
Abstract
Objective:
Cognitive remediation therapy is a moderately effective intervention for ameliorating cognitive deficits in individuals with schizophrenia-related disorders. With reports of considerable variability in individual response to cognitive remediation therapy, we need to better understand factors that influence cognitive remediation therapy efficacy to realise its potential. A systematic review was conducted to identify and evaluate predictors of cognitive outcome.
Methods:
An electronic database search was conducted identifying peer-reviewed articles examining predictors of cognitive response to cognitive remediation therapy.
Results:
A total of 40 articles accounting for 1681 cognitive remediation therapy participants were included; 81 distinct predictors of cognitive response were identified. Data synthesis and discussion focused on 20 predictors examined a minimum three times in different studies. Few of the examined predictors of cognitive outcome following cognitive remediation therapy were significant when examined through systematic review. A strong trend was found for baseline cognition, with reasoning and problem solving and working memory being strongly predictive of within-domain improvement. Training task progress was the most notable cross-domain predictor of cognitive outcome.
Conclusion:
It remains unclear why a large proportion of participants fail to realise cognitive benefit from cognitive remediation therapy. However, when considering only those variables where a majority of articles reported a statistically significant association with cognitive response to cognitive remediation therapy, three stand out: premorbid IQ, baseline cognition and training task progress. Each of these relates in some way to an individual’s capacity or potential for change. There is a need to consolidate investigation of potential predictors of response to cognitive remediation therapy, strengthening the evidence base through replication and collaboration.
Introduction
Impaired cognitive functioning is a core aspect of schizophrenia experienced by around 75% of those so diagnosed (Heinrichs et al., 2013). Cognitive deficits manifest across a broad range of domains (Schaefer et al., 2013) and have been associated with poorer functional outcomes in areas such as vocational and educational pursuits, independent living and community and social relations (Bowie et al., 2008; Fett et al., 2011; Green, 1996; Strassnig et al., 2015). In the absence of approved pharmacotherapies (Opler et al., 2014), there has been an acceleration of research investigating the efficacy of cognitive remediation therapy (CRT) in ameliorating cognitive deficits with the aim of improving functional outcomes. Meta-analyses quantifying the efficacy of CRT have reported small-to-moderate effect sizes, but have been unable to account for the heterogeneity detected across multiple cognitive domains (Grynszpan et al., 2011; d = 0.38; McGurk et al., 2007; d = 0.41; Revell et al., 2015; d = 0.13; Wykes et al., 2011; d = 0.45).
Available evidence regarding rates of reliable change following CRT indicates that approximately 44% 1 of participants fail to realise a cognitive benefit (Bryce et al., 2018; Choi and Medalia, 2005; Hodge et al., 2010; Lindenmayer et al., 2017; Medalia et al., 2001; Medalia and Richardson, 2005; Penadés et al., 2006; Vita et al., 2013; Wykes et al., 1999). Such variability in response has the potential to undermine the effectiveness of CRT in real-world settings. To enable a more nuanced matching of individual needs and capacity for change to the most appropriate CRT tool, there is a need to better understand the factors that influence individual response to, and in turn the efficacy of, CRT (Vinogradov et al., 2012).
Efforts to identify factors that influence the efficacy of CRT have had limited success. McGurk et al. (2007; 26 studies; 1151 participants), Grynszpan et al. (2011; 16 studies; 805 participants) and Wykes et al. (2011; 40 studies; 2104 participants) each examined potential moderators of cognitive outcome in their respective meta-analyses. Collectively, neither key methodological, participant or treatment effects were found. McGurk et al. found that increased training hours and treatment approach (i.e. use of drill and practice) appeared to confer a greater benefit in the verbal learning and memory domain. Wykes et al. found that lower baseline psychotic symptoms influenced outcome, though poorer clinical presentation did not prevent improvements in global cognition. In their narrower examination of first episode psychosis, Revell et al. (2015; 11 studies; 615 participants) found that greater improvements in global cognition were realised in studies where more than 66% of participants were male. However, the primary objective of these meta-analyses was to evaluate the efficacy of CRT. Moderator analysis was undertaken to examine between-study variability only where heterogeneity was detected and did not consider the range of variables that have been investigated in the wider literature. In the absence of participant data, these meta-analyses failed to account for differential responses within respective study cohorts and excluded potentially rich sources of data in the form of single-arm trials and secondary analyses exploring predictors of outcome.
Review articles are free from these constraints, and several have touched on the purported predictors and moderators of cognitive response to CRT (Cellard et al., 2011; Kaneko and Keshavan, 2012; Keshavan et al., 2014; Kurtz, 2012; McGurk et al., 2013; Wykes and Spaulding, 2011). Common themes to emerge include participant age, symptom stability, baseline cognition, motivation and genetic influence.
To our knowledge, no systematic review of the CRT evidence base has been conducted to provide this broader view. Moreover, with an acceleration of secondary predictor analysis over the last 5 years, there is no current, comprehensive synthesis of the literature that can be used to inform clinical decision-making or to guide future research in this important field.
Aims of the study
With a focus on cognitive response to CRT in individuals diagnosed with schizophrenia, we aimed to (1) provide a systematic review of the predictor literature, (2) bring the field up-to-date by considering publications up to and including September 2017 and to (3) evaluate the quality of the evidence at a predictor level. We considered moderators, mediators and predictors (significant main effect) of cognitive outcome (Kraemer, 2016) and, where examined, factors that differentiated subgroups of responders compared to non-responders. These are all factors that influence individual response to, and therefore the efficacy of, CRT and are collectively referred to as ‘predictors’ of response or cognitive outcome. We limited the scope of the review to studies where CRT was the sole intervention, excluding those that incorporated such adjunctive therapies as social cognition/skills training and vocational rehabilitation.
Methodology
Search strategy
Methods of the analysis and inclusion criteria were informed by Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA; Liberati et al., 2009) and registered with PROSPERO (https://www.crd.york.ac.uk/prospero/CRD42016037400). Studies were identified through electronic database searches and by examining reference lists of published meta-analyses and review articles. Search terms ‘cognitive training’ OR ‘cognitive remediation’ OR ‘cognitive rehabilitation’ OR ‘cognitive enhancement’ AND ‘schizophrenia’ AND ‘predictor*’ OR ‘mediator*’ OR ‘moderator*’ were applied to Scopus, Web of Science and PsycINFO databases and Cochrane Collaboration Controlled Trials Register for all years until 30 September 2017. As the examination of predictor variables is often exploratory and not directly referred to in article titles and abstracts, we also hand searched articles that had been identified in preparation for another manuscript using search terms ‘cognitive training’ OR ‘cognitive remediation’ OR ‘cognitive rehabilitation’ OR ‘cognitive enhancement’ AND ‘schizophrenia’ AND ‘randomized’ OR ‘clinical trial’ OR ‘randomly assigned’ for the period 2009 to 30 September 2017 across the above-mentioned databases. Finally, articles comprising the most recent meta-analyses (Grynszpan et al., 2011; Revell et al., 2015; Wykes et al., 2011) were manually reviewed for evidence of covariate and/or post hoc analysis.
Study selection
Search outputs were collated in spreadsheet format. Duplicates were removed, and articles not published in English excluded. Eligibility assessment was performed independently in an unblinded standardised manner by two reviewers, M.P.R. and R.S. Inclusion criteria were (1) peer-reviewed article; (2) randomised controlled trial (RCT), or single-arm trial, or retrospective review of such; (3) majority (⩾70%) participants diagnosed with schizophrenia/schizoaffective disorder; (4) inclusion of CRT treatment arm as defined by the Cognitive Remediation Expert Working Group (2012; as referenced by McGurk et al., 2013); (5) at least one pre- and post-intervention measure of cognition that was independent of the cognitive training tasks and (6) analysis of at least one predictor/determinate of cognitive outcome. Studies that included social cognition/skills training and/or parallel rehabilitation activities (i.e. not treatment as usual activities outside of study control), such that the specific effects of each could not be distinguished, were excluded. Initial screening focused on article titles and abstracts; for the remaining records, full articles were considered. Review results were coded, cross-tabulated, with disagreements resolved by consensus and/or consultation with a third party.
Data extraction and analysis
The first author extracted resultant study data into a spreadsheet template. Data included participant characteristics for CRT trial arm, study and intervention details, predictor and outcome measures, statistical methods and summary of pertinent results. Predictor summary information was collated by category (i.e. demographics, clinical presentation, baseline cognition). If an article reported both post-intervention and follow-up data, post-intervention results informed our discussion.
A meta-analysis was not conducted for two reasons. First, we combined data obtained from multiple study designs, including RCTs, RCTs with multiple treatment arms and no control, quasi-RCTs, single-arm trials and retrospective studies that included only the treatment arm or that combined single-arm trial results with treatment arm results. Second, for a majority of included predictors, we had insufficient data to support subgroup or meta-regression analysis within a meta-analytic framework. To enhance the otherwise narrative review, a box-score analysis of predictor variables was conducted (Green and Hall, 1984). To complete the box-score analysis, for each article, a list of predictor variables and cognitive outcome domains was compiled. At a summary level, if a predictor was statistically significantly associated with any of the cognitive outcome domains examined, it was coded as ‘+’ to denote positive associations or ‘−’ to denote negative associations (no mixed associations were found). If no statistically significant associations were found, be that using correlations, analysis of covariance, regression or modelling techniques, it was coded as ‘0’. If multiple analytic techniques were used, for example, correlations followed by regression, results from the final confirmatory analysis were reported. This process was repeated at a cognitive domain level. Predictor variables have been grouped by category to aid interpretation. Summary scores have been reported according to whether analysis was conducted at a Total Sample or CRT Subgroup level. These are mutually exclusive categories that when summed reflect the total number of articles to examine the predictor variable.
To further increase the rigour of the review, the quality of the predictor evidence was assessed by the first author (M.P.R.). Criteria developed by a consensus group of 21 international experts to allow for the ‘grading of evidence for moderators’ within systematic reviews of RCTs were applied (Pincus et al., 2011: 2). Specifically, consideration was given to whether (1) a priori hypothesis framed the research, (2) the research was theory driven or evidence based, (3) predictor variables were measured pre-randomisation, (4) measures were valid and (5) there was a direct test of interaction. Details regarding how each criterion was assessed have been included in Supplementary Table 3. Where a criterion was not applicable, for example, conducting assessments prior to randomisation in single-arm trials, the overall rating was adjusted accordingly.
Consideration of the methodological issues associated with systematic reviews and subgroup analysis encouraged caution regarding interpretation of the results and conclusions drawn (Bender et al., 2008; Lagakos, 2006).
Results
In all, 40 articles, considering 2652 study participants, of whom 1681 received CRT, were included in the final review. Figure 1 presents the flow of studies through the selection process. Two articles were combined due to examination of the same predictors at different time points (Choi and Medalia, 2010; Choi et al., 2010) as were another two articles due to them being different treatment arms on the same study examining the same covariates (Medalia et al., 2000, 2001). A total of 16 articles involved secondary analysis of either one (12 articles) or multiple (4 articles) trials, resulting in some overlap of study cohorts. An additional two were follow-up extensions of Fisher et al. (2009, 2010, 2016). With such secondary analysis encouraged (Furberg and Friedman, 2012), overlapping study cohorts were included where distinct predictors were examined. Where a cohort/predictor overlapped, it was included once in the box-score analysis and subsequent discussion. This occurred on four occasions – Fisher et al. (2015) and Biagianti et al. (2016) who were examining task engagement/progression; Wykes et al. (2007a, 2007b) and Greenwood et al. (2011) examining medication type; Twamley et al. (2011) and Burton et al. (2015) examining premorbid IQ and ethnicity and Reeder et al. (2017) and Cella and Wykes (2017) who both examined the average number of tasks completed per session – with consistency of reported associations. Also excluded from graphic and narrative summaries was Medalia and Richardson (2005) examination of baseline symptoms, due to contradictory reporting, and Penadés et al.’s (2016) examination of baseline symptoms, due to lack of clarity around which subscales were used. On both occasions, no association was found with cognitive outcomes. Other predictor variables examined by these authors were included.
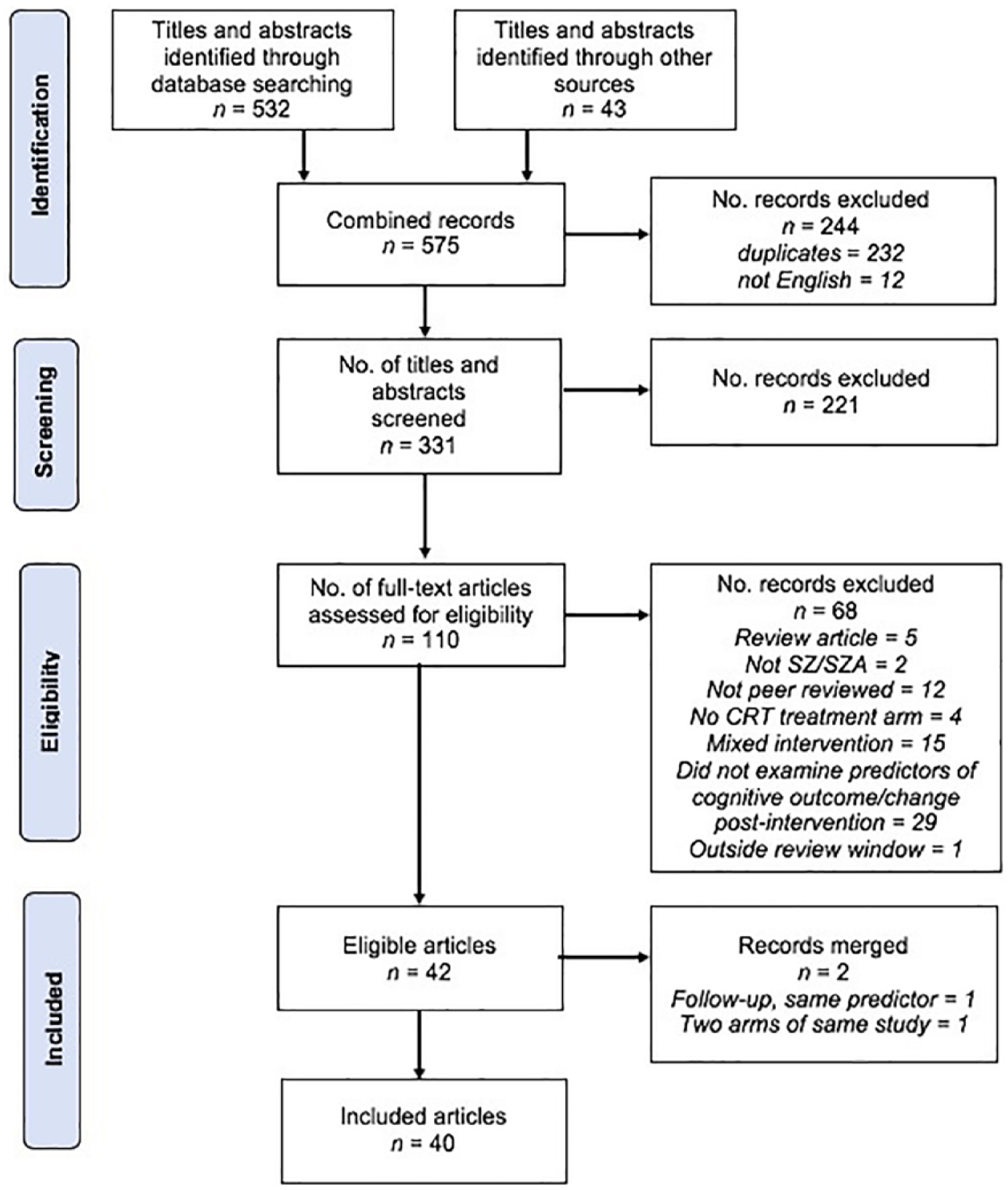
PRISMA flow diagram of article selection process.
Study characteristics
A summary of participant and treatment characteristics for the CRT arm of included articles is provided in Table 1. Participant characteristics were similar to those reported in the Wykes et al. (2011: 474) meta-analysis, being individuals aged in their mid-30, majority of males, with approximately 12 years of education. CRT trial arm size averaged 43 participants (range = 10–131). A total of 15 different core treatment/training programmes were considered: 8 articles used Posit Science’s auditory/visual training, 7 articles Delahunty and Morice’s (1993) CRT, 5 articles CogPack (and once in combination with another treatment), 3 articles each NEAR and Compensatory Cognitive Training and 2 articles each REPYFLEC and CIRCuiTS. CogRehab was used alone once and in combination twice.
Summary characteristics of included articles for CRT trial arm.
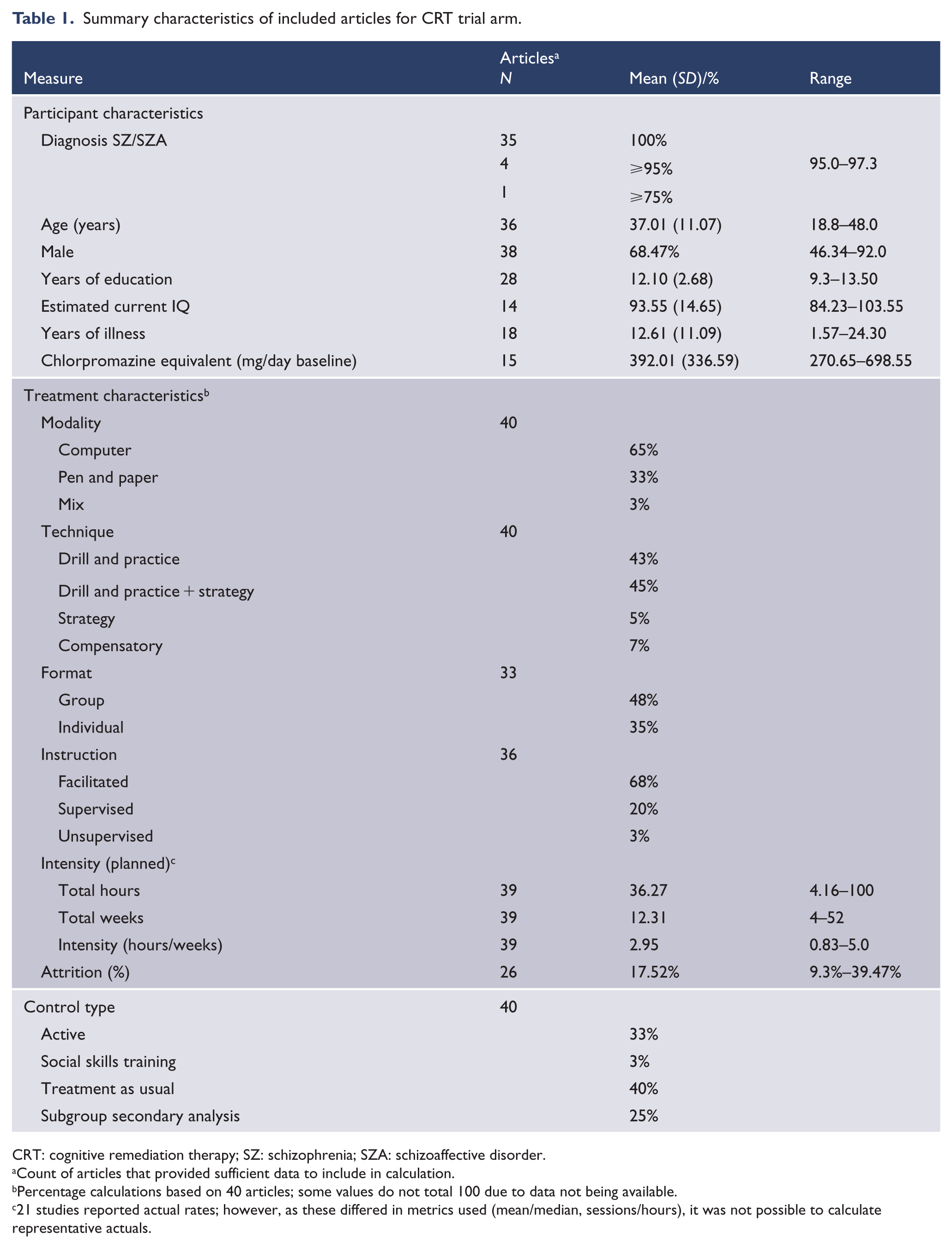
CRT: cognitive remediation therapy; SZ: schizophrenia; SZA: schizoaffective disorder.
Count of articles that provided sufficient data to include in calculation.
Percentage calculations based on 40 articles; some values do not total 100 due to data not being available.
21 studies reported actual rates; however, as these differed in metrics used (mean/median, sessions/hours), it was not possible to calculate representative actuals.
Computer-based programmes predominated, and a majority of the programmes were facilitator led across a mix of group and individual formats. Treatment programmes varied in duration and intensity; treatment sessions ranged from 25 to 120 minutes and were delivered one to five times a week. Supplementary Table 1 provides at the article level, participant characteristics, active and control treatment details, a full list of predictor variables and a summary of cognitive outcome domains. Supplementary Table 2 details statistical methodology and pertinent variable-level results.
Predictor characteristics
Twenty-nine articles declared an intention to examine at least one predictor of response (Table 2). Of these, seven examined the influence of catechol-O-methyltransferase (COMT) polymorphisms on cognitive outcome, six with a specific focus on single nucleotide polymorphism rs4680. Three articles planned examination of a broad range of predictors of response. Four looked more specifically at whether training task progress predicted response, though only three were included in predictor summary tables due to the aforementioned overlapping predictor/cohort. Two articles each examined the influence of symptoms, age, cognitive insight and training dose. Single articles examined the influence of anticholinergic burden, correlates with cortical thickness, intrinsic motivation, serum brain-derived neurotrophic factor (BDNF) levels, early versus later course of illness and specific versus general cognitive training. The remaining articles conducted covariate or post hoc predictor analysis, at times incorporating the above-mentioned predictors.
Author list with corresponding predictor focus and count of predictors and cognitive domains examined.
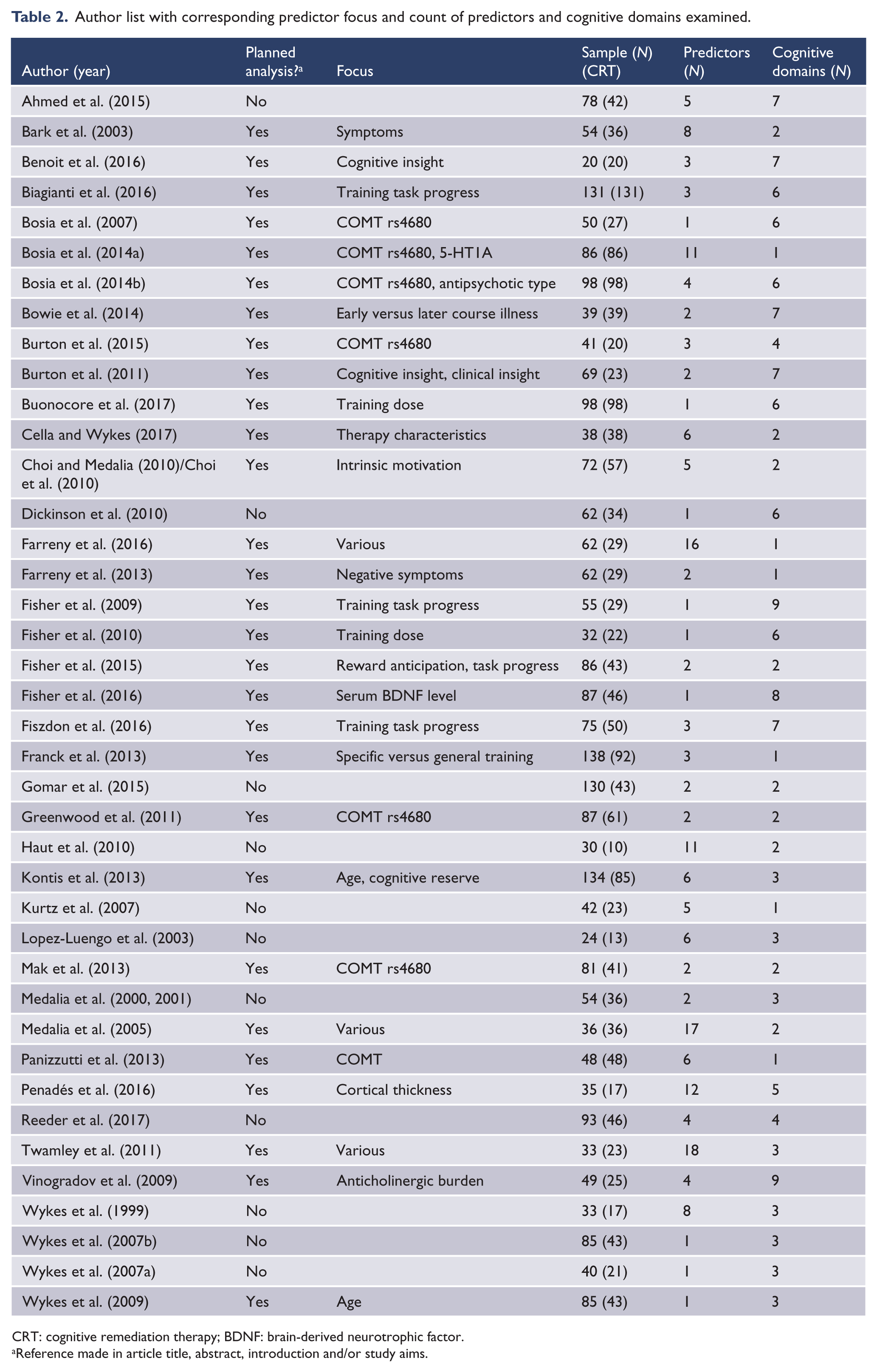
CRT: cognitive remediation therapy; BDNF: brain-derived neurotrophic factor.
Reference made in article title, abstract, introduction and/or study aims.
An average of 4.8 predictor variables (range = 1–18) were considered across an average of 3.95 cognitive domains per article (range = 1–9). Nine articles (Bark et al., 2003; Farreny et al., 2016; Haut et al., 2010; Kurtz et al., 2007; López-Luengo and Vázquez, 2003; Medalia and Richardson, 2005; Penadés et al., 2016; Twamley et al., 2011; Wykes et al., 1999), using a mix of correlational, analysis of (co)variance and regression techniques, had less than 5 participants per predictor. Overall, 81 distinct predictors of cognitive response were identified; 24 clinical, 12 each baseline cognition and treatment characteristics, 10 participant characteristics, 8 genetic, 7 demographic details, 5 subgroup (e.g. younger vs older age group), 2 baseline functioning and 1 cortical; 50 predictors were analysed once and 11 were analysed twice. Our discussion focuses on the 20 (25%) predictors that were examined a minimum three times in different studies, with age group considered alongside the continuous variable ‘age’. Information regarding predictors examined less than three times is available in Supplementary Figure 1.
There was little consistent evidence regarding associations between predictor variables and cognitive outcome measures (see Figure 2 and Table 3). Of the articles that examined the influence of ethnicity, sex, diagnosis (schizophrenia vs schizoaffective disorder), antipsychotic dose and number of hospitalizations, there were no associations found. The opposite was true for training task progress and age group, where each article reported significant associations. The prognostic value of the balance of the predictors varied in strength. The influence of age on cognitive outcome was the most frequently examined association (17 studies). Of the predictor category groupings, the strongest trends towards an association were found in specific baseline cognitive domains, with reasoning and problem solving (R-PS; five positive associations) and working memory (WM; two out of three associations were positive) domains being more strongly predictive of within-domain improvements and in premorbid IQ. Training task progress was the most notable cross-domain predictor of cognitive outcome. We also examined potential interactions between CRT efficacy and the association between predictor variables and outcome domains. No such association was found.
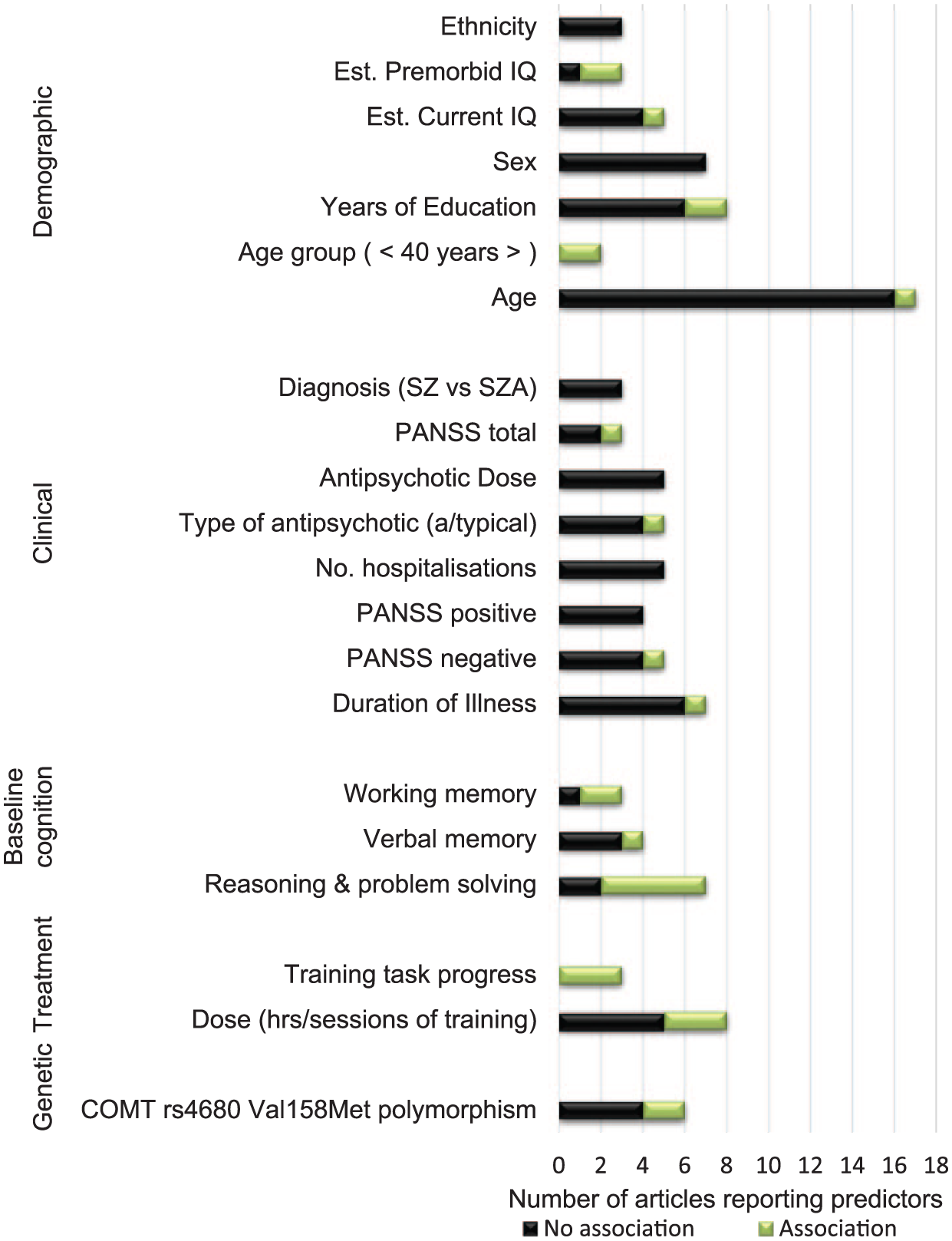
Horizontal bar graph showing count of articles that examined predictors of cognitive response to cognitive remediation therapy, grouped by category.
Box-score review of predictors of cognitive response to cognitive remediation therapy (CRT) at summary and cognitive domain level.
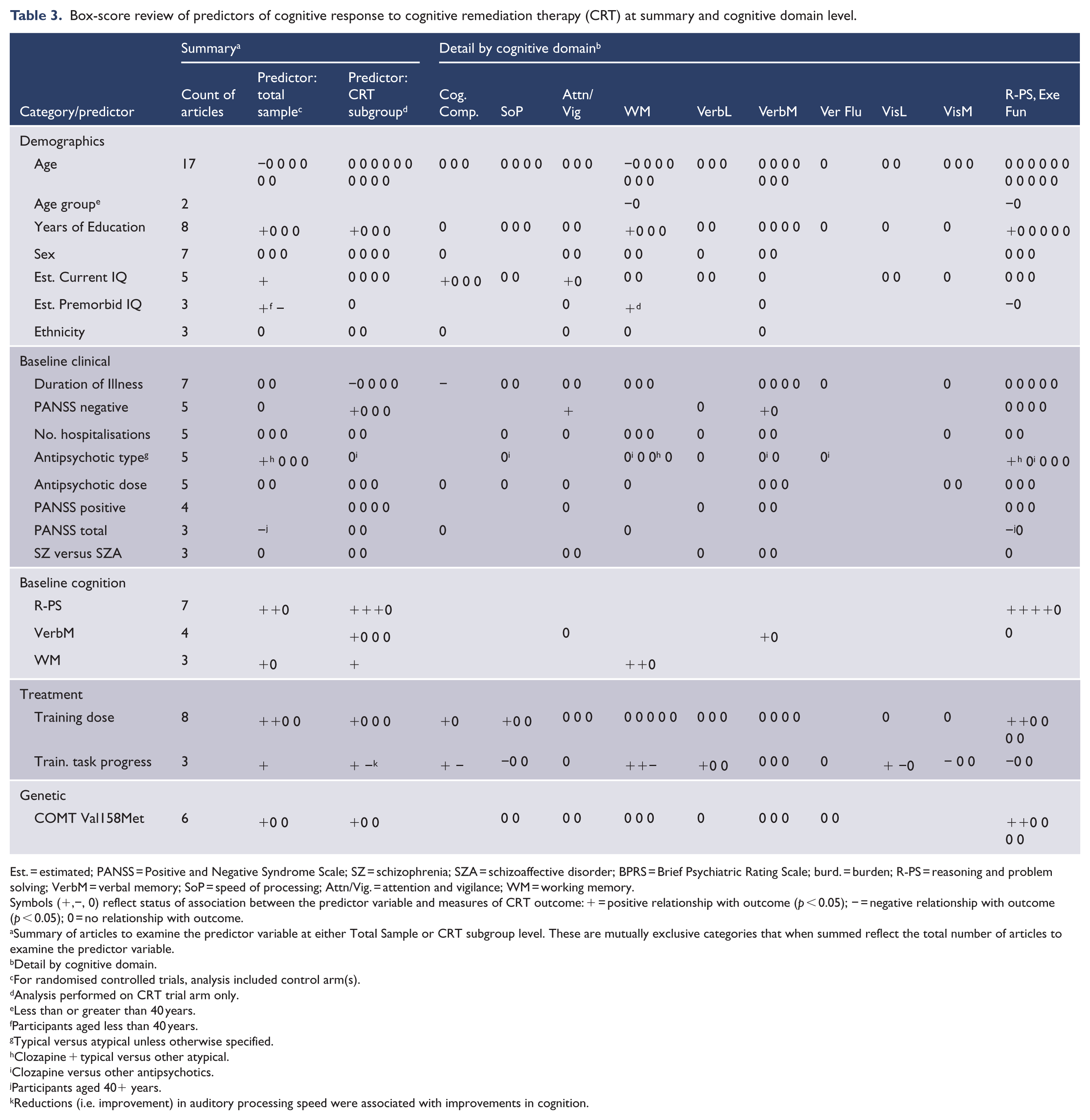
Est. = estimated; PANSS = Positive and Negative Syndrome Scale; SZ = schizophrenia; SZA = schizoaffective disorder; BPRS = Brief Psychiatric Rating Scale; burd. = burden; R-PS = reasoning and problem solving; VerbM = verbal memory; SoP = speed of processing; Attn/Vig. = attention and vigilance; WM = working memory.
Symbols (+,−, 0) reflect status of association between the predictor variable and measures of CRT outcome: + = positive relationship with outcome (p < 0.05); − = negative relationship with outcome (p < 0.05); 0 = no relationship with outcome.
Summary of articles to examine the predictor variable at either Total Sample or CRT subgroup level. These are mutually exclusive categories that when summed reflect the total number of articles to examine the predictor variable.
Detail by cognitive domain.
For randomised controlled trials, analysis included control arm(s).
Analysis performed on CRT trial arm only.
Less than or greater than 40 years.
Participants aged less than 40 years.
Typical versus atypical unless otherwise specified.
Clozapine + typical versus other atypical.
Clozapine versus other antipsychotics.
Participants aged 40+ years.
Reductions (i.e. improvement) in auditory processing speed were associated with improvements in cognition.
Quality of predictor evidence base
Assessment of the quality of the predictor evidence is presented in Supplementary Table 3. Of the more frequently examined potential predictors of cognitive response, few were theory driven or evidence based and fewer were undertaken with a priori hypotheses. A majority of predictor variables were said to be measured pre-randomisation and the validity and reliability of primary measures of cognitive outcome were largely acceptable, with most studies using neuropsychological tests and test batteries previously vetted in the Wykes et al. (2011) meta-analysis or assessed as appropriate for cognitive assessment in schizophrenia (Bakkour et al., 2014). However, few analyses included tests of interaction. While not included in the summary, only eight articles reported having accounted for multiple comparisons.
Predictor results by category
Demographics
Estimated premorbid IQ
Evidence regarding the influence of estimated premorbid IQ on cognitive outcome was complicated by contrary associations across domains. Performing subgroup analysis, Kontis and colleagues (Kontis et al., 2013) reported that the association was limited to participants aged under 40 years, with higher premorbid IQ, dichotomised at the median, and positively associated with WM improvements. When re-analysed as a continuous variable across the full sample, higher premorbid IQ was positively associated with both WM and R-PS-planning improvements. Franck et al. (2013) reported a different pattern of association, with higher premorbid IQ associated with less post-intervention improvement on R-PS. Twamley et al. (2011) found no correlates with attention/vigilance (Attn/Vig), prospective memory, verbal learning or verbal memory domains (VerbL, VerbM) when examining CRT completers. Inconsistencies across domains examined and level of analysis (total sample, subgroup x age, subgroup x completers), along with methodological concerns regarding the use of dichotomies in regression (Royston et al., 2006), preclude further interpretation.
Estimated current IQ
Less support was found for estimated current IQ as a predictor of response, with only one of the five articles reporting an association. Ahmed et al. (2015) reported that current IQ predicted improvement in attention and a cognitive composite. Two other articles that examined the influence of current IQ on a cognitive composite found no association, though Panizzutti et al.’s (2013) study cohort overlapped with that of Vinogradov et al. (2009) when pooling data from two RCTs. Neither Bosia et al. (2014a) or Benoit et al. (2016) found current IQ to influence cognitive response to CRT.
Years of education
Years of education has been examined across a broad range of cognitive domains, with two of eight articles reporting an association with cognitive outcomes. The positive correlation reported by Haut et al. (2010) with an untrained WM task (r = 0.32, n = 21, p = 0.22) was weak and not significant. They reported no association with a lexical decision task. In modelling performed by Bosia et al. (2014a), a relationship was found between years of education and R-PS (F = 5.04, p = 0.033), though it was unclear how much of the variance was explained. No association was reported by this group when conducting similar analysis examining a measure of attention across another sample (Bosia et al., 2014b). The weight of evidence suggests that years of education exerts little influence on cognitive response to CRT (Ahmed et al., 2015; Farreny et al., 2016; Medalia et al., 2000, 2001; Penadés et al., 2016; Twamley et al., 2011).
Age
When considered as a continuous variable, a majority (n = 16) found no association between age and cognitive outcome. This was true even for the more rigorous studies with larger sample sizes using statistical modelling (Biagianti et al., 2016; Bosia et al., 2014a, 2014b; Dickinson et al., 2010) with tests of interaction (Franck et al., 2013).
Two subgroup analyses failed to clarify the role of age on cognitive outcome. Interpretation is, however, limited by methodological concerns. In overlapping sample cohorts, Kontis et al. (2013) and Wykes et al. (2009) applied a somewhat arbitrary dichotomisation of age, being those aged less than or greater than or equal to 40 years, in part to ‘achieve relatively balanced sample sizes’ (Wykes et al., 2009: 254). Dichotomisation results in a loss of both information and power (Royston et al., 2006). Moreover, Kontis et al.’s use of multiple dichotomies (age, premorbid IQ, vocabulary, cognitive reserve) across multiple, unadjusted regression analyses significantly increased the risk of spurious findings (Lagakos, 2006). Wykes et al. reported that CRT improved WM in both age groups; however, only younger participants improved post-intervention on R-PS-planning. No effect was found on R-PS-cognitive flexibility. In comparison, Kontis et al. reported that CRT improved WM in younger but not older participants. No effect was found for cognitive flexibility and planning aspects of R-PS. When Kontis et al. examined age as a continuous variable, increased age was associated with poorer post-intervention WM, independent of treatment.
Baseline clinical
Regarding clinical predictors of cognitive response to CRT, neither diagnosis (schizophrenia vs schizoaffective disorder), number of hospitalisations, nor antipsychotic dose was found to influence outcome.
Duration of illness
One of seven articles found an association between duration of illness and cognitive outcome. Analysing a sample of convenience comprising early versus long-term course of illness, Bowie et al. (2014) reported a negative relationship between duration of illness (range = 1–43 years) and improvement on a cognitive composite (r = −0.43, n = 39, p = 0.001). It is not clear whether the absence of any other reported associations (Bosia et al., 2014a; Farreny et al., 2016; Kurtz et al., 2007; López-Luengo and Vázquez, 2003; Penadés et al., 2016; Twamley et al., 2011) is due to there being less variability in illness duration as there was limited reporting of range of illness duration. Using age as a proxy for duration of illness, it is possible that Farreny et al. (2016, age range = 18–60 years) and Twamley et al. (2011, age range = 21–69) approximated the variability engineered by Bowie and colleagues with no reported associations in these two studies.
Medication type
One of five articles found that medication type influenced outcome, with the use of either clozapine or typical medication conferring a benefit on R-PS-planning not apparent in those taking other atypical medications (Wykes et al., 2007b). No effect was found on measures of WM or R-PS-cognitive flexibility, and the authors noted that participants taking Clozapine had more room for improvement, having a lower baseline planning score (Wykes et al., 2007b). Where clozapine was compared with other antipsychotics (Bosia et al., 2014) or where typical were compared to atypical antipsychotics (Medalia et al., 2000, 2001; Wykes et al., 1999, 2007a), no effect was found.
Baseline psychotic symptoms
The majority of articles reported no association between baseline symptoms and CRT cognitive outcomes. Eleven articles examined the predictive role of baseline symptoms, of which nine were included in the box-score analysis. Comparisons were facilitated by frequent use of Positive and Negative Syndrome Scale (PANSS; Kay et al., 1987) subscale or factor scores, with Haut et al. (2010) and Wykes et al. (1999) using the Brief Psychiatric Rating Scale (BPRS; Overall and Gorham, 1962). Kontis et al. (2013) reported that for both older adults and the full sample, higher overall symptomatology (PANSS total) was associated with less improvement in R-PS-planning; no association was found with R-PS-cognitive flexibility or WM. Two additional articles that analysed PANSS total (Bosia et al., 2014a; Vinogradov et al., 2009), and two that examined BPRS total score (Haut et al., 2010; Wykes et al., 1999), found no associations with cognitive outcomes. No associations were reported between positive symptoms and cognitive outcomes in four articles (Bark et al., 2003; Bosia et al., 2014a; Farreny et al., 2016; Twamley et al., 2011). Conversely, Twamley et al. (2011) found that higher PANSS negative symptom scores were correlated with greater improvements on measures of Attn/Vig and VerbM but not prospective memory. Bosia et al. (2014a) also reported a correlation between PANSS negative and cognitive outcome (R-PS); however, it did not emerge as a predictor when included in general linear model analysis. Farreny et al. (2016) similarly found correlations (p < 0.10) between R-PS and PANSS factors (positive, excited, disorganised) that were not predictive when considered in regression analysis. Neither Bark et al. (2003) or Farreny et al. (2013), who sought to better understand the interaction between symptoms and treatment response, found symptoms to be predictive of cognitive response to CRT.
Baseline cognition
Nine articles examined the influence of baseline cognition on cognitive response to CRT, with a majority focused on within-domain response (i.e. pre-intervention value predicting the corresponding post-intervention value). R-PS was the most frequently examined baseline predictor and had the strongest association with outcome. Biagianti et al. (2016), Bosia et al. (2014a), Farreny et al. (2016) and Kontis et al. (2013) all reported positive associations, with higher baseline R-PS predicting greater within-domain improvement. This was irrespective of measure or CRT programme. The two articles that did not replicate these results used more stringent measures of effective change, calculating either reliable change indices (RCI) that accounted for practice effects and measurement error (Medalia and Richardson, 2005) or improvement thresholds that required a minimum 50% of within-domain measures to have improved at least one standard error of the sample’s test baseline score (Wykes et al., 1999).
Of the other cognitive domains, a strong positive trend was also evident in WM (Biagianti et al., 2016; Kontis et al., 2013), though contrary results were reported by Wykes et al. (1999) when considering a more clinically rigorous improvement threshold. The opposite pattern emerged on measures of VerbM, with a majority of articles not finding baseline VerbM predictive of within-domain change (Farreny et al., 2016; Medalia and Richardson, 2005; Twamley et al., 2011). On finding that increased training hours and a drill and practice approach were associated with improvements in verbal learning and memory, McGurk et al. (2007) hypothesised that the domain might be more sensitive to the method and length of treatment. Indeed, the only article in this review to report a positive association between baseline and VerbM outcome was Biagianti et al. (2016) in a pooled sample of 131 participants engaged in 40 hours of targeted drill and practice auditory training. In comparison, Farreny et al. (2016) analysed results from 29 participants engaged in a strategy-based CRT programme, Medalia and Richardson (2005) applied a stringent RCI to a 5-hour intervention involving 36 participants, and Twamley et al. (2011) analysed 23 completers who completed 24 hours of compensatory training.
Treatment
Treatment dose
Three of eight articles found that treatment dose, being the number of hours trained or sessions attended, influenced cognitive response to CRT. This was most apparent in studies that compared groups who differed in length of treatment. For example, Fisher et al. (2010) examined the differential responses of participants who received either 50 or 100 hours of targeted cognitive training. While both groups improved on VerbL, VerbM and R-PS, extended training conferred additional benefit in speed of processing (SoP) and cognitive composite. A change from auditory to visual training across the two 50-hour blocks meant it was unclear what combination of training dose and spectrum of training conferred the reported benefit. However, support was recently found in a study that compared the differential effect of 3 months (36 sessions) compared to 6 months (72 sessions) of the same CRT protocol (Buonocore et al., 2017). Buonocore et al. (2017) reported that both groups improved across VerbM, WM, verbal fluency (VerbF), SoP and R-PS domains; however, greater improvements were realised in R-PS by the group to receive 6 months CRT. From this, Buonocore et al. concluded that 36 sessions appeared sufficient to confer maximal benefit in a majority of domains, with little further benefit realised after 3 months training.
Of the six studies to examine the association between number of sessions completed and cognitive outcome, only one reported a significant association. Reeder et al. (2017) reported that number of sessions completed correlated with improvements in R-PS; study completers, being participants who completed a minimum of 20 sessions, averaged 27.5, 45-minute sessions (range = 20–41). Of the five articles to find no association, Farreny et al. (2016) reported a median (range) of 26 (20–32) sessions attended across 16 weeks, while López-Luengo and Vázquez (2003) reported a range of 19–90 sessions attended across 8–76 weeks. Kurtz et al. (2007) reported mean (SD) training hours of 67.4 (28.7) for the CRT group, with the large SD indicating greater variability around the mean. There was minimal variability in training dose reported by Ahmed et al. (2015; mean = 48.40, SD = 4.11). Twamley et al. (2011) reported the lowest training dose, with an average attendance of 10.6–12.0 sessions.
Training task progress
There is strong evidence of an association between training task progress, that is, evidence of improvement on CRT tasks and cognitive response to CRT. Of the earliest studies to investigate this association, Fisher et al. (2009) reported that improvement on a trained auditory processing task predicted post-intervention improvements across WM-verbal and cognitive composite. More recent analysis has explored underlying mechanisms of action. Biagianti et al. (2016) pooled results from three RCTs delivering 40 hours of computer-based auditory training to examine the relationship between auditory processing speed (APS) and cognitive outcome. They reported that, after controlling for baseline cognition, faster APS at the point of APS plateau (i.e. the point after which gains no longer manifest) predicted improvements across cognitive composite, WM-visual and verbal, visual learning (VisL), visual memory (VisM), SoP and R-PS domains (Biagianti et al., 2016). Fiszdon et al. (2016) have also explored mechanisms of treatment effect, examining the interaction between progress on PSSCogRehab training tasks and cognitive response to CRT. Improvements on training tasks correlated with improvements in VerbL, VerbM, VisM and WM.
Genetic
The influence of the Val158Met polymorphism of the COMT rs4680 gene is the most frequently analysed genetic predictor of cognitive response to CRT. The weight of evidence, being four of six articles, suggests that purported associations between COMT rs4680 and cognition do not always extend to CRT response across Attn, SoP, WM, VerbL, VerbM or R-PS domains (Bosia et al., 2014; Burton et al., 2015; Greenwood et al., 2011; Mak et al., 2013). Of the two articles reporting an association, Boisa et al. (2007, 2014a) found that Met carriers made greater improvements on a measure of R-PS compared to Val/Val carriers. However, closer examination of their 2007 results reveals the effect was restricted to Met carriers receiving CRT compared to Val/Val carriers receiving no intervention; no difference was reported between Met versus Val/Val carriers receiving CRT (Bosia et al., 2007). As outlined by Greenwood et al. (2011), any number of factors might account for the variability in results, including small sample sizes comprising unequal groups that limits statistical power (Burton et al., 2015).
Discussion
This systematic review represents the first rigorous synthesis of the evidence base examining predictors of cognitive response to CRT. Through the application of strict criteria that excluded interventions that were found to incorporate social cognition or adjunctive rehabilitation and that gave preference to post-intervention over follow-up results, it was possible to address some of the potentially confounding factors that could account for heterogeneity of results (McGurk et al., 2013). With a meta-analysis not possible due to study design variability and data limitations, the largely narrative accounting was enhanced by inclusion of a box-score analysis and assessment of the quality of the predictor evidence. While this lacks the robustness and objectivity of a meta-analysis and fails to account for the size of effects across included articles (Green and Hall, 1984), it provided a methodical way of recording and presenting a summary of the review outcomes.
When examined as a systematic review, it is quickly apparent, from consideration of the evidence base, that very few of the currently examined predictors of cognitive response to CRT are significant. This supports results of earlier meta-analyses (Grynszpan et al., 2011; McGurk et al., 2007; Revell et al., 2015; Wykes et al., 2011), where no factors emerged as consistent moderators of treatment effect. It also draws attention to the limitations of more cursory reviews that often focus on findings of significance without adequate consideration of the weight of studies that find no such associations. Through systematic review, it has been possible to identify a number of areas worthy of closer examination that would otherwise have been masked or overlooked using meta-analytic techniques.
Demographic considerations
There is little evidence to suggest that differences in gender, age, level of education or current IQ effect the efficacy of CRT or would act as barriers to realising individual benefit from CRT. The influence of premorbid IQ on CRT efficacy was less clear cut. Premorbid IQ has previously been conceived of as both a risk factor and as a protective factor in the development of schizophrenia (Khandaker et al., 2011) and, as such, may operate at different levels on CRT outcome. It is possible that the relationship between premorbid and current IQ might be more predictive of CRT response. There is limited evidence that individuals with a comprised IQ trajectory, typically defined as premorbid and current IQ below 90 and within 10 points of each other, are less likely to generalise training effects to independent measures of cognition compared to those with preserved (premorbid and current IQ ⩾ 90 and within 10 points of each other) or declined (estimated current IQ at least 10 points less than estimated premorbid IQ; Fiszdon et al., 2006) IQ trajectories. This proposal needs further investigation.
The lack of an effect of age on response to CRT is consistent with results of earlier meta-analyses. As per Wykes et al. (2011: 482), it is possible that the lack of association could be attributable to the narrow range of ages examined, with a majority of articles reporting mean ages in the 30s. While some evidence suggests that recent-onset participants have greater potential to benefit from training (Bowie et al., 2014; Corbera et al., 2017), effect sizes from the recent meta-analysis of CRT efficacy in early schizophrenia (Revell et al., 2015) were smaller than those found in chronic schizophrenia. There is a risk of conflating evidence of cognitive decline across the lifespan (Harada et al., 2013) with the ability of older adults to benefit from cognitive interventions. Evidence from healthy older adults (Kueider et al., 2012) and those with mild cognitive impairment (Hill et al., 2017) suggests that the capacity to benefit from CRT remains intact across some, but perhaps not all, cognitive domains.
Baseline clinical considerations
The paucity of associations between clinical factors and cognitive outcome is in line with evidence of the relative independence of clinical and cognitive domains (Heinrichs et al., 2013). Although small to moderate correlations have been found between both negative and disorganised symptoms and specific domains of cognition (de Gracia Dominguez et al., 2009; O’Leary et al., 2000; Ventura et al., 2010), symptom severity appears at worst to attenuate rather than prevent gains from CRT (Wykes and Spaulding, 2011). Regarding medication effects, evidence of the relative effects of different types of antipsychotic medication remains equivocal (Goff et al., 2017), and it is difficult to tease out other factors that could confound results, such as dose and anticholinergic burden.
Baseline cognition considerations
One of the stronger trends to emerge was the influence of baseline cognition on within-domain improvement following CRT. However, evidence was limited to three domains, with the strongest effects found in R-PS and WM. It is plausible to suggest that an individual’s baseline cognitive profile in part influences their ability to engage in and benefit from CRT, and a case has been made for both positive and negative associations. Some have suggested that stronger baseline performances aid target engagement and resultant treatment gains (Biagianti et al., 2016), while others have suggested that poorer baseline performance allows more room for improvement (Twamley et al., 2011). These are not mutually exclusive and might vary by domain, warranting further enquiry. There is a need to extend research in this area to consider the impact of CRT on a wider range of cognitive domains and to determine whether there is a threshold of performance below which participants are less likely to benefit from CRT.
Treatment considerations
Vinogradov et al. (2012) presented a persuasive argument that cognitive training needed to be of sufficient intensity and duration to drive the cortical reorganisation associated with enduring change. Evidence to-date suggests that there is a point at which further training is unlikely to confer additional cognitive benefit, being circa 20 hours. However, more follow-up studies are needed to determine whether the longer training periods result in more enduring cognitive change or drive greater functional improvements. It also remains unclear what role intensity of training plays in driving cognitive change and whether the influence of duration and intensity differs according to training type (see Popov et al., 2011).
The mediating role of training task progress on cognitive response to CRT is an emergent area of investigation being innovatively led by Vinogradov and colleagues (Biagianti et al., 2016; Fisher et al., 2009, 2015; Vinogradov et al., 2012). While the consistency in results to-date is encouraging, the evidence base is small and needs to be extended across a wider range of research groups considering a more diverse range of CRT interventions. A potential limitation is that operationalisation of training task progress will likely vary across studies and by training task, making cross-study comparison difficult, and would need to be clearly delineated from potential practice effects. Moreover, the prognostic value of training task progress is somewhat limited as it can only be measured subsequent to CRT commencement. A complimentary line of enquiry should examine potential correlates of task progress, such as learning potential (Davidson et al., 2016; Kurtz and Wexler, 2006; Rempfer et al., 2011; Wiedl and Wienöbst, 1999), that could better inform treatment planning.
Genetic considerations
Interest in genetic influences on the efficacy of CRT in schizophrenia is natural given evidence of the high heritability of schizophrenia (Sullivan et al., 2003) and of neurocognitive traits (Husted et al., 2009). However, given the complex interaction of multiple genetic risk variants on cognitive endophenotypes (Greenwood et al., 2011, 2012) coupled with evidence that measures of cognition may be more distal to underlying genetic risk and therefore less sensitive in detecting associations between cognitive change and purported genetic risk variants (Rose and Donohoe, 2013), it is unlikely that investigation of single-risk variants will yield consistent results.
Methodological considerations
There are a range of more general limitations in CRT research that add complexity and challenge interpretation when examining predictors of CRT response. These have been comprehensively explicated by others (McGurk et al., 2013) and will not be restated here.
Regarding study inclusion criteria, the diagnostic threshold of a minimum 70% of participants diagnosed with schizophrenia/schizoaffective disorder followed the precedent set in previous meta-analyses (e.g. Wykes et al., 2011). While it is possible that a tighter criterion might have increased the specificity of the findings to schizophrenia/schizophrenia affective disorder, 39 of 40 studies far exceeded this threshold (Table 1). Furthermore, given the relatively small evidence base to have examined predictors of response to CRT, we opted to be as inclusive as possible by including single-arm trials and retrospective analyses of these. We recognise that these study types carry a risk of bias and that our conclusions might be somewhat different if these studies had been excluded. However, as our interest was restricted to the application of CRT to schizophrenia-type disorders, and single-arm trials are by definition limited to the population under investigation, we believe that the slightly increased possibility of bias was an acceptable risk.
Use of systematic review has exposed a number of methodological issues that, in limiting what conclusions can be drawn, should be addressed in ongoing efforts to understand factors that influence the efficacy of CRT in individuals with schizophrenia. First is the large number of potential predictors of response that have been assessed only once or twice. Of the included literature, it was only possible to review a quarter of the examined variables. While there is publication pressure to identify and highlight unique findings, lack of replication renders a large proportion of the predictor literature inconclusive.
Variability in methodological approach and rigour was apparent across the evidence base. Had the quality guidelines outlined by Pincus et al. (2011) been applied as study selection criteria, few of the studies reviewed would have been included in this systematic review. This in part reflects the lack of a comprehensive synthesis of the predictor evidence base to inform future research, the sometimes exploratory nature of the analysis being undertaken, and the potentially misinformed use of covariates to control for baseline between group differences (see Kraemer, 2016). Only 8 articles reported controlling for multiple comparisons and 14 reported tests of interaction. A more specific methodological concern relates to multiplicity issues associated with systematic reviews and the risk of over-interpreting pooled results (Bender et al., 2008; Wang et al., 2007). Multiplicity issues are compounded when examining multiple groups, subgroups and time points. While it was not possible to control for these, we identified whether full sample or subgroup analysis was performed and have been cautious in the interpretation of outcomes.
Future direction
Having reviewed the evidence base thus far, it remains unclear why around 44% of people do not receive cognitive benefit from CRT. However, when considering only those variables where a majority of articles reported a statistically significant association with cognitive response to CRT, three stand out: premorbid IQ, baseline cognition and training task progress. Each of these relates in some way to an individual’s capacity or potential for change. There is a need to both extend and consolidate the promising lines of enquiry to emerge from this review, being the influence of baseline cognition and training task engagement on the efficacy of CRT.
We need to move beyond consideration of factors such as age, gender and duration of illness in considering the neurobiology of neuropsychiatric illness and neurobiology of learning and learning potential (Vinogradov et al., 2012). Moreover, closer attention to the potential influence of non-specific factors on response to CRT is warranted (see Wykes and Spaulding, 2011). Radhakrishnan et al. (2016) found a small but significant effect (Cohen’s d = 0.12, SD = ±0.16) of non-CRT-specific factors in RCT control groups, and there is recent evidence that therapist alliance may influence CRT response (Cella and Wykes, 2017). The exact type and nature of these effects remain to be characterised.
No study has investigated all predictors with the same data set. There might be cross cultural, education or socioeconomic differences that influence CRT outcomes differently internationally. We need to conduct large-scale investigations informed by a priori hypotheses, ideally involving cross-research group collaboration or international data pooling initiatives (indeed where appropriate ethical approvals have been given to re-analyse existing data sets, the international community might consider such an initiative straight away). How we define and measure improvement (Medalia and Richardson, 2005) also needs further consideration. Finally, in the face of evident interindividual variability, we need to reconsider whether traditional group-level analysis is sufficiently sensitive to detect predictors of such differential patterns of response (Jacobson et al., 1984).
Supplemental Material
Supplementary_Figure_1 – Supplemental material for A systematic review of factors that influence the efficacy of cognitive remediation therapy in schizophrenia
Supplemental material, Supplementary_Figure_1 for A systematic review of factors that influence the efficacy of cognitive remediation therapy in schizophrenia by Maree P Reser, Reneta Slikboer and Susan L Rossell in Australian & New Zealand Journal of Psychiatry
Supplemental Material
SysRev_Supplementary_Tables_clean_v2.0 – Supplemental material for A systematic review of factors that influence the efficacy of cognitive remediation therapy in schizophrenia
Supplemental material, SysRev_Supplementary_Tables_clean_v2.0 for A systematic review of factors that influence the efficacy of cognitive remediation therapy in schizophrenia by Maree P Reser, Reneta Slikboer and Susan L Rossell in Australian & New Zealand Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The first author (M.P.R.) gratefully acknowledges the contribution of an Australian Government Research Training Programme Scholarship in supporting this research.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.