
Abstract
Objectives:
Although there is growing international recognition of pathological technology use (PTU) in adolescence, there has been a paucity of empirical research conducted in Australia. This study was designed to assess the clinical features of pathological video gaming (PVG) and pathological Internet use (PIU) in a normative Australian adolescent population. A secondary objective was to investigate the axis I comorbidities associated with PIU and video gaming.
Method:
A total of 1287 South Australian secondary school students aged 12–18 years were recruited. Participants were assessed using the PTU checklist, Revised Children’s Anxiety and Depression Scale, Social Anxiety Scale for Adolescents, revised UCLA Loneliness Scale, and Teenage Inventory of Social Skills. Adolescents who met the criteria for PVG or PIU or both were compared to normal adolescents in terms of axis I comorbidity.
Results:
The prevalence rates of PIU and PVG were 6.4% and 1.8%, respectively. A subgroup with co-occurring PIU and PVG was identified (3.3%). The most distinguishing clinical features of PTU were withdrawal, tolerance, lies and secrecy, and conflict. Symptoms of preoccupation, inability to self-limit, and using technology as an escape were commonly reported by adolescents without PTU, and therefore may be less useful as clinical indicators. Depression, panic disorder, and separation anxiety were most prevalent among adolescents with PIU.
Conclusions:
PTU among Australian adolescents remains an issue warranting clinical concern. These results suggest an emerging trend towards the greater uptake and use of the Internet among female adolescents, with associated PIU. Although there exists an overlap of PTU disorders, adolescents with PIU appear to be at greater risk of axis I comorbidity than adolescents with PVG alone. Further research with an emphasis on validation techniques, such as verified identification of harm, may enable an informed consensus on the definition and diagnosis of PTU.
Introduction
Pathological use of digital technologies, particularly the Internet and video games, is a topic of increasing research and conjecture in psychology and psychiatry (Sim et al., 2012; Weinstein and Lejoyeux, 2010). Although computer-based activities have been demonstrated empirically, under certain conditions, to become psychologically, socially, and/or physically detrimental to the user (Kuss and Griffiths, 2012; Mentzoni et al., 2011; Tejeiro Salguero and Morán, 2002), some authors have challenged the notion that problematic technology use should constitute a mental disorder in its own right (Blaszczynski, 2006; Pies, 2009; Wood, 2008). Complicating this issue is the fact that terms such as pathological technology use (PTU), technology dependency, maladaptive technology use, excessive technology use, and technology-based addiction have been used in the extant literature, and that these terms are often regarded as synonymous despite evident variations in definitional criteria (King et al., 2013c) .
Notwithstanding objections to the disorder, it has been proposed that Internet Use Disorder, which refers to maladaptive video gaming and Internet use, should be included in the appendix of the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a subject of further empirical inquiry. Although this announcement has led to a degree of recognition of digital technology-based problems within clinical nomenclature, there remains some uncertainty as to the definition, aetiology, and correlates of the disorder. To aid current psychiatric understanding of PTU, a critical task of research is to examine the relationship of PTU to psychopathology (e.g. depression and anxiety) to determine whether certain disorders may be a risk or predisposing factor for PTU (Starcevic, 2013). The present study was designed in accordance with this broad objective, and aimed to assess axis I comorbidity of two PTU disorders – pathological video gaming (PVG) and pathological Internet use (PIU) – in a normal Australian adolescent population.
Standardised measurement of PTU represents a contentious issue, with several inconsistencies in approaches and tools currently evident in the literature (King et al., 2013c). A common limitation of available tools is the lack of consideration of Internet use and video gaming as activities that may sometimes overlap but are otherwise distinct (King and Delfabbro, 2013). The proposed Internet Use Disorder classification in its current format is not sensitive to this delineation, as it contains nine criteria that refer to both activities. Specifically, the criteria refer to: (1) pre-occupation with Internet gaming; (2) withdrawal symptoms when Internet access is taken away; (3) tolerance: the need to spend increasing amounts of time engaged in Internet gaming; (4) unsuccessful attempts to control Internet gaming use; (5) continued excessive Internet use despite knowledge of negative psychosocial problems; (6) loss of interests, previous hobbies, and entertainment as a result of, and with the exception of Internet gaming use; (7) use of Internet gaming to escape or relieve a dysphoric mood; (8) has deceived family members, therapists, or others regarding the amount of Internet gaming; and (9) has jeopardised or lost a significant relationship, job, or educational or career opportunity because of Internet gaming use. As can be observed, seven of the nine criteria refer to Internet gaming (video gaming), whereas the remaining criteria refer to general Internet use. Although this problem of conceptualisation may be considered on first impression as relatively minor, it may have significant consequences in regard to clinical formulation and treatment. For example, a generic PTU classification (or Internet Use Disorder) may overlook, or mistakenly attribute, features and/or correlates that are unique to, or more typical of, either video gaming or Internet use.
Adolescents are known to be especially vulnerable to the development of PTU (Tejeiro et al., 2012). Epidemiological studies suggest that the average Australian adolescent spends almost 5 hours per day engaged in digital media activities, including 2.5 hours using the Internet (Australian Communications and Media Authority, 2007, 2008). Arguably, this level of involvement suggests that digital media use represents a formative environmental influence on adolescent development, and presents many opportunities for enhancing and/or interfering with multiple areas of functioning and daily living. Although research evidence has indicated that online video games may sometimes enable beneficial social relationships for adult players (Cole and Griffiths, 2007; Yee, 2006), several studies of Internet use and gaming among adolescents have documented the negative effects of excessive use, including aggressive behaviour (Anderson et al., 2010), attention problems (Swing et al., 2010), poor academic achievement (Smyth, 2007), decreased empathy (Bartholow et al., 2005), reduced sleep (King et al., 2013b) and impaired social functioning (Gentile et al., 2011). Available research has assisted in quantifying the sequelae of excessive use of digital technology; however, less is known about the standard clinical presentation and associated psychopathology of PTU disorders in adolescence.
The estimated prevalence rate of PTU in adolescence varies by country and by methodological approach. A recent meta-analysis by Ferguson et al. (2011) reported that the most precise prevalence estimate of PTU in Western industrialised countries is 3.1%. However, very few studies of adolescents with PTU have been conducted in the Australian context. A study by Porter et al. (2010) used an online survey to examine self-reported patterns of problem video gaming. The study was advertised on 53 online forums over a 4-month period and recruited 1945 participants. The overall sample was 92.6% male and drawn mainly from Australia and New Zealand, Canada, Europe, and the USA. The majority reported playing video games every day (62.1%), playing longer than planned (59.8%), and playing despite believing that they should not do it (52.0%). The overall prevalence of problem video gaming was 8.0%. This prevalence rate was relatively high as compared to extant studies of PVG (Ferguson et al., 2011; King et al., 2013c), but consistent with online surveys using self-selection methods of recruitment known to target Internet enthusiasts. The adolescent subsample included 1042 people in total, and about 9% of this subsample met the criteria for problem video gaming. Although comorbidity was not assessed, the authors suggested that problem video gamers may be at risk of social anxiety due to reporting having fewer real-life friends and a preference for online social activity. Specific analyses of adolescent users were not conducted.
A study by Thomas and Martin (2010) surveyed 1326 school students (51% male) to assess video gaming and Internet use and prevalence of pathological use. They reported that lifetime participation and general frequency of use was higher than reported in past studies, suggesting a greater uptake and use of digital media among youth. Prevalence rates of problem use for arcade video games (4.2%), video games (5.0%), and the Internet (4.6%) were comparable to past research. However, as significantly more adolescents were regularly involved in these activities, the results indicated an increase in the total number of adolescent problem users. Comorbidity was not assessed in this study.
In summary, there is only a limited evidence base on the presentation and comorbidity of PTU in adolescents in Australia. Although there have been several studies conducted in Asian countries, Europe, the UK, and the USA, or studies that have used online methods to recruit participants worldwide, very few studies have been conducted in the Australian context only. There currently exists a need to better understand the relationship between pathological digital technology use and psychopathological symptoms in adolescence. Although the mental health risks associated with digital technology use have been documented in survey-based and experimental research studies, there has been no systematic attempt to distinguish PIU and PVG as separate presentations. Therefore, this study aimed to assess the clinical features and axis I comorbidity of PVG and PIU in a large, normal Australian adolescent population. A secondary objective was to identify the range of comorbidities that occur with PIU and PVG.
Methods
Fifty secondary schools in the outer metropolitan region of Adelaide, South Australia, were randomly selected from a comprehensive list of public and private schools. Catholic schools were excluded due to barriers in obtaining ethical clearance. Each school principal was sent a letter and a 1-week follow-up email invitation to participate. The study was promoted as an investigation of electronic media use and mental health in young people. Each participating school was provided with an individualised summary report of findings, which included an indication of the number of adolescents at risk of mental health problems. In total, seven coeducational schools (four public, three private) provided consent to participate. The remaining schools either declined to participate (N = 20) or did not respond to the invitations (N = 23). A total of 1287 high school students aged 12–18 years were recruited. Data were collected from June to August 2012. The study was approved by the Human Research Ethics Subcommittee at the University of Adelaide, and the Department for Education and Child Development. All participants provided informed consent and were free to withdraw from the study at any time.
Measures
A standardised questionnaire assessed basic demographic information (i.e. age, sex, school, grade, ethnic background, main language spoken at home), and dimensions of electronic media use (i.e. media ownership and accessibility, frequency of use of each device in a typical week period over the previous 3-month period, function and social context of media use, and age at which the devices were first used). Psychometric assessment involved the administration of the following tools: the PTU checklist (Sim et al., 2012); the Revised Children’s Anxiety and Depression Scale (RCADS; Chorpita et al., 2000); the Social Anxiety Scale for Adolescents (SAS-A; La Greca, 1999); the revised UCLA Loneliness Scale (Russell et al., 1980), and the Teenage Inventory of Social Skills (TISS; Inderbitzen and Foster, 1992).
The PTU checklist is a 10-item self-report questionnaire used to assess the persistent and recurrent maladaptive use of computers, video games, the Internet and other digital technologies (Gentile et al., 2011; Sim et al., 2012). All questionnaire items were administered using a generic wording (i.e. this activity), with two adjacent columns containing response categories that referred to Internet and video game play, to assess PIU and PVG as separate concepts. For example, an item assessing preoccupation states: Have you become more preoccupied with this activity, or planning the next opportunity to engage in this activity?; an item assessing withdrawal states: Have you become restless or irritable when attempting to cut down or stop engaging in this activity? Internet use referred to any online activity, excluding video gaming which was encompassed by the PVG checklist. The PTU checklist was developed using the fourth edition of the DSM (DSM-IV) criteria for pathological gambling, and it has been shown to have good psychometric properties, including high convergent and predictive validity (King et al., 2013c). PTU checklist items converge with criteria for the proposed DSM-5 Internet Use Disorder category. Scores that include five or more affirmative (yes) responses indicate PTU (Sim et al., 2012).
The RCADS is a widely used tool for assessing children’s symptoms corresponding to selected DSM-IV anxiety and major depressive disorders. The 47-item scale comprises six subscales (i.e. Social Phobia, Panic Disorder, Major Depression, Separation Anxiety Disorder, Generalized Anxiety, and Obsessive–Compulsive). The RCADS has demonstrated good psychometric properties in the Australian population (De Ross et al., 2002).
The SAS-A is a 22-item measure designed to assess the dimensions of social anxiety in adolescents. The measure provides a total score as well as subscale scores in three anxiety domains: fear of negative evaluation, social avoidance of peers, and general social avoidance. Higher scores indicate greater levels of anxiety. The SAS-A has proven convergent validity with the Revised Children’s Manifest Anxiety Scale and the Children’s Depression Inventory (Inderbitzen-Nolan and Walters, 2000).
The revised UCLA Loneliness Scale is a 20-item scale designed to measure subjective feelings of loneliness and social isolation. The tool has been demonstrated to be psychometrically sound. Its unitary factor structure provides a global loneliness score (Russell, 1996). The UCLA Loneliness Scale has been used previously in studies of online behaviour and loneliness (Kraut et al., 1998).
The TISS is a 40-item self-report measure designed primarily to identify adolescents with poor social skills. The TISS yields scores on positive (i.e. prosocial) and negative (i.e. asocial) domains of social behaviour. The test has demonstrated high test–retest reliability, and it correlates significantly with other psychometric measures of social behaviour, as well as self-monitoring data, ratings by peers, and sociometric data (Matson and Wilkins, 2009).
Procedure
The study was conducted at each secondary school during class hours. Three of the authors (DK, DLK, and TZ) facilitated data collection at each of the secondary schools. Upon obtaining consent, a teacher administered the questionnaire to each student in the classroom. An online version of the questionnaire was available via Survey Monkey for those schools with the requisite information technology infrastructure. The online version was completed by 429 participants (33%). Completed surveys responses were compiled and analysed using SPSS for Windows, version 18.0 (IBM Corporation, Armonk, New York, USA). A total of 73 responses were excluded due to erroneous responses or missing data.
Data analysis
Initial descriptive analyses, independent samples t-tests, and chi-square tests were performed on the data set to determine broad demographic differences in relation to the status of PTU. Specific PTU subgroups were created by applying inclusion criteria (i.e. a score > 4 on the PTU checklist) to identify non-PTU, PVG-only, PIU-only, and combined PVG and PIU users. To evaluate potential differences in clinical features and comorbidity rates across different PTU profiles, analysis of variance (ANOVA) techniques were used.
Results
Table 1 presents a summary of the demographic characteristics of the overall sample (N = 1214). The age range of the sample was 12–18 years, with a mean age of 14.8 years (SD = 1.5). A chi-square test indicated that sex was equivalently represented across age groups. There were no significant sex differences in terms of weekly Internet use and television viewing, but male adolescents reported a significantly higher amount of video gaming per week than female adolescents, t(1212) = 15.4, p < 0.01, with a Cohen’s d of 0.89 indicating a very large effect size. As expected, independent samples t-tests revealed that adolescent pathological technology users spent significantly more time per week using the Internet (Mdiff = 226 min), watching television (Mdiff = 115 min), and playing video games (Mdiff = 113 min) than other adolescents.
Demographic and electronic media use characteristics of adolescents with and without PTU classification.
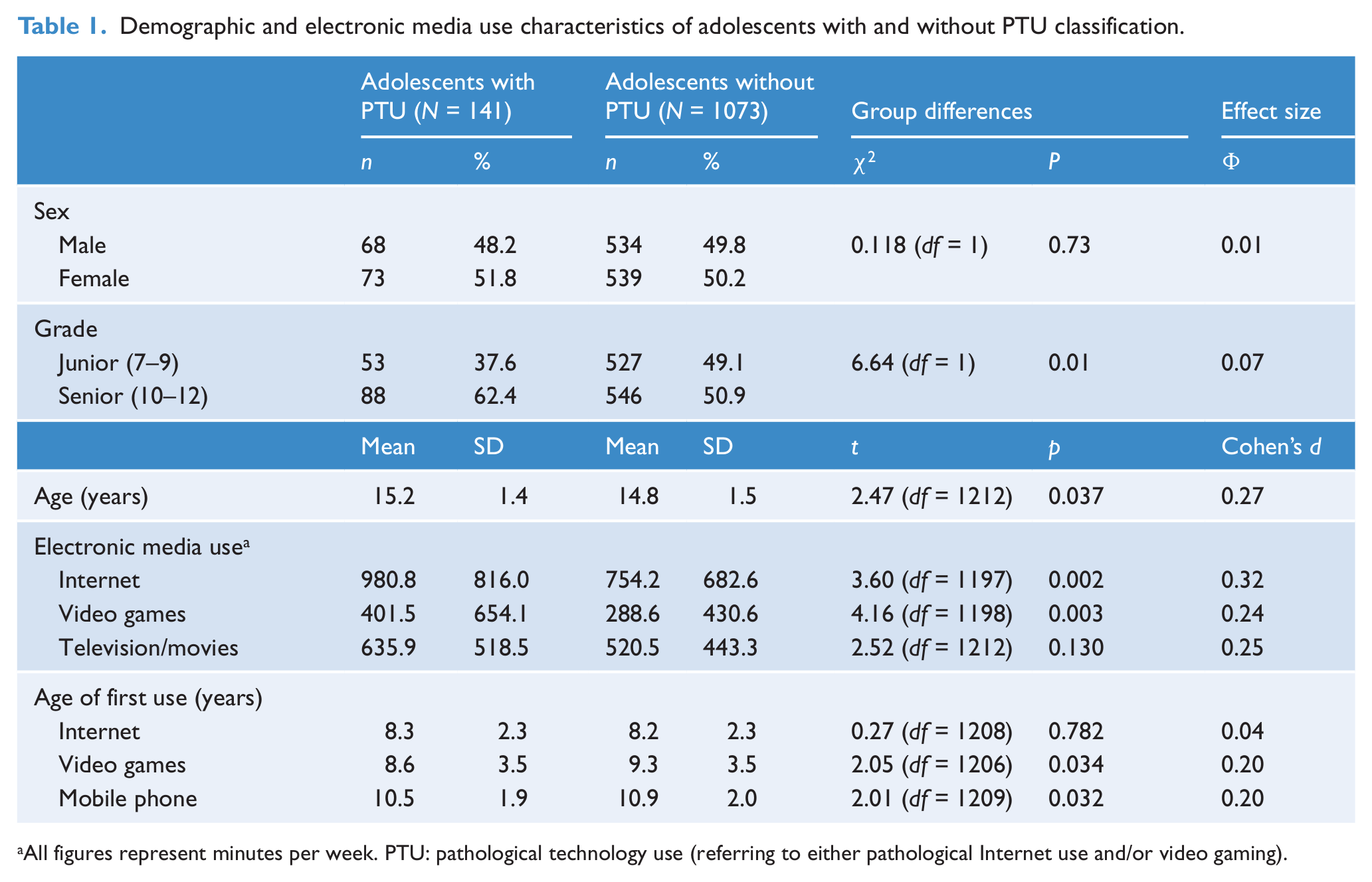
All figures represent minutes per week. PTU: pathological technology use (referring to either pathological Internet use and/or video gaming).
In total, 141 (11.6%) participants met the requisite criteria for pathological use of either video games and/or the Internet. The prevalence of PIU and PVG was 6.4% and 1.8%, respectively. A subgroup of combined PIU and PVG users was also identified (3.3%). As presented in Table 1, pathological technology users as a broad collective did not differ significantly in terms of age or sex. However, further analysis revealed that pathological video gamers were predominantly male (78%), whereas pathological Internet users were mainly female (74%; χ2 = 35.8, p < 0.001, Φ = 0.17). This result suggested that, although both sexes were similarly at risk of PTU, each sex was attracted to different types and functions of digital technology. PTU-classified adolescents were generally slightly older than non-PTU adolescents, but this age difference was equivalent to less than 3 months, which was unlikely to be meaningful in developmental terms.
Tables 2 and 3 present a comparison of the type and severity of clinical features of PVG and PIU-classified adolescents as compared to their normal counterparts. The purpose of this analysis was to identify those PTU symptoms that increase significantly when considering normal and clinical subgroups in relation to each other (i.e. those items that may be better at distinguishing clinical from subclinical users). With regard to PVG, it was found that normal adolescents tended to score more highly on items assessing preoccupation, inability to self-limit, and playing video games as an escape than on other items. A one-way ANOVA assessing PTU group symptom profiles indicated that these same items demonstrated significant but relatively smaller differences as compared to other PTU checklist items. Symptoms with the largest group differences were tolerance, withdrawal, lies and secrecy about use, and conflict at school or work. Interestingly, although an item on antisocial behaviour was relatively rarely endorsed, adolescents with PVG and PIU scored significantly higher on this item than PVG-only users. Given that video gaming was predominantly a male activity, it was reasoned that the normal subgroup’s PTU scores may have been biased by the inclusion of female adolescents who did not play video games. To minimise this sex bias, a secondary analysis was conducted which examined the PTU subgroups in relation to a male-only normal subgroup (n = 527). This analysis yielded a comparable pattern of significant results with identical post-hoc interpretations to those presented in Table 2, indicating that observed differences were not overly influenced by the inclusion of normal female adolescents in the analysis.
Pathological Video Gaming (PVG): Type and severity of clinical features according to clinical classification.
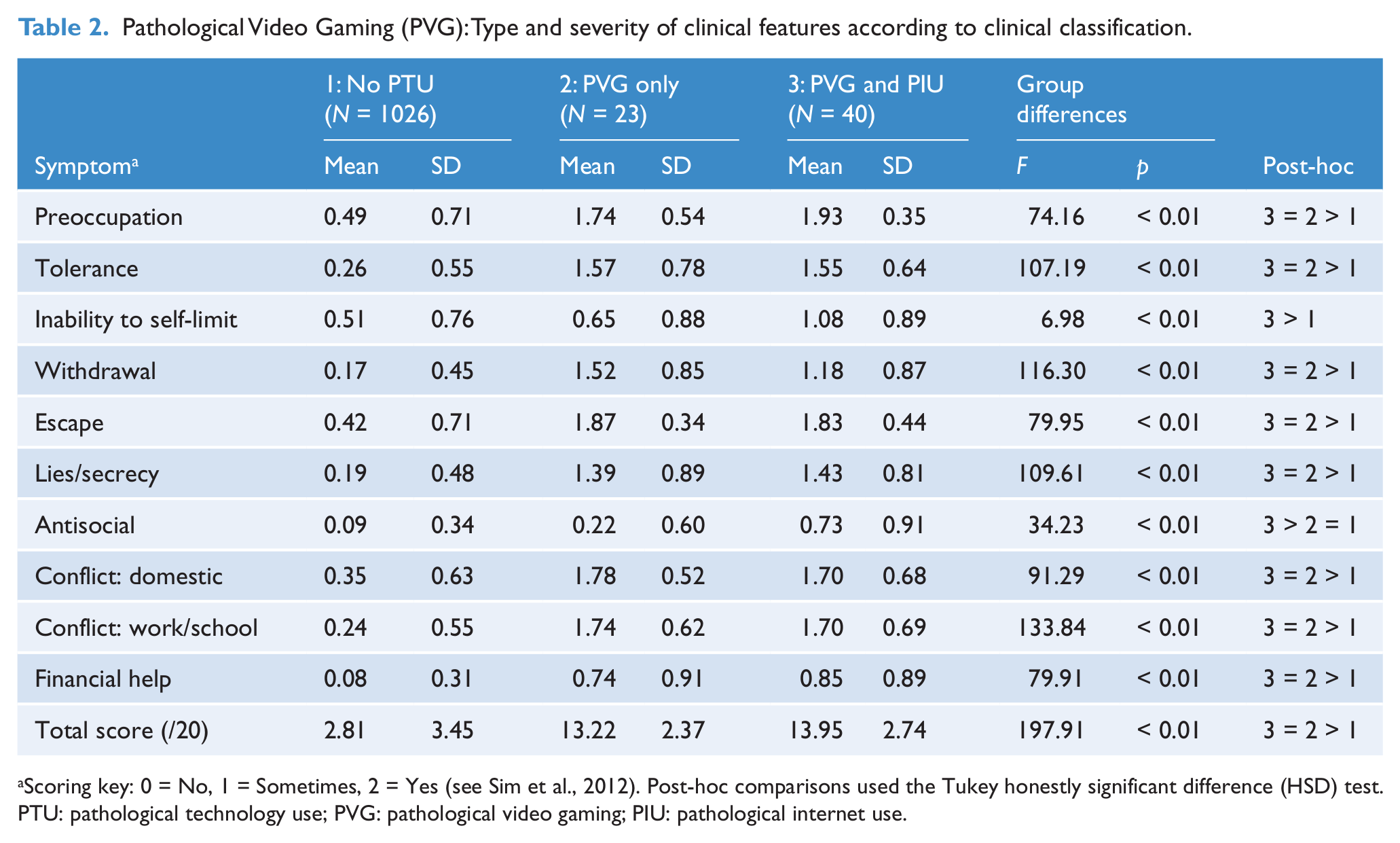
Scoring key: 0 = No, 1 = Sometimes, 2 = Yes (see Sim et al., 2012). Post-hoc comparisons used the Tukey honestly significant difference (HSD) test.
PTU: pathological technology use; PVG: pathological video gaming; PIU: pathological internet use.
Pathological Internet Use (PIU): Type and severity of clinical features according to clinical classification.
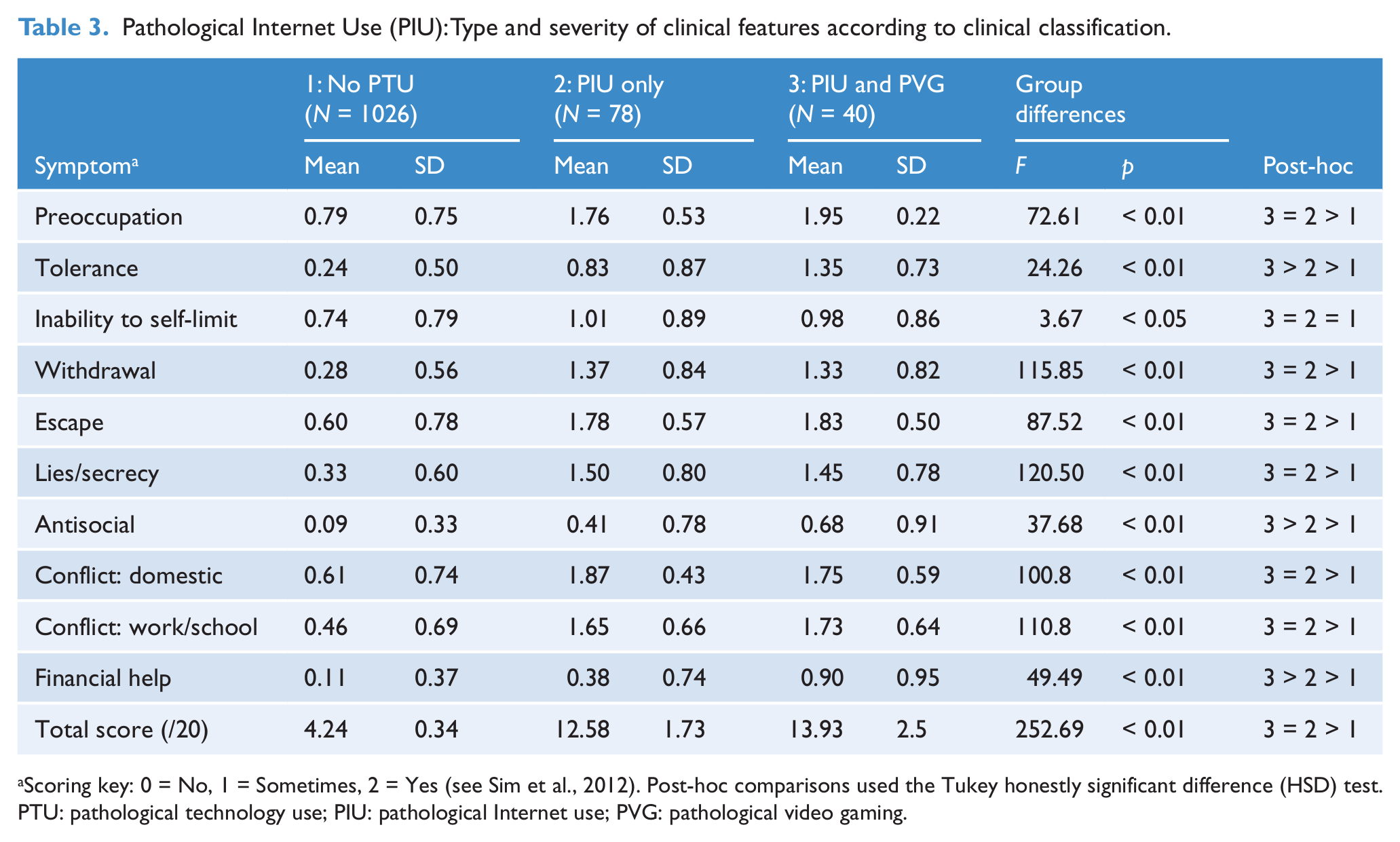
Scoring key: 0 = No, 1 = Sometimes, 2 = Yes (see Sim et al., 2012). Post-hoc comparisons used the Tukey honestly significant difference (HSD) test.
PTU: pathological technology use; PIU: pathological Internet use; PVG: pathological video gaming.
With regard to PIU, we found that normal adolescents tended to score higher on items assessing preoccupation, inability to self-limit, and using the Internet as an escape, as compared to other items. However, these items were less able to distinguish normal and clinical groups than items assessing withdrawal, lies and secrecy, and conflict. The addition of a PVG classification among PIU-classified adolescents was observed to significantly increase the mean score on the item assessing tolerance. Overall, the strongest clinical features of PVG and PIU (i.e. tolerance, withdrawal, deception, and conflict) were endorsed by the PTU subgroups at comparable levels of severity, indicating that the disorders were similar in general presentation of clinical features.
Table 4 presents a summary of comorbidity profiles according to the PTU classification group. The aim was to assess the potential differences in mental health indicators according to type of PTU. Several key differences between normal adolescents and those classified with PIU and/or PVG in relation to axis I symptomatology were evident. PIU-classified adolescents scored significantly higher on the SAS-A than other groups, with scores tending to fall within the clinical range (i.e. > 50) as compared to other groups’ scores in the subclinical range. The PIU group’s RCADS scores on the Major Depression, Panic Disorder, and Separation Anxiety subscales were significantly higher and fell in the borderline range, whereas normal and PVG-classified adolescents scored in the normal range. Secondary analysis identified no statistically or clinically significant sample-level sex differences in Major Depression, Panic Disorder and Separation Anxiety scores, indicating that these PTU between-group analyses were not influenced by sex. The most at-risk PTU group included adolescents with co-occurring PVG and PIU classifications, who reported RCADS Panic Disorder and Separation Anxiety subscale scores in the clinical range. Overall, the PIU groups (i.e. PIU-only and PIU/PVG groups) demonstrated significantly more severe depression and anxiety symptoms than either normal or PVG-only adolescents. In contrast, the PVG-classified group’s SAS-A, UCLA, and RCADS scores did not differ significantly from the non-PTU group. Examination of TISS scores indicated that PVG-classified adolescents showed significantly worse prosocial skills and more asocial behaviour than all other subgroups. However, a follow-up regression analysis indicated this result could be partially accounted for by the over-representation of male adolescents in the PVG group. Overall, the results suggested that PIU was associated with more severe axis I comorbidity as compared to PVG and normal adolescents, independent of a sex effect.
Comparisons between adolescents with and without PTU profiles in terms of comorbidity and social functioning.
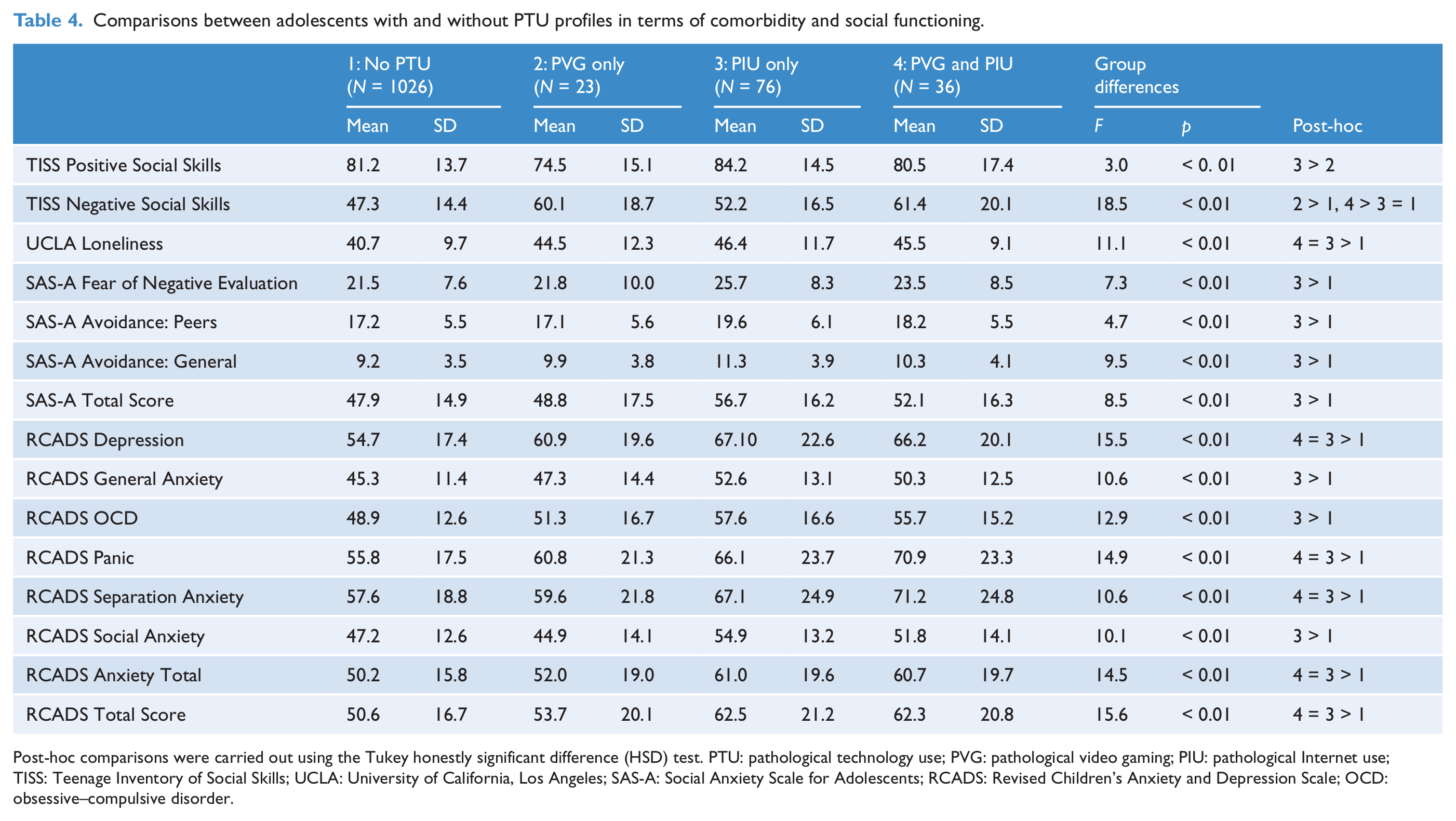
Post-hoc comparisons were carried out using the Tukey honestly significant difference (HSD) test. PTU: pathological technology use; PVG: pathological video gaming; PIU: pathological Internet use; TISS: Teenage Inventory of Social Skills; UCLA: University of California, Los Angeles; SAS-A: Social Anxiety Scale for Adolescents; RCADS: Revised Children’s Anxiety and Depression Scale; OCD: obsessive–compulsive disorder.
Discussion
This study was designed to assess the clinical features and axis I comorbidity of PVG and Internet use in a normal Australian adolescent population. Overall, this study suggested that 11.4% of adolescents met the criteria for PTU, with boys and girls similarly at risk. The prevalence rates of specific PIU and PVG were 6.4% and 1.8%, respectively. An additional subgroup defined by co-occurring PIU and PVG (3.3%) was also identified, a finding which indicates that there is a considerable overlap of the two disorders. Prevalence rates in this study were comparable to several recent large (i.e. N > 1000) studies assessing PIU and PVG (see King et al., 2012a), and rates were consistent with limited Australian data on adolescents and adults (Porter et al., 2010; Thomas and Martin, 2010). The over-representation of males in terms of PVG was consistent with past research (e.g. Cao and Su, 2007; Gentile et al., 2011; King et al., 2013a; Rehbein et al., 2010). However, the finding that female adolescents were over-represented in the PIU group was a novel result as compared with data published in 2010 and earlier (King et al., 2012a). This may reflect an emerging trend towards the greater uptake and use of portable Internet-enabled devices among female adolescents, and particularly the growth in popularity of online social networking via sites such as Facebook (Smahel et al., 2012).
To our knowledge, this study was the first to evaluate the clinical features of PVG and PIU, both individually and in relation to each other. It is currently not clear which features of PTU may be more normative and therefore lacking in utility for clinical diagnosis. Given the preliminary nature of the DSM-5 category of Internet Use Disorder, there is a need for studies that identify features which may be typical (i.e. non-pathological) characteristics of electronic media use. Our data indicated that normal adolescents tend to endorse PTU checklist items related to preoccupation, inability to self-limit use, and using technology as a means of escape. This suggests that these aspects of PTU may be more likely to fall along a continuum representing healthy versus problematic use, and for this reason may be less useful in differentiating problem users. This was consistent with Charlton and Danforth’s (2007) study which showed that cognitive salience (preoccupation) may indicate a non-clinical form of obsession with an activity such as video gaming. Along a similar line, Przybylski et al. (2009) have suggested that preoccupation may occur harmoniously (i.e. the activity is personally important, freely chosen, and in harmony with other aspects of life) or obsessively (i.e. thoughts of the activity are intrusive and cause conflict with aspects of daily life).
As the diagnostic criteria for technology-based pathological behaviour continue to be debated (King and Delfabbro, 2013; Pies, 2009; Starcevic, 2013), the collection of data that delineate the primary clinical features of PTU may offer a useful contribution to the task of refining diagnosis. This study suggests that the most salient items in determining pathological use of both video games and the Internet refer to tolerance, withdrawal, deception, and conflict. Notably, two of these items (withdrawal and conflict) align with an emerging, research-driven definition of PVG (King et al., 2013c). Similarly, Porter et al.’s (2010) proposed definition of problematic video gaming has prioritised withdrawal symptoms as a primary feature. The least salient items referred to antisocial behaviour (e.g. theft) and need of financial assistance (i.e. a bailout). As noted by King et al. (2013), it may be that video gaming, even at high levels of engagement, has significantly lower associated financial costs aside from the initial expense of acquiring video gaming equipment and software. This highlights the flaw in adapting the criteria for one disorder (i.e., pathological gambling) to an activity that does not share common properties with gambling. The DSM-5 Internet Use Disorder criteria does not include pathological gambling-related items on financial difficulties and the need for a bailout from significant others. On this basis, further studies of PTU may consider exclusion of these items.
In its current form, the DSM-5 Internet Use Disorder category is intended as stand-in criteria that signify theoretical importance, and acts to guide further research undertakings. Accordingly, the DSM-5 category does not prioritise any single criterion over another, as other disorders might specify a delineation of primary versus peripheral criteria. It is hoped that this study can add to and guide further investigations aimed at determining criteria of principal importance to the definition and diagnosis of PTU. Further, researchers should be open to the possibility that existing disorders (e.g. pathological gambling and substance dependence disorders) may not, on their own, provide a sufficient guiding framework of clinical indicators to best define PTU. For example, pathological gambling is maintained, in part, by cognitive distortions (e.g. illusion of control, gambler’s fallacy, superstitious beliefs), whereas the underlying cognitions of problem video game playing are unlikely to take this form (King et al., 2012b). Greater knowledge of cognitive factors, among other factors, which underlie PTU may enable development of new items for inclusion in clinical definitions such as Internet Use Disorder.
A notable concern with current assessment tools used to classify PTU is the potential for over-diagnosis (King et al., 2013c). Consistent with recent studies (Choo et al., 2010; Gentile et al., 2011; Tejeiro et al., 2012; Tsitsika et al., 2011), this study reports a prevalence rate of PTU in excess of 5% in a general population sample of adolescents. A prevalence rate at this high level should be regarded by researchers and clinicians alike with a measure of healthy scepticism. This finding would suggest that either PTU has emerged as a leading psychiatric problem among adolescents, with an actual prevalence almost as high as depression and anxiety, or that estimates of PTU are biased towards overestimation of the true nature and severity of pathology. As noted previously, the inclusion of certain items in tools that inflate scores may lead to misdiagnosis. Inappropriate cut-offs that do not reflect true clinical significance is an additional concern. Although this study was consistent with past research in its method of identification of technology-related problems, caution is recommended in considering these findings. As noted by Ferguson et al. (2011), further research with a focus on the identification of harm resulting from excessive technology use should be conducted. External validation by psychiatric consultation may assist in this research endeavour (Tao et al., 2010).
Adolescents’ axis I comorbidity profiles were assessed in relation to several PTU classifications. Notably, PIU-classified adolescents scored significantly higher and within the clinical range on several clinical measures of anxiety and depression, whereas PVG-classified adolescents did not differ greatly from their normal counterparts. Some past research on adolescents has indicated that video game play may have a curvilinear relationship with well-being and pathological use. For example, Durkin and Barber (2002) reported that those youth who did not play video games at all were similar developmentally to those who played excessively, with relevant benefit to those who played a moderate amount. In our study, the most common anxiety-related complaints among PIU adolescents were fear of social situations, panic symptoms, and separation fears. These results converge with an established body of research literature on the relationship between Internet use and psychopathology (see Byun et al., 2009). Given that our findings are based on cross-sectional data, it was not possible to determine whether comorbid disorders preceded or developed concurrently to PIU. However, these findings suggest that pathological Internet users may be at greater risk of co-occurring psychopathology. Adolescent clients referred for problems with Internet use may be more likely than those with video gaming problems to present with axis I features. However, this does not suggest that adolescents with PVG are unlikely to present with axis I pathology. Further research is needed on the comorbidity profiles of PTU users, including adolescents and adults, which may consequently aid in the development of a standard clinical formulation for PTU.
The present study investigated PTU in the largest sample of Australian adolescents since 2005 (see Thomas and Martin, 2010). The recruitment of adolescents from a random selection of Australian secondary schools had distinct methodological advantages over comparable studies that used an anonymous, online survey of international samples biased by self-selection (Griffiths et al., 2004; Porter et al., 2010). The inclusion of two PTU checklists in addition to other psychometric assessment tools with Australian norms was also a notable strength. However, this study should be viewed in consideration of its limitations. First, it was cross-sectional in design and therefore precludes statements of causality or temporal relationships in regard to PTU and comorbidity. Second, youth self-report of mental health issues may not be in and of itself an accurate indication of clinical status. Third, given that data were drawn from adolescents in attendance at school, it is possible that more clinically severe cases may not be represented due to school refusal or other mental health reasons. As noted previously, there remains the important issue of how best to measure and classify PTU disorders. The definition, criteria, and cut-off scores for PTU remain under development and subject to debate (Ferguson et al., 2011; King et al., 2013c). Accordingly, these results should be considered in light of any future variations.
In conclusion, this study suggests that PTU among Australian adolescents remains an issue warranting clinical concern. Although male vulnerability to development of problematic video gaming behaviours has been frequently documented for nearly three decades (Griffiths et al., 2012), females may be at increasing and potentially greater risk of PIU. PIU was associated with more severe comorbid axis I features than PVG, which may present complications for the assessment and treatment of this disorder. Further research on technology-based problems in adolescence is warranted, with an emphasis on validation techniques to develop an informed consensus on the definition and diagnosis of PTU.
Footnotes
Acknowledgements
We thank the students who participated in this study, and the teachers and principals for assistance with data collection. We are grateful to Dr Chad Ebesutani for assistance with scoring of psychometric data.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This study received financial support from a 2012 Young Researcher Grant funded by the European Association for the Study of Gambling.