
Abstract

Introduction
Alcohol continues to be the western world’s favourite recreational drug, use of which induces a compelling state of anxiolytic euphoria for several hours in most people.
Overuse of alcohol is associated with a range of negative health and social consequences. These consequences relate to both the highly intoxicating and aggressogenic nature of alcohol in the short-term (Parrott and Zeichner, 2002), and toxicity from chronic overuse, with about half of alcohol deaths due to acute effects and the other half chronic illness (Connor et al., 2005), including cancers, which account for at least 25% of all alcohol-related deaths.
Alcoholism has been the most commonly used term to describe the behavioural pattern of alcohol overuse in clinical practice. We use the term ‘alcoholism’ here to encompass the series of changes in formal diagnostic systems over the past 60 years since the publication of the Diagnostic and Statistical Manual of Mental Disorders, First Edition (DSM-I) in 1952. From DSM-I to DSM-IV there have been two main shifts in diagnostic conception of alcoholism (Sellman, 1994); DSM-5 represents a third, which is a return to the 1960s unitary formulation of alcoholism (Figure 1).
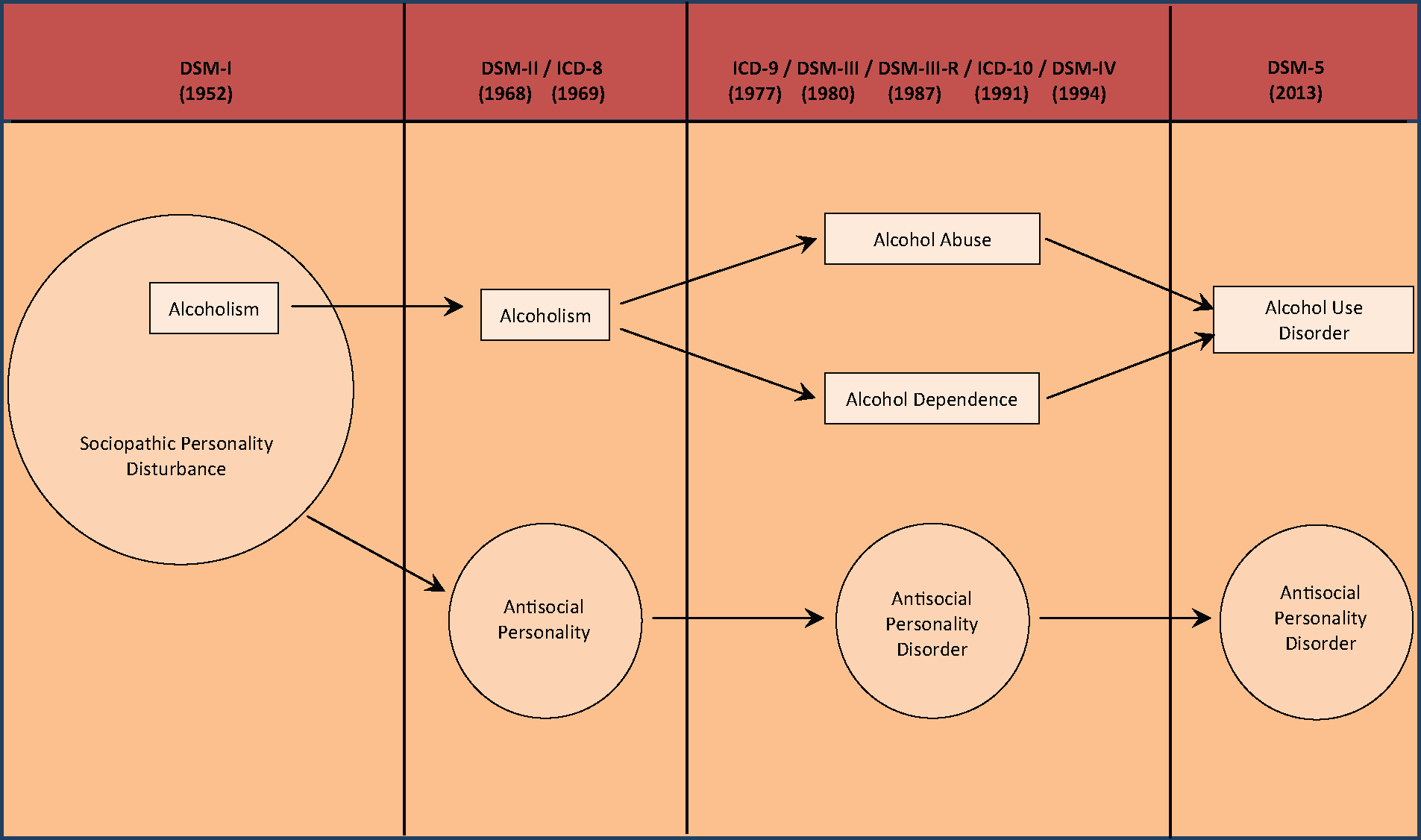
Shifts in the diagnosis of alcoholism over the past 60 years.
The birth of alcoholism
In the 1952 DSM-I (American Psychiatric Association (APA), 1952), alcoholism was conceptualised as a subset of sociopathic personality disturbance, so for the next 15 years, up until DSM-II (APA, 1968), people with alcoholism were considered to be personality disordered. However, during that time the pre-eminent EM Jellinek published The Disease Concept of Alcoholism (Jellinek, 1960). This highly influential book was undoubtedly instrumental in the development of alcoholism as a disorder in its own right in DSM-II, separate from antisocial personality.
The International Classification of Diseases, 8th Revision (ICD-8) was published a year later (World Health Organization (WHO), 1969) and contained, by transatlantic agreement, the same overuse description as DSM-II: ‘an alcohol intake which is great enough to damage … physical health, or … personal or social functioning, or when it has become a prerequisite to normal functioning’.
Alcoholism in the 1960s, therefore, was conceptualised broadly as a behavioural disorder across a punctuated continuum of heavy drinking, from intermittent through to increasingly compulsive use.
Alcoholism divided
The next shift in the diagnosis of alcoholism was strongly influenced by a description of alcohol dependence syndrome in 1976 (Edwards and Gross, 1976) reflected in the diagnostic description in the European-based ICD-9 in 1977 (WHO, 1977). In order to accommodate a dependence syndrome, alcoholism was divided into two separate alcohol use disorders: alcohol dependence and harmful alcohol use. Alcohol dependence was focused around the key symptom ‘compulsion to use’, with the implication that in harmful alcohol use there remained a relative degree of behavioural flexibility albeit within a behavioural pattern of use associated with alcohol-related problems.
The same division of alcoholism into two new disorders occurred in the American DSM-III published in 1980 (APA, 1980), with alcohol dependence being the principal alcohol use diagnosis and harmful use replaced by the pejorative sounding term alcohol abuse. But the Edwards and Gross description of alcohol dependence syndrome was ignored. In its place was the use of ‘multiple problems in multiple areas’ (as a result of excessive alcohol use) as the central idea in both diagnoses, only differentiated by the additional presence of either acquired tolerance or withdrawal in alcohol dependence. However, within 10 years DSM-III-R (APA, 1987) yielded to the WHO’s ICD-9 description of alcohol dependence, based on the Edwards and Gross formulation of the alcohol dependence syndrome. An international consensus had then been forged, on both a dual alcohol use disorder diagnostic system as well as essential similarity in the description of alcohol dependence, a consensus which was to be continued into ICD-10 in 1991 (WHO, 1991) and DSM-IV in 1994 (APA, 1994).
DSM-IV criteria for alcohol dependence and alcohol abuse have been the leading descriptions for both clinical and research purposes for the past 20 years in Australasia as well as internationally. Alcohol dependence has been the dominant disorder, so that patients could progress from abuse to dependence, but the reverse could not, by definition, occur.
Unification of two alcohol use disorders into a new alcoholism
It is now 36 years since alcoholism was divided in the ICD-9 into two separate alcohol use disorders: abuse and dependence. DSM-5 (APA, 2013) now collapses these two disorders back into a single alcoholism diagnosis, formally called alcohol use disorder – a return to the 1960s unitary diagnosis. This has occurred as a result of three decades of international research which in the end has not confirmed a dichotomy in the behavioural pattern of pathological overuse of alcohol, but rather supports a continuum.
Saha and colleagues (2006) have outlined a history of increasingly sophisticated statistical research on the issue of whether there are distinct subtypes of alcoholism. They describe a variety of methods utilised, including cluster analysis, latent class analysis and factor analysis, each technique associated with limitations and, overall, producing a mixed set of findings. They then describe the first large-scale study (n=22,526) of the combined DSM-IV criteria for alcohol dependence and abuse using item response theory. They found that apart from the abuse criterion of presence of legal problems, the remaining 10 abuse and dependence criteria formed a continuum of severity. Hasin and Beseler (2009) then reported another large-scale study (n=27,324) utilising a ‘discontinuity approach’, which has the advantage of exploring the association between a set of criteria and established risk factors for the disorder in question. With the development of DSM-5 specifically in mind, they confirmed the lack of discontinuity between alcohol abuse and dependence when the DSM-IV criteria for each were carefully examined.
Alcohol use disorder is one disorder again, now defined by 11 criteria. The term ‘dependence’ has been discarded, while all the dependence criteria have been retained. ‘Craving’, as a new criterion, more aligned with addiction than dependence, has been revived, while ‘legal problems’ has been omitted. Alcohol use disorder, the new alcoholism, covers a wide spectrum of misuse again as it did previously in the 1960s.
Although the term addiction is referred to in the title to the overall Section in which the new alcoholism is described, addiction has not been used as a formal diagnostic term in the DSM-5, which allows the diagnostic net to cover lower levels of compulsion – the ‘apprenticeship phase’ of addiction development.
The mean time gap between each of the five versions of the APA’s Diagnostic and Statistical Manual of Mental Disorders has been close to 15 years. DSM-5 alcohol use disorder can be expected to be in circulation and influencing international clinical practice and research until close to 2030. What are the clinical implications?
New era
One of the most positive implications flowing from the DSM-5 changes is the fresh stimulus they may give clinicians to undertake enthusiastic assessment of all patients’ alcohol misuse.
In the past, there has been confusion at times in the minds of clinicians, particularly in non-addiction settings, about the difference between abuse and dependence – leading to some avoiding making alcohol use diagnoses altogether. Perhaps it has also been possible for ambivalent clinicians to dismiss alcohol problems in their patients on the basis of a cursory formulation that the alcohol misuse is ‘just abuse’. Ridding the diagnostic system of the judgemental term ‘abuse’ is also likely to facilitate a more mainstream health perspective of this area of psychiatry in contrast to a moral approach to the clinical consideration of psychoactive substance use.
DSM-5 encourages clinicians to think of alcoholism along a continuum of severity, so that rather than simply concentrating on whether a person meets criteria for making a diagnosis there is encouragement to consider the degree to which a person meets the criteria for alcoholism. This will likely facilitate more comprehensive longitudinal assessments of people’s alcohol misuse beginning with questions such as: ‘How old were you when you were first intoxicated with alcohol?’; ‘When did you get into a pattern of drinking alcohol?’; and ‘When has been the heaviest period of alcohol use in your life so far?’. Determination of lifetime severity will be on the basis of how many of the 11 criteria are met in this heaviest period (mild: 2+, moderate: 4+, severe: 6+).
By including the new criterion ‘craving’, DSM-5 moves the overall concept of alcoholism towards the central feature of compulsion to use in line with the last two decades of neurophysiological research (Hyman and Malenka, 2001).
Remembering 11 diagnostic criteria
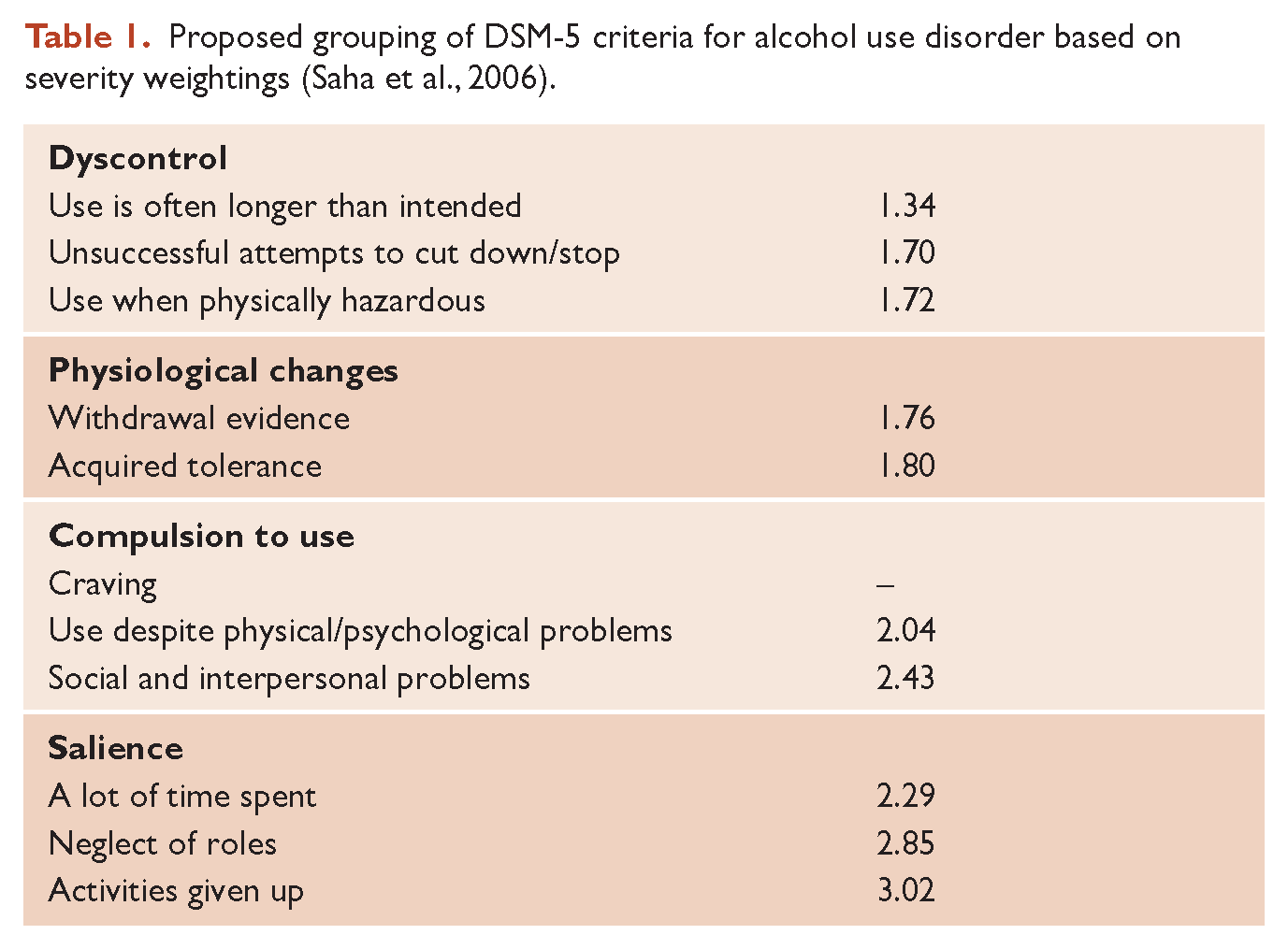
Remembering 11 criteria is a challenge, although DSM-5 has suggested a clumping into four groupings: impaired control, social impairment, risky use, and pharmacological. There is no research quoted that supports these particular groups, so alternatives based on data are likely to be proposed.
The Saha et al. (2006) study above used item response theory to yield severity estimates for each of the DSM-5 criteria (apart from the new criterion – craving). These estimates can be used to clump criteria according to level of severity, forming a progressive pattern, as can be seen in Table 1.
Proposed grouping of DSM-5 criteria for alcohol use disorder based on severity weightings (Saha et al., 2006).
Abstinence advice in the light of the new alcoholism
One of the fundamental challenges of working with people with alcohol use problems is providing good advice, when asked, about abstinence. The old chestnut debate of abstinence versus controlled drinking of the 1970s and 1980s was resolved in the hallmark 1995 work of Sobell and Sobell (1995) whereby recovery from severe alcohol dependence is associated with abstinence in contrast to recovery from less severe dependence through controlled drinking. Severe dependence was never specifically defined, which may have tempted some clinicians to consider the apparent space between the two alcohol use disorders – dependence and abuse – to be the right place to heed Plato’s advice to ‘carve nature at its joints’, although this was not made explicit in the DSM-IV. The fact that a body of research has indicated a radically different treatment goal for what is now being considered, once again, a single disorder, suggests there is progression of the disorder across a threshold as it becomes more severe.
In real-life practice, there has never been clear, unequivocal space between dependence and abuse. The issue of when abstinence is the appropriate therapeutic advice to give, when requested, has continued to challenge clinicians working across the continuum of alcohol problems. This has been particularly so in the area of mild–moderate alcohol dependence, where the diagnostic threshold for DSM-IV alcohol dependence has been relatively low at three of the seven criteria.
Although findings have been somewhat mixed, when those who achieve good outcomes following treatment are divided into abstainers and moderate drinkers, the severity of dependence is usually found to be significantly higher in the former (Rosenberg, 1993). The level of severity at which lifelong abstinence becomes the appropriate advice remains unclear.
One pragmatic solution has been to divide dependence into mild and moderate–severe (based on the DSM-III-R formulation of severity) and include mild dependence with alcohol abuse and hazardous (below diagnostic threshold) drinking as representing the Sobell and Sobell ‘mild’ alcohol problem group, from which people usually recover through controlled drinking. This identifies ‘moderate–severe’ dependence as theoretically indicative of more severe addiction to alcohol and from which people usually recover through abstinence.
But clinical practice often throws up contrary cases: people with alcohol abuse who become abstinent from alcohol long-term following a significant alcohol-related event such as serious injury; people with mild–moderate alcohol dependence who become abstinent for a variable number of months before returning to successful controlled drinking; and (of course) people with severe alcohol dependence who devise ingenious ways of drinking from time to time (controlled relapses) – for example, using disulfiram intermittently.
Clearly, further research is required to establish new methods for determining individuals’ capacity for controlled drinking, including perhaps new neurophysiological technologies. In the meantime, and probably even in the presence of such future assessment aids, people with alcoholism will determine their own long-term solutions through a series of personal natural experiments over time, with alcohol treatment workers assisting as therapeutic guides.
With alcoholism now returned to a unitary condition and acknowledged in the DSM-5 as representing a spectrum of severity across a continuum, the oversimplified treatment-goal dichotomy of abstinence versus controlled drinking can now also be collapsed. Abstinence can also be more easily considered on a continuum, individualised and defined by time, rather than being considered just one life-long therapeutic strategy.
A starting point for discussion about abstinence with patients could be the following graded advice (when advice has been solicited), as described in Table 2.
Suggested abstinence advice in relation to severity of alcohol use disorder (DSM-5).
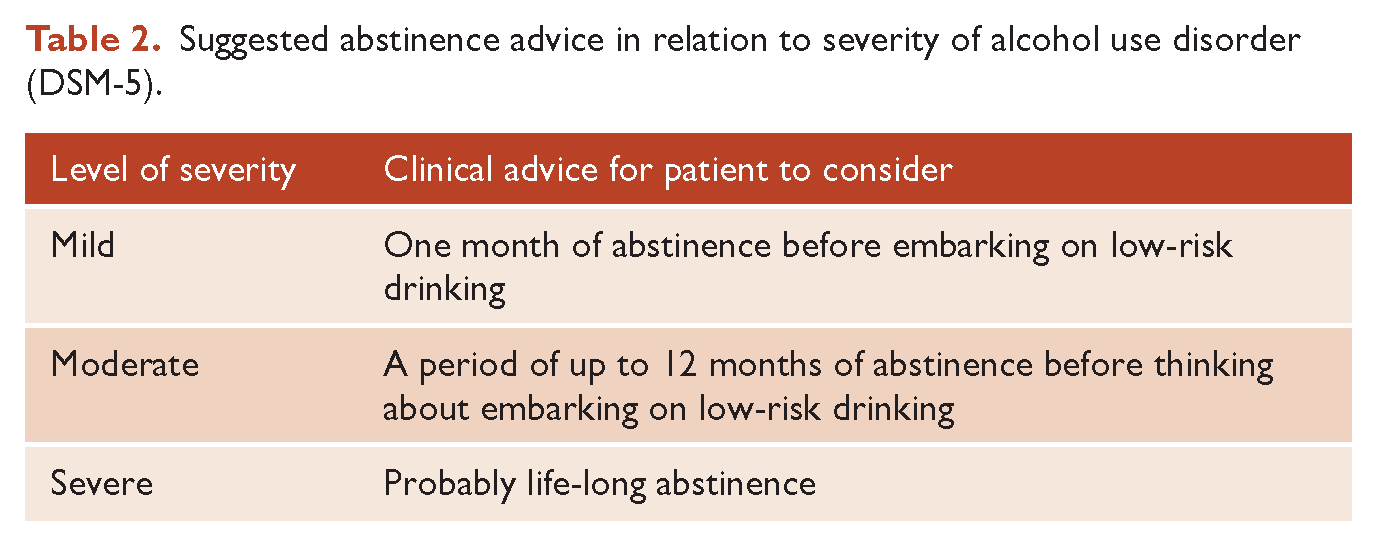
Therapeutic advice for heavy drinkers who do not meet the criteria for alcohol use disorder will probably remain as return to low-risk drinking, without consideration of a short period of abstinence. However, anecdotal reports from popularised public campaigns such as FebFast and Dry July in New Zealand, which encourage a month’s abstinence, and the Australian-initiated Hello Sunday Morning campaign, which advocates for a complete break in alcohol use for 3 months or more, have documented health benefits for non-alcoholic heavy drinkers. The advice for people with moderate alcoholism to possibly abstain for up to 12 months is more unsubstantiated.
The old dichotomous abstinence debate of the 1960s and 1970s is awakened in this DSM-5 era. The scene is set for a new series of well-conducted randomised controlled trials exploring the validity of a continuum of advice across the continuum of alcoholism severity.
Final comments
The DSM-5 formulation of alcoholism sets a new framework for treatment and research of people with alcohol problems, which will be welcomed by those who have long felt sceptical about a dichotomy of alcohol use disorders. However, it can be expected that further research will likely refine the diagnostic criteria for alcoholism. Clearly not all criteria are equal and yet are treated as such in the scoring of individual criteria in DSM-5. There is likely to be some redundancy within the 11 criteria, particularly related to various problems associated with alcohol misuse. We further propose that research is needed to extend our knowledge of the clinical application of the alcohol use disorder criteria, to determine at what level of problem severity varying periods of abstinence, as opposed to controlled drinking, becomes the appropriate treatment goal.
The great limitation in contemporary knowledge – the gap between observable behaviour and brain activity – is evident once again in this new iteration of diagnostic criteria. DSM-5 has been unable to achieve clear consilience between neurophysiological processes that develop in response to ongoing alcohol use and the complexity of human behaviour consequential to those pathological brain developments. It is anticipated that continuing research across this divide will perhaps yield a DSM-6, which achieves this unity of knowledge (Wilson, 1998).
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors declare there is no conflict of interest.