
Abstract
Objective:
To investigate the correlations between cognitive function and clinical outcome variables.
Method:
Patients diagnosed for the first time with schizophrenia between January 2004 and June 2010 were cognitively tested in conjunction with diagnostic procedures. Cognitive test data were connected to Danish healthcare registers and patients were followed in the registers from their first contact with psychiatric in- and outpatient care until October 2011.
Results:
Patients had impaired attention, processing speed and executive function as measured by Trail Making Test part B; their executive functions, as measured by the Wisconsin Card Sorting Test (WCST), and working memory, as measured by Rigshospitalet’s digit span test, were unaffected as compared to norms. The admission rate, from schizophrenia diagnosis to the end of the study, was predicted by Trail Making Test part A, Rey’s Auditory Verbal Learning Test (RAVLT), RAVLT (total learning), RAVLT (memory), d2 Test of Attention (total) and d2 type 2 error (error of commission), independent of gender, age and schizophrenia subtype. The length of hospitalization after the schizophrenia diagnosis was mainly determined by the schizophrenia subtype (schizophrenia simplex: incidence rate ratio (IRR) 0.24; 95% confidence interval (CI) 0.15–0.40, p < 0.001). Diagnosis was secondarily determined by deficits in attention and executive function, Trail Making Test part B, d2 Test of Attention (total), d2 type 1 error (error of omission), d2 type 2 error, and also by age and substance use disorder. The outpatient contact rate from schizophrenia diagnosis to the end of the study was predicted by d2 Test of Attention, Trail Making Test part A, and d2 type 2 error. The annual rate of criminal conviction, institutionalization and social retirement pension was mainly predicted by substance misuse.
Conclusion:
Cognitive function only predicted hospitalization and outpatient contacts to a minor degree in a cohort of newly diagnosed patients with schizophrenia.
Keywords
Introduction
A core feature of schizophrenia is cognitive deficits, particularly in attention, memory, reasoning and problem-solving, but also, to a lesser degree, in the visual, spatial and vocabulary domains (Buchanan et al., 2005; Green et al., 2000; Heinrichs and Zakzanis, 1998). Cognitive test scores of patients diagnosed with schizophrenia are generally 1–2 standard deviations below the scores of healthy controls (Cannon et al., 1994; Nielsen, 2011). When compared with other severe mental disorders, for example, major depression and bipolar disorder, patients with schizophrenia are more severely impaired on a wider range of cognitive domains (Bora et al., 2011; Buchanan et al., 2005).
The time of onset of cognitive deficits or cognitive decline is unknown. Deficits appear to be present before the first episode of psychosis (Caspi et al., 2003), and evidence points towards cognitive deficits present in childhood, with a possible relative decline in cognitive function from early adolescence to late adolescence in persons later diagnosed with schizophrenia (Kremen et al., 2010; Osler et al., 2007). The cognitive deficits in patients with schizophrenia appear to be stable over time and are partly independent from primarily positive, but also, to a lesser degree, negative symptoms (Bonner-Jackson et al., 2010; Sponheim et al., 2010; Szøke et al., 2008). However, some studies do suggest further cognitive decline as a function of psychotic relapses (Eberhard et al., 2003; Levander et al., 2001).
The correlations between cognitive deficits and daily life functions, for example, employment, independent living and social functioning, the stability of cognitive function, and the independence of cognitive symptoms from positive symptoms have all fuelled research into cognitive function (Dominguez et al., 2009; Fett et al., 2011; Green, 1996; Green et al., 2000; Nuechterlein et al., 2011; Szøke et al., 2008; Ventura et al., 2010). Correlations between cognitive function and functional outcomes have been shown in cross-sectional and longitudinal studies (Fett et al., 2011; Harvey, 2007). Cognitive function has also been linked to other outcomes, such as treatment adherence, and has been inversely linked to risk of admission and number of contacts (Goldberg et al., 2011; Johansen et al., 2011; Osler et al., 2007).
The aim of this study was to investigate the correlations between the cognitive functions of newly diagnosed patients with schizophrenia and hospitalization and outpatient contacts, as well as the risk of criminal convictions, institutionalization and social retirement pensions.
Methods
Design
Patients diagnosed with schizophrenia for the first time, were cognitively tested between January 2004 and the end of June 2010 at the Clinic for Young People with Schizophrenia, Aarhus University Hospital, Risskov, Denmark. All patients underwent a semistructured diagnostic interview (Present State Examination). The date of diagnosis was retrieved from the registers to allow data linkage to other registers. The cognitive test data were linked to the nationwide Danish healthcare registers via unique personal identifier numbers (Pedersen, 2011). Patients were followed in the registers from the index date of schizophrenia diagnosis until the end of October 2011.
Measures
A battery of cognitive tests including the Wisconsin Card Sorting Test (WCST) (Axelrod, 2002; Heaton, 1981), Trail Making Test parts A and B (Strauss et al., 2006), Rey’s Auditory Verbal Learning Test (RAVLT) (Strauss et al., 2006), Rigshospitalet’s digit span test and the d2 Test of Attention (Bates and Lemay, 2004), were used.
Wisconsin Card Sorting Test
The WCST measures executive function (Axelrod, 2002; Heaton, 1981). The test consists of four stimuli cards (one with a red triangle, one with two green stars, one with three yellow crosses, and one with four blue circles). The subject must sort 64 or 128 cards with different patterns to the stimuli cards (either by color, geometric shape or number of objects) and is given feedback (correct/incorrect) after each match. After 10 consecutive correct matches, the matching concept is shifted without any forewarning. There was no time limit for the test. The 64-card version was used in this study. Norm values were extracted from the existing literature (Egan et al., 2011).
Trail Making Test parts A and B
Trail Making Test part A measures attention and processing speed, while part B is used for measuring attention, executive function and processing speed (Strauss et al., 2006). Part A requires the subject to connect 25 encircled numbers with a pencil line in the correct order. Part B requires the subject to connect 25 encircled numbers and letters in alternating order with a pencil line. Norm values were extracted from the existing literature (Strauss et al., 2006).
Rey’s Auditory Verbal Learning Test
The RAVLT measures verbal learning (Strauss et al., 2006). The test consists of 15 words that are read aloud to the person five times. Immediate and delayed (20 min) recall is measured. Norm values were extracted from the existing literature (Badcock et al., 2011; Vakil et al., 2010).
Rigshospitalet’s digit span test
This test measures immediate and working memory. The test consists of a sequence of numbers read aloud to the subject. They must then immediately recall the number sequence, backwards and forwards. The length of the sequence increases. The length of the longest number span is recorded as the test result. Norm values were delivered with the original test package and are not published.
d2 Test of Attention
This test measures sustained attention (Bates and Lemay, 2004). The test consists of 14 lines with 47 symbols on each line. The symbols are either a letter d or a letter p with one, two, three or four small dashes above or below them. Each subject is asked to go through the lines and cross out all the d symbols with one or two dashes above or below them. The test is reported with a d2 total score, d2 type 1 error (error of omission) and d2 type 2 error (error of commission). Norm values were extracted from the existing literature (Bates and Lemay, 2004).
Demography
The International Classification of Diseases, 10th revision (ICD-10) F20.x (schizophrenia subtypes) (World Health Organization, 1992) and possible ICD-10 F10–F19 (mental and behavioural disorders due to psychoactive substance use) diagnosis was retrieved from the Danish Psychiatric Central Research Register (DPCRR) (Mors et al., 2011). Other possible diagnoses were not retrieved, for example, initial referral diagnosis.
Admission rates were calculated as the number of admissions per year since schizophrenia was diagnosed; the number of bed days and outpatient contacts were calculated in a similar manner. Data was extracted from the DPCRR (Mors et al., 2011). Criminal convictions were extracted from the Danish Central Crime Register (Munkner et al., 2009). Accommodation status was defined as either living or not living in an institution. Data was provided by the Danish accommodation database (Thygesen et al., 2011), which registers the accommodation status of all inhabitants in Denmark. The patients’ means of living, for example, work, school, social welfare or early retirement pension status, were retrieved from the Integrated Database for Labour Market Research (Thygesen et al., 2011). Educational levels were also identified from the Integrated Database for Labour Market Research (Thygesen et al., 2011) and were divided into three categories: (1) primary school (mandatory; covers from first to 10th grade); (2) vocational education (for example, plumber); and (3) high school (begins at completion of primary school). Finishing an education, getting a criminal conviction, living in an institution or receiving social retirement were dichotomized (yes/no). Specific age limits were set for the previously mentioned variables to give all cases the same time at risk and to allow full retrieval from the registers.
Medication
Medication variables were obtained from the Danish National Prescription Registry, which contains all prescription-based medications collected from pharmacies (Kildemoes et al., 2011). Data from medication use during hospitalization was not registered in this database.
Antipsychotics were divided into first-generation antipsychotics (FGAs) and second-generation antipsychotics (SGAs).The FGA group consisted of: chlorpromazine, chlorprothixene, flupenthixol, fluphenazine, haloperidol, levomepromazine (methotrimeprazine), periciazine, perphenazine, pimozide, pipamperone, prochlorperazin and zuclopenthixol. The SGA group consisted of: amisulpride, clozapine, olanzapine, quetiapine, risperidone, sertindole, sulpiride and ziprasidone. The antipsychotic depot injection group consisted of flupenthixol, fluphenazine, haloperidol, perphenazine, risperidone and zuclopenthixol. Antidepressants were defined according to the World Health Organization (WHO) anatomical therapeutic chemical (ATC) code N06A. Benzodiazepines were defined according to the WHO ATC codes N05BA, N05CD, N05CF and N03AE. Antiepileptics were defined according to the WHO ACT code N03A (World Health Organization, 2009).
The Danish Data Protection Agency and National Board of Health and Statistics Denmark approved the use of the data. No ethical research committee approval was needed, as cognitive test data was obtained from registers for statistical purposes only.
Statistical analysis
A demographic description of cases was performed. Cognitive tests were described comparing mean scores to the norm values using the Student’s t-test. If distributional assumptions were not met, the Wilcoxon rank-sum test was used.
Regression analyses were performed with cognitive test results standardized to z-scores. This was done to determine the relationship between cognitive function and several outcomes. In the regression analyses, the candidate variables were: Trail Making Test parts A and B; RAVLT (total learning); RAVLT (delayed-recall); WCST (number of categories completed); WCST perseverative score; Rigshospitalet’s digit span forwards and backwards; d2 (total score); d2 type 1 error; d2 type 2 error; diagnosis; age and gender. Candidate variables were tested by univariate regression analysis before inclusion in the multivariate regression analysis with a significance level of p < 0.10. If the univariate regression was not significant, candidate variables were excluded from the multivariate analysis. One exception from the exclusion were candidate variables established as possible confounders, defined as a 20% change in the regression estimates of the remaining candidate variables. The candidate variables were used in the regression analyses with the dependent variables: mean admission rate per year since schizophrenia diagnosis; mean number of hospitalized days per year since schizophrenia diagnosis; mean number of outpatient contacts per year since schizophrenia diagnosis; criminal convictions before age 23; institutionalization before age 22 and social retirement pension before age 22. P values of less than 0.05 were generally considered statistically significant. Statistical analyses were performed using STATA 12 (StataCorp LP, College Station, Texas, USA) at the Statistics Denmark server via remote access.
Results
The study population consisted of 109 patients diagnosed with schizophrenia for the first time, 57 men and 52 women (p = 0.55). The mean age at schizophrenia diagnosis was 24.6 years (SD = 3.4). Almost half (47.7 %) of the patients were diagnosed with an undifferentiated schizophrenia diagnosis (ICD-10, F20.3), and nearly one-third (32.1 %) were diagnosed with paranoid schizophrenia (ICD-10, F20.0). These two diagnoses were significantly more frequent than the remaining schizophrenia diagnostic subtypes. Twenty-nine (26.6 %) patients were diagnosed with a substance use disorder as an auxiliary diagnosis, as shown in Table 1.
Patient demographics.
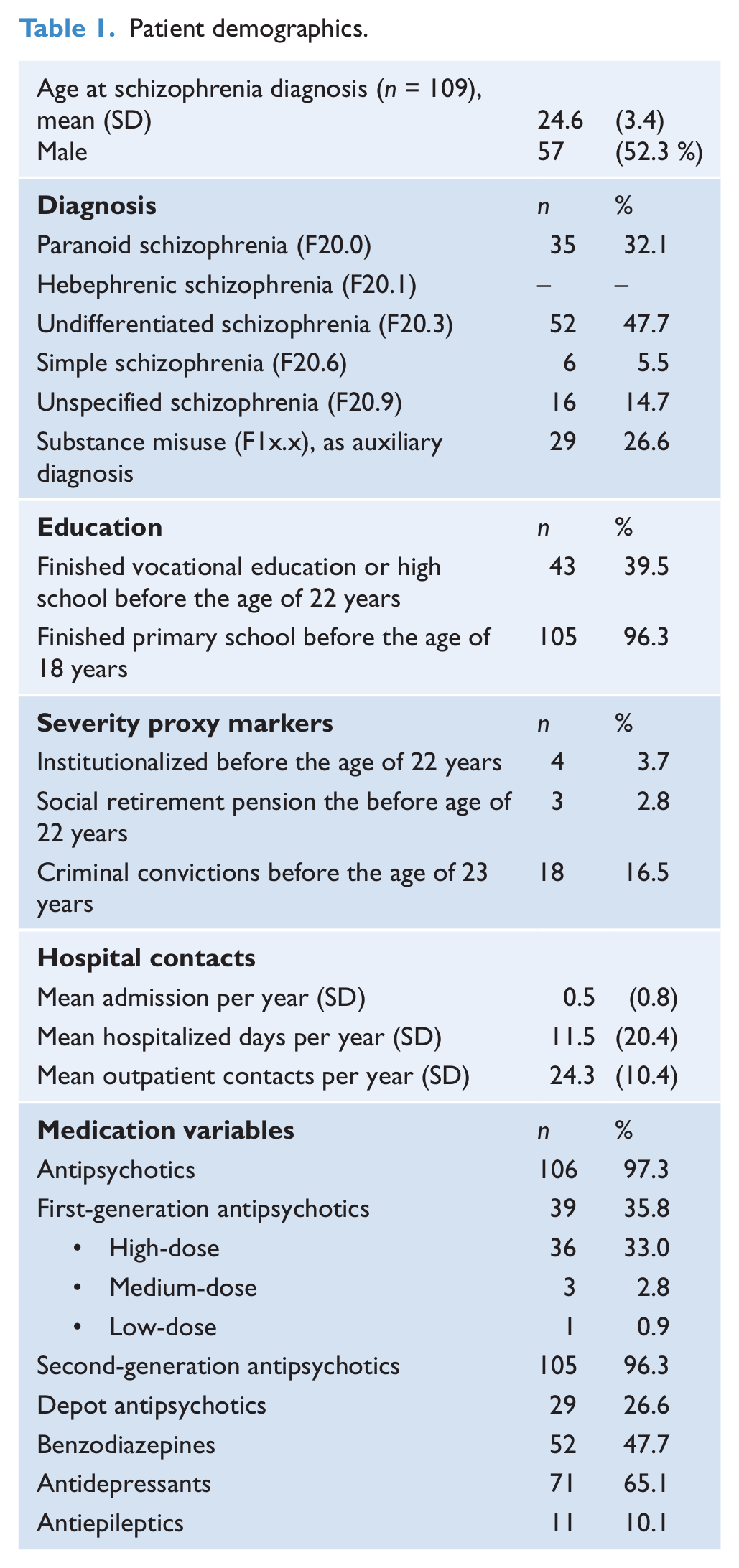
Four (3.7 %) patients were living in an institution before age 22 and three patients (2.8 %) received early retirement pension before age 22. Overall, the mean annual rate of admission after schizophrenia diagnosis was 0.5 (SD = 0.8); the mean annual rate of hospitalized days after schizophrenia diagnosis was 11.5 (SD = 20.4) days and the mean annual number of outpatient contacts after schizophrenia diagnosis was 24.3 (SD = 10.4).
Patients were significantly impaired on most tests of cognitive function compared to the norms (Table 2). Almost all of the 109 patients were subjected to all cognitive tests, with the exception of the WCST-64 (short form), which used a sample of 65 patients. We conducted post-hoc analyses of patients subjected to the WCST versus patients not subjected to the WCST on age at testing, age at diagnosis, gender, schizophrenia subtype specifier and the remaining cognitive tests. No significant differences on any outcomes were found except on the Trail Making Test part A (mean 48.8 ± 29.8 s vs. mean 33.7 ± 16.8 s, p < 0.05) and the Trail Making Test part B (mean 115.6 ± 68.2 s vs. 75.6 ± 34.9 s), in which non-WCST patients did significantly worse.
Mean cognitive test scores.
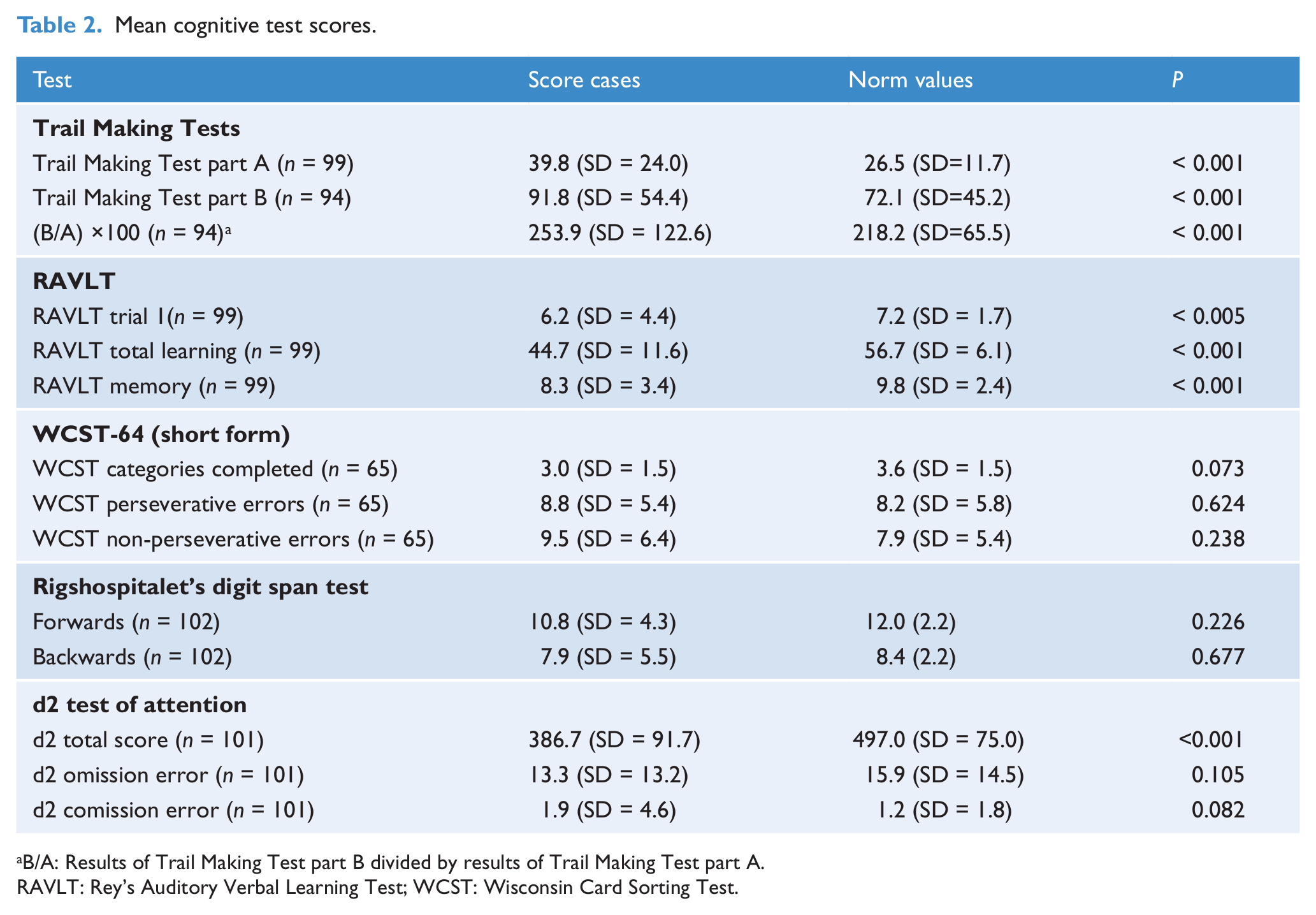
B/A: Results of Trail Making Test part B divided by results of Trail Making Test part A.
RAVLT: Rey’s Auditory Verbal Learning Test; WCST: Wisconsin Card Sorting Test.
Regression analyses were used to examine the effect of cognitive function on hospitalization and outpatient contacts (Table 3). The main findings indicated that the cognitive tests predicted risk of admission, defined as number of admission per year, independently of gender, age and schizophrenia subtype: Trail Making Test part A (IRR = 1.12, 95% CI 1.04–1.21, p < 0.005),where a slow performance increased the annual rate of admissions; RAVLT total learning (IRR = 0.85, 95% CI 0.79–0.92, p < 0.001), where a high number of words immediately recalled decreased the risk of admission; RAVLT memory (IRR = 1.38, 95% CI 1.17–1.63, p < 0.005), where a high number of words remembered increased the risk of admission; d2 total (IRR = 0.81, 95% CI 0.71–0.92, p < 0.005), where a high number of symbols processed decreased the annual rate of admission; and d2 type 2 error (IRR = 0.90, 95% CI 0.84–0.97, p < 0.005), where a high number of type 2 errors decreased the risk of admission. The length of hospitalization, defined as the number of days hospitalized per year, is primarily predicted by diagnosis subtype (for example, schizophrenia simplex (IRR = 0.24, 95% CI 0.15–0.40, p < 0.001)), but also, to a minor degree, by deficits in attention and executive domains: Trail Making Test part B (IRR = 1.04, 95% CI 1.01–1.06, p < 0.005), where a slow performance increased the mean annual length of hospitalizations; d2 total (IRR = 0.80, 95% CI 0.78–0.82, p < 0.001), where a greater number of symbols processed decreased the mean annual length of hospitalizations; d2 type 1 error (IRR = 0.93, 95% CI 0.89–0.97, p < 0.001) and d2 type 2 error (IRR = 0.95, 95% CI 0.94–0.96, p < 0.001), where a higher number of errors decreased the mean annual length of hospitalizations. Besides cognitive tests, increased age also increased the mean annual length of hospitalization age (IRR = 1.04, 95% CI 1.03–1.05, p < 0.001), as well as substance use disorder diagnoses (IRR = 1.09, 95% CI 1.03–1.16, p < 0.01). Low outpatient contact rate was predicted by poor attention (Trail Making Test part A (IRR = 0.95, 95% CI 0.91–0.99, p < 0.05)). A slower performance decreased the mean annual number of outpatient contacts, and d2 type 2 errors (IRR = 0.96, 95% CI 0.93–0.99, p < 0.05). A high number of errors decreased the mean annual number of outpatient contacts.
Predictors of hospital contacts as tested by zero-inflated Poisson regression.
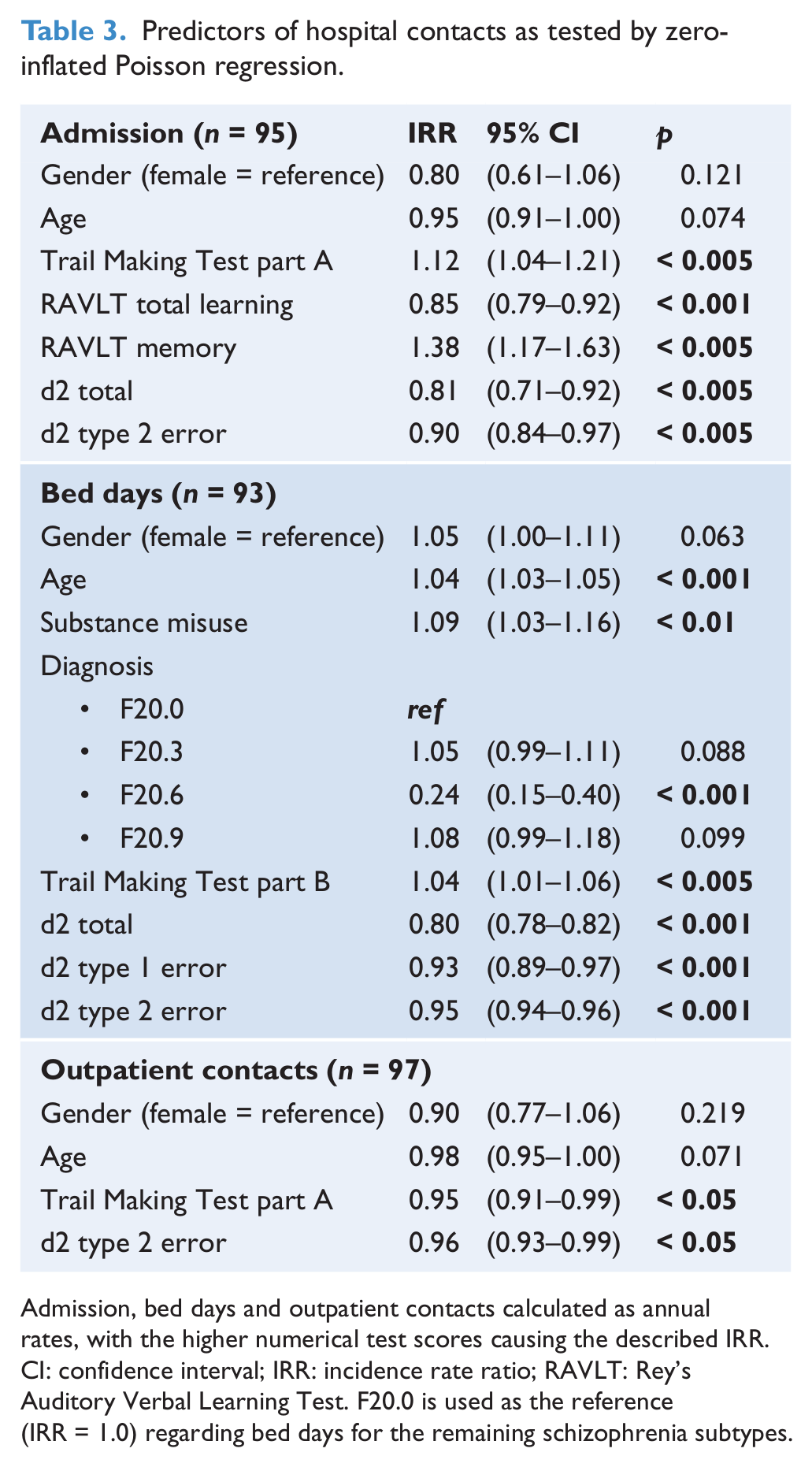
Admission, bed days and outpatient contacts calculated as annual rates, with the higher numerical test scores causing the described IRR.
CI: confidence interval; IRR: incidence rate ratio; RAVLT: Rey’s Auditory Verbal Learning Test. F20.0 is used as the reference (IRR = 1.0) regarding bed days for the remaining schizophrenia subtypes.
Regression analyses were also used to test the effects of candidate variables on annual rates of criminal convictions, institutionalization and social retirement pension and showed that substance use diagnosis increased the risk of a criminal conviction (OR 4.59, 95% CI 1.44–14.62, p < 0.05). Performing well on the digit span forward test was significantly correlated to a decreased risk of being institutionalized (OR = 0.29, 95% CI 0.08–1.00, p < 0.05) (Table 4).
Predictors of demographic variables by logistic regression. Ordered logistic regression was used in determining predictors of age at schizophrenia diagnosis.
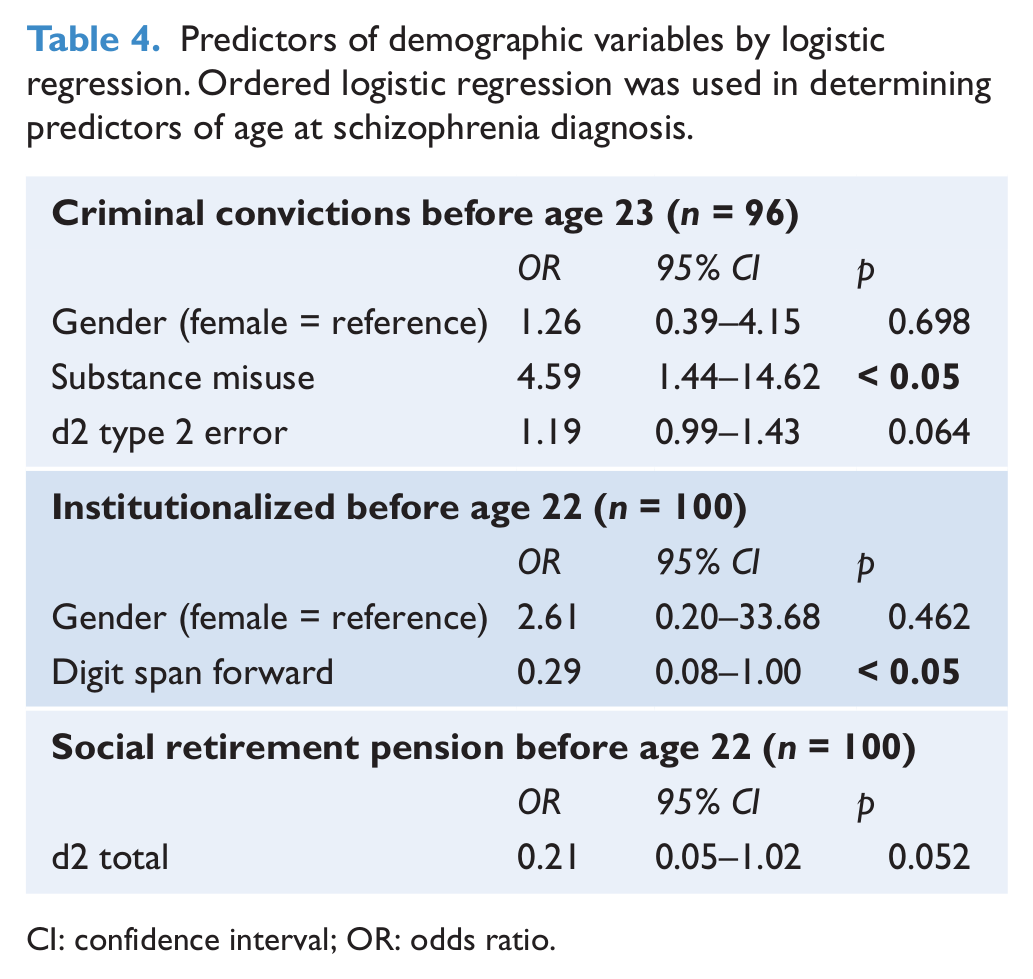
CI: confidence interval; OR: odds ratio.
Discussion
We found that the population, consisting of young patients newly diagnosed with schizophrenia, had cognitive deficits with regard to attention, processing speed, executive functions and memory domains. We also found that cognitive function predicted hospitalization and outpatient contacts to a lesser degree.
Our study population showed poorer performance compared to the norms on the Trail Making Test parts A and B, RAVLT and d2 tests. We did not find any difference in performance on the WCST or Rigshospitalet’s digit span test, perhaps as a consequence of relatively preserved executive function. Another possible explanation is that the norms for the Rigshospitalet’s digit span test date back to 1987. This could partially be due to the so-called Flynn effect, which could explain the finding of no difference compared with norms, contrary to our finding on the RAVLT (Baxendale, 2010). Most cognitive tests were administered to all patients except the WCST, where only 65 of 109 patients were tested. The WCST-tested and WCST non-tested patients were compared, and no significant differences with regards to age at diagnosis, age at testing, schizophrenia subtype specifiers, d2 test, RAVLT test or digit span test were determined. The non-WCST patients were only significantly different on the Trail Making Test parts A and B. It would seem that patients not subjected to the WCST did significantly worse on tests of processing speed and executive function, which suggests an explanation as to their lacking ability to finish the WCST test, as well as our finding of a non-significant difference on WCST between patients and norms.
Another reason for the non-affected cognitive function on some cognitive domains could be selection bias. Patients were tested cognitively as part of their inclusion in the Clinic for Young People with Schizophrenia, and all patients were newly diagnosed with schizophrenia. As a result of this selection, the group would have had fewer psychotic episodes, possibly resulting in a smaller decline of cognitive functioning (Eberhard et al., 2003; Levander et al., 2001).
Regression analysis showed that cognitive function explained some of the variance in risk of admission, length of hospitalization and number of outpatient contacts. The annual risk of admission was linked to poor performance on the Trail Making Test part A, with longer time periods increasing the risk of admission. The RAVLT test was linked with the annual risk of admission outcome measure, with better performance and more words remembered decreasing the risk of admission. Similar results were seen on the d2 total score, with more markers processed linked to decreased number of admission. These findings suggest that processing speed, attention and verbal learning are associated with risk of admission. Other studies have shown similar results (Goldberg et al., 2011; Osler et al., 2007), although these studies were not adjusted for diagnosis and substance use.
Contrary to these findings, we also found that good performance on the RAVLT delayed-recall tests, eg. more words remembered, increased the risk of admission. Additionally, more type 2 errors on the d2 test decreased the risk of admission. The latter could perhaps be explained by the minimal variation in this measure, as shown in Table 2, giving more extreme values a higher predictive value. The counterintuitive results of good RAVLT (total learning) and poor RAVLT memory correlated with lower annual rates of admission, resulting in further analyses. If the group of most frequently admitted patients were excluded from the analyses, we were not able to show a significant correlation to any of the RAVLT scores. So as not to bias our data, all patients were included in the analyses shown.
The length of hospitalization was primarily predicted by schizophrenia subtype specifier, with schizophrenia simplex having a significantly lowered risk of long hospitalization compared to other subtypes of schizophrenia. This finding is perhaps explained by the differences in clinical presentation, where patients diagnosed with schizophrenia simplex are not hallucinating or delusional, but are more severely disturbed by negative symptoms, perhaps thereby decreasing their risk of longer hospitalizations compared to other schizophrenia subtypes. The length of hospitalization was also predicted by age (older patients were hospitalized for a longer time period), substance abuse and some cognitive tests. Poor performance on the Trail Making Test part B increased the length of hospitalization, whereas a good performance on the d2 total test decreased the length of hospitalization. These results corresponded with our findings that attention domains increased the risk of admission. Trail Making Test part B, which measures executive function as well as attention, also predicted the length of hospitalization, with poor performance increasing the duration of hospitalization. As seen in the analysis of admission risk, d2 errors were inversely linked to hospitalization length, with poor performance decreasing the length of hospitalization. The main outcome of the d2 test is the total score, showing attention domain difficulties, whereas the d2 type 1 errors show difficulties with strategy, where increased tempo can decrease performance. With our current data set, we could not ascertain if the increased number of errors is a consequence of problems with strategy or attention.
An increased number of outpatient contacts was predicted by good performance on tests of attention and processing speed, as shown by faster results on the Trail Making Test part A; fewer type 2 errors on the d2 also increased the number of outpatient contacts. The d2 type 2 error has a very low variance and the clinical implications of this result are hard to interpret. Our results on the outpatient contact rate are in agreement with previous studies showing that patients with higher cognitive function have a higher attendance in outpatient treatment (Johansen et al., 2011).
The analyses on criminal convictions showed substance misuse increased the risk of a conviction, with cognitive tests indicating neither an increased nor decreased risk. In the regression analysis of institutionalization we only found a significant correlation with the digit span forward test, with better performance decreasing institutionalization.
Our data show only minor effects of cognitive results on the outcome measures (admission, hospitalization length and outpatient contact) compared to, for example, schizophrenia subtype specifier and substance misuse. All the outcome measures were converted to annual rates to account for individual differences in follow-up time among participants, so the observed IRRs are a result of a mean annual rate, with some patients having an accumulated occurrence of one or several outcomes in parts of the study period. Even though the IRR and OR can seem small, and perhaps clinically meaningless, the risk should be interpreted with the knowledge of outcomes being converted to annual rates. Second, patients’ cognitive test scores were converted to z-scores before the regression analyses, thereby standardizing the distribution of test values. In outcomes with very little variation, for example, d2 type 2 errors, there is a risk of interpreting smaller differences in the regression analyses as being of significance, even though the small differences might not be clinically noteworthy. Our clinical outcomes, for example, the annual rate of admission, length of hospitalization, etc., all have a large variation in our cohort. In a larger study, participants could be subdivided into smaller groups, investigating patients with high, medium or low service use, but due to our small sample size, this was not possible.
Our data was not collected for research purposes, but the cases included in this study were all treated at the Clinic for Young People with Schizophrenia using a standardized protocol for diagnosis, inclusion and follow-up (Bertelsen et al., 2008). The cognitive tests were performed as part of this protocol. Data from the cognitive tests were linked to the extensive Danish registers via a unique personal identifier number (Munk-Jørgensen and Østergaard, 2011). Data on admission, bed days and outpatient contacts were all retrieved from the DPCRR (Mors et al., 2011). The DPCRR was established in 1969 and contains information on all admissions, outpatient contacts and emergency room visits since 1995 (Mors et al., 2011). Data is validated at both the Danish National Patient Register and at the Centre of Psychiatric Research, Risskov, where the register is based (Mors et al., 2011). In this study, we used the individual schizophrenia diagnosis, including the subtype specifier, listed in the DPCRR for descriptive measures (as shown in Table 1), as well as independent variables in the regression analyses. Systematic studies validating the clinical diagnoses in the register against research diagnoses do not exist. However, in several studies some diagnoses, for example, schizophrenia, dementia and single-episode depression, have been validated (Bock et al., 2009; Jakobsen et al., 2005; Löffler et al., 1994; Phung et al., 2007). The substance use disorder diagnosis was also retrieved from the DPCRR and is known to be under-reported, representing only patients with a significant substance use problem (Hansen et al., 2000).
Data on accommodation, education and source of income were all retrieved from the Integrated Database for Labour Market Research (Petersson et al., 2011; Thygesen et al., 2011). This database contains information from several registers, and the validity of each variable depends on the source (Petersson et al., 2011). The key variables in the database are generally considered of high quality, although no validity studies have been conducted (Petersson et al., 2011).
The data on criminal convictions were retrieved from the Danish National Crime Register (Munkner et al., 2009). Judgements made in the Nordic and in the European Council member countries regarding Danish citizens or other people domiciled in Denmark at the time of the crime are registered just like Danish judgements, provided they have been made known to the Danish authorities (Ravn, 2001). The Danish National Crime Register has been described previously as one of the most thorough, comprehensive and accurate crime registers in the world (Munkner et al., 2009). All of the described registers cover all of the people residing in Denmark, and linkage of data from different registers or databases is possible through a unique personal identifier number (Munk-Jørgensen and Østergaard, 2011).
There were some limitations to our study. The cognitive tests were performed for clinical and not research purposes, and not all patients were tested with all cognitive tests. The use of cognitive testing for all patients newly diagnosed with schizophrenia was introduced as a standard procedure in 2006, and as a consequence, not all patients referred to the clinical unit were tested initially. The cognitive tests were not repeated, and we were unable to show stability of cognitive function over time or the inter-rater reliability of the tests. The specific data retrieved on individual patients have not been validated, but the general data quality in the Danish registers is high, as described earlier. Owing to study design, we risked contaminating our results by confounding. In the regression analyses, we did initial univariate analyses and allowed non-significant, independent variables to be included in the multivariate analysis if the results were affected by more than 20%, thereby adjusting for the known variables confounding the results. We were unable to control for confounding variables not retrieved or measured in the study. The current data have only explained part of the total variance seen in risk of admission, length of hospitalization, outpatient contact rates, criminal convictions, risk of institutionalization and risk of social retirement pension. Differences in clinical psychopathology might be of greater importance than cognitive function, as suggested by the correlations between length of hospitalization and schizophrenia simplex. In this study we were unable to investigate these correlations, as we did not have access to clinical ratings of positive, negative, affective or aggressive symptoms from our participants.
Conclusions
This study showed that cognitive function was decreased compared to norms in our group of newly diagnosed patients with schizophrenia, and that cognitive function, to a smaller degree, predicted admission, length of hospitalization, outpatient contacts and risk of institutionalization.
Footnotes
Acknowledgements
We thank Michael F Green for discussing the project, as well as reading and commenting on the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
R.Ernst Nielsen has received research grants from H. Lundbeck for clinical trials, speaking fees from Bristol-Myers Squibb, AstraZeneca, Janssen-Cilag, Lundbeck and Servier, and has acted as advisor to AstraZeneca and Otsuka Pharmaceutical Group. P. Munk-Jørgensen has previously received grants from Wyeth (now Pfizer), Lundbeck, Bristol-Myers Squibb, Janssen-Cilag, AstraZeneca and Servier, although he has nothing to declare since October 2009.