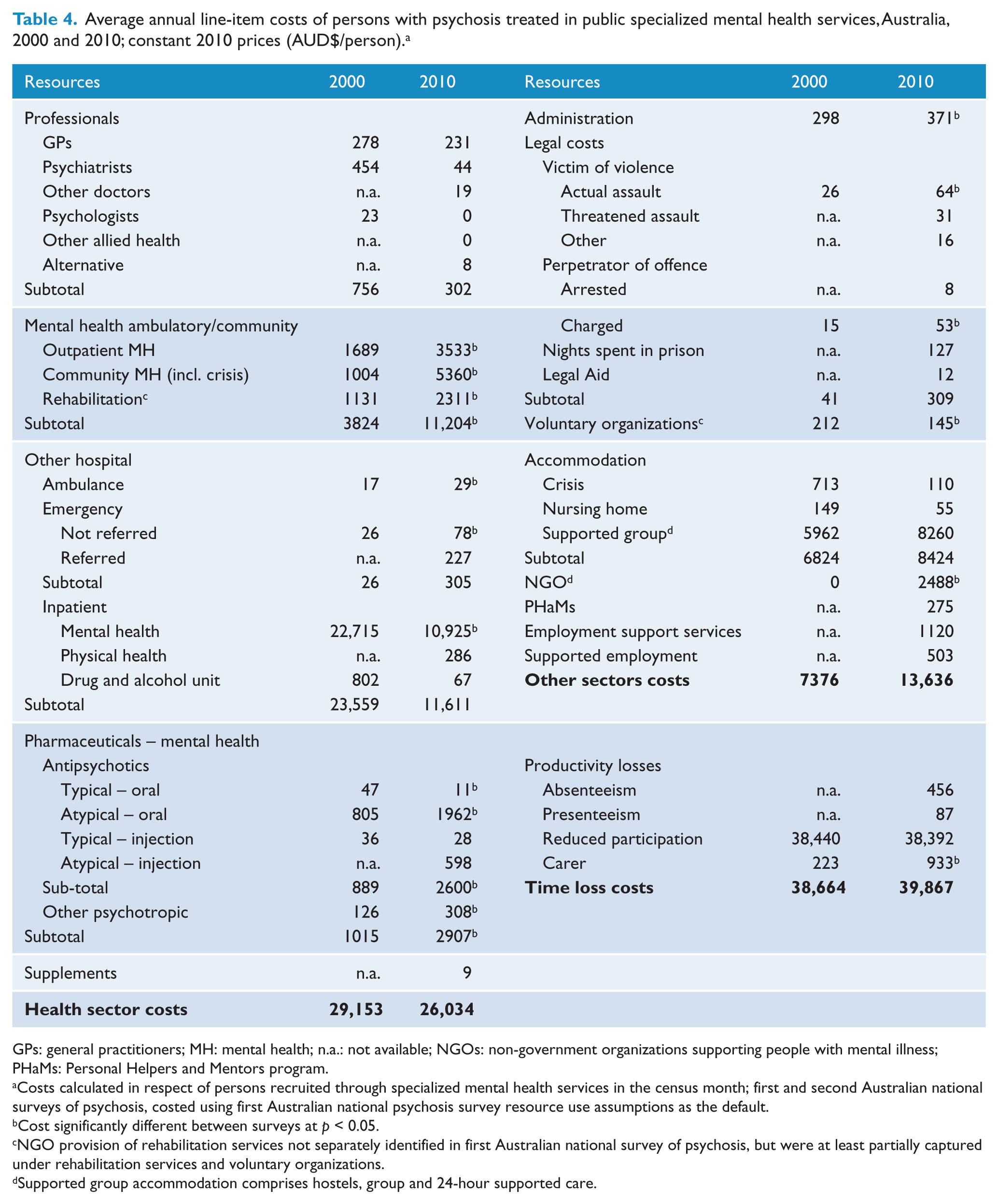
GPs: general practitioners; MH: mental health; n.a.: not available; NGOs: non-government organizations supporting people with mental illness; PHaMs: Personal Helpers and Mentors program.
Costs calculated in respect of persons recruited through specialized mental health services in the census month; first and second Australian national surveys of psychosis, costed using first Australian national psychosis survey resource use assumptions as the default.
Cost significantly different between surveys at p < 0.05.
NGO provision of rehabilitation services not separately identified in first Australian national survey of psychosis, but were at least partially captured under rehabilitation services and voluntary organizations.
Supported group accommodation comprises hostels, group and 24-hour supported care.
As summarized in Table 5, almost three-quarters of this increase in average annual costs ($3183 per person) can be attributed to the inclusion of new items in the cost analysis of the second survey. These additional items (Table 2) were included primarily due to refinements in the survey interview schedule. However, a limited number of items, in particular the Personal Helpers and Mentors Scheme (PHaMs), costing an average $275 per person, did not exist at the time of the first survey. The remaining increase in costs (i.e. costs arising in respect of items that were common across both surveys) reflects a net increase in average costs of $1161 per person.
Cost differential between the average annual costs of psychosis for persons treated in public specialized mental health services in 2000 and 2010 a , by sector and commonality of line items; constant 2010 prices (AUD$/person).
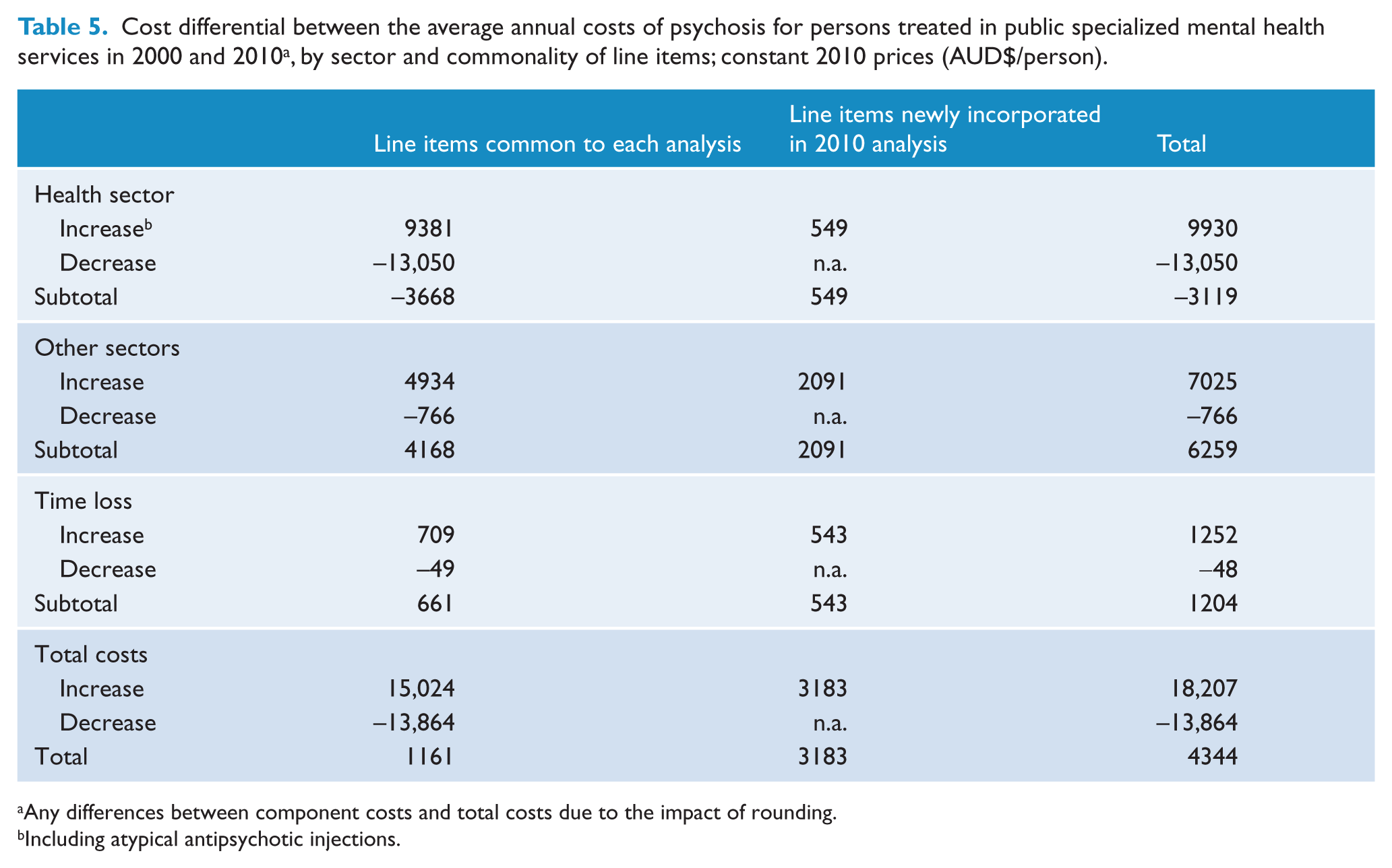
Any differences between component costs and total costs due to the impact of rounding.
Including atypical antipsychotic injections.
Most newly incorporated costs (65.7%) occurred within sectors other than the health sector, with smaller increases of similar size occurring within the health sector and for productivity losses. The greatest net increase in costs for items common across both analyses also occurred within other sectors, followed by productivity losses. There was a net decrease within the health sector.
Average annual health sector costs decreased by $3119 (10.7%) to $26,034 per person between the first and second national surveys, driven by a more than 50% reduction in psychiatric inpatient costs to $10,925 per person (Table 4). The estimated costs for private health professionals other than general practitioners (GPs) were also significantly lower in the second survey. Offsetting these reductions were significant increases in emergency department, ambulatory and medication costs as detailed below. GP costs showed no significant difference between the surveys.
The average costs of emergency department attendances increased 11.7-fold (i.e. 11.7 times the cost estimated for the first survey) from $26 to $305 per person between the surveys, the greatest relative increase estimated. The increase was primarily due to the inclusion of costs for attendances in which the individual was subsequently referred for admission to hospital, at a cost of $227 per person. For emergency department visits in which the individual was not referred for admission to hospital, costs tripled to $78 per person. These impacts are reflected in the breakdown for emergency department costs in Table 4.
Ambulatory costs, encompassing outpatient and community mental health care, increased 2.9-fold between the surveys to $11,204 per person. The cost of pharmaceutical treatment also increased 2.9-fold over the 10-year period to $2907 per person. This rise was primarily driven by the 3.2-fold increase in the cost of atypical antipsychotic medications to $2560 per person. The cost of other psychotropic agents also increased 2.4-fold over the period to $308 per person. In contrast, there was a 2.1-fold (53.0%) reduction in the cost of typical antipsychotic medications to $39 per person.
Average annual costs in other sectors increased 1.8-fold over the period of investigation, increasing by $6259 to $13,636 per person. Newly incorporated resource items gave rise to one-third of the increase ($2091 per person). For items common across both surveys, NGO support and accommodation gave rise to average increases of $2488 and $1600 per person, respectively (Table 4), almost two-thirds of the total increase. The increase in the costs of NGO support was assessed off a zero base, given that NGO services were not separately delineated in the first survey analysis, but were at least partially captured under rehabilitation services and voluntary organizations.
The costs associated with use of voluntary organizations (drop-in centres; NGO drug and alcohol support agencies; community organizations for financial or material aid) declined by almost one-third, from $212 to $145 between the surveys, when first survey usage assumptions were employed (i.e. assuming six occasions of service provision across all providers).
Analysis of the accommodation data shows a trend towards increased expenditure overall and for supported group accommodation specifically, where average annual costs increased by 38.5% from $5962 to $8260 per person. In contrast, the average annual costs of crisis accommodation reduced 84.6% from $713 to $110 per person, while costs for nursing homes reduced to almost one-third at $55 per person. Only the reduction in crisis accommodation costs was statistically significant.
Legal costs included in both surveys comprised criminal justice costs arising because of assaults (actual, not threatened) and for individuals charged with an offence. Average annual costs for these items increased 2.4-fold and 3.5-fold, respectively, from the first to the second survey, to $64 and $53 per person, respectively. If new items in 2010 are taken into account, legal costs increased by $268 per person (7.5-fold), with $193 (72.0%) due to the addition of new items, including incarceration at $127 per person.
The greatest component cost in each analysis was productivity losses, which showed minimal change between the surveys, increasing by $1204 to $39,867 per person (Table 4). Over half of the observed increase in productivity losses was due to the 4.2-fold ($709) increase in the assessed losses arising from the reduced participation of carers (Table 4). Costs for absenteeism and presenteeism gave rise to a further $543 per person. Losses due to reduced economic participation of individuals with psychosis were extensive and constant.
Discussion
This paper provides a comprehensive assessment of change in the costs of psychosis for individuals receiving current treatment within PSMHS over the decade to 2010. The analysis is based on individual data collected in the first and second Australian national surveys of psychosis, undertaken in 1997/1998 and 2010, and costed for 2000 and 2010, respectively. The first survey costing methodology was used as the reference approach. Detailed information on newly incorporated items was separately identified to minimize distortions and maximize transparency.
The average annual costs per person with psychosis receiving current treatment through PSMHS increased 5.8% in real terms between the studies. This increase was a composite of three factors: an increase in costs for several line items common to both analyses, particularly in the health sector and other sectors ($15,024); the inclusion of new items in the second survey analysis ($3183); and the reduction in costs of items common to both analyses ($13,864), particularly mental health inpatient services ($11,790). Overall, there was a redistribution of costs within the health sector and, to a more limited extent, other sectors, as well as an overall increase in costs in other sectors.
The greatest absolute impact on any individual item was the 52% reduction in average mental health inpatient costs to $10,925 per person per annum on average between the first and second surveys. While no directly comparable data are available for the ‘average person with mental illness’, the average cost per mental health separation (ICD-10 F00-F99) is estimated to have declined by about a quarter over the period encompassing the financial years 1999–00 (1 July 1999 to 30 June 2000) to 2009–10. This decline reflects a greater relative increase in separations than recurrent national expenditure: separations doubled from 159,292 to 329,533 (Australian Institute of Health and Welfare, 2001, 2011a), whilst recurrent national expenditure increased by 50%, from $1126 million to $1692 million (Table 6).
National recurrent expenditure for selected mental health resources, 1999–00 and 2009–10; constant 2009–2010 prices.
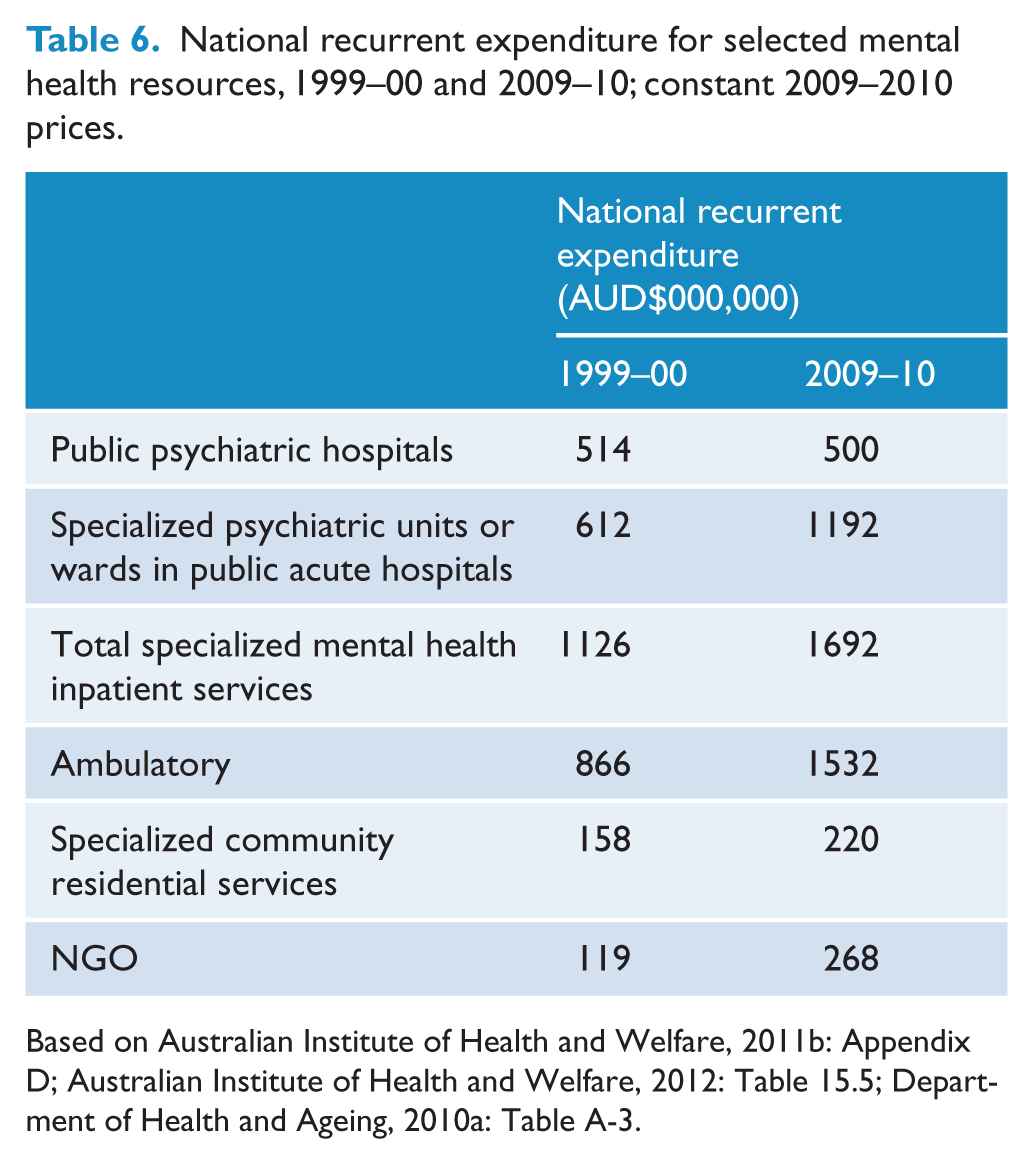
Based on Australian Institute of Health and Welfare, 2011b: Appendix D; Australian Institute of Health and Welfare, 2012: Table 15.5; Department of Health and Ageing, 2010a: Table A-3.
The increase in recurrent national expenditure on specialized mental health inpatient services between 1999–00 and 2009–10 was driven by a doubling of expenditure on specialized co-located units (Table 6) that was at least in part due to increased costs of provision (Department of Health and Ageing, 2010b: 46). In contrast, expenditure on stand-alone psychiatric hospitals decreased by 2.6% (Table 6), expenditure at its highest level in 2009–10 since the nadir in 2001-02. In 2001-02, expenditure on stand-alone psychiatric hospitals was $482 million (constant 2009–10 prices), 41% lower than at the introduction of the First National Mental Health Plan in 1992–93 (based on Australian Institute of Health and Welfare, 2011b: Appendix D; Australian Institute of Health and Welfare, 2012: Table 15.5; Department of Health and Ageing, 2010a: Table A-3). The reduction was primarily directed at the provision of non-acute hospital beds (Department of Health and Ageing, 2010b: 6).
Together, the mental health inpatient cost data presented in this paper, and the national expenditure data outlined above, indicate that the reduction in expenditure on stand-alone psychiatric hospitals appears to have had a predominant and lasting impact on service provision to the population with psychosis. Further, concern expressed consequent to the first survey that mental health inpatient care might be being used as surrogate accommodation (Carr et al., 2002), no longer appears valid. If there was use of mental health inpatient care as surrogate accommodation, it has either greatly reduced or is no longer so.
The greatest absolute increase in cost for any individual item was for community mental health, which increased 5.3-fold to $5360 per person per annum on average. Overall, the average cost per person for ambulatory care increased 2.9-fold to $11,204, exceeding mental health inpatient costs. In comparison, national expenditure on ambulatory care increased 1.8-fold over the period 1999–00 to 2009–10 (Table 6). Given that increases in community health service contacts and expenditure were commensurate between 2001–02 and 2009–10 (based on Australian Institute of Health and Welfare, 2011b: Appendix D; Australian Institute of Health and Welfare, 2011c: Table 4.2; Department of Health and Ageing, 2010a: Table A-3), the above data indicate that people with psychosis have been major beneficiaries of investment in ambulatory care. Such investment is consistent with policy directives from the outset of the National Mental Health Strategy and concomitant funding initiatives over the period. Further, with investment in mental health ambulatory care reportedly receiving almost half of the replacement services funding arising from the reduction in services provided through stand-alone psychiatric hospitals (Department of Health and Ageing, 2010b), the observed investment in community mental health can be seen, at least in part, as a consequence of this shift in funding priorities.
With ambulatory costs comprising 42.3% of health sector costs in 2010, and mental health inpatient costs falling from 77.9% to 42.0% of health sector costs between the surveys, inpatient care can now justifiably be considered as just one of several pillars of psychosis treatment alongside ambulatory care and pharmaceutical treatment, rather than as the mainstay.
The real costs of pharmaceutical treatment almost tripled over the 10-year period 2000 to 2010, driven by atypical antipsychotic medication. Across oral and injectable formulations, the costs of atypical antipsychotics increased 3.2-fold (218.0%), which is highly commensurate with the increase of 217.7% in the level of dispensing for these agents observed over the period 2000 to 2011 (Stephenson et al., 2013). Similarly, the cost of typical antipsychotics reduced by 53.0% within the study period compared with a 61.2% reduction in levels dispensed, as reported by Stephenson and colleagues.
Decreased inpatient costs, and increased outpatient and medication costs over time have also been observed in the United States of America (Wu et al., 2005) and France (Sarlon et al., 2012). In the USA, the change was linked to financial incentives operating within and towards the Medicaid program, and possibly to the uptake of atypical antipsychotics. In France, indirect reference was also made to atypical antipsychotics as a possible cause for the increase in medication costs. Inflation may also have influenced these results, as it is unclear if constant pricing was employed.
Augmenting the shift towards ambulatory care within the Australian health sector has been a significant increase in mental health support provided through NGOs, particularly for rehabilitation. Between the first and second surveys, the costs of rehabilitation across NGO providers and PSMHS were assessed to have increased 3.7-fold (data not shown). In comparison, the costs of mental health support services provided through NGOs is estimated to have increased 2.3-fold nationally between 1999–00 and 2009–10 (Table 6), with most growth occurring since 2003 following the introduction of the Third National Mental Health Plan (Department of Health and Ageing, 2010b: 40). Given that utilization of NGO services was concentrated amongst persons recruited through these services (Neil et al., 2014), the data support a major investment in NGO service provision for people with psychosis, a further reflection of the shift towards community-based care.
In the current analysis, the costs for emergency department visits not referred for admission were found to have tripled over the 10-year period to 2010. This increase in costs is due to a 2.6-fold real increase in unit cost and a 4.9-fold increase in the average number of emergency department visits not referred for admission. This increase in visits is, in turn, consequent to a 2.8-fold increase in the number of people seeking care, and a 1.7-fold increase in the number of times these individuals sought care. The cause of this increase in demand on emergency departments is worthy of further investigation, particularly in light of the decrease in inpatient costs. The increase may in part be due to the lack of immediately available acute mental health beds when individuals are assessed as being in need of admission, as has been shown for Victoria (Emergency Medicine Research Unit, 2006) and/or insufficient community-based care, as has been suggested in South Australia (Kalucy et al., 2005).
GP costs show no significant difference between the surveys, even though policy initiatives have sought to promote ‘shared care’ in the treatment of the mentally ill (Lee et al., 2010). That there is no difference in costs of GP care is likely to reflect the population being studied (i.e. current clients of PSMHS). This grouping of individuals has been postulated to comprise acute and/or recently active recurrent cases (Neil et al., 2014). It is our contention that this group is less likely to receive treatment under a shared care arrangement at this point of their illness trajectory, thus the impact of initiatives directed at shared care for the wider population of people with psychosis is not well captured in this study.
The decrease in costs for professional consultations other than for GPs is likely to be, at least in part, due to an artifact of the data collection process. The relevant elements of the survey instrument changed from the first to the second survey where they were incorporated under a generic item, rather than being separately delineated.
Within this study, the average annual costs for accommodation are assessed as having increased by almost a quarter, driven by a 38.5% increase in supported group accommodation costs, offset by a 84.6% decrease in the costs of crisis accommodation. Neither the increase in accommodation costs nor supported group accommodation costs were assessed as statistically significant, but a redistribution of accommodation costs towards more stable long-term accommodation is indicated.
Long-term stable accommodation is of benefit to the well-being of the population with psychosis whilst, given the available data, also generating direct cost offsets. However, investment in community residential services for people with mental illness has been identified as inadequate relative to the reduction in inpatient services since the implementation of the National Mental Health Strategy in 1993 (Department of Health and Ageing, 2010b: 49). This concern appears to be substantiated for people with psychosis. The 38.5% increase in supported group accommodation costs assessed within this analysis parallels a similar 39.5% increase in total national expenditure on specialized mental health community residential services over the decade to 2009–10 (Table 6), with both considerably less than the 51.9% decrease in mental health inpatient costs between the surveys.
A large fall in the costs of voluntary/charitable organizations was observed between the surveys. This fall, a reduction in costs by over a quarter, is primarily due to a halving in the unit cost from $152 to $76 (constant 2010 prices). Offsetting the price reduction was a 46% increase in the number of persons accessing these services (21.9% and 31.9% in the first and second surveys, respectively). Given that the best available data were used in the assessment, and as voluntary organizations are dependent upon donations, the question arises as to whether these organizations are doing more with the same amount or, given demands on the charity dollar, are doing more with less.
In comparison to the halving of the unit cost for voluntary organizations, the unit cost for criminal justice events (Magistrates’ Court costs) experienced a 2.5-fold real increase (i.e. over and above inflation) from $182 (constant to 2010) to $454 over the decade. This increase in turn underpinned the increase in legal costs for items common across both surveys: a 2.5-fold increase in the costs of assaults (actual, not threatened) and a 3.6-fold increase in the costs of individuals charged with an offence. For both surveys, the costs of actual assaults (one of the three ‘victim of violence’ categories) exceeded the costs of individuals being charged with an offence.
The greatest costs in each analysis were productivity losses, accounting for 51.4% and 50.1% of total costs in the two surveys. The primacy of productivity losses in the costs of schizophrenia and psychosis is consistent throughout the literature, in analyses employing a spectrum of approaches (Chang et al., 2008; Gustavsson et al., 2011; Mangalore and Knapp, 2007; Wu et al., 2005). The productivity losses for both surveys primarily arose from reduced participation of individuals with psychosis, and were remarkably constant between the surveys, reflecting similar average durations of weeks not worked: 43.7 weeks (first survey) and 42.4 weeks (second survey). In both surveys, the number of individuals in receipt of government income support remained constant at 85%, with the proportion receiving a Disability Support Pension actually increasing from 68.3% in the first survey (Jablensky et al., 1999) to 73.7% in the second survey.
Productivity losses associated with the reduced participation of carers did show a significant 4.2-fold increase between the surveys. This increase can be attributed to a 2.4-fold increase in the number of carers receiving the Carer Payment, from 1.4% (11/763) to 3.4% (170/5074), and to the provision of care for a longer period of time on average. The average duration of care received in the previous 12 months was 39.9 and 50.1 weeks in the first and second surveys, respectively.
The uptake in the Carer Payment is lower than for the Australian population in general, for whom there was an almost 5.0-fold increase between 1998 and 2010 (Department of Families, Housing, Community Services and Indigenous Affairs, 2011). Of several reasons put forward for the uptake (Kingston, 2008), the ageing of the population and increased eligibility criteria are likely to have had a much greater impact for the population in general.
This study is the first to fulfill a call within the literature for new studies of the COI of psychotic disorders to employ comparable methodologies (McEvoy, 2007). No other set of studies has been identified throughout the COI literature that use such refined data in the assessment and comparison of costs over time.
This study provides continuing evidence of the comparative importance of productivity losses in the costs of psychosis. It also confirms the findings of previous studies indicating a shift from inpatient care towards community-based care, and an increase in medication costs. In addition, it highlights extensive growth in other sector costs, indicating the critical importance of including these costs, and an appraisal of the services they provide, in future studies. Finally, these data support the reality of mental health service provision that extends beyond the health sector and, given the overarching importance attributed to social and economic needs within this population (Morgan et al., 2011, 2012), underpin a need for a collaborative and integrated system of care that crosses sectoral boundaries. A whole-of-government approach is a strategic means of implementing care directed at maximizing the well-being of people with psychosis, care that addresses the multiple, complex needs of these individuals.
While the assessed redistribution of costs is consistent with government policy initiatives and funding directives, the question remains as to whether the redistribution has led to an improvement in outcomes for individuals with psychosis? A comparison of the study data with cross-sectional data collected during the first national psychosis survey in 1997/1998 suggests some improvement in the overall course of disorder, a higher proportion of people satisfied with their own independence, and a smaller proportion reporting unmet needs (Morgan et al., 2012). However, the proportion with obvious or severe dysfunction in quality of self-care has remained unchanged at 32%, and levels of employment have remained consistently low. It is evident, given the primacy of productivity losses within the costs of psychosis that improvements in employment will be necessary to achieve significant cost reductions in the future.
The treatment, support and care of people with psychosis remains a ‘work in progress’. Significantly more remains to be achieved in order that the well-being of people with these disorders can be improved, let alone maximized. Such improvements will be dependent on additional investment, at least in the short term. The efficiency of any interventions should necessarily be assessed to ensure their value for money.
Strengths and limitations
To obtain the most robust assessment of change in cost profiles between the first and second Australian national surveys of psychosis, every effort was made to maximize comparability by limiting differences in survey design and implementation, and costing methodology employed. In consequence, the current results apply only to that proportion of the population with psychosis actively receiving treatment through PSMHS. From the companion paper (Neil et al., 2014), it is clear that cost profiles may differ according to primary service provider (e.g. PSMHS, NGOs, etc). The change in cost profiles for the entire population with psychosis, including individuals primarily supported through NGOs, general practitioners and private providers, and, in turn, the change in total costs of psychosis over the last decade, are therefore unknown. Future research on these changes would provide decision-makers with information on the comparative uptake of initiatives and identify areas of ongoing need.
Conclusions
Over the decade to 2010, there was little overall change in the costs of psychosis for individuals treated within public specialized mental health services. However, a significant redistribution of costs is observed within and between the health sector and other sectors. This redistribution is in line with government initiatives arising from the National Mental Health Plan directed at ambulatory care and NGO services, offset by reductions in mental health inpatient care. Mental health inpatient costs reduced by more than a half between the surveys. A redistribution of accommodation costs towards more stable long-term accommodation appears to have occurred in spite of minimal investment. Productivity losses remain the greatest component cost for psychosis, still giving rise to over half the annual average costs consequent to the high and constant levels of low employment participation in this population. The data presented support the reality of ‘specialized mental health services’ that extend beyond the ‘health sector’, and the need for a broad-ranging, strategic and functional whole-of-government approach to care. In turn, the growth in other sector costs indicates the critical importance of including these costs in future studies.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis (SHIP). The members of the Survey of High Impact Psychosis Study Group are: V. Morgan (Project Director); A. Jablensky (Chief Scientific Advisor); A. Waterreus (Project Coordinator); A. Mackinnon (Statistician); R. Bush, D. Castle, M. Cohen, C. Galletly, C. Harvey, P. McGorry, J. McGrath, H. Stain (Site Directors); V. Carr (Australian Schizophrenia Research Bank); A. Neil (Health Economics); B. Hocking (SANE Australia); S. Saw (Australian Government Department of Health and Ageing). Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The study was funded by the Australian Government Department of Health and Ageing.
The report also uses data collected in the framework of the Collaborative Study on Low-Prevalence (Psychotic) Disorders (LPDS), an epidemiological and clinical investigation which was part of the National Survey of Mental Health and Wellbeing, Australia 1997–1998. The members of the Low-Prevalence (Psychotic) Disorders Study Group were: Professor Assen Jablensky (Project Director and Team Leader, Western Australia); Professor Vaughan Carr (Adviser); Dr David Castle (Deputy Team Leader, Western Australia); Dr Mandy Evans (Team Leader, Australian Capital Territory); Professor Oye Gureje (Deputy Team Leader, Victoria); Dr Carol Harvey (Deputy Team Leader, Victoria); Professor Helen Herrman (Team Leader, Victoria); Mrs Ailsa Korten (Statistician); Associate Professor John McGrath (Team Leader, Queensland); Ms Vera Morgan (Project Database Manager). Other investigators at the four sites included: Scott Henderson, Stephen Rosenman, Jo Medway (Australian Capital Territory); David Chant, Susette Cardy, Chris Young, Ben Chapple (Queensland); Ian Gordon, Tom Trauer, Helen Evert, Tony Pinzone (Victoria); Anna Waterreus (Western Australia). A complete list of the investigators is available in: Jablensky A, McGrath J, Herrman H, et al. on behalf of the study group (1999) People Living with Psychotic Illness: An Australian Study 1997–98. National Survey of Mental Health and Wellbeing – Report 4. Canberra: Australian Mental Health Branch, Commonwealth Department of Health and Aged Care. Ethics approvals for the study were obtained from relevant institutional ethics committees. Full details are available on request.
This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the LPDS and SHIP surveys and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded under contract to the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.