
Abstract
The rates of smoking among people with mental illness have been found to be very high, especially among specific groups. A national survey of people living with psychotic illness in Australia found that 73% of men and 56% of women smoked tobacco [1]. A meta-analysis of over 40 studies conducted in 20 countries found that, in most studies, smokers with schizophrenia and other types of severe mental illness were significantly heavier smokers than smokers within the general population [2].
The physical health effects of tobacco smoking are well known [3], with many losing years of life [4] and spending their last years with significant illness and disability caused by their tobacco use [5].
In addition to the serious physical health effects of smoking, many people with severe mental illness live on a disability pension or limited income and high tobacco use can make it difficult or impossible to afford good food, accommodation and other essential and non-essential items [6].
Contact with a health service can be an important opportunity to receive information and support to address tobacco use. Systematic reviews have confirmed the effectiveness of brief smoking cessation advice from physicians and other health workers [7,8]. Evidence has shown that people with mental illness are often concerned about tobacco use and are as motivated to quit tobacco as the general population [9]. Studies have also shown that many people with mental illness, if given information and support, are able to quit [10–14]. Despite the serious health and social impacts of tobacco use on people with mental illness, and the opportunity to provide help, employees within mental health services often fail to address it. People with mental illness often do not receive support and in some cases are actually discouraged from quitting tobacco [15]. An Australian study of 300 smokers with psychosis found 74% had not been advised to quit smoking by their psychiatrist and 86% had not been advised to quit by case managers. Fifteen per cent had been advised that smoking was ‘an acceptable activity for them’ [16]. Another Australian study found that less than one fifth of patients in inpatient psychiatric units had been offered advice or information about tobacco smoking [17].
Mental health workers are often not trained to address tobacco use, with one study finding only 27% of GPs and only 7.3% of psychiatrists had received training in providing brief smoking interventions [18].
Tobacco legislation is increasingly prohibiting smoking in enclosed public places, workplaces and shared areas. Many hospitals and health services are implementing totally smoke-free policies and there are many very complex concerns raised within mental health services about patient care, occupational health and safety, and legal issues [19,20]. The attitudes of workers to managing tobacco use have been shown to significantly affect the successful implementation of tobacco policies [21–23].
Objectives
The aims of this study were to assess mental health workers’ attitudes to addressing patients’ tobacco use, to identify any perceived barriers that prevent people with mental illness from receiving the support they require to tackle tobacco use, and to determine the workers’ recommendations for policy and practice change within mental health services in South Australia.
Methods
Ethics approval
This study had ethics approval from the Cancer Council South Australia Human Research Ethics Committee.
Inclusion and exclusion criteria
Mental health workers from government and non-government adult mental health services in Adelaide, South Australia were included in this study. The list of government adult mental health services was obtained from the White Pages telephone directory, and a list of all non-government mental health services was provided by the Mental Health Coalition, the South Australian non-government mental health peak body. Government mental health services included acute and extended care inpatient units, rehabilitation, community care, and assessment and crisis intervention services. Non-government mental health services included supported accommodation, respite, personal care, drop-in centres, supported employment and other support services. Mental health workers from private and child and adolescent mental health services were not included as their needs were considered to differ to those of government and non-government adult mental health services.
Recruitment
A survey package was mailed to the 75 eligible mental health services in Adelaide, South Australia (53 government and 22 non-government) in August 2007. The package included a letter introducing the study, instructions, two questionnaires and a reply paid envelope. One of the questionnaires was to be completed by the team leader and sought organization details. The other questionnaire was to be distributed by the team leader to all team members and assessed their attitudes towards tobacco related issues. Individual responses were confidential and questionnaires were returned to the researchers. Organizations which had not returned any questionnaires by a selected date received a reminder phone call to prompt a response.
Measures
Questionnaires completed by the team leader provided information on organization name and classification, type of service provided and number of staff members within the team. The pen and paper questionnaire completed by all staff assessed a range of attitudes towards tobacco use in mental health settings, with questions such as ‘how important is it to help your patients address tobacco addiction?’ and ‘what percentage of your patients do you think want support to reduce or quit tobacco?’ Participants provided their response on a Likert scale, for example, rating from 1–10, with one indicating ‘not at all important’ and 10 indicating ‘extremely important’. Participants were also asked to further explain their responses with open-ended questions.
Statistical analyses
Descriptive statistics for demographics and ratings were computed using SPSS version 15.0. Qualitative data were analysed using interpretive analysis, which involved two key stages of grounded theory, open coding and categorization [24]. For this process, data were coded by three independent researchers, two with extensive clinical mental health experience and expertise in tobacco research with these populations and one with extensive experience in tobacco control research and evaluation. Responses were coded into categories identified by the researchers, and where a response fitted into more than one of the categories, multiple categories were allowed. For example if a participant responded, ‘It is very important to address tobacco but it also needs to be the patient's choice’. This participant's response would have been categorized into the two categories, ‘ it is important’ and ‘ it is a matter of choice’. Inter-rater agreement was high (85% or higher for all coded categories).
Results
Participant characteristics
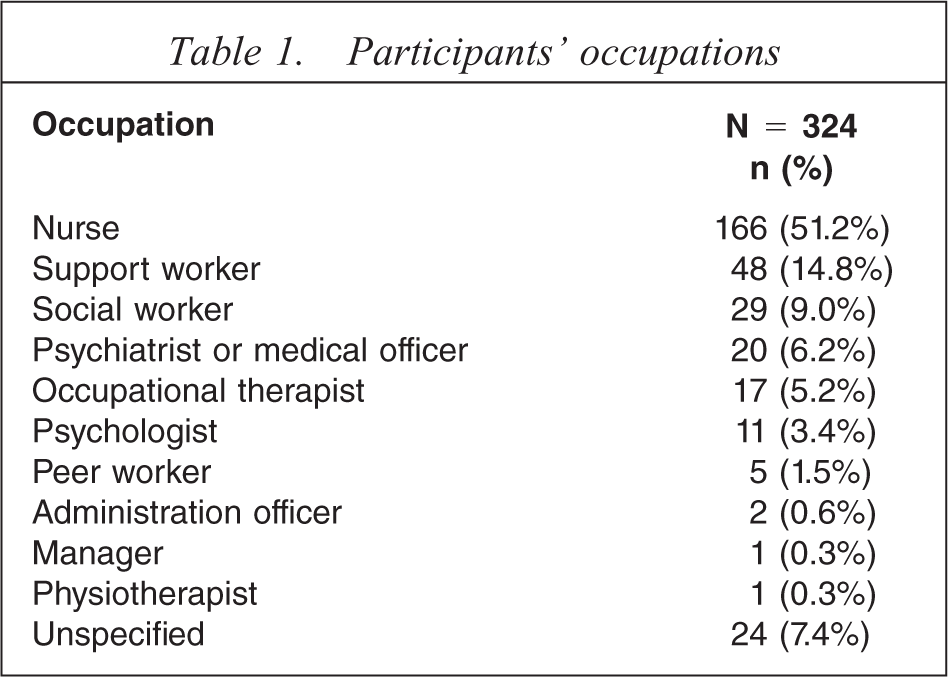
A total of 324 completed questionnaires were returned from mental health workers of various occupations. Table 1 shows that just over half of the participants who completed questionnaires were nurses.
Participants’ occupations
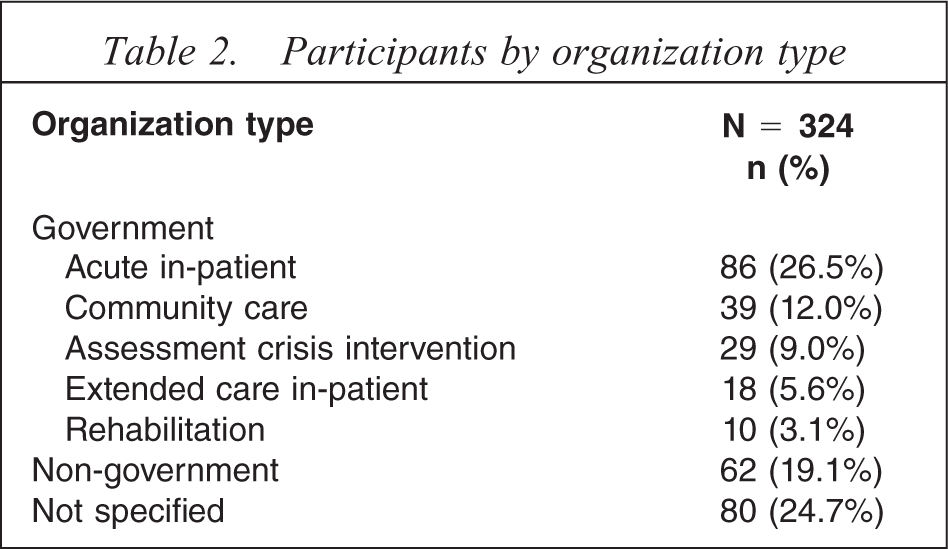
The 324 completed questionnaires were returned from 45 organizations (60% response rate). Table 2 shows that 56.2% of participants were from government organisations and 19% were from non-government organizations. Twenty-four per cent of the responses received were from organizations where the team leader failed to complete the questionnaire describing their organization's details, thus organization type is unspecified.
Participants by organization type
Attitudes towards the importance of addressing tobacco use with patients
Participants were asked to indicate how important they believed addressing tobacco addiction with their patients was on a 1-10 Likert-rating scale, with one indicating ‘not at all important’ and 10 indicating ‘extremely important’. Of the 322 (99.4%) participants who responded, 60.6% rated the importance as seven or above and 17% rated the importance as four or less, with an average rating of 6.9 (SD = 2.6).
Participants were then asked to explain their rating in open-ended format, with 281 (86.7%) participants providing a response. Table 3 shows that once responses were categorized by the researchers, more than half of the participants who provided a response felt it was important to help patients address their tobacco addiction.
Explanation of rating the importance of addressing tobacco use with patients (n = 281)
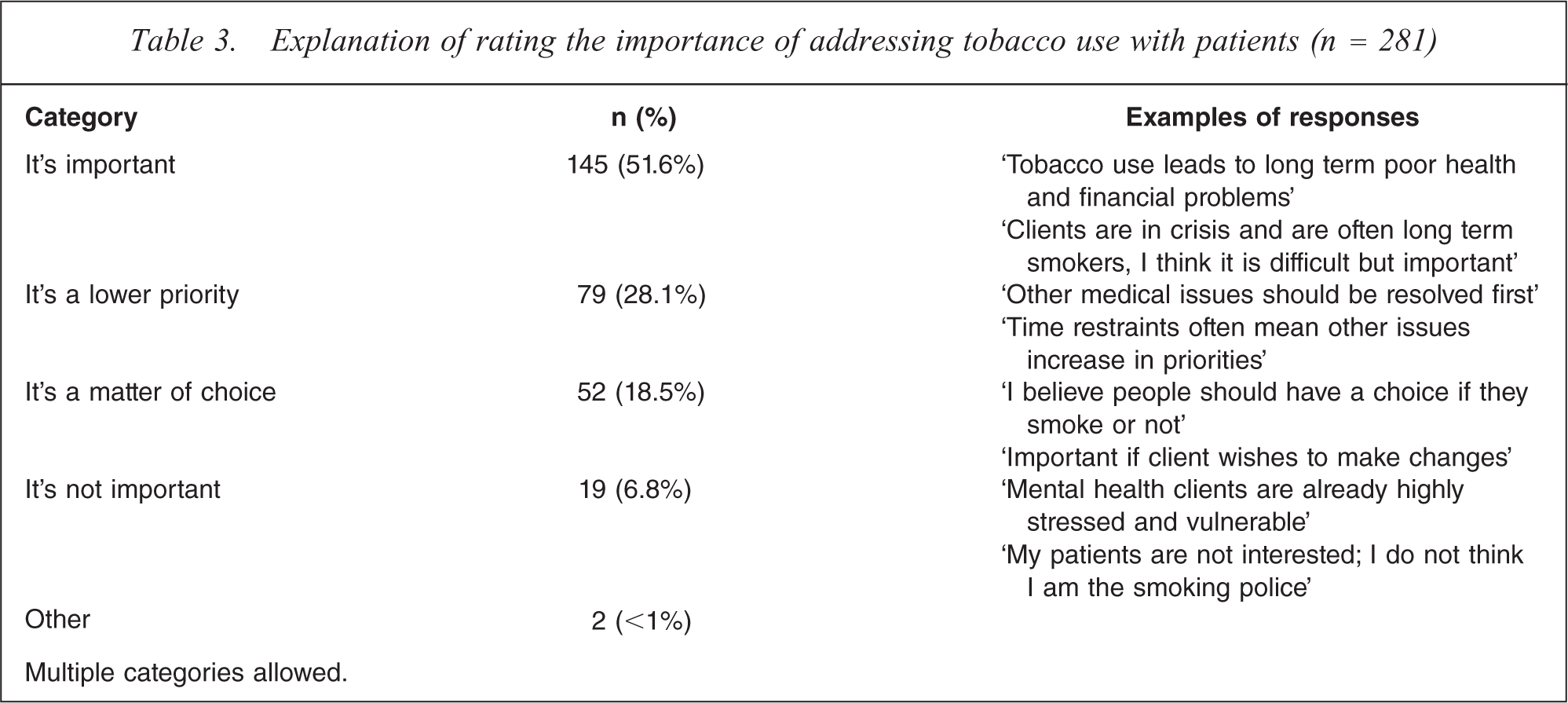
Multiple categories allowed.
Of the 145 participants who indicated it was important to address tobacco use, 65.5% felt it was important for health reasons and 39.3% indicated that it was important for financial reasons.
Attitudes toward mental health service involvement in assisting people with a mental illness to quit or reduce tobacco use
Participants were asked how involved they thought mental health services should be in helping people with a mental illness quit smoking or reduce their consumption. Participants indicated their attitude on a 1–10 Likert-rating scale, with one representing ‘not at all’ and 10 representing ‘a lot’. Of the 320 (98.8%) participants who responded, 69.3% rated the level of involvement as seven or above and 12.3% rated the importance as four or less, with an average rating of 7.3 (SD = 2.4).
Frequency of raising the issue of tobacco use with patients
Participants were asked to indicate how often they raise the issue of tobacco use with their patients, with a score of 1 indicating ‘never’ and 10 indicating ‘often’. A total of 315 (97.2%) participants responded, and on average rated a score of 5.7 (SD = 2.7).
A total of 253 (78.1%) participants explained their rating. Of the participants who provided an explanation, 36% said that they discuss tobacco use only when they are concerned about their patients’ tobacco use or if their patient raises the issue. For example: ‘If I notice they are coughing or showing other smoking related illness’,‘It's discussed if they identify it an issue.’
Twenty six percent (26.1%) said they raise the issue of tobacco use with patients often or as part of assessment. For example: ‘Every time I see them’; ‘On admission, ask if smoke, how many, strength and if they are interested in quitting or reducing’.
Perceptions of patients wanting support to quit smoking or reduce tobacco use
Participants were asked what percentage of their patients (0–100%) they thought wanted support to quit or reduce tobacco use, with 313 (96.6%) participants providing a response. The average rating was 33.5% (SD = 24.9). Thirty-three per cent of participants felt that more than half of their patients wanted smoking cessation support. However, 9.9% felt that none of their patients wanted support to address tobacco use.
Perceptions of the percentage of patients who could quit or reduce tobacco use if they received nicotine replacement therapy, information and support
Participants were asked what percentage of their patients (0–100%) they believed would be able to quit smoking or reduce consumption if they received nicotine replacement therapy, information and support. Of the 302 workers who responded (93.2%), 37% felt that more than half of the patients could quit or reduce with nicotine replacement therapy, information and support. Further, 7% of participants did not think any of their patients could quit or reduce consumption.
Perceived barriers to quitting or reducing tobacco use for people with a mental illness
Participants were asked to indicate what barriers made quitting or reducing tobacco use difficult for people with a mental illness. Responses were provided from 308 (95.1%) participants; and of these, 45.1% perceived boredom and social isolation to be a barrier to quitting or reducing tobacco use, 26% felt a lack of information and support, 25.7% felt their mental illness and 21.8% felt the addiction was a barrier.
Addressing barriers to quitting or reducing tobacco use for people with a mental illness
Participants were then asked to indicate how these barriers could be addressed. Responses were provided from 244 (75.3%) participants; with the provision of information and support listed most commonly (59%).
Suggestions for change to tobacco policies and practice
Participants were also asked if they had any suggestions for changes to be made to tobacco policies and practices within mental health services, with responses received from 147 (45.4%) participants. Suggestions for changes that should be made were provided from 85% of participants, while the other 15% indicated that no changes are required. The most commonly suggested changes were support for smoke-free areas (28.6%) and the provision of information and support (28.6%).
Conclusion
This survey aimed to assess mental health workers’ attitudes to addressing tobacco use, to identify system-related barriers that may prevent people with a mental illness from receiving the support they require to quit smoking, and to determine workers’, suggestions for policy and practice change within mental health services in South Australia. Results from the survey indicate that more than half of the participants surveyed believed it was important to address tobacco addiction with their patients for reasons such as health, finances, mental health and medication.
Over two thirds of the participants felt that mental health services should be involved in helping people with a mental illness quit smoking. However, only approximately one quarter of participants reported that they raise the issue of tobacco use with their patients often, or as part of the assessment and, approximately one third reported that they only raise the issue if they are concerned, or if a patient raises the issue of tobacco use with them first. Although most workers felt mental health services should be involved in addressing tobacco use, many reported waiting until there is a serious tobacco related problem before addressing it with their patients. This finding indicates some mental health workers are still ambivalent about addressing tobacco use or lack the skills and confidence and it suggests there is a need for professional development for all mental health workers. This finding also indicates there is a need to incorporate asking about tobacco use in standardized assessments and address it within the development of mental health care plans.
Many participants believed that their patients would like support to address tobacco use and if provided with the assistance of nicotine replacement therapy, information and support, many could successfully quit or reduce their tobacco consumption. This finding suggests people with mental illness are motivated and if they were to receive good information and support many could quit or reduce their tobacco use.
Over the last few years across Australia there has been much debate about the implementation of smoke-free hospitals and health services. This survey found that mental health workers recommended changes to tobacco policies and practices within mental health services and in particular they felt an increase in smoke-free areas and information and support should be provided to assist people with mental illness to address tobacco use.
This study has some limitations; firstly it was conducted only within the Adelaide metropolitan area and therefore only provides feedback from mental health workers in this location. Rural and remote based mental health workers and those in other services around Australia may have had different experiences and as a result have different attitudes. Also, the study asked workers to report their feelings about tobacco use within mental health services; it did not measure actual worker practices.
Another limitation was that 24% of the responses were received from organizations where the team leader failed to describe the type of organization and number of staff, this meant comparisons between organisations and information about the proportion of staff completing the questionnaire is not available.
The study was also conducted in 2007 and since that time many mental health workers in South Australia have been involved in training about helping people with mental illness to address tobacco use and significant change to policies and practices have been discussed and are being implemented.
This study has shown that many mental health workers believe it is important to address tobacco use and that many of their patients want, and would benefit from support. They also believe that services need to implement significant tobacco policy change and these changes should include the provision of information and support for patients, nicotine replacement therapy, the routine addressing of tobacco use within standard assessments and mental health care plans, the provision of increased smoke free areas and staff training.
This study has shown that most mental health workers involved are recognizing the importance of addressing tobacco use with their patients and the need for policy, practise and continuing professional development.
Footnotes
Acknowledgements
We thank Jacqueline Hickling and Deb Shaw, Tobacco Control Research and Evaluation Program, Cancer Council South Australia.