
Abstract
Objective:
We evaluated the psychiatric comorbidities in adults who were diagnosed with Diagnostic and Statistical Manual of Mental disorders, 5th edition attention-deficit/hyperactivity disorder as a function of recalled symptom onset before and after the age of 7 years and whether the childhood attention-deficit/hyperactivity disorder symptoms were associated with psychiatric comorbidities.
Method:
In all, 214 adults who were diagnosed with Diagnostic and Statistical Manual of Mental disorders, 5th edition attention-deficit/hyperactivity disorder and 174 non-attention-deficit/hyperactivity disorder controls (aged 17–40 years) received psychiatric interviews to confirm their previous and current attention-deficit/hyperactivity disorder status and other psychiatric diagnoses. Demographics and risks of lifetime psychiatric disorders were compared among three groups: (1) attention-deficit/hyperactivity disorder, onset <7 years (early-onset); (2) attention-deficit/hyperactivity disorder, onset between 7 and 12 years (late-onset) and (3) non-attention-deficit/hyperactivity disorder controls. We also tested the effects of attention-deficit/hyperactivity disorder symptoms on the risk of later psychiatric comorbidities by Cox regression analyses.
Results:
Regardless of the age of onset, attention-deficit/hyperactivity disorder was significantly associated with a wide range of psychiatric comorbidities. There were similar comorbid patterns between early- and late-onset attention-deficit/hyperactivity disorder. Regardless of attention-deficit/hyperactivity disorder diagnosis, increased severity of attention-deficit/hyperactivity disorder symptoms was associated with higher risks of oppositional defiant disorder, conduct disorder, dysthymia and sleep disorder but not major depression, which was associated with the attention-deficit/hyperactivity disorder diagnosis.
Conclusion:
Our findings suggest that elevating the threshold of age of onset to 12 years in Diagnostic and Statistical Manual of Mental disorders, 5th edition would not over-diagnose attention-deficit/hyperactivity disorder in the adult population. Recalled childhood attention-deficit/hyperactivity disorder symptom severity was correlated with conduct disorder, oppositional defiant disorder, dysthymia and sleep disorders.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is considered a continuous condition that develops in childhood and might persist into adulthood (Biederman et al., 2010). Although this view has been challenged recently (Moffitt et al., 2015), contemporary clinical consensus suggests that diagnosing adult ADHD requires an accurate recall of childhood symptoms (Adler and Chua, 2002). The age-of-onset criterion (AOC) for ADHD in Diagnostic and Statistical Manual of Mental disorders, 4th edition (DSM-IV), which requires that impairing symptoms should develop by 7 years, seems to have been determined arbitrarily (Barkley and Biederman, 1997). Overestimation of age-of-onset of ADHD by retrospective recall leads to high false-negative diagnostic rate, and thus, a large proportion of adults in need of help are missed (Kieling et al., 2010). For adults first evaluated for ADHD, there may be 50% chance to miss the diagnosis if we use the AOC of DSM-IV by self-report (Kessler et al., 2005) and by parents’ report (Todd et al., 2008). Several cross-sectional studies also found no difference between adults with ADHD onset prior to and after 7 years in psychiatric comorbidity, familial transmission (Faraone et al., 2006b), neuropsychological functioning (Faraone et al., 2006a), personality traits (Faraone et al., 2009), substance use (Faraone et al., 2009) and the response to stimulants (Reinhardt et al., 2007).
The newly published Diagnostic and Statistical Manual of Mental disorders, 5th edition (DSM-5) extends the maximum age-of-onset of ADHD symptoms to 12 years and lowers the symptom threshold to 5 while diagnosing individuals who are aged 17 years and older, intending to decrease the false-negative rate of diagnosing adult ADHD. After the launch of the DSM-5, the first published study that evaluates the validity of this new criteria in adolescents by cross-sectional surveys suggests an increase in prevalence from 7.38% to 10.84% (Vande Voort et al., 2014), which is, however, contradictory to an only 0.1% increase in the previous report by Polanczyk et al. (2010). There is actually no difference in the patterns of comorbidities and severity of impairment between early-onset and late-onset ADHD in these two studies. There has been no such study for adult ADHD after the DSM-5 was published. Given the doubts of overtreatment for ADHD, further validation of adult ADHD according to the DSM-5 criteria is necessary (Batstra and Frances, 2012).
Longitudinal (Biederman et al., 2012; Mannuzza et al., 1993) and cross-sectional (McGough et al., 2005) studies showed similar patterns of psychiatric comorbidities in ADHD adults as those in youths with ADHD (Gau et al., 2010; Spencer, 2006), although controversy existed with regard to anxiety and depression (Klein et al., 2012; Murphy and Barkley, 1996). The psychiatric comorbid pattern is thought as an ambiguous support for the validity of adult ADHD (Faraone et al., 2000). Child ADHD and adult ADHD were viewed as the same syndrome (Faraone, 2000) because of similar comorbid patterns (Biederman et al., 1993). This study intends to testify the validity of the DSM-5 criteria for ADHD by evaluating whether there are similar psychiatric comorbid patterns between adults with ADHD symptoms onset by and after 7 years of age.
From the developmental view, depressive, anxiety and disruptive disorders often develop several years after the onset of ADHD (Taurines et al., 2010). The development of later psychiatric comorbidities may be the results of psychosocial stress and adaptation of the earlier disorders, biological/genetic factors and interactions between these factors (Taurines et al., 2010). To clarify the complex correlations of these disorders is out of the scope of this study. Psychiatric comorbidities usually bring impacts on affected individuals, e.g., depressive disorder and/or conduct disorder (CD) may lead to higher suicidality (Biederman et al., 2008; James et al., 2004) and poorer quality of life (Klassen et al., 2004) in adolescence and adulthood. Fewer studies have evaluated whether ADHD symptom severity during childhood affects the risk of developing comorbidities among adults with ADHD; we therefore want to provide more information in prediction.
Aims of the study
The first study aim is to compare the risk of developing other psychiatric disorders between adults with early-onset, late-onset ADHD and adult controls without lifetime or current ADHD diagnosis (non-ADHD controls) to verify the new DSM-5 AOC. The second aim is to verify whether increased inattention or hyperactivity/impulsivity symptoms during childhood would lead to higher risks for CD, oppositional defiant disorder (ODD), anxiety disorders and depressive disorders. We hypothesize that there are comparable patterns and risks of developing psychiatric comorbidities between early- and late-onset ADHD. Childhood ADHD symptom severity might not be necessarily correlated with the risk of developing depressive disorder (Biederman et al., 1998), but might be correlated with other comorbidities.
Method
Participants and procedures
The procedure and sources of participants are summarized in Table 1, and the details of procedure are described in Supplementary Material. In brief, we recruited adults with ADHD, aged 17–40 years, from two resources: follow-up cases with childhood medical record of ADHD in the National Taiwan University Hospital (NTUH) and new cases by advertisement or referred by psychiatrists or family physicians in NTUH. They were clinically diagnosed with ADHD or subthreshold ADHD (age onset >7 years old or only five out of nine symptoms of each of the inattention and hyperactivity–impulsivity subscales) according to the Diagnostic and Statistical Manual of Mental disorders, 4th edition–Text Revision (DSM-IV-TR) diagnostic criteria for ADHD. Non-ADHD controls were recruited by advertisement.
Procedure and source of participants.
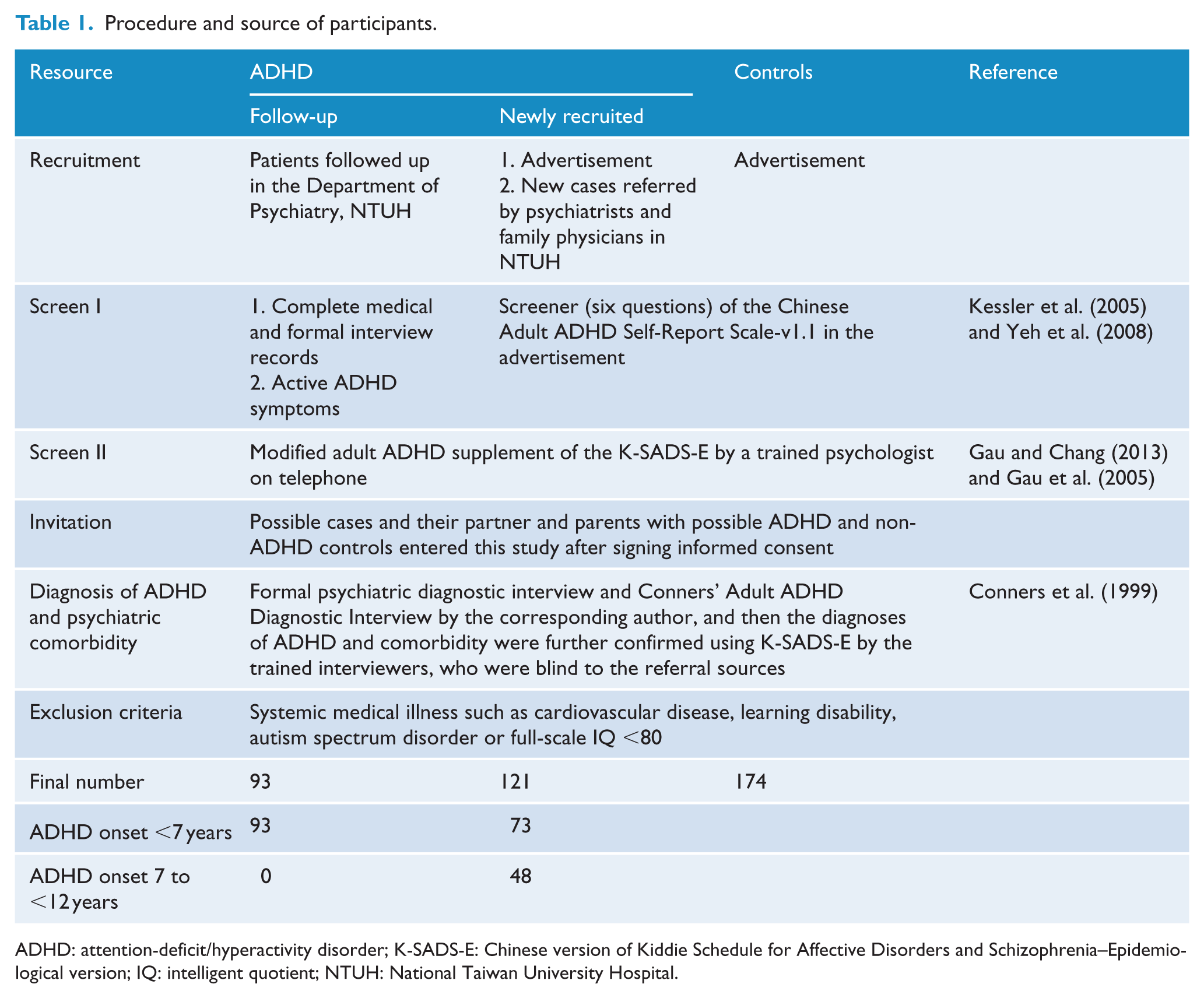
ADHD: attention-deficit/hyperactivity disorder; K-SADS-E: Chinese version of Kiddie Schedule for Affective Disorders and Schizophrenia–Epidemiological version; IQ: intelligent quotient; NTUH: National Taiwan University Hospital.
The Research Ethics Committee of NTUH, Taiwan (approval number, 2010003087R; ClinicalTrials.gov number, NCT01247610), approved this study prior to its implementation. All the participants received full explanation about the study design, objectives and procedures of the study and their rights to confidentiality and autonomy. They could withdraw from the study whenever they had doubts. For adults with ADHD, psychiatric service was provided no matter whether they participated in the study or not. There were no incentives for all the participants except that we provided the reports of all the assessments completed in this study (including brain imaging reports) with face-to-face explanation of the results.
After the whole interview process (Table 1), adults who met the diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) for ADHD were classified into two groups by the age of onset: <7 years old (early-onset) and 7 to <12 years old (late-onset). We asked participants to recall the age of onset of each disorder of which they report a positive history during the psychiatric interview. All the participants received intelligence assessment using the Wechsler Adult Intelligence Scale III–Revised.
Measure
The Chinese Kiddie Schedule for Affective Disorders and Schizophrenia–Epidemiological version
The Chinese Kiddie Schedule for Affective Disorders and Schizophrenia–Epidemiological version (K-SADS-E) has been proven to be a reliable and valid instrument to assess child and adolescent psychiatric disorders (Gau et al., 2005). The corresponding author modified the ADHD, ODD and CD supplement of the Chinese K-SADS-E for the diagnosis of childhood ADHD, ODD and CD, and current adult ADHD diagnosis in adult populations (Gau and Chang, 2013). Other diagnoses included in the K-SADS-E are originally derived from the SADS (Merikangas et al., 1998), a semi-structured interview based on DSM-IV-TR criteria which has been widely used in assessing mental disorders in adult population (Wu et al., 2011). The inter-rater reliability was high for major depression, 0.79; bipolar disorder, 0.71; and anxiety disorder, 0.86 (Wu et al., 2011).
Interviewer training
The corresponding author was responsible for training interviewers for the psychiatric interview including the Chinese K-SADS-E and Schedule for Affective Disorders and Schizophrenia (SADS) interviews (including the modified adult ADHD supplement). The details of training procedure are described elsewhere (Lin et al., 2015) and in Supplementary Material.
Agreement in reporting ADHD symptoms
Before study implementation, we used a follow-up sample of 56 young adults with childhood diagnosis of ADHD and 50 typically developing young adults without lifetime or current diagnosis of ADHD to examine the agreement between child report and adult’s retrospective recall of childhood ADHD symptoms as assessed by the ADHD supplement of the Chinese K-SADS-E. There was high agreement in reporting childhood ADHD symptoms at two time points, i.e., at childhood and adulthood, either by self-report or by parents’ report, and there was 100% agreement in the diagnosis of ADHD (see Supplementary Material for detailed descriptions).
Statistical analyses
Data analysis was conducted using SAS 9.2 (SAS Institute Inc., Cary, NC). We used linear regression for continuous variables, Chi-square for categorical variables and the Bonferroni correction method to adjust for multiple comparisons in the post hoc analyses. Raw data and odds ratios of psychiatric comorbidities between groups were calculated by the logistic regression model. Kaplan–Meier survival curves of all groups were analyzed for the probability of onset of each psychiatric comorbidity, with the age-of-onset as survival time of the affected individuals and age at interview as the time of censor. Hazard ratios, the differences in the probability of developing each psychiatric comorbid disorder between any two groups, were calculated by the Cox proportional hazards regression. To evaluate the influence of ADHD symptoms on each psychiatric comorbid disorder, we performed Cox regression adjusting for ADHD, age and sex. Statistic tests are two-tailed, and a p value <0.05 is considered significant.
Results
Sample characteristics
Table 2 summarizes the sample characteristics. There was no significant difference in sex, intelligent quotient (IQ) and occupation. Adults with ADHD had more ADHD symptoms and were older and more likely to be married than non-ADHD controls. Adults with early-onset ADHD had significantly more hyperactive symptoms than their late-onset counterparts. There was no difference in the proportion of ADHD medication use between the early-onset and late-onset ADHD groups.
Demographics and ADHD symptoms.
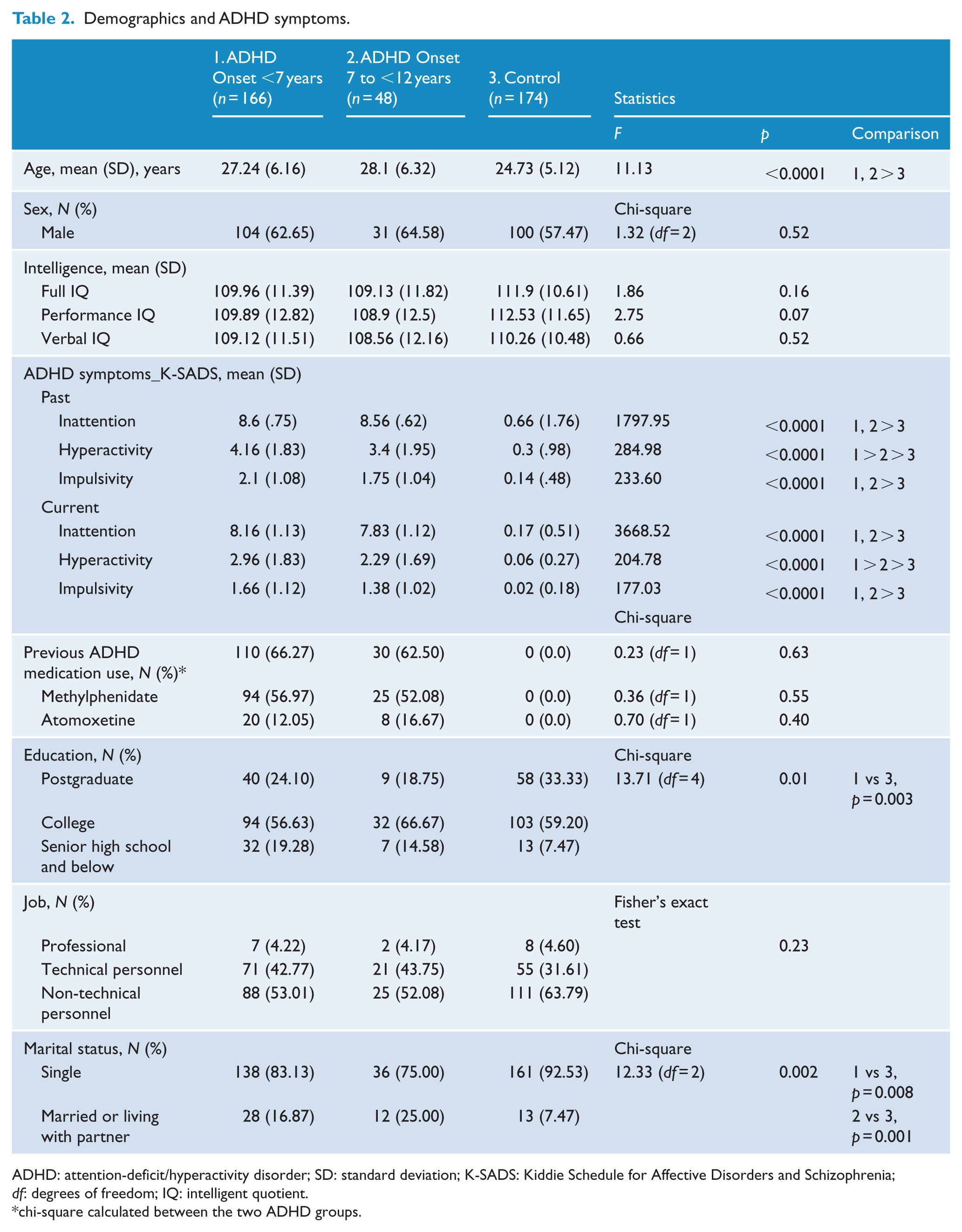
ADHD: attention-deficit/hyperactivity disorder; SD: standard deviation; K-SADS: Kiddie Schedule for Affective Disorders and Schizophrenia; df: degrees of freedom; IQ: intelligent quotient.
chi-square calculated between the two ADHD groups.
Risks of psychiatric comorbidities
The rates for lifetime psychiatric comorbidity of the early-onset ADHD, late-onset ADHD and non-ADHD groups were 50.0%, 50.0% and 4.0% for ODD; 34.9%, 31.3% and 4.0% for CD; 7.8%, 4.2% and 1.7% for tic disorder; 38.6%, 37.5% and 2.3% for mood disorders; 39.2%, 45.8% and 3.5% for anxiety disorders; 4.8%, 2.6% and 0.6% for obsessive–compulsive disorder (OCD); 21.7%, 14.6% and 0.6% for substance use disorder; and 38.6%, 33.3% and 1.2% for sleep disorders, respectively (Supplementary Table 1). Cox regression models revealed that adults with ADHD were more likely than controls to develop CD, ODD, mood disorders (particularly major depression), anxiety disorders (particularly specific phobia), substance (particularly nicotine) use disorders and sleep disorders (Supplementary Table 2). There was no difference of time-dependent risks between the two ADHD groups (Figure 1) in the simple and multiple analyses that adjusted for age and sex (for details, see Supplementary Table 2).
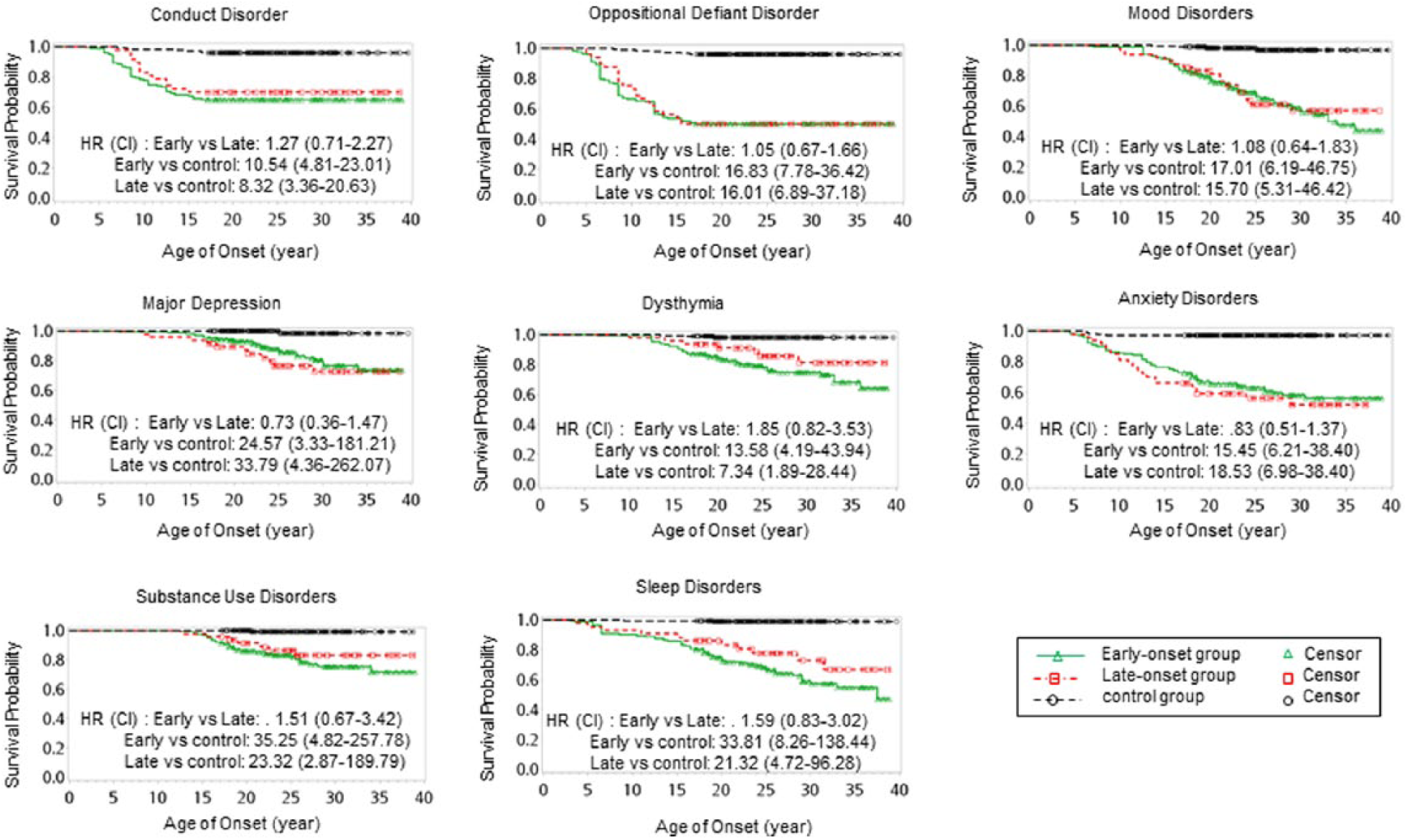
Kaplan–Meier curve of psychiatric comorbidity by groups.
After adjusting for age and sex, ADHD-related increases in the risks of dysthymia and ODD could be explained by inattention symptoms and CD and ODD by hyperactivity/impulsivity symptoms. ADHD diagnosis had significant effects on the risk of major depression, which had no linear correlation with ADHD symptoms. On the other hand, the effect of ADHD diagnosis on the risk of anxiety disorder was largely shared with inattention symptoms (Table 3). Among the two ADHD groups, the mean age of onset (standard error [SE]) was 6.2 (1.6) years for ADHD, 9.1 (3.4) years for ODD, 9.4 (3.1) years for CD, 13.3 (6.4) years for any anxiety disorder, 19 (6.6) years for dysthymia and 20.9 (6.2) years for major depression.
Cox regression estimates of DSM-5 ADHD and previous ADHD symptoms on lifetime psychiatric comorbidities.
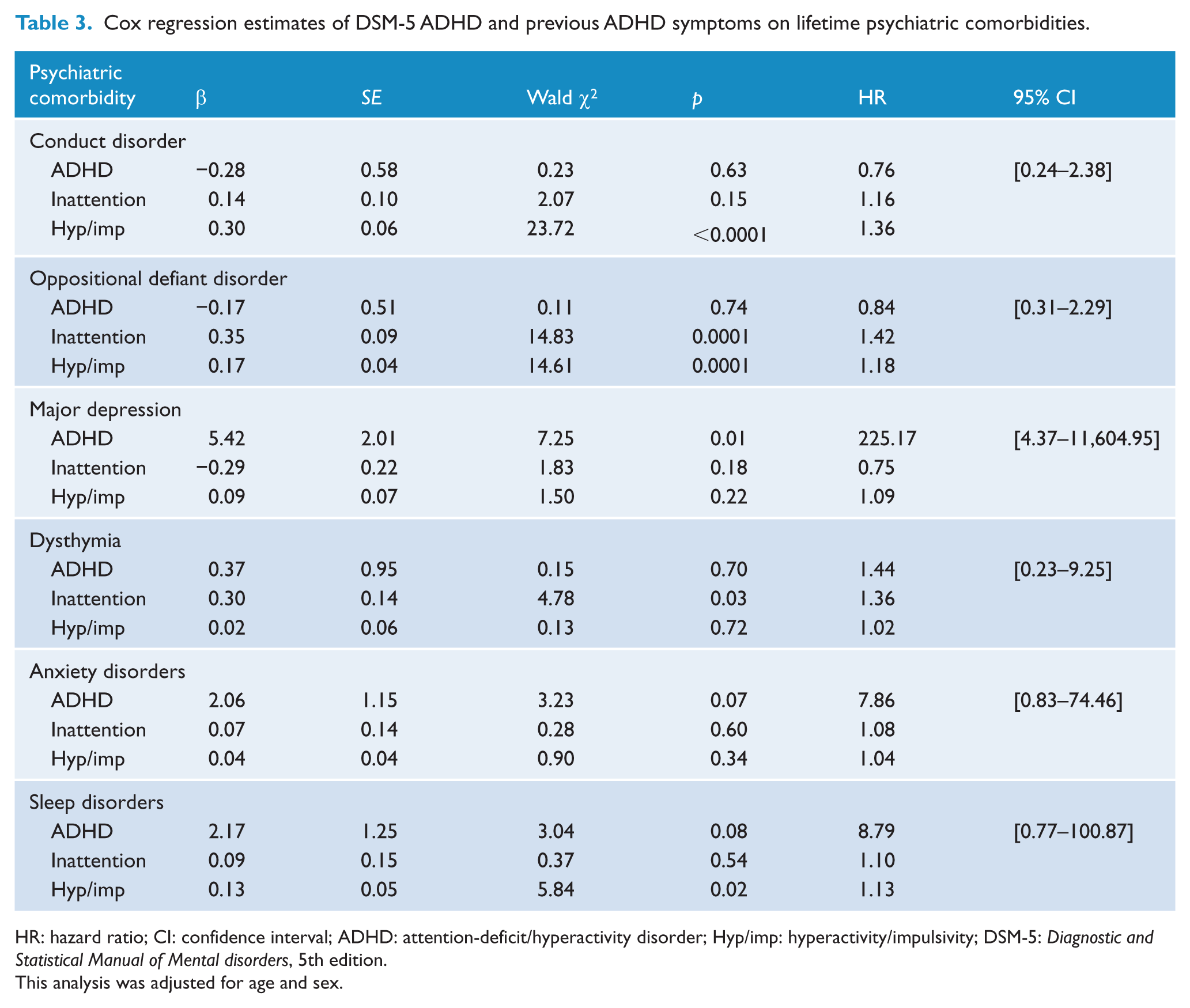
HR: hazard ratio; CI: confidence interval; ADHD: attention-deficit/hyperactivity disorder; Hyp/imp: hyperactivity/impulsivity; DSM-5: Diagnostic and Statistical Manual of Mental disorders, 5th edition.
This analysis was adjusted for age and sex.
Discussion
The main finding of this study was that adults with ADHD, regardless of the recalled age of onset, had significantly higher risks of developing psychiatric comorbidities than controls. Using DSM-5 criteria, we found that in adults with ADHD, previous ADHD symptoms were associated with increased risks of ODD, CD, dysthymia and sleep disorder but not major depression. The finding that similar risks of developing lifetime psychiatric comorbidity between early-onset and late-onset ADHD in this study supports the new DSM-5 change in the AOC (Faraone et al., 2006b; Hesslinger et al., 2003).
In this study, adults with early-onset ADHD had more symptoms of hyperactivity than adults with late-onset ADHD, echoing the findings that the externalizing behavior is more likely to be identified and recalled at earlier age and inattention tends to be neglected and be noticed during later age when the individual faces increasing academic and life demands (Applegate et al., 1997; Vande Voort et al., 2014; Willoughby et al., 2000). Extension of the AOC helps identify this population that might be overlooked if the diagnosis is based on the DSM-IV criteria (Ramtekkar et al., 2010).
We found that there were comparable age-corrected risks of developing CD and ODD between early- and late-onset ADHD groups, despite more hyperactivity symptoms reported by adults with early-onset than late-onset ADHD and the positive correlation between hyperactivity and the risk of CD/ODD in our study. It is possible that the positive effect of hyperactivity symptoms on the risks of ODD/CD was mainly contributed by the early-onset group because of the sample size disparity between these two groups, or adults with late-onset ADHD under-reported hyperactivity symptoms, or there are different pathways from ADHD to ODD/CD in the early- and late-onset groups. Longitudinal studies are warranted to answer this question.
A recent longitudinal prospective community study further identifies a population of adult-onset ADHD which is etiologically different from child-onset ADHD, and most of the adults with child-onset ADHD no longer meet the diagnostic criteria despite having mild impairment associated with ADHD symptoms (Moffitt et al., 2015). That study does not report the age-of-onset of adult-onset ADHD symptoms and other psychiatric disorders, such as substance disorders, at the age of 38 years and thus cannot rule out the possibility that adult-onset ADHD symptoms are residuals of other psychiatric disorders. Adults with late-onset ADHD in our study on average recalled their ADHD onset earlier than other psychiatric disorders for years, compatible with the developmental course of comorbidities in early-onset or DSM-IV ADHD (Taurines et al., 2010). Therefore, despite the basis of the recalled material, the new-recruited ADHD in our sample is more likely to be the continuation of childhood ADHD, or the persistent ADHD, rather than adult-onset ADHD. Because some of the mild, short and non-recurrent episodes of disorders might be under-reported in the retrospective study (Simon and VonKorff, 1995) and there is a tendency for adults to under-report their childhood ADHD symptoms (Barkley et al., 2002; Moffitt et al., 2015), the severity of ADHD symptoms of our clinical ADHD sample might be higher than that of Moffitt’s community childhood ADHD sample, which could also explain for the low persistence rate of their childhood ADHD (Moffitt et al., 2015). Similarly, probably due to under-report, the risk of psychiatric comorbidity of our study, compared to some clinical longitudinal studies (Biederman et al., 2012), was relatively low.
Previous studies have also shown that the dating of symptoms was frequently unreliable (Angold et al., 1996) and unstable (Green et al., 1991). Although in a cohort sample, which was followed from young adolescence to adulthood, there was a high agreement between childhood symptoms collected at two time points (6–8 years apart) either from the participants or their parents, the possibility of under-report of symptoms and inaccurate recall of age of onset still exists. Despite the possibility that some who reported symptom onset between 7 and 12 years might actually have had symptoms prior to 7 years, our study still validates that newly diagnosed adult ADHD with ‘recalled’ age onset between 7 and 12 years has similar psychiatric comorbid patterns and risks as those with ‘recalled’ and actual onset before 7 years and thus supports the utility of the DSM-5 AOC in diagnosing the fresh adult cases who have to report the age of onset by recall.
The symptom severity during childhood or the diagnosis of ADHD is more determining than the recalled age-of-onset of ADHD in the psychiatric outcomes of the affected adults. The risks of CD, ODD, dysthymia and sleep disorders were associated with ADHD symptom severity independent of ADHD status, yet the diagnosis of ADHD would carry the risk of major depression independent of symptom severity. A previous study had shown that the persistence of depression was not predicted by the severity of ADHD (Biederman et al., 1998), thus ADHD symptoms might not have the linear effect on the development and maintenance of major depression. The development of the comorbid conditions among youths with ADHD might represent a more severe psychopathology and thus warrants clinical interventions extending to adults with ADHD to offset further adverse social and psychiatric outcomes (Jerrell et al., 2014).
There are some limitations in our study. First, the clinic- and community-based participants were recruited in a hospital in northern Taiwan, thus the results might not be generalized to other geographic area in Taiwan. Second, the intelligence was relatively high in our sample and could not be generalized to the population of lower intelligence. The enrolling criterion of IQ >80 in our study would partly lead to this result. Third, this study might suffer from recall bias. The accurate age of onset of ADHD and other psychiatric comorbidity might be questionable. Longitudinal follow-up studies will be helpful to validate our findings. Fourth, the prevalence of substance use disorder in our study is significantly lower than other studies (Biederman et al., 1993), which reflected the self-selection bias in our sample and relatively low rate of substance use disorder in Taiwan (Gau et al., 2005, 2007). Younger average age and higher education level of non-ADHD controls further suggest a self-selection bias that these healthy controls might have concerns about their health status and thus are more willing to have mental examinations and brain imaging study for free, leading to the low lifetime risk of substance use disorder. Fifth, it is hard to evaluate the treatment effect for the follow-up subsample in the development of psychiatric comorbidity.
Conclusion
Despite above-mentioned limitations, our study provides further evidence to support the validation of DSM-5 ADHD AOC by demonstrating similar risks of developing psychiatric comorbid disorders in ADHD regardless of the age of onset. In our study, an increase in ADHD symptoms leads to increased risks in ODD, CD, dysthymia and sleep disorders, while the diagnosis of ADHD contributes to the risk of major depression. Both dimensional and categorical approaches to evaluate the risks for developing psychiatric disorders in ADHD have significant clinical relevance.
Footnotes
Acknowledgements
We would like to express our thanks to Ms Yu-Lun Lin for data management and psychiatric interviews, Ms Tiffany (Ting-Fong) Liu for editing the English and all of the participants for their time and effort.
Declaration of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the National Health Research Institute (NHRI-EX100-10008PI, NHRI-EX101-10008PI, NHRI-EX102-10008PI and NHRI-EX102-10008PI), Taiwan.