
Abstract
Objectives:
Studies have attempted to identify additional risk factors within the group identified as ‘ultra high risk’ (UHR) for developing psychotic disorders in order to characterise those at highest risk. However, these studies have often neglected clinical symptom types as additional risk factors. We aimed to investigate the relationship between baseline clinical psychotic or psychotic-like symptoms and the subsequent transition to a psychotic disorder in a UHR sample.
Method:
A retrospective ‘case–control’ methodology was used. We identified all individuals from a UHR clinic who had subsequently developed a psychotic disorder (cases) and compared these to a random sample of individuals from the clinic who did not become psychotic within the sampling time frame (controls). The sample consisted of 120 patients (60 cases, 60 controls). An audit tool was used to identify clinical symptoms reported at entry to the clinic (baseline) using the clinical file. Diagnosis at transition was assessed using the Operational Criteria for Psychotic Illness (OPCRIT) computer program. The relationship between transition to a psychotic disorder and baseline symptoms was explored using survival analysis.
Results:
Presence of thought disorder, any delusions and elevated mood significantly predicted transition to a psychotic disorder. When other symptoms were adjusted for, only the presence of elevated mood significantly predicted subsequent transition (hazard ratio 2.69, p = 0.002). Thought disorder was a predictor of transition to a schizophrenia-like psychotic disorder (hazard ratio 3.69, p = 0.008).
Conclusions:
Few individual clinical symptoms appear to be predictive of transition to a psychotic disorder in the UHR group. Clinicians should be cautious about the use of clinical profile alone in such individuals when determining who is at highest risk.
Introduction
It has long been known that psychotic disorders have a prodromal period prior to the onset of the frank disorder (Chapman, 1966; Conrad, 1958; Kraepelin, 1921). In the mid-1990s, researchers began investigating the possibility of identifying this ‘prodromal’ period prospectively, with the aim to intervene earlier in the course of these disorders (Phillips et al., 1999). This research was informed by retrospective descriptive studies of the schizophrenia prodrome, which reported a range of ‘attenuated’ or low-intensity/frequency positive psychotic symptoms occurring prior to the onset of a psychotic disorder (Chapman, 1966; Yung and McGorry, 1996a, 1996b). Clinical criteria, such as the ‘ultra high-risk’ (UHR) criteria, were developed in Melbourne to identify a help-seeking population at substantially elevated risk of developing psychosis in the near future (Bell, 1992; Yung et al., 2003). This clinically defined population was initially found to have a rate of ‘transition’ to a frank psychotic disorder of around 40% in the first 12 months after presentation (Phillips et al., 2000; Yung et al., 2003). The number of clinical services providing care to individuals meeting UHR criteria has expanded worldwide. There have been a number of randomised trials of indicated prevention strategies in this population, despite ethical concerns and questions regarding the validity of the criteria (Rosen, 2000; Yung, 2011; Yung and McGorry, 1997).
Despite the promising initial predictive validity of these criteria, the rates of ‘false positives’ and the more recent suggestion of lower transition rates in more established clinics (Yung et al., 2007) have prompted researchers to investigate the utility of additional clinical predictors within this group to further identify those at highest risk. This approach has proved somewhat encouraging. Initially, our group in Melbourne found that a combination of attenuated psychotic symptoms and genetic risk; a long duration of symptoms prior to presentation; poor social functioning as measured by the Global Assessment of Functioning (GAF) (American Psychiatric Association, 1994); and poor attention as measured by the subscale of the Scale for Assessment of Negative Symptoms (SANS) (Andreasen, 1983) substantially improved prediction above UHR criteria (Yung et al., 2004). Other prospective studies have also reported that a number of clinical predictor variables improved the predictive validity of the transition to psychosis in this population (Cannon et al., 2008; Ruhrmann et al., 2010). Indeed, there is some consistency in the results of these studies with variables, including low baseline functioning and ‘unusual thought content’, replicated in independent samples (Thompson et al., 2011).
Most of these larger prediction studies have used research assistants to assess participants using standardised research tools such as the Brief Psychiatric Rating Scale (BPRS) and, latterly, specific assessment tools developed for this population (Comprehensive Assessment of At Risk Mental States (CAARMS) (Yung et al., 2005) and Structured Interview for Prodromal Symptoms (SIPS) (Miller et al., 2003)), which provide overview scores of symptom domains. This is in contrast to the original research approach that retrospectively focused on individual symptom types; for example, suspiciousness and thought blocking (Yung and McGorry, 1996a). This symptom-based approach may be of importance in understanding the symptom progression and mechanisms of symptom development but has received less recent research focus. Outside of specialised research clinics, treatment decisions, such as whether to start antipsychotic medication, are likely to be made on the basis of symptom profile (primarily attenuated psychotic symptoms) or specific psychotic symptoms rather than rating scales. There is little research evidence to support decisions based on symptom profile at present. Research at our clinic suggested that clinicians were not very accurate at predicting who would develop a psychotic disorder in a UHR group based on clinical judgement alone (Nelson and Yung, 2010) but there was no information on how they were actually making these decisions.
In terms of clinical symptoms that might enhance prediction of who might develop a psychotic disorder in this group, there are several areas to consider. A number of psychotic and ‘psychotic-like’ symptoms do not occur in schizophrenia spectrum disorders alone. They also can be present in a variety of non-psychotic disorders such as post- traumatic stress disorder and personality disorders, in particular borderline personality disorder (Zanarini et al., 1990). Particular symptoms such as depersonalisation, derealisation, dissociation and non-typical hallucinations (i.e. not conforming to classical definitions of hallucinations) have been reported to be more characteristic of emerging borderline personality disorder than schizophrenia spectrum disorders (George and Soloff, 1986; Nishizono-Maher, 1993; Pope et al., 1985; Zanarini et al., 1990). In a recent study, psychotic symptoms were found to be prevalent in depression and anxiety disorders (Wigman et al., 2012), and are known to occur relatively frequently in the general population (van Os et al., 2009). Some of the psychotic symptoms seen in those who meet the UHR criteria therefore may not represent an evolving or underlying psychotic disorder but rather represent ‘incidental’ psychotic-like symptoms associated with non-psychotic mental disorders (Nelson and Yung, 2009; Sprong, 2008; Yung et al., 2009). On the other hand, it is unclear whether attenuated symptoms more traditionally associated with a diagnosis of schizophrenia, such as ‘Schneiderian’ first-rank symptoms, represent those on an early pathway to schizophrenia or schizophrenia spectrum disorders, or whether symptoms are more pleomorphic and less specific to disorders, especially in the ‘prodromal’ stages. Further understanding of whether ‘core’ symptoms of disorders can help to distinguish specific groups early can therefore help predictive models and inform early treatment approaches.
There are some data on whether specific psychopathology can enhance the prediction of who will transition to a psychotic disorder in those who meet UHR criteria. However, this tends to be confined to broad symptom domains or symptom clusters, which can be diverse in phenomenological terms; for example, paranoid ideas, hallucinations and bizarre ideas (Cannon et al., 2008; Ruhrmann et al., 2010; Thompson et al., 2011). Few have specifically investigated symptom types (Mason et al., 2004). One study investigated individual scale items as predictors and found that odd ideas/magical ideation, auditory hallucinations and anhedonia/asociality were the most useful additional symptom item predictors, but this study had a relatively small sample with low numbers of transitioned ‘cases’ (Mason et al., 2004). Traditional views on the psychopathology of psychotic symptoms divide them in the ‘form’ of the symptom and the ‘content’ of the symptom (Sims, 1988). Symptom content such as specific paranoid delusions has been found to be associated with transition in some samples but not in others (Thompson et al., 2011) and ‘bizarre’ delusions (Ruhrmann et al., 2010) and grandiosity have also been cited (Lencz et al., 2003). Despite this, no study has looked systematically at symptom content and therefore we have limited data on whether particular content influences risk; for example, does more bizarre delusional content, or disturbances of ego boundary present early and increase risk for transition?
We aimed to collect a more ‘in-depth’ assessment of psychotic-like symptoms (form or content) and investigate whether individual specific baseline attenuated psychotic symptoms or ‘psychotic-like’ symptoms could be useful additional clinical predictors of transition to a psychotic disorder in a UHR group. We hypothesised that: (1) baseline attenuated psychotic symptoms relating to thought disorder, unusual thought content, ego boundary disturbances and bizarre delusions would increase the risk of developing any type of psychotic disorder; and (2) those with attenuated formal thought disorder, negative symptoms and disturbance of ego boundary at baseline would be more likely to develop a schizophrenia-like psychotic disorder than another type of psychotic disorder.
Materials and methods
Design
This was a retrospective ‘case–control’ type study of patients meeting the UHR criteria treated at a specialised UHR clinic. We examined a consecutive series of patients who subsequently developed a psychotic disorder (‘cases’) and compared this to a randomly selected sample from the clinic who had not developed a psychotic disorder within a known time frame (‘controls’).
Setting
The study took place at the PACE (Personal Assistance and Clinical Evaluation) Clinic, which is part of the wider Orygen Youth Health service in Melbourne. To be eligible for treatment at the PACE Clinic, patients must live in northwestern Melbourne, be aged between 15 and 30 years old, and be identified as meeting at least one of the following criteria for an at-risk mental state (ARMS) as assessed by the CAARMS criteria (Yung et al., 2005): the Attenuated Psychotic Symptoms (APS) group with sub-threshold psychotic symptoms with respect to intensity or frequency of symptoms; the Brief Limited Intermittent Psychotic Symptoms (BLIPS) group with symptoms of psychotic intensity but with a total duration (untreated) of less than 7 days; and the trait group (schizotypal personality disorder or family history of a psychotic disorder in a first-degree relative and non- specific symptoms for at least 1 month associated with a significant decrease in functioning). For full operationalised criteria see Yung et al. (2003). All patients attending the clinic were offered up to 12 months of treatment using a cognitive behavioural case management model (for further information see Nelson and Yung, 2007).
Participants
All individuals accepted into the PACE Clinic between 30 June 2003 and 31 October 2008, inclusive, were included in the sample; there were no exclusions. All referrals to the clinic in this period were recorded in a central database. There were 605 individuals seen at the clinic during this period.
Sample
The sample for this study consisted of the following two groups within the overall 605 individuals.
Transitioned ‘cases’
All subjects who were known to have ‘transitioned’ to a full threshold psychotic disorder at 31 January 2010 (n = 66) were identified as ‘cases’. The majority of these ‘transition’ cases were identified during their time attending the clinic. Some were subsequently identified from other sources including follow-up research interviews. Additionally, to supplement our own database, we searched the electronic records in the Victorian public mental health client information management system (CMI), a database which documents all contact with public mental health services in the state of Victoria. This was done for the entire 605 sample and included any transition cases that were not identified by the other methods (n = 3). Transition to psychosis (threshold psychotic disorder) in the clinic is determined using the CAARMS criteria in accordance with earlier studies (Yung et al., 2003, 2004). This operationalised definition of transition to first-episode psychosis consists of daily frank positive psychotic symptoms for longer than 1 week (Yung et al., 2005). For the three cases identified by the clinical database, transition was identified by presence of a DSM-IV-TR (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision) psychotic disorder that fulfilled the above definition. Of the 66 subjects who were known to have developed a psychotic disorder, six were identified from the PACE database as already psychotic at the first appointment with a PACE clinician. They were therefore excluded from the sample. The median time to transition was 1.5 years with a range of 0.1–6.5 years.
Non-transitioned ‘controls’
A random sample of subjects who were known to have not transitioned on 31 January 2010 were the control group; ‘non-transition’ status was established through a combination of known clinical contact with the PACE Clinic, using details from our central database which included follow-up research assessments and additionally searching electronic records in the Victorian public mental health client information management system (as above). The search was conducted on 31 January 2010; the search gave no indication that any of the subjects in this random sample had developed a psychotic disorder. Hence, it was assumed that all these subjects remained free from transition up to the date of search (censor date). A total of 539 potential controls were identified. A total of 60 of these subjects were randomly selected to equal the number of transitioned cases. The random sample of these ‘control’ individuals was selected using random number generation. Thus, cases and controls were not individually matched but they were from the same period of recruitment. This is important as year of recruitment is known to be a strong predictor of development of a psychotic disorder (Yung et al., 2007). The time to follow-up ranged from 1.2 to 6.5 years with a median of 4.5 years.
Symptom measures
An auditing tool was developed specifically for the study in order to gather detailed information from the clinical file about cases and controls, from their time of referral to 4 weeks following initial contact with a PACE clinician. The audit tool was divided into a number of separate sections. For the assessment of psychotic symptoms we included all symptoms assessed in the Operational Criteria for Psychotic Illness (OPCRIT) tool (McGuffin et al., 1991). The OPCRIT is a 90-item computer-based diagnostic tool which generates diagnoses according to 12 operational diagnostic systems (Craddock et al., 1996). OPCRIT is widely used in order to make valid diagnoses of psychotic disorders using information obtained from clinical files and has good validity (McGuffin et al., 1991). We included additional symptom items, especially those related to symptom content, that are not adequately covered by the OPCRIT tool; for example, specific delusional and hallucinatory symptom content. This provided a comprehensive assessment of attenuated psychotic and other psychotic-like symptoms (dissociative, depersonalisation, derealisation and post-traumatic symptoms). The audit tool is included as an online appendix.
Assessment of psychosis diagnosis
Diagnosis at transition to a psychotic disorder was assessed using the OPCRIT tool. All relevant data in the file up to 4 weeks from the date of transition was included in order to produce an OPCRIT diagnosis.
Procedure
For each of the cases and controls, the auditing tool was completed by a research assistant using information from the patients’ clinical files. In order to properly assess baseline symptomatology, we used data from the clinical notes from date of first contact with a PACE clinician until 4 weeks after contact. All patients accepted into the PACE Clinic received a thorough initial assessment, which included the CAARMS and a full assessment of clinical symptoms. However, in some cases, given engagement problems, the assessment process continued for a few sessions. Most symptoms were recorded on the thorough initial assessment but occasionally further symptoms were elicited in the first few weeks of engagement with the clinician.
For ‘cases’ that developed a psychotic disorder, the OPCRIT was also administered by auditing clinical notes dated from time of transition until 4 weeks afterwards. Only the DSM-IV diagnoses generated by the OPCRIT program were used. Consequently, the research assistant was not blind to the transition status of the individual but was not aware of the study hypotheses. The accuracy of the ratings of the presence/absence of symptoms by the research assistant was regularly checked by one of the investigators (BN) following initial training by two investigators (AT and BN). The study had full ethical approval from the local hospital Research and Ethics Committee.
Data analysis
Transition to a psychotic disorder was used as the outcome of interest and the dependent variable. For the purposes of this study, the independent variables were all symptom questions included in the audit tool. However, when there were small numbers of responses for items (such as thought insertion or thought withdrawal), it was necessary to combine or group symptoms in some instances. The number of responses to an item that was considered satisfactory for analysis was set at around n = 10, a priori. These groups were formed on the basis of conventional psychopathological descriptions (Sims, 1988) by consensus between three of the authors (AT, BN and AY). When the original symptoms were combined into groups this is indicated in Table 2.
The items detailing OCD symptoms were poorly recorded in the clinical file and were therefore omitted from the analysis. Bizarre delusions were not adequately defined and hence not well recorded using the audit tool and not subject to analysis. Some symptoms such as behavioural perplexity and flattened, inappropriate or restricted affect were omitted due to the small number of individuals reporting these and the inability for these symptoms to be meaningfully grouped with other symptoms. All other items were included in the original form or combined into appropriate groupings according to traditional psychopathological schemes.
We performed a survival analysis using log-rank test and Cox regression to investigate the relationship between symptom variables and transition to a psychotic disorder, with time to transition as a time-to-event variable. In the case of binary factors, an exact log-rank test (based on the distribution of the sum of independent hypergeometric random variables) was used.
As there were a relatively large number of variables, any association of < 0.1 in the univariate analysis was then subject to a multivariate analysis controlling for other possible predictive symptom variables. We then repeated this multivariate analysis additionally adjusting for age, gender, duration of psychotic symptoms and intake group. The additional adjustment was performed as a number of these variables, especially duration of symptoms and intake group, are known to be associated with transition to a psychotic disorder in our population (Yung et al., 2004).
A secondary analysis was performed to investigate hypothesis two, that particular symptoms would be associated with transition to a schizophrenia-like disorder. The grouping of psychotic disorders was based on that of Baldwin et al. (2005), which has previously been used in this population. In this grouping, the schizophrenia-like psychosis group included schizophrenia, schizophreniform psychosis and schizoaffective disorder. The symptoms (independent variable) specifically tested were: (1) thought disorder (and specifically tangentiality and thought blocking); (2) negative symptoms; and (3) delusions of ego boundary, delusions of thought interference and command hallucinations. As with the above analysis, this was then subject to a multivariate analysis controlling for other possible predictive symptom variables.
Results
Sample demographics
The demographics of the sample are shown in Table 1. Similar to recent samples from our clinic, 59% were female and less than 10% of individuals met the trait only entry criteria. The OPCRIT DSM-IV diagnoses at transition were: bipolar I disorder, 1 (1.7%); brief psychotic disorder, 1 (1.7%); delusional disorder, 1 (1.7%); major depressive disorder with psychotic features, 6 (10.0%); psychosis not otherwise specified (NOS), 33 (55.0%); schizoaffective disorder, 1 (1.7%); schizophrenia, 6 (10.0%); and schizophreniform disorder, 11 (18.3%).
Demographics of the sample.
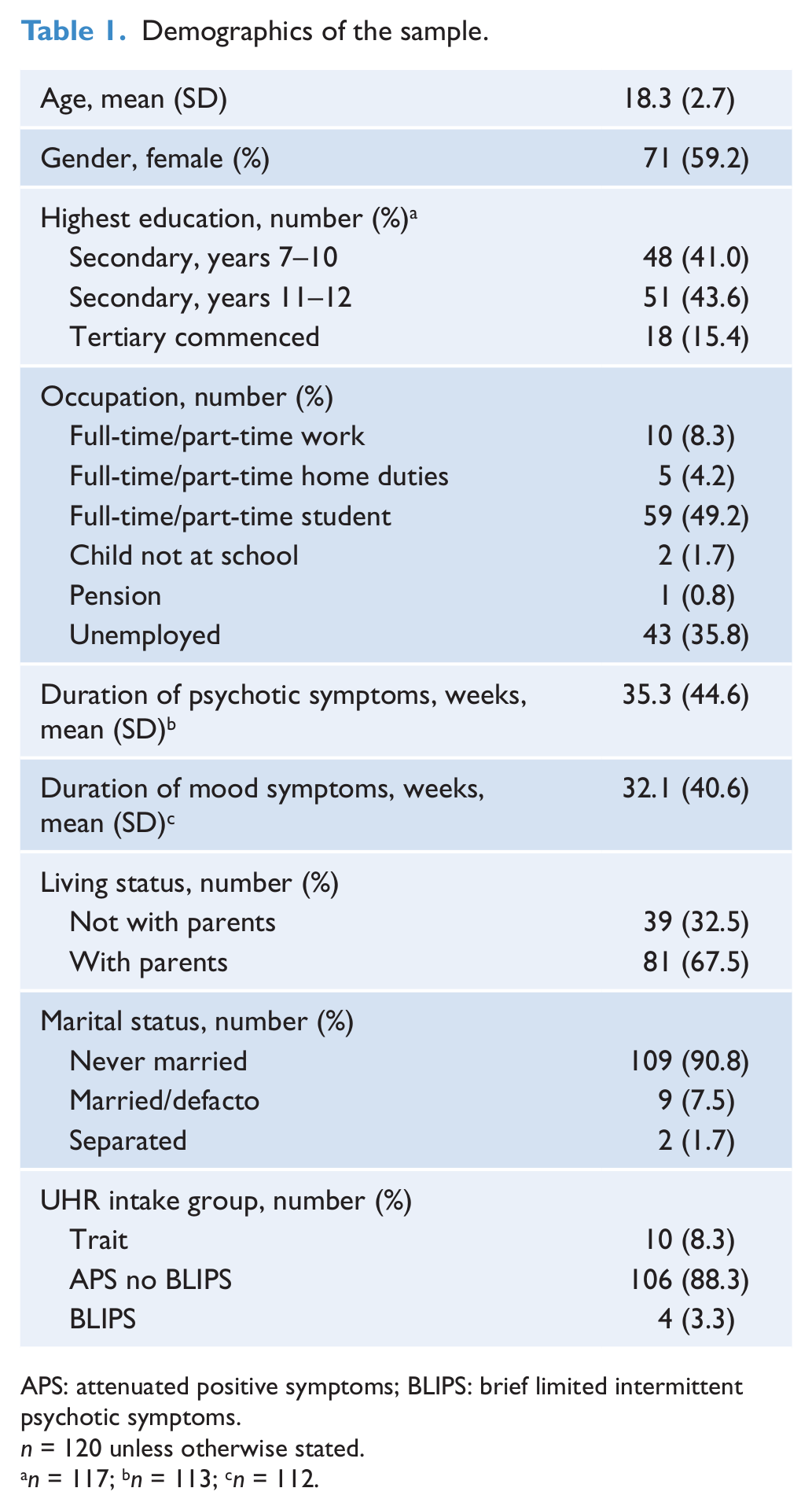
APS: attenuated positive symptoms; BLIPS: brief limited intermittent psychotic symptoms.
n = 120 unless otherwise stated.
n = 117; bn = 113; cn = 112.
Symptom form/content and relationship to development of psychosis
Univariate analysis
Table 2 shows the hazard ratios for all the symptom items (form and content) in the sample. In the instances where the symptoms were combined, this is indicated in the table and the individual symptoms described. The symptoms that were significantly associated with transition to a psychotic disorder in the survival analysis were: presence of thought disorder (controls, n = 8; cases, n = 14), any delusion (controls, n = 39; cases, n = 48) and elevated mood (controls, n = 2; cases, n = 10).
Prevalence of symptom form and content with associated hazard ratios (and p-value) of developing a psychotic disorder.
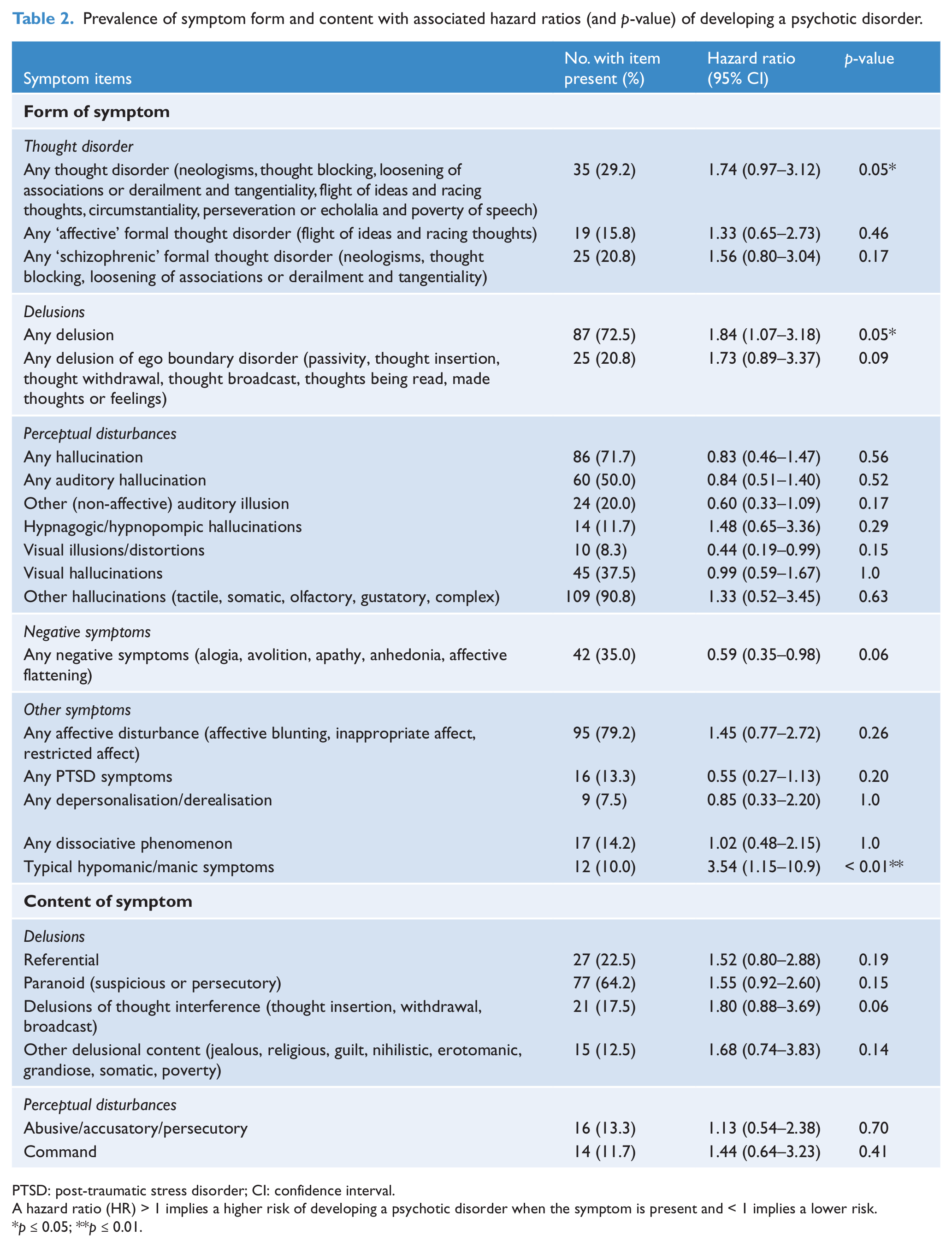
PTSD: post-traumatic stress disorder; CI: confidence interval.
A hazard ratio (HR) > 1 implies a higher risk of developing a psychotic disorder when the symptom is present and < 1 implies a lower risk.
p ≤ 0.05; **p ≤ 0.01.
Multivariate analysis
Table 3 shows that of these three symptoms, elevated mood remained significant after adjusting for other factors in the analysis (hazard ratio 2.69, p = 0.002). The presence of this factor is associated with a 2.7-fold increase in the transition to a psychotic disorder (95% confidence interval (CI): 1.29–5.63). None of the remaining symptom items achieved significance after adjusting for the two factors discussed above.
Adjusted analysis of the joint significance of variables that were associated with a p-value of predictors ≤ 0.1 in the univariate analysis (Table 2).
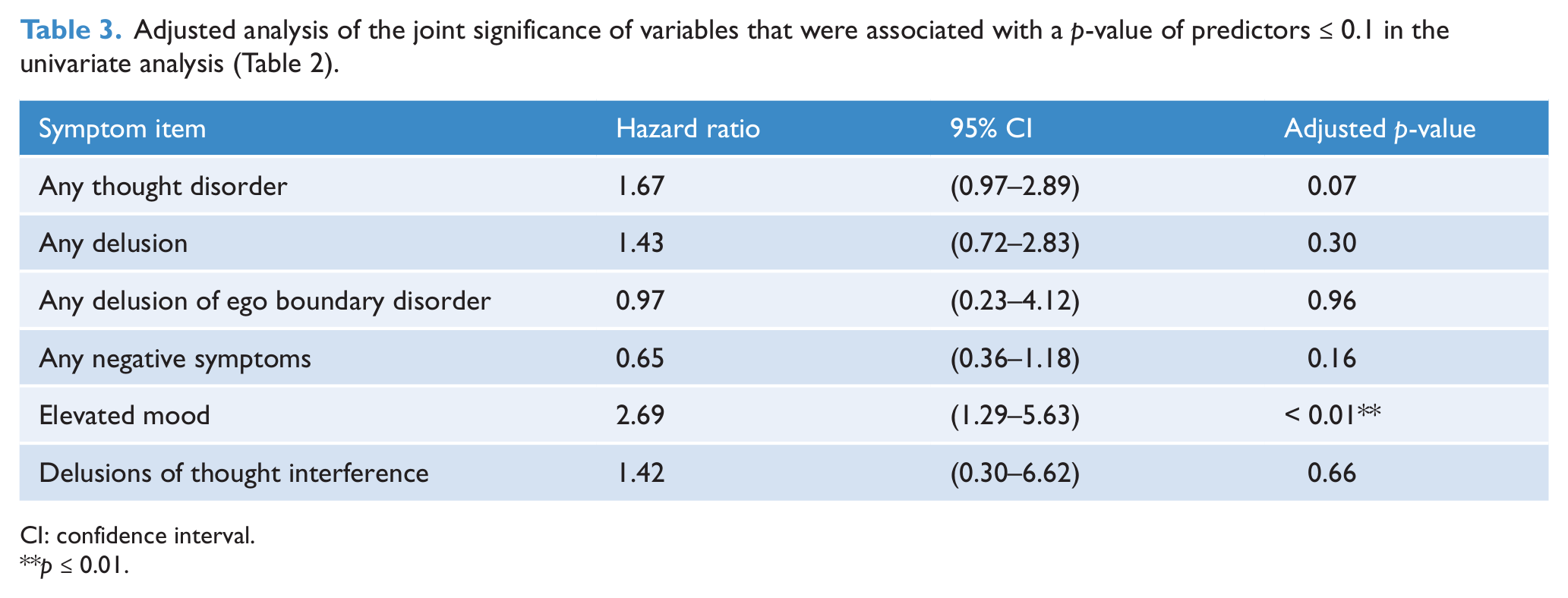
CI: confidence interval.
p ≤ 0.01.
Given that thought disorder was a combined symptom item made up of a number of individual symptom items, we also analysed these specific items separately. For the thought disorder questions, only one of the subjects in the study either experienced flight of ideas, neologism, perseveration/echolalia or poverty of speech. Derailment/loosening of associations and circumstantial thought disorder were only seen in three and four subjects, respectively. Thus, no analysis was carried out for these variables. The only variables that were analysed were racing thoughts, thought blocking and tangentiality. After adjustment for the other symptom items, only thought blocking was associated with development of a psychotic disorder (hazard ratio 2.26; 95% CI: 1.15–4.44, p = 0.017).
We repeated the multivariate analysis adjusting for the potential confounders of age, gender, duration of symptoms and intake group. Eight subjects were omitted due to missing information on some items. After adjusting for age, gender, duration of psychotic symptoms and intake group status, the results from the analysis remained essentially the same as above.
Relationship between specific symptoms and schizophrenia-like psychotic disorder
The analysis investigating the relationship between specific symptoms and development of a schizophrenia-like psychotic disorder is shown in Table 4. ‘Schizophrenic’ formal thought disorder at entry to the clinic was associated with development of a schizophrenia-like disorder (hazard ratio 3.69, p = 0.008). This item was composed of neologism, perseveration/echolalia or poverty of speech, derailment, loosening of associations, circumstantial thought, thought blocking and tangentiality. Of these thought disorder items, two had > 10% prevalence and were subject to further analysis. Of these two, both thought blocking and tangentiality were associated with a higher risk of transition to a schizophrenia-like disorder (Table 4). None of the other baseline symptoms investigated was associated with an increased risk of transition to a schizophrenia-like psychotic disorder.
Symptom form and content items as predictors of developing a schizophrenia-like psychotic disorder with associated hazard ratios, confidence intervals and p-values.
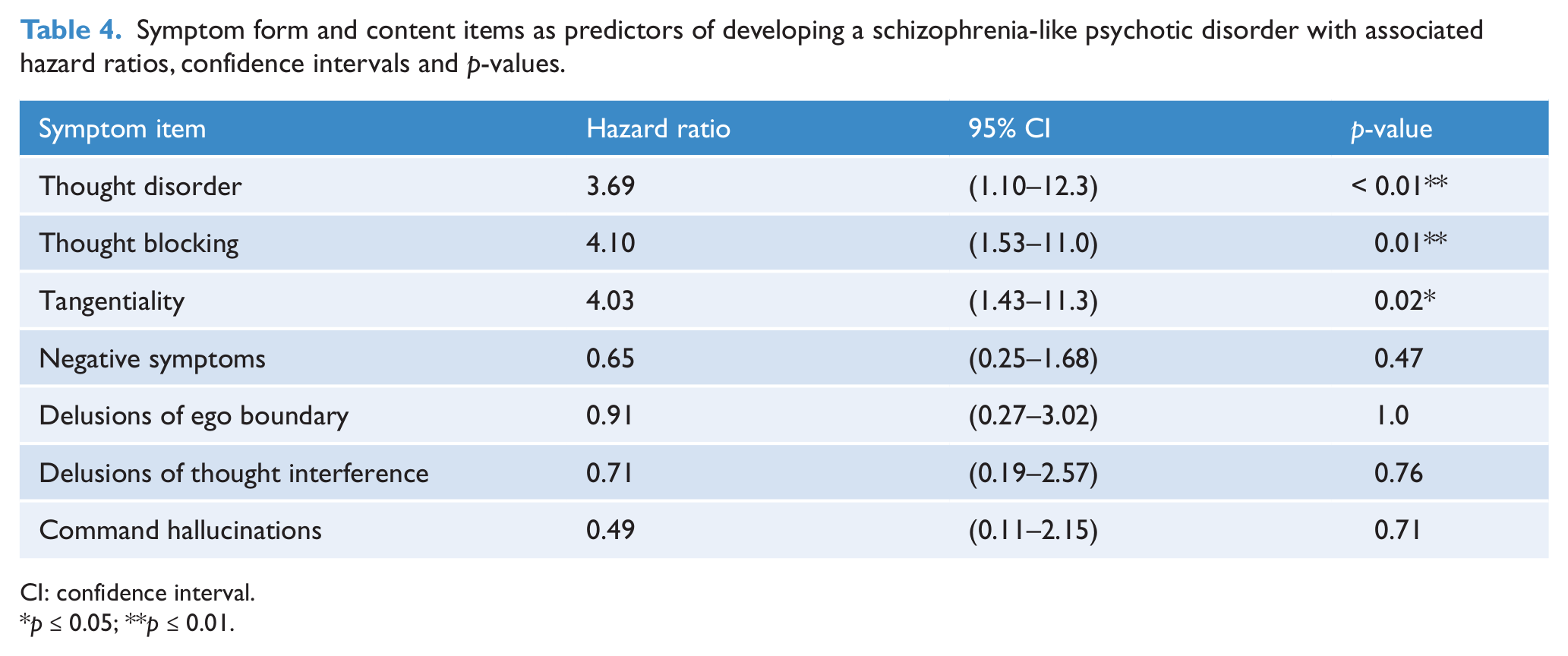
CI: confidence interval.
p ≤ 0.05; **p ≤ 0.01.
Discussion
Principal findings
In this study we investigated whether the form or content of specific individual attenuated psychotic symptoms and other psychotic-like symptoms at entry to a UHR service could predict subsequent transition to a full threshold psychotic disorder. The results indicate that only a few of the clinical symptoms (either form of symptoms or symptom content) predicted whether an individual would transition to a psychotic disorder. Those most predictive when other symptoms were adjusted for were the presence of formal thought disorder, especially thought blocking and tangentiality, and elevated mood. The presence of unusual thought content in terms of delusions of any type was associated with transition to psychosis in the main analysis but not when other symptoms were adjusted for. We also found that, of the symptoms we proposed would be associated with increased risk of a schizophrenia-like disorder, thought disorder was associated with this outcome.
Comparison to previous work
There appears to be some consistency in our results compared to other studies. The finding in the main analysis, that presence of any delusion was predictive of transition to psychosis, is broadly consistent with the findings of other studies. For example, both the North American Prodrome Longitudinal Study (NAPLS) (Cannon et al., 2008) and our own study using their predictor variables (Thompson et al., 2011) reported that unusual thought content, broadly a measure of delusional type thinking, was predictive of developing a psychotic disorder. The finding that thought disorder was predictive has similarities with the findings of the European Prediction of Psychosis Study (EPOS), which reported increased levels of ‘bizarre thinking’ as an important predictor, which the authors linked to thought disorder (Ruhrmann et al., 2010).
Overall, in terms of the attenuated psychotic symptoms, our findings indicate that disturbance of thought content and form, specifically thought blocking and tangentiality, are more related to imminent onset of psychotic disorder, especially in those who develop a schizophrenia-like disorder. Perceptual disturbances in general did not appear to add any additional predictive value. Perceptual disturbances may belong more to the category of ‘incidental’ attenuated psychotic symptoms (i.e. occur in the context of evolution/onset of non-psychotic disorders) and may be considered less predictive of transition in the absence of other psychotic phenomena. Indeed, hallucinations are the most prevalent of psychotic-like symptoms in general population samples (Horwood et al., 2008; van Os et al., 2001) and most would not appear to be of clinical significance (van Os et al., 2009). Whether the presence of hallucinations alone in individuals who meet the UHR criteria indicates a reduced risk to those presenting with symptoms other than hallucinations, would need further study. Of note, only one of a number of prospective prediction studies has indicated that the presence of hallucinations increases the risk of transition (Mason et al., 2004).
As expected, the presence of formal thought disorder, although a relatively infrequent symptom, was associated with transition to both psychotic disorder in general and a schizophrenia-like disorder in particular. A more surprising result was the association between elevated mood and transition to a psychotic disorder. To our knowledge, only one study by Lencz and colleagues has reported a relationship between manic symptoms (in this case grandiose ideas) and development of a threshold psychotic disorder (Lencz et al., 2004). As with the thought disorder symptoms, the frequency of reporting was relatively low. To explore this further, we examined whether the presence of elevated mood was related to the development of a primary manic psychosis. Prospective studies have suggested that mood lability/elevation is the strongest risk factor for the subsequent diagnosis of a bipolar spectrum disorder (odds ratio (OR) 14), greater even than a family history of mania (OR 7) (Angst et al., 2003). This did not appear to be the case in the present study, with only one individual receiving a bipolar I diagnosis at transition. However, we are aware of the limitations of our ratings of diagnosis at transition and note the high number of cases given a diagnosis of psychosis NOS and the longitudinal instability for such a diagnosis in first-episode psychosis cohorts (Addington et al., 2006; Schimmelmann et al., 2005). The result may represent the difficulty in distinguishing between clinical trajectories early in the course of symptoms. Specifically, what might strike clinicians as an emergence of bipolar disorder (manic symptoms) may in fact go on to become a non-bipolar psychotic disorder.
Our results provide some support for the proposal that ‘prodromal’ psychotic symptoms follow a more diffuse or ‘pleomorphic’ course as opposed to a clear one from the outset. This is consistent with the clinical staging model for psychiatric disorders proposed by McGorry and colleagues (2006). Authors have suggested that psychotic symptoms do not occur de novo but often develop from more subtle changes in perception or thinking (Gross et al., 1998; Klosterkotter et al., 2001; Nelson et al., 2012). It may be that symptoms often attributed to schizophreniform disorder, as described by the classical phenomenological descriptions, are part of a natural development of some symptoms and represent chronicity, rather than being disorder-specific in the early stages. There are no studies of symptom form and content over the time course of a psychotic disorder and little is known of symptom stability. In support of this suggestion are the reports of different types of delusions present in patients with a first episode of schizophrenia as opposed to those with a chronic illness (Lucas et al., 1962; Rajapakse et al., 2011). On the other hand, an alternative hypothesis would suggest content and form of symptoms are on a continuum. Symptoms that are more typical of a phenomenological description of schizophrenia-spectrum disorders may be more often associated with a transition to a psychotic disorder or specifically to a schizophrenia-spectrum disorder, and that other symptoms might occur either transiently in young adults with vulnerable brains in the context of increased stress, or as epi-phenomena in the context of the development of other, non-psychotic, psychiatric disorders. The lack of additional prediction from any of the ‘psychosis-like’ symptoms we investigated and the association between thought disorder and developing a schizophrenia-like disorder might support this hypothesis. Further research is needed into these models, as they are likely to influence early treatment approaches and the further categorising of psychosis risk.
Strengths and limitations of the study
The main strength of this study is that it uses data from a relatively large number of individuals with baseline symptom data who subsequently developed a psychotic disorder (n = 60). Therefore, it has the benefit of increased power compared with other studies in the field. Despite this, the numbers are still relatively small, especially when investigating diagnostic groups, and should be interpreted with this caveat. It should also be noted that our ‘case–control’ sample is not completely adequate, as we know that transitions of ‘controls’ could occur a number of years after entry into the clinic, although the rate is much lower after 2 years (Yung et al., 2012). Our analysis using survival methodology and the censoring of cases addresses this problem to some extent. Given this limitation, our conclusions are regarding the relationship between symptoms and short-term risk of transition.
There are some problems using clinical files to extract the symptom data. Whilst using the CAARMS and a standard interview format, clinicians were not using a standardised assessment of form and content of all possible symptoms. We cannot be certain that our symptom data was not subject to bias due to some questions not being asked systematically.
Not all symptoms were present in sufficient cases to allow investigation individually and therefore we needed to combine a number of symptoms into broader groups. We set a priori the prevalence of a symptom at around 10% in order to reduce the possibility of type 1 errors in interpreting associations with very low numbers. Some symptoms were not directly recorded as such in the notes and were open to considerable interpretation by the data collectors and therefore omitted from the analysis; the most important of these was the overall category of bizarre delusions. However, more specific types of delusional ideas of a bizarre nature were captured in the audit (e.g. delusions of ego boundary disorder).
With regard to the transition diagnosis, we were aware that around 50% of the OPCRIT diagnoses taken at the time of transition were given as psychosis NOS. This may be because the duration of symptoms was not sufficient to fulfil the criteria for other types of psychotic diagnosis. It is possible that this biased the analysis of the relationship between symptoms and a schizophrenia-like psychotic disorder. Unfortunately, accurate data on all diagnoses made by clinicians later in the treatment were not available on all subjects and therefore we could not compare these with the transition OPCRIT diagnoses. Consequently, we would argue some caution as to these results and would encourage replication in independent samples with re-evaluation of diagnosis at a time point post-transition.
Finally, it should be noted that the use of the Victorian public mental health database to provide additional information on transition status involves the assumption that each subject was still alive and remained in contact with the Victorian public mental health services up to the date of the search. However, it should be noted that the level of clinical follow-up was substantial, with most patients being seen at the clinic and for at least a year, and then, for a number of individuals, at subsequent research interviews. All ‘transitions’ from research studies or within the clinical service were recorded on the PACE Clinic database.
Clinical implications
A particularly topical debate, given the concerns regarding rates of antipsychotic prescribing for non-psychotic disorders, is the assumption that clinicians can predict, based on clinical impression, who is at an increased risk of developing a psychotic disorder within a group identified as meeting UHR criteria. This study suggests that although some symptoms may be more predictive of the development of a psychotic disorder, these are limited in number and predictive power. Specifically, the development of thought disorder and elevated mood may be indicators of a more imminent risk of transition to psychosis within the UHR group. However, we would not currently recommend using simply the symptom profile or clinical experience to predict outcome in this group, as our previous research highlights (Nelson and Yung, 2010). It should also be noted that a combination of several symptoms and other risk factors appears to have the highest predictive validity predictive for developing a psychotic disorder in other studies (Cannon et al., 2008; Thompson et al., 2011). A comprehensive and longitudinal evaluation of symptoms, functioning and other risk factors is thus recommended wherever possible.
Conclusions
The study suggests that for individuals meeting UHR criteria, the utility of specific clinical psychopathology in predicting increased risk for psychosis is somewhat limited and should be used in combination with other known risk factors.
Footnotes
Acknowledgements
The authors would like to acknowledge all the clinicians involved in assessing and treating the patients during the study period. We would also like to thank Kally Yuen for assistance in data analysis.
Funding
Orygen Youth Health receives funding from the Colonial Foundation Philanthropic Trust.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.