
Abstract
Objective:
Decline in psychosocial functioning seems to be a core feature in schizophrenia across various phases of the disorder. Little is known about the relationship between psychosocial functioning and protective factors or psychopathologies in individuals in the prodrome phase of psychosis. We aimed to investigate whether psychosocial functioning is impaired in individuals in the putative prodromal phase of schizophrenia, and, if so, to identify factors associated with compromised psychosocial functioning.
Method:
Sixty participants at ultra-high risk (UHR) for psychosis and 47 healthy controls were recruited. All subjects were assessed in terms of psychosocial functioning using the Quality of Life Scale. A clinical assessment of psychopathology and protective factors, including resilience and coping style, was also conducted.
Results:
Psychosocial functioning in UHR participants was found to be compromised; this dysfunction was associated with negative symptoms, adaptive coping, and resilience. In addition, baseline resilience was lower among those in the UHR group who converted to frank psychosis than among those who did not.
Conclusions:
These findings imply that treatment strategies for individuals at UHR for psychosis should be comprehensive, promoting resilience as well as targeting the reduction of positive and negative symptoms to foster social reintegration and recovery.
Introduction
Psychosocial functional impairment is a core feature in schizophrenia, including deficits in social and interpersonal function, occupational and role function, and independent living. In fact, it is generally more enduring and devastating than the positive symptoms that define the onset of overt psychotic disorder. This compromised psychosocial functioning is seen in individuals at ultra-high risk (UHR) for psychosis, that is, in the putative prodromal phase (Addington and Addington, 2005; Addington et al., 2008; Mason et al., 2004; Svirskis et al., 2007; Yung et al., 2003, Yung et al., 2004), and also in the first-episode and chronic phases of schizophrenia (Addington and Addington, 2005; Bellack et al., 1990). The extent of social dysfunction in individuals at UHR for psychosis may not differ from that in first-episode or even multi-episode schizophrenia patients (Addington et al., 2008). In addition, social dysfunction may persist over time (Niendam et al., 2007) and it is a potential predictor of overt psychosis onset in UHR individuals (Cannon et al., 2008; Ruhrmann et al., 2008; Yung et al., 2004).
Research on factors associated with impaired psychosocial functioning in patients with chronic schizophrenia (Eack and Newhill, 2007) has extensively reported that schizophrenia’s negative symptoms are key factors influencing psychosocial functioning (Blanchard et al., 1998; Wittorf et al., 2008). Other studies also found positive symptom psychopathologies (MacEwan and Athawes, 1997), depression (Jin et al., 2001), and neurocognition (Sharma and Antonova, 2003) to be associated with social functioning. Similarly, in patients with first-episode schizophrenia, negative symptoms were found to be associated with social dysfunction (Ho et al., 1998; Song et al., 2011; Voges and Addington, 2005).
Therefore, given the persistence and impact on the prognosis of schizophrenia’s underlying social impairment factors, identification of these factors during the prodromal phase is likely to help prevent overt psychosis earlier. Since the prodromal phase of a psychotic disorder is relatively free from chronic secondary morbid processes, including the long-term effects of antipsychotic medication, earlier identification may lead to improvements in the long-term outcome of schizophrenia. Along these lines, several studies have focused on the relationships between social dysfunction and psychopathologies, such as negative (Corcoran et al., 2011) and depressive symptoms (Ruhrmann et al., 2008). Corcoran et al. (2011) reported that in 56 young people at UHR, although both depressive and negative symptoms were related to poor social function, linear regression analysis determined that this association was primarily explained by the effects of negative symptoms, particularly among ethnic minorities (non-white). Meanwhile, Ruhrmann et al. (2008) found that in a German cohort of individuals at early (n = 58) and late (n = 157) initial prodromal states, depression but not negative symptoms consistently explained impaired subjective quality of life.
Recently, protective factors such as coping style, self-esteem, and resilience have been studied for their possible roles in symptom formation, social function, and prognosis in severe mental disorders, such as depression (Dumont and Provost, 1999) and schizophrenia (Harrow and Jobe, 2007; Ho et al., 2010). For example, the results of a 15-year long-term follow-up study (Harrow and Jobe, 2007) of schizophrenia patients suggested that better outcomes were associated with protective factors such as favorable personality and attitudinal approaches and greater resilience. The previously mentioned German cohort study (Ruhrmann et al., 2008) reported that for the 58 subjects in the early initial prodromal stage (defined by the presence of basic symptoms or a reduction in functioning with genetic liability), internal control orientation and positive self-concept emerged as additional predictors of subjective impaired quality of life; unfortunately, related data were not available for the 157 individuals in the late initial prodromal stage, as defined by the presence of attenuated positive symptoms (APS) or brief limited intermittent psychotic symptoms (BLIPS).
Thus, in individuals at UHR, as defined by the presence of APS, BLIPS, or a reduction in functioning with genetic liability, more work is needed to clarify the factors associated with psychosocial functioning, focusing on protective factors as well as psychopathologies. We aimed to investigate whether the psychosocial functioning of help-seeking individuals in the putative prodromal phase of schizophrenia is impaired, and, if so, to identify the factors associated with compromised psychosocial functioning. Based on previous studies (Addington et al., 2008; Corcoran et al., 2011; Ruhrmann et al., 2008), we hypothesized that: (1) individuals at UHR for psychosis show impaired psychosocial functioning compared to healthy controls; and (2) psychosocial functioning is associated with negative symptoms, depressive symptoms and psychosocial protective factors of resilience, and adaptive coping style.
Methods
Participants
The present study was part of the Green Program for Recognition and Prevention of Early Psychosis (GRAPE) project; the details of this project have been described elsewhere (An et al., 2010; Kim et al., 2011a; Kim et al., 2011b; Lee et al., 2011). Sixty participants at UHR were recruited between May 2007 and February 2011 from the Clinic FORYOU (Future of Resilient Youth), a research clinic associated with the GRAPE project at the Severance Hospital and Severance Mental Health Hospital of Yonsei University Health System, Seoul, South Korea. All participants met the inclusion criterion of being between 15 and 35 years of age. Participants were evaluated using the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) (First et al., 2002a; First et al., 2002b).
The healthy control (HC) group consisted of 47 individuals who responded to internet advertisements. We posted our study agenda on the home page of the recruiting site for several days. We screened the volunteers, who were comparable to the UHR subjects with respect to age, sex, and educational level. Individuals were excluded from the HC group if they currently met the criteria for an Axis I disorder, had a history of psychiatric illness, or had a family history of psychotic illness. As a reward, the participants were paid US$20 for their participation. The exclusion criteria for all participants included a current or past neurological illness, traumatic brain injury, or current or past major psychiatric disorder with psychotic features. The UHR group members were diagnosed according to the criteria of the Structured Interview for Prodromal Syndromes (SIPS) (McGlashan et al., 2003). UHR participants presented with one or more of the three prodromal syndromes outlined in the SIPS (McGlashan et al., 2003): (1) BLIPS (n = 11), defined as emerging psychotic symptoms with spontaneous remission within one week; (2) attenuated positive prodromal syndrome (APPS; n = 52), defined as recent attenuated positive psychotic symptoms of sufficient frequency or severity; and (3) genetic risk and deterioration syndrome (n = 4), defined as a combination of genetic risk and recent functional decline. The DSM-IV diagnoses of the UHR group included the following: depression (n = 25), anxiety (n = 10), eating disorders (n = 2), substance (cannabis) abuse (n = 1), impulse control (n = 1), post-traumatic stress (n = 1), somatoform disorder (n = 1), and schizotypal (n = 6), schizoid (n = 1), avoidant (n = 1), and borderline (n = 1) personality disorder.
The present study was carried out in accordance with the Declaration of Helsinki (2008). The Institutional Review Boards at Severance Hospital and Severance Mental Health Hospital approved this study. All participants gave written informed consent. Written informed consent was obtained from all subjects and additionally from the parents if subjects were under 18 years of age.
Measures
Psychosocial functioning status was evaluated using the Heinrichs–Carpenter Quality of Life Scale (QLS) (Heinrichs et al., 1984), a 21-item rater-administered scale (each item was scored 0–6, with higher scores reflecting better functioning). The QLS yields a total score (21 items, range 0–126) and scores for four subscales that address:
interpersonal relationships and social networks (e.g. friends, social activity, and social initiative; 1–8 items, range 0–48);
instrumental role functioning (e.g. work functioning and occupational role; 9–12 items, range 0–24);
intrapsychic foundations (e.g. sense of purpose, motivation, and anhedonia; 13–17, 20, 21 items, range 0–42); and
common objects and activities (COAs, e.g. use of objects and participation in activities; 18–19 items, range 0–12).
The version of the scale translated into Korean is widely used and reported to be a reliable tool for the assessment of objective functional status of patients with schizophrenia (Song et al., 1999; Song et al., 2011). In the current study, the internal consistencies (alpha) of the total score and four subscales scores were each > 0.81 with the exception of COAs (0.66).
Protective factors were assessed in the areas of resilience and coping style. Resilience was measured using the 25-item Connor–Davidson Resilience Scale (CD-RISC) (Connor and Davidson, 2003), in which participants rated items on a 5-point scale (from 0 = not true at all to 4 = true nearly all of the time) according to how much they agreed with each item as it applied to them. Examples of CD-RISC items are:
Able to adapt to change;
Can deal with whatever comes;
When things look hopeless, I don’t give up;
Not easily discouraged by failure;
Make unpopular and difficult decisions; and
Take pride in my achievements.
The total score was created by adding up all responses; they ranged from 0 to 100, with higher scores reflecting greater resilience. The CD-RISC has been shown to have good psychometric properties in Korean psychiatric populations (Baek et al., 2010). The internal consistency (alpha) of the total resilience score was 0.95 in the current study.
Coping styles were measured using the Ways of Coping Questionnaire (WCQ) (Folkman and Lazarus, 1985); this is a 62-item self-report tool that asks subjects to rate how often they have used different coping strategies during their most recent stressful events. The WCQ has several subscales: problem-focused coping, wishful thinking; distancing; seeking social support; emphasizing the positive; self-blame; tension reduction; and self-isolation. The Korean version of the WCQ (Kim, 1987) has been widely used and has yielded two (adaptive active coping and maladaptive passive coping) or four subscales (problem focusing, tension reduction, wishful thinking, and social support seeking). Items regarding adaptive active coping include ‘I knew what had to be done, so I doubled my efforts to make things work’ and ‘I talked to someone to find out more about the situation.’ Items addressing maladaptive passive coping included ‘I went on as if nothing had happened’ and ‘I hoped a miracle would happen.’ For the current study, adaptive and maladaptive coping scores were calculated first, and then relative scores were calculated to control response bias, according to methods used in prior studies (Lysaker et al., 2004; Lysaker et al., 2007). To provide a relative score for adaptive coping, total scores were divided by the mean total score, and a result greater than 1 was considered indicative of a relatively greater reliance on that coping strategy.
The presence of psychopathology was evaluated using the Scale for the Assessment of Negative Symptoms (SANS) (Andreasen, 1984a), the Scale for the Assessment of Positive Symptoms (SAPS) (Andreasen, 1984b), and the Montgomery–Åsberg Depression Rating Scale (MADRS) (Montgomery and Åsberg, 1979) including the criteria of the SIPS (McGlashan et al., 2003). As some of the scales were not available prior to April 2008, some data (CD-RISC: two in the UHR group; WCQ: 16 in the HC group and nine in the UHR group) were not included in the statistical analysis.
Procedures
Clinical interviews and assessments were administered by a psychiatrist within a week following recruitment into the study. Each participant received a packet of questionnaires that included the CD-RISC, QLS, and WCQ.
Statistical analysis
All rating scores had acceptable skewness and kurtosis (< 1.0). Group differences in terms of demographics and clinical characteristics, including protective factors of resilience, relative adaptive coping scores, and psychopathologies were examined using independent t-tests. The total score and four subscores of the QLS were also compared using independent t-tests between the UHR and HC groups. In addition, exploratory non-parametric analysis was conducted for resilience, adaptive coping style, psychopathologies, and QLS total score and subscores at baseline to compare between UHR individuals who converted to frank psychosis and those who did not during the follow-up period (6–36 months). Pearson’s correlation analysis was used to assess the relationships between psychosocial functioning status based on the QLS total score and subscores with resilience, adaptive coping, and prodromal symptoms. A series of hierarchical regression models (on the QLS total subscores) were then used to examine the association of prodromal symptoms by SIPS, depressive symptoms, and protective factors, including resilience and adaptive coping, entered in that order. Additional variations on these models were also run. In light of shared variance and high correlation (r = 0.46, p = < 0.001) between the negative symptoms of SIPS and depressive symptoms, there is an increased probability that a good predictor will be found to be non-significant and rejected from the model. Therefore, an alternate hierarchical regression model was run entering depressive symptoms in the step prior to the prodromal symptoms. Missing data were subjected to listwise deletion in the regression analysis. The same statistical procedure was also conducted in UHR individuals with depression as a comorbid disorder (n = 25). The criterion for significance was set at p < 0.05.
Results
Comparison of demographic and clinical characteristics between the UHR and HC groups
The demographic and clinical characteristics of the groups are summarized in Table 1. There were no significant differences in age, sex, or educational level. The UHR group was significantly less resilient and more reliant on passive coping strategies. As expected, the UHR group showed more depressive, positive, and negative symptoms than the HC group. The majority (35/60) of the UHR group did not take antipsychotic medications. All medicated UHR group members were receiving atypical antipsychotics. There were no significant differences in age (p = 0.720), educational level (p = 0.435), psychopathologies (all p > 0.504), resilience (p = 0.141), and relative adaptive coping strategy (p = 0.885) between the antipsychotic medication group and the non-medicated group.
Clinical and demographic characteristics of the study groups.
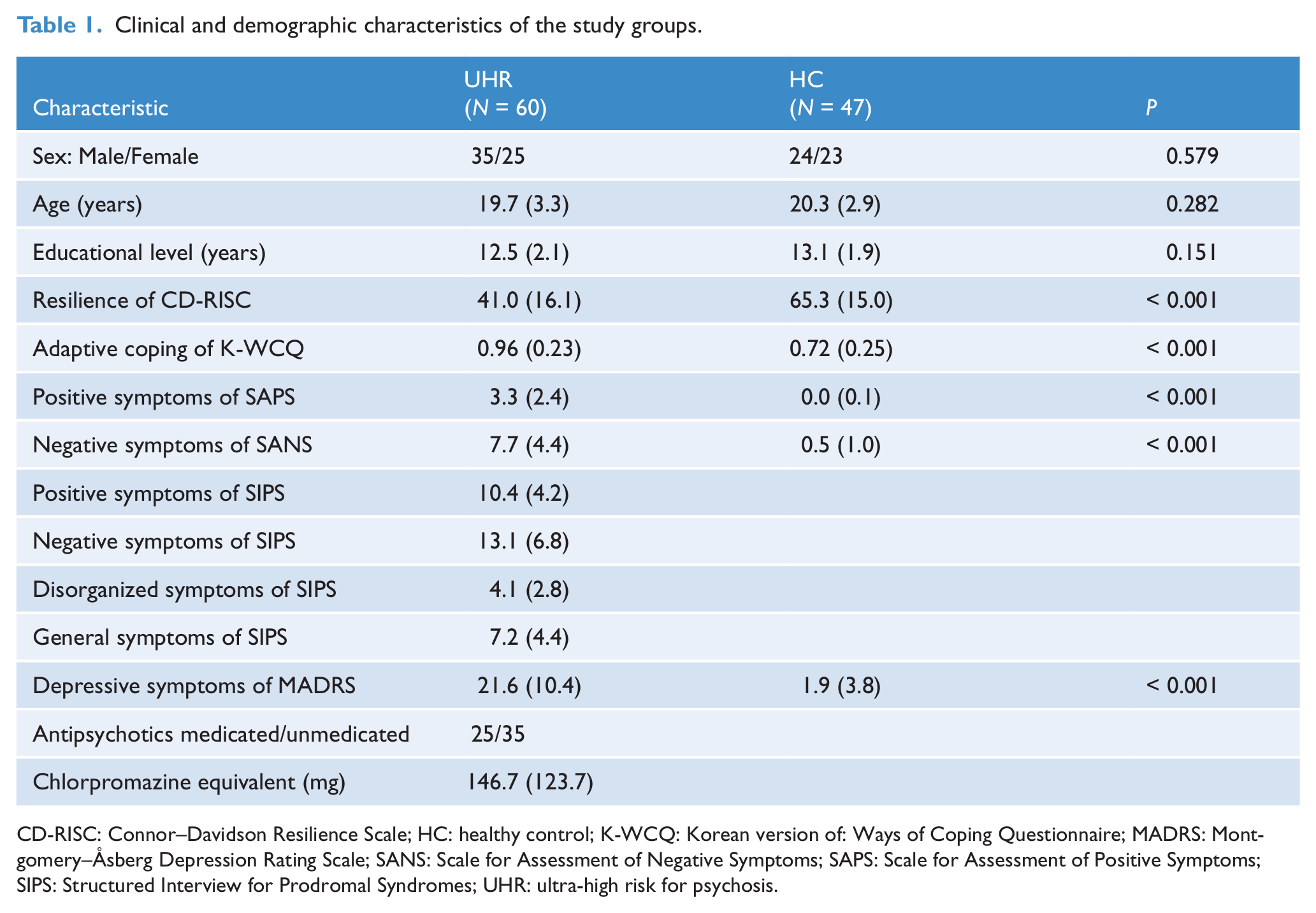
CD-RISC: Connor–Davidson Resilience Scale; HC: healthy control; K-WCQ: Korean version of: Ways of Coping Questionnaire; MADRS: Montgomery–Åsberg Depression Rating Scale; SANS: Scale for Assessment of Negative Symptoms; SAPS: Scale for Assessment of Positive Symptoms; SIPS: Structured Interview for Prodromal Syndromes; UHR: ultra-high risk for psychosis.
Of the 60 individuals in the UHR group, 49 were followed up (6–36 months). Ten UHR individuals developed frank psychotic disorders of schizophrenia (n = 9) or a psychotic manic episode of bipolar I disorder (n = 1) during this follow-up period. The conversion rate was 20.4% (10/49). Exploratory data analysis revealed that the UHR converters (n = 10; 31.0 ± 16.2) were significantly less resilient than the UHR non-converters (n = 39; 44.3 ± 16.1) at baseline (Mann–Whitney U test; z = -2.2, p = 0.029), though there were no other significant differences in baseline scores for psychopathologies (all p > 0.206), relative adaptive coping strategy (p = 0.202), or QLS total score and subscores (all p > 0.142).
Comparison of psychosocial functioning between the UHR and HC groups
The UHR group was found to have the following significant impairments in functioning: total (Cohen’s d = -3.6) and interpersonal (Cohen’s d = -3.5), instrumental role (Cohen’s d = -2.5), intrapsychic foundations (Cohen’s d = -3.2), and use of objects and participation in activities (Cohen’s d = -1.4), relative to the HC group (Table 2). At the time of baseline evaluation, there were no significant effects of sex (all p > 0.367) or antipsychotic medications (all p > 0.288) on the QLS total score or subscores.
Comparison of psychosocial functioning between study groups.
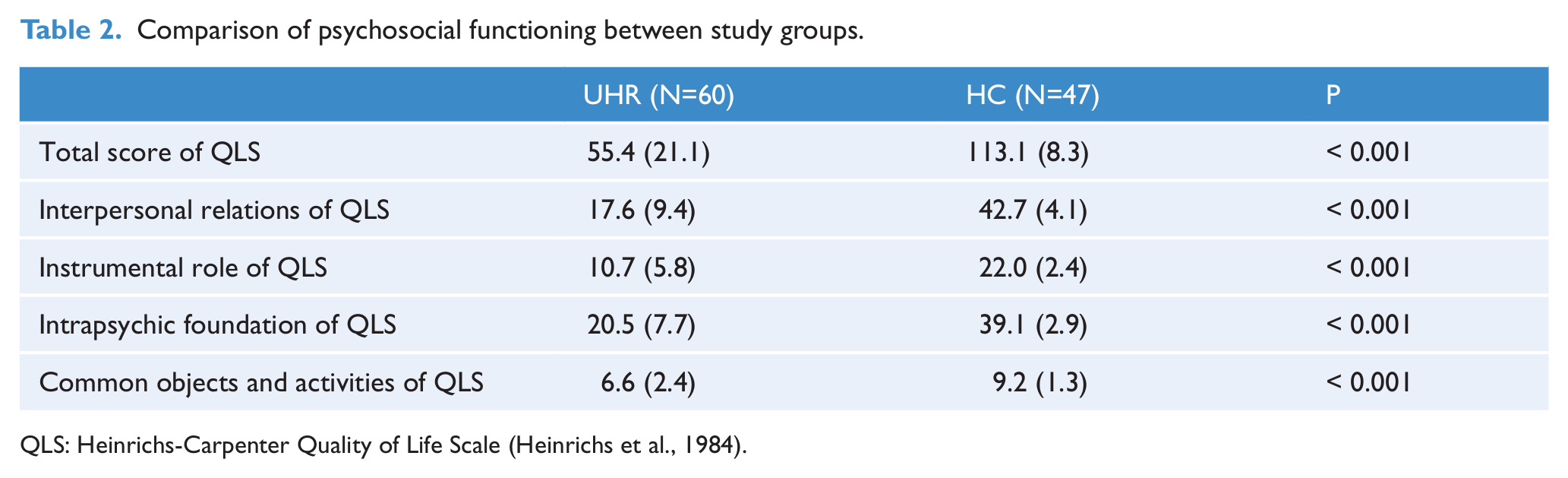
QLS: Heinrichs-Carpenter Quality of Life Scale (Heinrichs et al., 1984).
Association between psychosocial functioning status and resilience, coping strategy, and psychopathologies in the UHR group (based on the QLS total score and four subscores)
The preliminary Pearson’s correlation analysis results are presented in Table 3. The UHR individuals who were more resilient and showed less severe negative and depressive symptoms were found to have better total scores and subscores for interpersonal functioning and intrapsychic foundation. UHR individuals more reliant on adaptive coping strategies were found to have higher intrapsychic foundation and interpersonal relations. Table 4 summarizes the results of the standard hierarchical multiple regression analyses (Model 1).
Correlations of psychosocial functioning, protective factors, and psychopathologies in individuals at ultra-high risk for psychosis (N = 60).
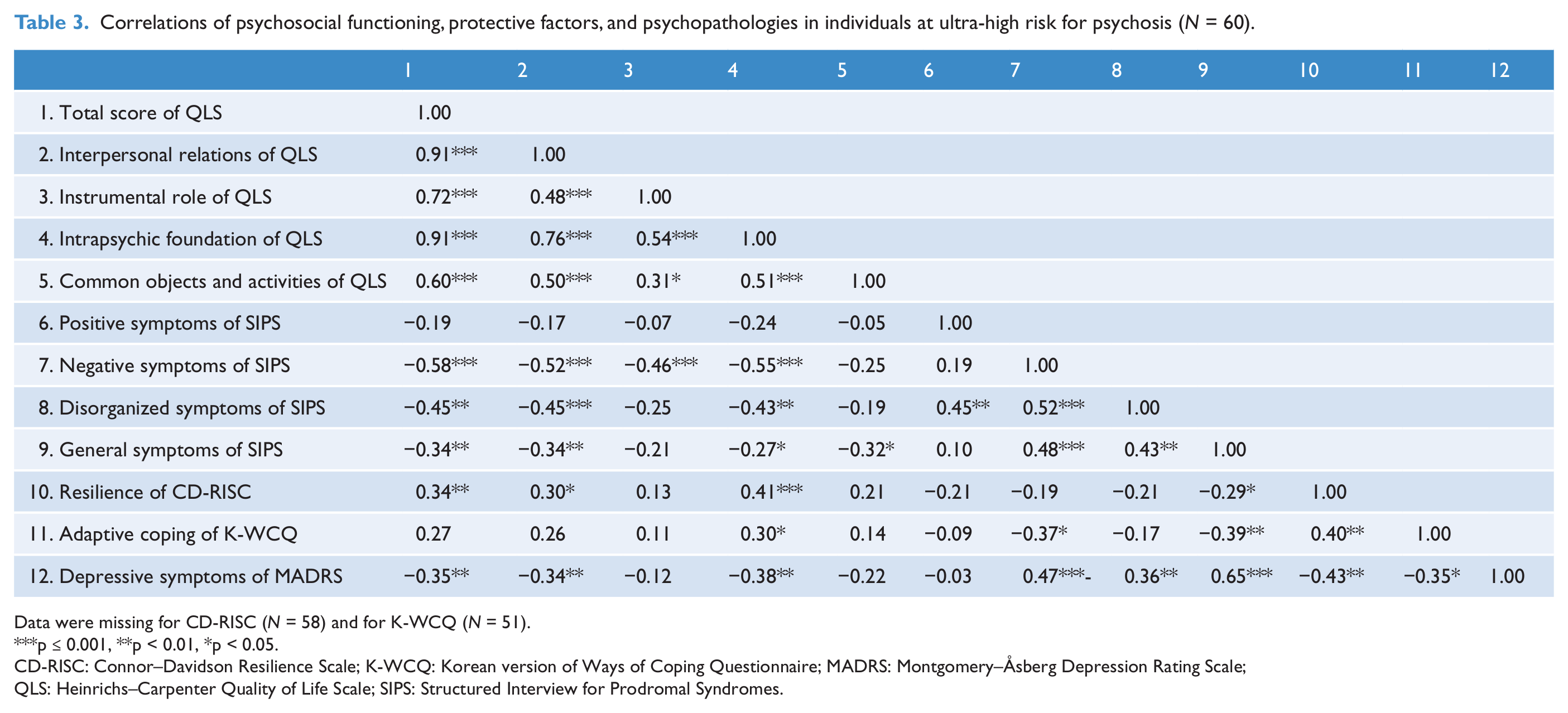
Data were missing for CD-RISC (N = 58) and for K-WCQ (N = 51).
p ≤ 0.001, **p < 0.01, *p < 0.05.
CD-RISC: Connor–Davidson Resilience Scale; K-WCQ: Korean version of Ways of Coping Questionnaire; MADRS:
QLS: Heinrichs–Carpenter Quality of Life Scale; SIPS: Structured Interview for Prodromal Syndromes.
Best weights and R2 for hierarchical regression with psychosocial functioning (QLS) in individuals at ultra-high risk for psychosis (N = 60).
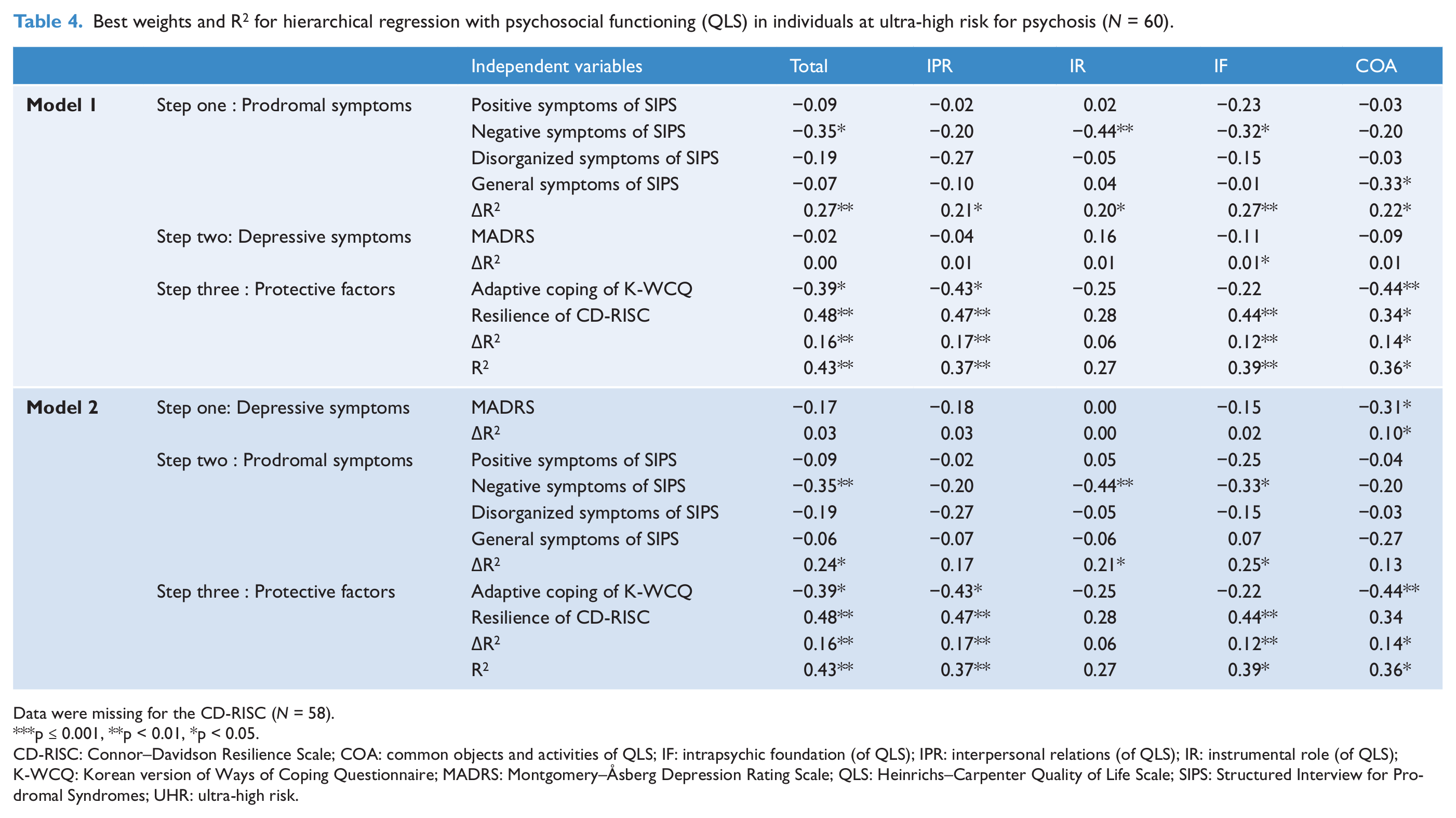
Data were missing for the CD-RISC (N = 58).
p ≤ 0.001, **p < 0.01, *p < 0.05.
CD-RISC: Connor–Davidson Resilience Scale; COA: common objects and activities of QLS; IF: intrapsychic foundation (of QLS); IPR: interpersonal relations (of QLS); IR: instrumental role (of QLS); K-WCQ: Korean version of Ways of Coping Questionnaire; MADRS: Montgomery–Åsberg Depression Rating Scale; QLS: Heinrichs–Carpenter Quality of Life Scale; SIPS: Structured Interview for Prodromal Syndromes; UHR: ultra-high risk.
Regression analysis with the QLS total and subscales scores as the dependent variables revealed that the prodromal negative symptoms of SIPS and resilience scores of CD-RISC, adaptive coping of K-WCQ were significant determinants that explained 43% of the variance of the total QLS score and between 36% and 39% of variance in three of four subscales (Table 3). The prodromal symptoms produced the most substantial increase in explanatory power in the total and subscales scores of the QLS, ranging from 20% to 27%. In particular, the negative symptoms of SIPS were significant and most substantial determinants among prodromal symptoms. Depressive symptoms explained between 0% and 1% of the variation in functioning status, when entered on the second step; it was significant only for intrapsychic foundations. The addition of protective factors of adaptive coping and resilience in step 3 produced a significant and substantial increase in explanatory power in the QLS total score (16%), interpersonal relationship and social networks (17%), intrapsychic foundations (12%), and COAs (14%).
Even in the alternate model, where measures of depressive symptoms were entered ahead of prodromal symptoms (Model 2), the results were not different from model 1. The depressive symptoms contributed only 10% at most of additional variance to the COAs only, which was substantially less variation than prodromal, especially negative symptoms and protective factors.
In UHR individuals with depression as the comorbid condition (N = 25), the preliminary Pearson’s correlation analysis found that there were significant relationships of subscore of interpersonal relation with negative (r = -0.51, p = 0.009) and depressive (r = -0.40, p = 0.008) symptoms. The subscore of intrapsychic foundation also showed a significant relationship with negative (r = -0.55, p = <0.001) and depressive (r = -0.38, p = 0.003) symptoms. However, subsequent hierarchical regression analysis with the interpersonal relation score and intrapsychic foundation score as the dependent variable showed no significant determinant in this subpopulation.
Discussion
The main findings of this study were that 60 young, help-seeking UHR individuals had clear deficits in psychosocial functioning compared to healthy young controls and that the key factors of their social dysfunction were prodromal symptoms, especially negative symptoms, protective factors of adaptive coping and resilience. In addition, baseline resilience was lower among those in the UHR group who converted to frank psychosis than among those who did not. In interpreting the results, it is important to note that this study was cross-sectional, and so it would be incorrect to infer causal relationships. Without longitudinal follow-up data, we cannot confirm that negative symptoms, adaptive coping, and resilience are predictive of psychosocial dysfunction in the short term.
However, UHR individuals were found to have poorer overall QLS scores and also poorer scores on the interpersonal relationships, instrumental role, intrapsychic foundations, and COA subscales. These results are consistent with those of previous studies (Addington and Addington, 2005; Addington et al., 2008; Mason et al., 2004; Svirskis et al., 2007; Yung et al., 2003; Yung et al., 2004) which found overall decreased QLS scores in UHR patients. Our UHR individuals had a somewhat lower QLS score (55.4 ± 21.1) than in previous studies (Mason et al., 2004; Yung et al., 2003; Yung et al., 2004; approximate mean = 72–77), but direct comparison is not possible. Our lower scores may be due to the referral health system in Korea, i.e. to access our research clinic based at a university hospital, most help-seeking individuals were referred from a primary psychiatric clinic near their residence. Thus, it is likely that relatively more distressed, lower functioning individuals at UHR may have been recruited at our research clinic. Examination of the effect sizes of functional impairments revealed that impairments in the use of common objects and the engagement in activities and instrumental role functions were relatively less severe than in the subdomains of interpersonal functioning and intrapsychic foundations, although the total QLS score and scores on all of its subdomains were within the range of considerable impairment in our UHR individuals. These findings suggest that the marked impairment in psychosocial functioning, especially interpersonal functioning and intrapsychic foundations, in individuals at UHR may emerge before the onset of overt psychotic symptoms.
Addressing psychopathologies, standard hierarchical regression analysis indicated that negative symptoms, but not depressive symptoms, were primarily associated with overall psychosocial functioning and interpersonal, intrapsychic, and COA functions. This is consistent with previous reports (Corcoran et al., 2011; Svirskis et al., 2007) that objective psychosocial functioning is associated with negative symptoms but not with objectively assessed depressive symptoms (Corcoran et al., 2011). Our finding of this association of negative symptoms with social dysfunction in UHR individuals is supported by numerous studies finding this association in first-episode schizophrenia patients (Ho et al., 1998; Song et al., 2011; Voges and Addington, 2005).
However, our finding is not compatible with the report by Rurhmann et al. (2008) that subjective quality of life was associated with depression but not with negative symptoms. In that study, psychosocial functioning was assessed using the Modular System for Quality of Life questionnaire (Pukrop et al., 2000), which consists of self-reported scales of quality of life including satisfaction with social function, while depressive symptoms were evaluated by subjective complaints on the Symptom Checklist SCR-90-R (Derogatis et al., 1976). Thus, the inconsistency in findings may arise from the difference in measurement strategies for psychosocial functioning (objective functioning vs. subjective satisfaction with social function) as Corcoran et al. (2011) discussed, or it may arise from the difference in measurement strategies for depressive symptoms (interviewer-rated vs. self-reported scales).
Regarding protective factors, adaptive coping style and resilience were found to be additional independent factors associated with overall psychosocial functioning and interpersonal and intrapsychic foundation function. This finding is in line with previous findings about the early initial prodromal state (Ruhrmann et al., 2008) and schizophrenia (Harrow and Jobe, 2007). For example, one such study (Ruhrmann et al., 2008) found that internal control orientation and having a generalized self-concept of one’s own ability, which are components of the Questionnaire of Competence and Control Orientation (Krampen, 1991), were independently associated with quality of life including subjective satisfaction with social functioning. The previously described long-term (15-year) follow-up study (Harrow and Jobe, 2007) of schizophrenia reported that more favorable outcomes were associated with internal resources of patients including favorable prognostic factors and greater resilience. Thus, among those at UHR, individuals with greater resilience and adaptive coping style seem to show better psychosocial functioning in the early or late initial prodromal state, or with schizophrenia.
More importantly, resilience was found to be significantly lower in UHR converters than in UHR non-converters during the follow-up period (6–36 months) in the current study. Previous reports on psychosocial vulnerability factors indicated that interpersonal stress sensitivity (Krampen, 1991) or perceived hostility bias (An et al., 2010) were noted in individuals at UHR. If these vulnerability-related needs in UHR individuals are not compensated for by protective factors such as resilience, then UHR individuals may be more likely to deteriorate into poor psychosocial functioning and frank psychosis. Therefore, to promote social functioning, psychosocial interventions should be developed to enhance resilience in addition to reducing negative symptoms. The plausible intervention strategy may be some kind of mindfulness-based approach, since this strategy was found to promote resilience as well as to reduce symptom-related distress in patients with severe mental illness (Davis and Kurzban, 2012). In the near future, there is need to test whether a psychosocial program that incorporates the mindfulness-based approach into the existing cognitive therapy for UHR individuals (Kim et al., 2011) could reinforce these protective factors and reduce the distressing symptoms, which might be helpful in preventing the transition to overt psychosis.
Our results should be interpreted in the context of the limitations of our study. As mentioned earlier, a major limitation is the lack of follow-up data to elucidate causal relationships among social functioning, psychopathologies, and protective factors. Long-term follow-up studies are needed to increase our understanding of the unique contribution of these variables to social functioning in UHR individuals. A further limitation was that no information was available on social support, premorbid functioning, neurocognitive function, and sociocognitive function, all of which may be relevant to psychosocial functioning in UHR individuals. In recent research findings, some authors touched on the importance of stress (Pruessner et al., 2011), stress sensitivity (Holtzman et al., 2012), and family factors (Meneghelli et al., 2011), and emphasized their therapeutic implications (Strobl et al., 2012). For long-term follow-up studies, all these factors should be combined to make for integrated and comprehensive results. Finally, in the current study, psychosocial functioning was assessed using the QLS, which measures the deficit symptoms of schizophrenia, a concept that overlaps that of negative symptoms. This may amplify the significance of negative symptoms. However, at the time of recruitment, the QLS was the most widely used scale in UHR studies, and more specific assessment tools such as Functioning: Social (Auther et al., 2006) and Global Functioning: Role (Niendam et al., 2006) were not available in Korean. Despite the limitations, to our knowledge this is the first study to investigate multiple psychosocial functioning measures, and it offers some further understanding of the nature of social deficits that occur in the putative prodromal phase of this illness.
In conclusion, the present study found that psychosocial functioning in individuals at UHR for psychosis is already at a markedly dysfunctional level compared to young healthy individuals, and the key associated factors of this dysfunction may not only be negative symptoms, but also resilience. In addition, resilience may be a potential protective factor preventing psychotic conversion. These findings imply that, for social reintegration and recovery, psychosocial interventions should be comprehensive, considering both negative symptoms and protective factors in treating patients, rather than managing positive symptoms alone.
Footnotes
Funding
This work was supported by a grant of the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare and Family Affairs, Republic of Korea (A090096) and by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MEST) (No. 2010-0026833).
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.