
Abstract
Objective:
To determine what motivates smokers with mental illness to participate in a smoking cessation or reduction programme and to report their attendance and cessation rates.
Method:
A group programme was provided to assist smokers with mental illness to cease or reduce their use of tobacco. People who registered to address their tobacco use completed a questionnaire which included information about their mental health, tobacco use, and what they wanted to achieve by attending the programme.
Results:
A total of 1043 smokers living with mental illness contacted the programme and asked for help to address their tobacco use between 2000 and 2011. At the first contact they were smoking an average of 27.4 cigarettes per day and had been smoking for 23.8 years, and 87% said they wanted to quit tobacco and a further 10% wanted to smoke less: 85% said they were concerned about the effect that smoking tobacco was having on their health, 56% were concerned for financial reasons, and nearly half (47.6%) said that they were concerned about both their physical health and their financial situation. In Adelaide, 148 Tobacco Free programmes were provided by mental health services. Of those who attended at least one session and completed an evaluation at the end of the programme, 22.5% reported not smoking. Most remained motivated to continue to address their tobacco use and many registered for a further programme.
Conclusions:
Many smokers living with serious mental illness are concerned about the impact of tobacco use on their health and finances and are motivated to address it. Group treatment programmes specifically designed for these people can achieve good cessation rates and should be readily accessible to all smokers with mental illness.
Introduction
The high rate of tobacco smoking by people with mental illness is well known (Lasser et al., 2000; Australian Bureau of Statistics, 2008; National Preventative Health Taskforce, 2008; Lawrence et al., 2009). A recent national study of people living with a psychotic disorder in Australia found 71.1% of men and 58.8% of women were smokers (Cooper et al., 2012). These findings are supported by a review of 42 international studies which found an average smoking prevalence of 62% amongst people with schizophrenia (de Leon and Diaz, 2005). In comparison, 15% of the adult Australian population were found to be current daily smokers in 2010 (Australian Institute of Health and Welfare, 2011).
A substantial proportion of tobacco smokers in Australia are people who are living with mental illness. The National Survey of Mental Health and Wellbeing (Australian Bureau of Statistics, 2008) found that of 3.6 million people who identified as current smokers in Australia, 32% had experienced mental illness in the previous 12 months. Access Economics (2007) calculated that people with mental illness smoke 16% more heavily than the general community and consume at least 42% of all cigarettes sold in Australia.
The serious health effects of tobacco use are well known, with studies finding that one in two long-term smokers die as a result of smoking. They die on average 13–14 years earlier than non-smokers, and they suffer more disease and disability (US Department of Health and Human Services, 2010). Tobacco smoking has been identified as one of the risk factors contributing to poor physical health, excess disability, and premature death experienced by people with severe mental illness (Mitchell and Malone, 2006; Kisely et al., 2008; Cooper et al., 2012; Galletly et al. 2012). In addition to the serious health effects, many people are spending a large percentage of their weekly income on tobacco, which can cause significant financial stress with less money for food, recreation, transport, clothing, and health care (Lawn et al., 2002).
It is often assumed that people living with mental illness are not concerned about their tobacco use and are not interested in addressing it (Etter et al., 2004; Siru et al., 2009; Ashton et al., 2010a). Ashton et al., (2010a), in a survey of mental health worker’s attitudes to addressing tobacco dependence with patients, found that two-thirds of workers believed that less than half of their patients wanted support to stop smoking and only 26% raised the issue of tobacco use regularly as part of their assessments or routine clinical care.
Despite the impact of tobacco use on the health, finances, and quality of life of smokers who live with mental illness, few programmes have been specifically provided to help this group of smokers (Etter et al., 2004; Lucksted et al., 2004; Williams and Foulds, 2007; Siru et al., 2009). In addition to an assumption that this group of smokers is not interested, this lack of specific interventions may also reflect a belief that people with mental illness are unable or unwilling to quit. Alternatively, it may be thought that population-level tobacco control measures are sufficient; however, in Australia, there has been no change in the rate of smoking amongst people with psychotic disorders between 1997 and 2010, despite a substantial decline in the prevalence of smoking in the general population (Cooper et al., 2012).
Group programmes are recognized as an effective way to assist smokers to quit tobacco. Carlson et al. (2002) described an 8-week group programme for smokers from the community with or without mental illness and reported a 36% smoking cessation rate at 3 months. Group programmes that are provided specifically for smokers with mental illness have also been shown to be effective. Currie and colleagues (2008) reported on a group programme for people with mental illness and found that at the end of a four- or eight-session programme, 16% of people had quit smoking. Morris et al. (2011) studied a community-based group programme for smokers with mental illness and compared it to the use of a telephone smoking cessation programme. They found those who received support from both Quitline and the group were significantly more likely to reduce tobacco use compared to those receiving only Quitline support. They reported a smoking cessation rate of 10%, by those who received at least one session and completed the evaluation at 6 months. Individual smoking cessations interventions have also been shown to be effective for this group, with Baker and colleagues (2006) finding that 30% of people with a psychotic disorder who completed all eight sessions of an individual intervention achieved cessation at 3 months.
The Tobacco Control Unit, Drug and Alcohol Services South Australia and the South Australia Mental Health Services developed the Tobacco and Mental Illness Project (TMIP), which delivered a smoking cessation programme within the adult mental health services in the Adelaide metropolitan area. Over 1000 people living with mental illness contacted the Project between 2000 and 2011 and asked for help to address their tobacco use.
This data provided an opportunity to determine what people say about their smoking, their motivation to address it, and what they want to achieve. This is important in understanding their thoughts about smoking, what prompts them to seek help and the motivations driving their attempts to address it. This information can be used to shape the development and provision of interventions specifically for this group of smokers and ensure that services best meet participants’ goals for better health and wellbeing.
The TMIP groups ran for over a decade and outcome data was collected throughout this period. This naturalistic data includes demographic and diagnostic information, along with rates of smoking cessation. Some data about cessation rates is reported briefly in the current paper, but detailed information about the efficacy of the programme will be published in a subsequent publication. Further information and resource material for the TMIP group programme can be obtained from the corresponding author.
Methods
Between 2000 and 2011, 148 group programmes were provided. Three programmes were located within hospitals and 145 were run in 15 community-based mental health services across the Adelaide metropolitan area. The size of the group usually ranged from 8–15 people. People with mental illness could register interest by contacting the TMIP if they wanted to quit or reduce their tobacco use or if they were just considering addressing it.
The programmes were facilitated by a peer worker, who was someone living with mental illness who was a comfortable non-smoker but had previously been a smoker, and a mental health worker who usually had a tertiary qualification such as occupational therapy or social work. Both the peer workers and the mental health workers received specific training provided by the TMIP about helping smokers with mental illness to address tobacco use. The sessions were structured and addressed a range of areas including problem solving, skills training, and motivational interviewing. Subsidized nicotine replacement therapy was available.
The programmes were provided over an 11-year period and during this time they evolved in response to feedback from participants, staff changes, and the availability of resources. Two of the most significant changes involved the number of sessions offered and entry into the programme. Between November 2002 and October 2005 the programme involved 15 sessions over 10 weeks and participants attended an initial interview before attending. From 2006 until December 2011 the programme involved 8–10 sessions held over an 8–10-week period and participants registered by phone or came directly to the programme. Participants involved after 2006 could commence at any session. The programmes provided between November 2002 and October 2005 have been described in more detail (Ashton et al., 2010b).
Data collection
A pre-programme questionnaire was completed by each person, which included demographic data and information about their mental health, tobacco use, their motivation to address it, and what they wanted to achieve. Between 2000 and 2005 those who expressed interest were asked to attend an interview to complete the questionnaire (n=184) and from January 2006 to December 2011 this information was collected over the telephone and at the first group session that they attended (n=859). Participants were asked their main reasons for wanting to address their tobacco use and these responses were coded by three separate individuals, with an agreement reached about the final coding. Often participants reported many different reasons for wanting to address their tobacco use and all were recorded; multiple codings were allowed for each participant.
If the participant gave written consent, information was sent to their doctor about their involvement in the Tobacco Free programme and until December 2008 the doctor was asked to send a written referral with information about the person’s psychiatric diagnosis and medications. From January 2009 to December 2011 a written referral from the doctor was not requested (n=355).
At the first session, participants completed the Fagerström test for nicotine dependence (Fagerström, 1990). From January 2006, participants were asked to use the Micro+ Smokerlyzer (Bedfont Scientific, Maidstone, UK) to measure breath carbon monoxide levels at the beginning and end of the programme. At the last session of the programme, participants completed an evaluation and participants who were not present were followed up by phone to complete the evaluation.
Descriptive statistics were analysed using SPSS for Windows version 19 (IBM).
Results
Characteristics of those who registered for the Tobacco Free group programme
A total of 1043 people who identified as having a mental illness contacted the Tobacco and Mental Illness Project and registered interest in attending the Tobacco Free group programme between 2000 and December 2011. About half (50.4%) were male; the men were aged (mean±SD) 41.89±11.21 years) and the women were aged 45.11±10.73 years). Of the participants, 66.2% had been told about the programme by their doctor or another health worker, 16.4% had seen a brochure or flier or had attended an information session run by the TMIP, 7.4% had heard about the programme from the Quitline, and 8.6% had heard about the programme from a friend, family member, or another participant.
From 2000 until 2008 the participants’ diagnosis was provided by their doctor (n=521). When this was not available, or if the participant registered after 2008, the diagnosis was provided by the participant. Overall, a diagnosis was recorded for 868 participants and of these, 53.8% were diagnosed with schizophrenia or schizoaffective disorder (Table 1). The Other category included post-traumatic stress disorder, personality disorders, eating disorders, and obsessive compulsive disorder.
Diagnosis of those registering for smoking cessation groups (n=868).
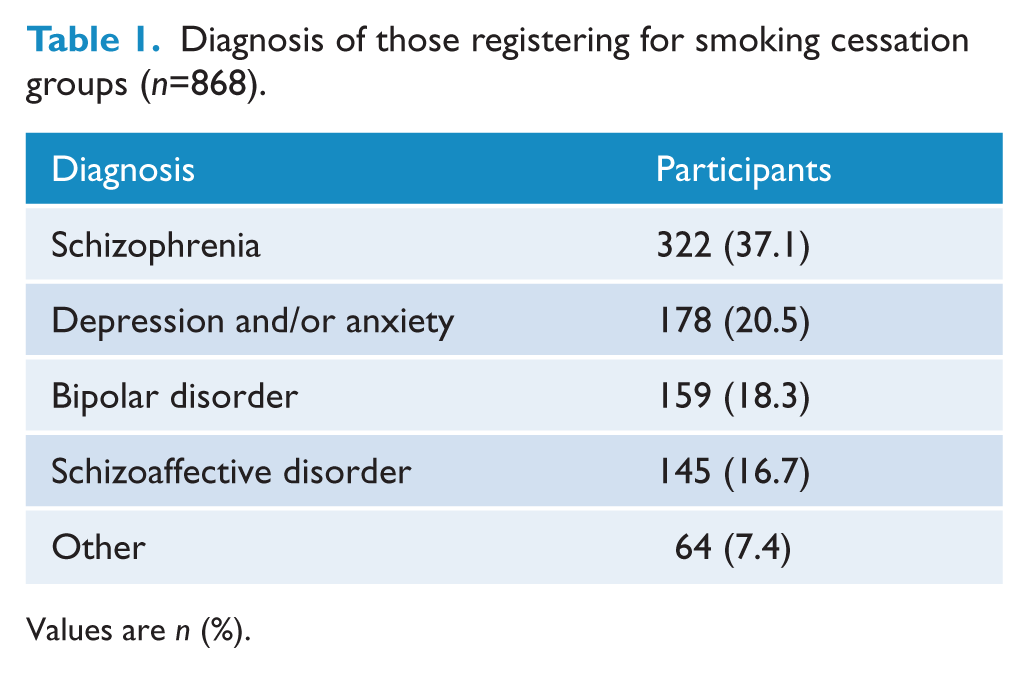
Values are n (%).
Participants were asked what type of housing they lived in. Of the 759 who completed this question, 47.7% of participants lived in public housing, 18.2% in their own home, and 16.1% in private rental, 10% lived with family, and 7.6% lived in supported residential facilities such as hostels or boarding houses.
Smoking
The number of cigarettes smoked per day at the point of registration was 27.4±14.7 (range 0–100). Twenty-eight participants (2.7%) said they had stopped smoking recently, but they wanted to attend the programme to get support and remain non-smoking, and 25% were smoking more than 30 cigarettes per day (Table 2). At the time of writing this would cost more than $100 per week in South Australia. Six participants (0.6%) reported smoking 100 cigarettes per day at registration.
Cigarette consumption per day (n=1043).
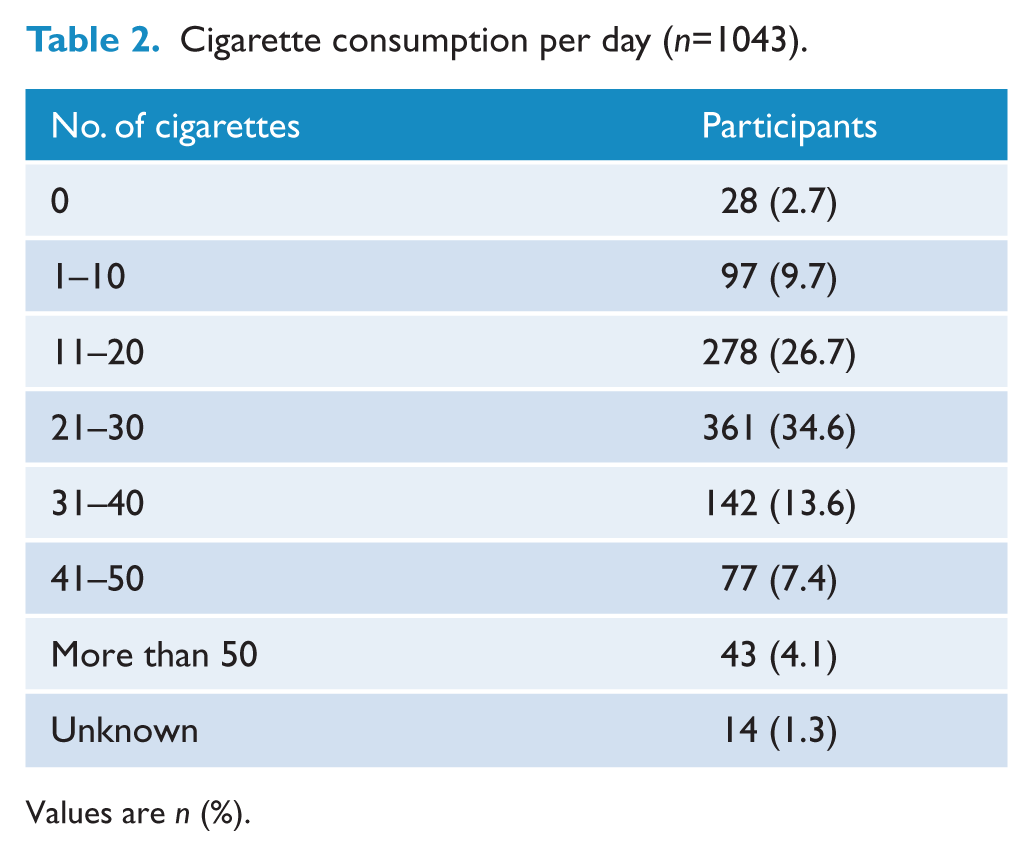
Values are n (%).
The number of years smoking was 23.8±11.91 (range 1–60 years). More than one-third (35.1%) of participants had been smoking for at least 30 years and 25 (2.3%) had been smoking for at least 50 years.
Previous attempts to quit
Of the 1043 participants, 871 (83.5%) said they had tried to quit tobacco before, and of these 47.9% had previously called the Quitline and 57.7% had used nicotine replacement therapy.
Motivations to seek help to address tobacco use
Participants were asked what they wanted to achieve by attending the Tobacco Free programme and of the 1018 who responded, 87.6% said they wanted to quit tobacco (62.5% wanted to quit tobacco without reducing first, 25.1% wanted to reduce and then quit tobacco), 10% aimed to reduce their tobacco use and did not intend to stop smoking, and 2.2% had other goals including learning about how they could address tobacco use in the future.
Participants were asked their main reasons for wanting to address their tobacco use (Table 3). Some participants provided multiple reasons and therefore their responses had multiple codings. Some examples of the qualitative responses are provided below:
Reasons for wanting to address tobacco (n=820).
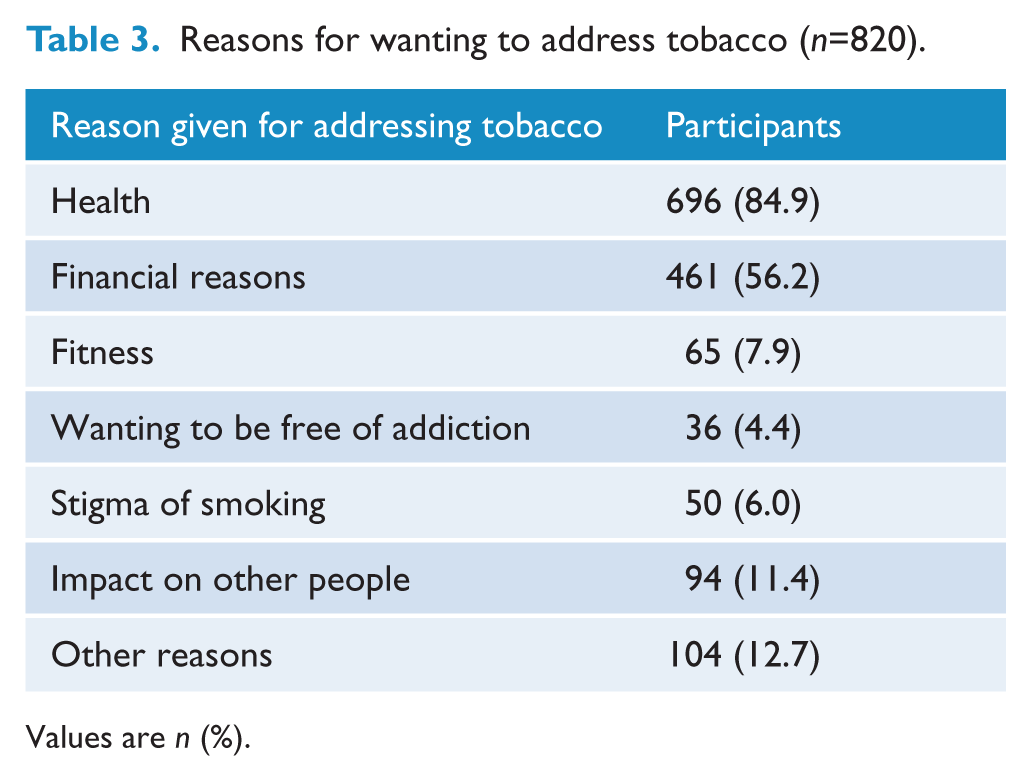
Values are n (%).
I don’t want to get long-term health problems, I want to feel better and to manage financially.
I am concerned about health; I don’t want emphysema like Mum, want to save to be able to travel and feel good about myself.
My son is worried about me, and it is costing $140 a fortnight.
Programme participation
Of the 1043 participants who registered for a Tobacco Free programme between 2000 and 2011, 816 (78.2%) attended at least one session in the first programme provided after their registration, 572 (53.3%) participants attended three or more sessions, and 227 (21.8%) did not attend at all. The reasons given for not attending the programme included being unwell or inability to get to the group because the location or time was difficult. Some said they had difficulty committing themselves or had decided that they no longer wanted to address their tobacco use. Others said they needed more practical assistance such as transport or one-to-one support to get to the group.
Nicotine dependence amongst those who attended at least one session
At the first session that participants attended, they completed the Fagerström Test for Nicotine Dependence (Fagerström, 1990) and 77% recorded a score of 6 or more, indicating that they were highly or very highly dependent on nicotine (Table 4).
Fagerström Score measured at the first session attended (n=718).
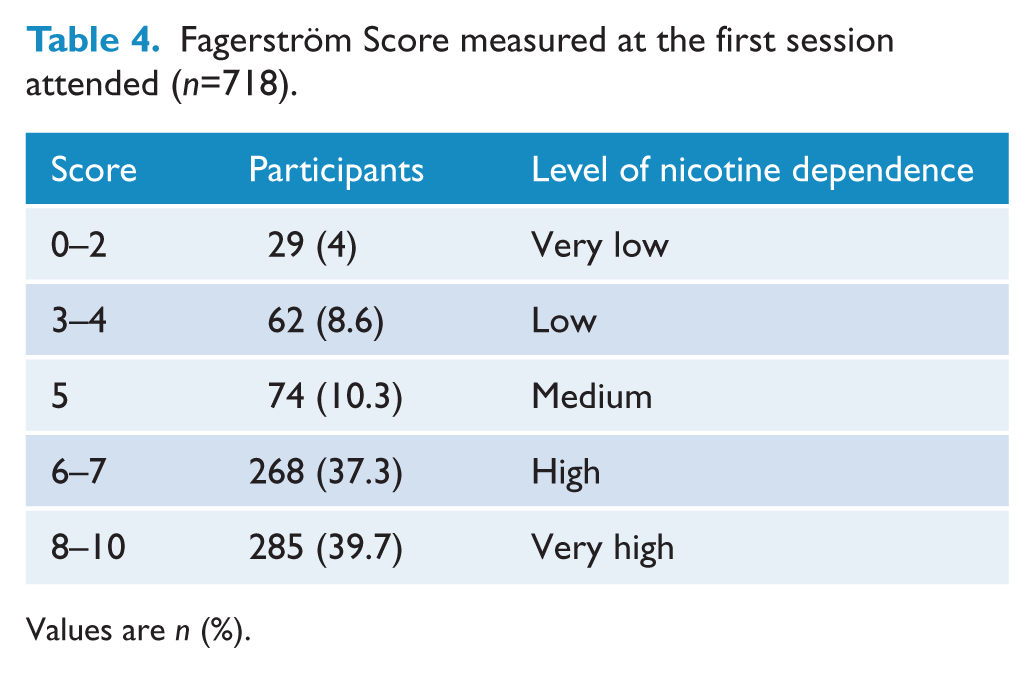
Values are n (%).
From January 2006, participants used a Micro+ Smokerlyzer to measure breath carbon monoxide levels. Readings were available at the beginning of the programme for 480 (72%) of the 666 participants who attended at least once. Their CO readings ranged from 0–59 ppm, with a mean score of 17.9 ppm, indicating regular smoking with significant levels of carbon monoxide in their blood. A score of 6 or less is an indication of not having smoked in the previous 8 hours and a score of 7–10 ppm indicates a light smoker or a non-smoker who has been breathing in poor-quality air or passive smoke (Bedfont Scientific).
Rates of smoking cessation at the end of first programme
Of the 816 participants who attended at least one session in the first programme provided after their registration, 631 (77.3%) could be contacted for evaluation at the end of the programme and 142 (22.5%) of these reported not smoking. Of the participants who attended three or more sessions, 494 (86.4%) could be contacted and 124 (25.1%) said they were not smoking. From January 2006 666 participants attended at least once, and of these 49.8% had a recorded carbon monoxide reading at the end of the programme; 85.7% of those who said they were not smoking had a verifying CO reading of 6 ppm or less and a further 8.5% had CO reading of 7–10 ppm.
Many participants remained motivated to continue to address their tobacco use and although further programmes were subject to the availability of staffing and resources at the mental health sites, when another course was offered many participants went on to register again. Of those who attended at least one session of the first programme provided, 57.4% registered for a further Tobacco Free programme.
Discussion
This study found that when a smoking cessation or reduction programme is offered within adult mental health services, many people with mental illness ask for help and take action to address their tobacco use. We found that despite most participants living with psychotic illness and being heavy smokers over many years, the majority (87.6%) reported that they wanted to quit tobacco and 10% wanted to reduce their smoking. Most were concerned about the impact tobacco was having on their health, and over half were concerned about the effect it had on their finances. Similarly, Dickerson et al. (2011) found that the most common reasons for quitting smoking by people with serious mental illness were health and finances.
We found that 66% of the participants had been encouraged by their doctor or health worker to contact the TMIP to ask for support to address their tobacco use, and a further 16% had seen a flier or attended an information session about the programme. It therefore appears that once information was provided, especially with encouragement from a clinician, people did go ahead and make contact with the TMIP.
Our findings therefore suggest that smokers with mental illness are concerned about their smoking for the same reasons as other smokers in the community and when health workers talk to them about their smoking and encourage them to address it, many do seek help. This finding endorses the document prepared by the Australian College of General Practice Supporting smoking cessation: a guide for health professionals 2011 (Zwar et al., 2011), which recommends that all health professionals ask their patients about tobacco, spend at least a few minutes talking to smokers about it, encourage them to seek help, and refer them to cessation support services.
We found that of those who sought help to address their tobacco use and participated in the Tobacco Free programme at least once, 22.5% were not smoking at the end of the programme and cessation rates were higher for those who attended at least three sessions, with a quarter not smoking at the end of the programme. There are several other studies which have evaluated the impact of smoking cessation programmes provided within community mental health services (Baker et al., 2006; Currie et al., 2008; Morris et al., 2011), and these studies have also shown that some people living with mental illness are able to stop smoking when provided with a specifically tailored programme.
This study has some limitations as it only considered the views of smokers living with mental illness who had heard about the Tobacco Free programme and were concerned about their tobacco use. People who had no interest in addressing tobacco use are not represented in this study. The study was also limited to the Adelaide metropolitan area, where the TMIP had conducted training for health workers and all mental health workers had been encouraged to talk to their clients about tobacco and, if they were interested, to refer them to the Tobacco Free programmes, so it may not be representative of other regions. The study primarily used self-reported smoking status as the Smokerlyzer was not always available to measure breath carbon monoxide levels and verify self-reported smoking status, and it was not possible when the evaluation was completed by phone. However, where a carbon monoxide reading was available there was a high degree of verification with self-reported smoking status. The study was a naturalistic study of a programme provided within mental health services over a 12-year period with some changes to data collection processes over that time. Whilst efforts were made to follow up all participants, some participants were lost to follow up so data about their success in quitting smoking was not available.
Although people with mental illness have been identified as a priority group by Tobacco Control Strategies, very few programmes targeting this group have been provided. Our study demonstrates that many people with mental illness are motivated to quit smoking, their reasons are pragmatic and logical, and they can be proactive about engaging with cessation programmes. Greater access to such programmes has the potential to reduce rates of smoking by people with mental illness, directly improving their physical health and quality of life.
Footnotes
Acknowledgements
Sincere thanks to all programme participants and to Mark Weston, Sheryl Mulconray, Sue Bertossa, Sue Condon and others involved in co-facilitating the programmes.
Funding
This programme and evaluation was funded by Drug and Alcohol Services South Australia, South Australian Department for Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper