
Abstract
Objective:
The aim of the present study is to examine the mental health correlates of anger in the general population using data collected as part of the 2007 Australian National Survey of Mental Health and Wellbeing (2007 NSMHWB).
Method:
The 2007 NSMHWB was a nationally representative household survey of 8841 Australians aged between 16 and 85 years. The survey assessed for 30-day DSM-IV mental health disorders and 30-day anger symptoms.
Results:
A range of mood, anxiety and substance use disorders were found to be independently associated with symptoms of anger after controlling for demographics and comorbidity. These included major depressive disorder, bipolar disorder, social phobia, generalised anxiety disorder, obsessive compulsive disorder, post-traumatic stress disorder, and alcohol and drug use disorders.
Conclusions:
This study is the first epidemiological investigation of the mental health correlates of anger in the Australian general population. Anger can have extremely maladaptive effects on behaviour and can lead to serious consequences for the individual and for the community. The findings of the present study denote the importance of assessing anger symptoms among individuals presenting with these common mental health disorders.
Introduction
Anger is an emotional experience shared by all human beings. For the most part, anger is functional and produces adaptive effects on behaviour. For some individuals, however, anger can be persistent and severe and have extremely maladaptive effects on behaviour (Ramirez and Andreu, 2006). Given that anger varies substantially across individuals and can lead to serious consequences for the individual and for the community, including the perpetration of violence (Eckhardt et al., 2008; Novaco, 1994), it is important to identify those most prone to experiencing elevated levels of anger.
Anger is a complex construct consisting of emotional, physiological, cognitive and behavioural components. For this reason researchers have been careful to distinguish between different conceptualisations of anger. For instance, distinctions have been made between the experience of anger and the expression of anger (Hawkins and Cougle, 2011; Moscovitch et al., 2008). Similarly, distinctions have been made between trait anger and state anger. Trait anger is considered to be a general predisposition for reactivity in which anger is experienced in response to a range of provoking stimuli (Ramirez and Andreu, 2006; Spielberger et al., 1983). State anger, on the other hand, has been defined ‘as an emotional state that … consists of subjective feelings that vary in intensity, from mild irritation or annoyance to intense fury and rage’ (Spielberger et al., 1983: 16). Thus, anger can be considered as a dimensional construct varying in severity.
Emerging research has indicated that a particular group of individuals who have the propensity to experience state and trait anger are those diagnosed with mental health disorders. While the DSM-IV-TR (American Psychiatric Association (APA), 2000) does not characterise a specific anger diagnosis, anger and related constructs are listed as associated symptoms for a number of disorders, including major depressive disorder (MDD), panic disorder (PD), generalised anxiety disorder (GAD), post-traumatic stress disorder (PTSD) and borderline personality disorder (BPD). Surprisingly, however, associations between anger and mental health disorders have received little research attention. Moreover, the clinical research that exists tends to focus on the Axis II disorders such as antisocial personality disorder (ASPD) and BPD (Baer and Sauer, 2011; Lobbestael et al., 2009). The few studies that examine the Axis I disorders, however, have indicated that anger is associated with a variety of mood, anxiety and substance use disorders (SUDs).
Anger has been shown to be positively associated with depression among individuals presenting for general psychiatric treatment (Newman et al., 2006) and depressed patients report more severe levels of anger and hostility compared to patients without depression and healthy controls (Fava and Rosenbaum, 1998; Riley et al., 1989; Sayar et al., 2000). As many as 30–49% of individuals with MDD and 28% with dysthymia have reported experiencing anger attacks (episodes of sudden and intense anger accompanied by symptoms of tachycardia, shaking, flushing, sweating and tightness of the chest) in a 6-month period (Fava et al., 1997; Sayar et al., 2000; Winkler et al., 2005). Individuals with bipolar depression (BD) report even higher rates of anger attacks, with rates between 53% and 62% (Benazzi, 2003; Perlis et al., 2004).
Similarly, individuals diagnosed with anxiety disorders frequently report experiencing symptoms of anger (Moscovitch et al., 2008). Approximately one-in-three patients (29–32%) with an anxiety disorder report experiencing anger attacks over a 6-month period (Gould et al., 1996). Among the anxiety disorders, PTSD is the most studied disorder in terms of its relationship with anger. It has been suggested that the relationship between PTSD and anger detected in research is simply a methodological artefact, whereby the two constructs are associated due to content overlap of the measures employed. Indeed, the DSM-IV-TR (APA, 2000) lists ‘irritability and outbursts of anger’ as one of the 17 symptoms delineating a diagnosis of PTSD. A number of studies, however, have demonstrated a correlation between PTSD symptom severity and multiple measures of anger even after anger items have been removed from the PTSD measures (Jakupcak et al., 2007; Orth et al., 2008).
Some studies have explored the association between anger and other anxiety disorders. Individuals with social phobia (SP), PD, GAD and obsessive compulsive disorder (OCD) have been shown to demonstrate higher levels of irritability and increased frequency and intensity of anger relative to controls (Baker et al., 2004; Erdem et al., 2008; Erwin et al., 2003; Fava et al., 1993; Whiteside and Abramowitz, 2005). Hawkins and Cougle (2011) analysed data collected as part of the National Comorbidity Survey-Revised (NCS-R), the only population-based study to date to have examined the association between anger and anxiety disorders. In this study, each anxiety disorder diagnosed at lifetime and 12 months was found to be positively associated with anger. These associations remained after controlling for demographic characteristics and other psychiatric comorbidities, including depression, BD, BPD and SUD.
Lastly, SUDs have been shown to be associated with symptoms of anger in clinical research. Individuals in treatment for a variety of SUDs self-report significantly elevated levels of anger compared to the general population (Reilly and Shopshire, 2000; Tivis et al., 1998). Individuals with SUD have also been shown to report elevated levels of state and trait anger and difficulties controlling anger compared to control samples (Aharonovich et al., 2001; Fernandez and Scott, 2009; Lin et al., 2004; Tivis et al., 1998). This association has been shown to exist after controlling for other comorbidities (Easton et al., 2007).
It is possible that individuals with mental health disorders experience anger as a result of their mental health symptoms. For instance, it has been argued that individuals with anxiety adopt feelings of anger in order to avoid more uncomfortable feelings associated with fear (fear avoidance theory) (Foa et al., 1995). For individuals with mood disorders, it has been suggested that depressive symptoms might lead to problems with anger regulation (Luutonen, 2007) and for those with SUDs, anger might result from the direct effects of the substances consumed or during substance withdrawal. It is also possible that anger can play a causal role in the development of mental health disorders. Indeed, high levels of trait aggression have been recorded for individuals with mood disorders (Painuly et al., 2007; Sayar et al., 2000), anxiety disorders (Trew and Alden, 2009) and SUDs (Easton et al., 2007).
Regardless of the direction of the association between anger and mental health disorders, the existing research has indicated that anger is associated with a range of mood, anxiety and substance use disorders. This research, however, tends to be restricted to the investigation of a limited number of comorbid disorders. In addition, the majority of studies have examined clinical samples and therefore may be subject to selection or referral bias (Berkson, 1946; Caron and Rutter, 1991). A large-scale investigation using a population sample would provide the context to control for a number of demographic and comorbid mental health characteristics that may account for heightened anger in the sample. Another major advantage of large-scale epidemiologic research is that samples are representative of the population of interest and therefore inferences can be made about that population.
To date, only one investigation of the mental health correlates of anger in a large-scale general population sample has been carried out (Hawkins and Cougle, 2011). Whilst this research has provided valuable insights, it was restricted to an examination of anxiety disorders. It is also unclear whether the findings reported in this study apply to the Australian population. Previous examinations of the 2007 Australian National Survey of Mental Health and Wellbeing (2007 NSMHWB) have revealed that mood, anxiety and substance use disorders are common in Australia and that many individuals suffer from more than one class of disorder (Slade et al., 2009; Teesson et al., 2009). An examination of anger across these disorders in the Australian general population, however, is yet to be performed. Such an examination would provide information on the prevalence of anger in the general population and also assist clinicians in the treatment and management of individuals with mental illness. Therefore, the aim of the present study is to identify the mental health correlates of anger in the Australian general population using data from the 2007 NSMHWB. Based on prior clinical and epidemiological research, we hypothesise that a range of mood, anxiety and substance use disorders will be associated with more severe levels of anger among individuals in the general population.
Method
Sample
The 2007 NSMHWB was a nationally representative face-to-face survey conducted by the Australian Bureau of Statistics (ABS), commissioned by the Australian Government Department of Health and Ageing. Interviews were carried out between August and December 2007. Participants were selected at random from a stratified, multistage area probability sample of private dwellings in Australia. The interview was completed by 8841 participants, representing a 60% response rate. A detailed description of the sampling design, methodology and sample characteristics has been provided elsewhere (Slade et al., 2009).
Structured questionnaire
A structured questionnaire was administered to participants. The demographic section assessed age, gender, education, employment and marital status, country of birth and prison history. The World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH CIDI 3.0; Kessler and Ustun, 2004) was used for the mental health diagnostic component of the survey. Thirty-day diagnoses ‘without hierarchy’ were derived based on lifetime diagnosis and the presence of symptoms of that disorder in the 30 days prior to interview. Diagnostic hierarchy rules were not applied in order to capture the true extent of comorbidity. Diagnoses of selected mood disorders (MDD, dysthymia, bipolar I and II), anxiety disorders (agoraphobia with or without PD, PD with or without agoraphobia, SP, GAD, OCD and PTSD) and SUDs (alcohol and drug abuse or dependence) were obtained based on the definitions and criteria of the DSM-IV. Alcohol use disorders (AUDs) were assessed for individuals who reported consuming at least 12 standard drinks in any 12-month period and drank a minimum of three standard drinks on at least one occasion during this period. Diagnoses of drug use disorders (DUDs) were obtained in relation to four classes of drugs: cannabis, stimulants, sedatives and opioids. DUDs were assessed for individuals who reported having used the substance more than five times in their lifetime.
The 2007 NSMHWB contained four ordinal items designed to measure the severity of anger symptoms in the 30 days prior to the interview. The first item asked how often respondents were ‘mad or angry’. Those who endorsed having experienced this at least ‘a little of the time’, were subsequently asked how often in the preceding 30 days they ‘were so angry they felt out of control’, ‘had an urge to hit, push or hurt someone’, or ‘had an urge to break or smash something’. Responses were recorded on a five-point Likert scale indicating: none of the time; a little of the time; some of the time; most of the time; or, all of the time. Answers were rated from 0 to 4 and scores across each item were summed to provide a total anger severity score for each participant, with a minimum possible score of 0 (indicting that a person did not experience feelings of anger at all) and a maximum possible score of 16 (indicating that a person experienced feelings of anger all the time, to the point where lack of control was felt and he/she had the urge to physically express that anger towards objects or other people). These 30-day anger items were also included in the NCS-R in the United States and demonstrated strong internal consistency (αstandardised = 0.81) (Hawkins and Cougle, 2011). Reliability analyses for the four items in the present study also demonstrated good internal consistency (αstandardised = 0.72). Hawkins and Cougle (2011) tested the validity of this anger severity measure and demonstrated that individuals diagnosed with intermittent explosive disorder (IED) in the NCS-R reported significantly greater anger symptoms than those without an IED diagnosis.
Analysis
To ensure the sample was representative of the general Australian population, data were weighted to conform to independent population estimates by state, part of state, age and gender. In addition, balanced repeated replicate weights were used to account for the complex survey sampling design. Descriptive statistics, prevalence estimates, mean anger severity scores and their standard errors were calculated. The total anger severity scores were positively skewed (skewness = 2.42) and therefore required a square root transformation, which reduced the skewness to 0.33. A series of simple linear regressions were conducted to identify demographic characteristics and mental health disorders significantly associated with anger severity. Multivariate linear regression analyses were carried out to determine which mental health disorders were independently associated with anger severity. All regression analyses were carried out using the transformed anger severity scores. To aid in interpretation, however, the mean anger scores from the original scale are provided. Unstandardised regression coefficients (β), standard errors (SEs) and corresponding alpha levels (p) are reported. All tests conducted were two-tailed using a predetermined alpha level of 0.05.
Results
Demographic characteristics associated with anger
The mean score for anger severity across the total sample was 1.25 (SE = 0.03). Among those with a 30-day mental health disorder diagnosis it was 2.46 (SE = 0.12), compared to 1.12 (SE = 0.02) for those without a current diagnosis. Simple regression analyses revealed that participants who reported more severe levels of anger were younger (β = −0.01, SE = 0.001, p < 0.001), less likely to be male (β = −0.10, SE = 0.02, p < 0.001) and less likely to be married (β = −0.13, SE = 0.02, p < 0.001). They were also more likely to have completed secondary education (β = 0.07, SE = 0.02, p = 0.003), to be employed (β = 0.22, SE = 0.02, p < 0.001) and to have been born in Australia (β = 0.08, SE = 0.03, p = 0.002). There were no significant effects for prison history.
Mental health characteristics associated with anger
Table 1 presents the mean anger scores across all 30-day mental health disorder diagnoses and the estimates and associated standard errors for the simple and multivariate regression analyses. Significant associations were found between each 30-day disorder and anger severity in the simple regressions and after controlling for demographic characteristics found to be significantly associated with anger severity (i.e. age, gender, marital status, education, employment status and country of birth). However, after controlling for demographic characteristics and all other disorders, MDD, BD, SP, GAD, OCD, PTSD, AUD and DUD remained significantly associated with anger severity. Younger age (β = −0.01, SE = 0.001, p < 0.001) and being female (β = −0.11, SE = 0.02, p < 0.001) were also significantly associated with anger after controlling for all other 30-day mental health disorders. The final model accounted for 13% of the total variance (R2 = 0.13). Multicollinearity was not detected for the independent variables included in the multiple regressions.
Weighted prevalence for 30-day DSM-IV disorders, mean anger severity scores, and regression analyses predicting anger severity (n = 8839).
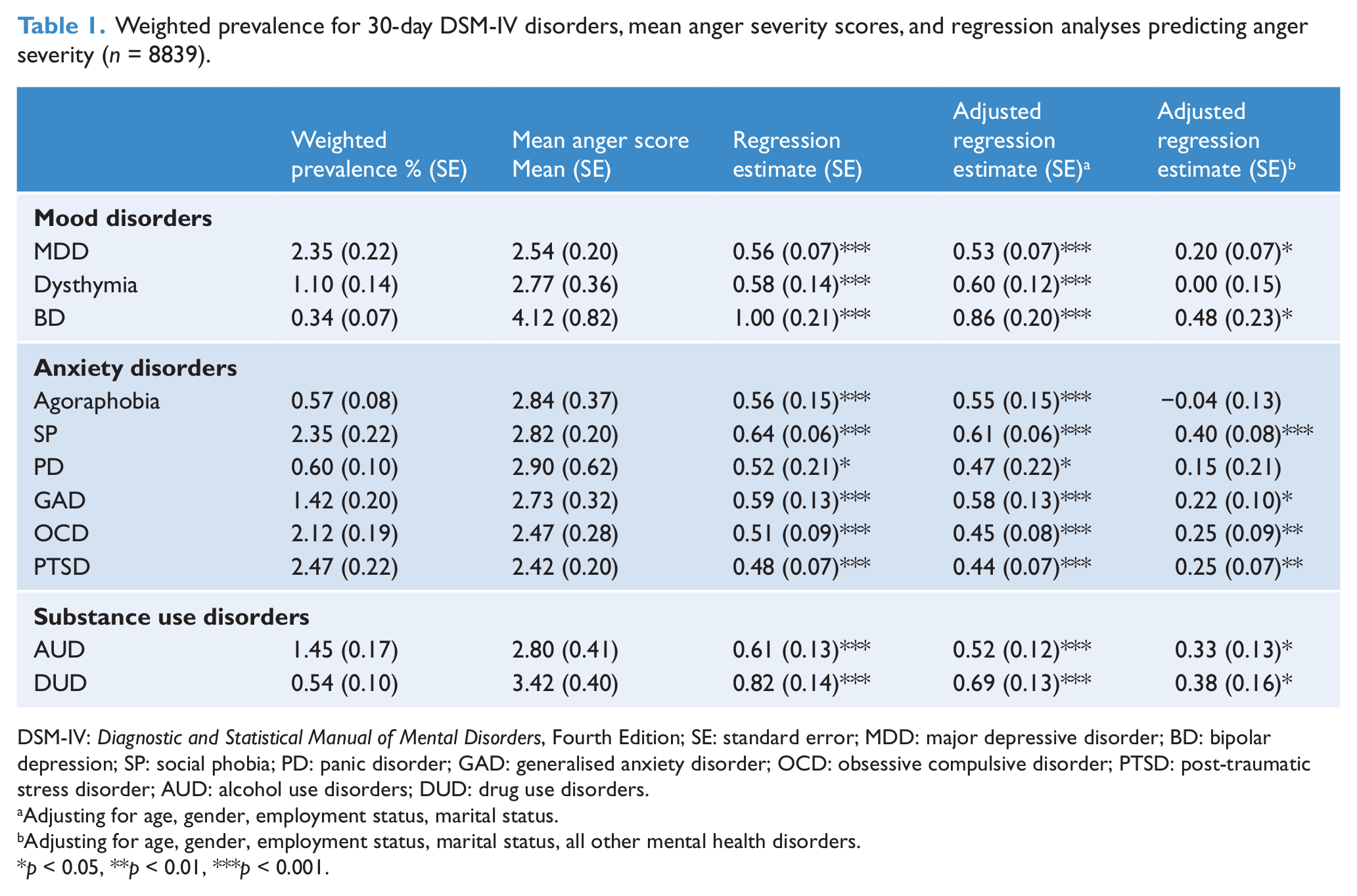
DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; SE: standard error; MDD: major depressive disorder; BD: bipolar depression; SP: social phobia; PD: panic disorder; GAD: generalised anxiety disorder; OCD: obsessive compulsive disorder; PTSD: post-traumatic stress disorder; AUD: alcohol use disorders; DUD: drug use disorders.
Adjusting for age, gender, employment status, marital status.
Adjusting for age, gender, employment status, marital status, all other mental health disorders.
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
The present study is one of the first large-scale epidemiological studies to examine the mental health correlates of anger in the general population. Each mood, anxiety and substance use disorder investigated was significantly associated with anger severity after controlling for demographic characteristics. These findings are in line with previous research demonstrating that individuals with mental health disorders experience elevated symptoms of anger in their day-to-day lives (Fava and Rosenbaum, 1998; Gould et al., 1996; Lin et al., 2004; Tivis et al., 1998). This evidence is concerning given the fact that heightened levels of anger are associated with maladaptive behaviours that can lead to negative consequences for the individual and for the community (Eckhardt et al., 2008; Novaco, 1994).
Individuals who were younger and those who were female reported more severe levels of anger after controlling for comorbid mental health disorders. This is consistent with research demonstrating that younger individuals tend to report more severe levels of anger compared to older individuals (Blanchard-Fields and Coats, 2008; Mahon et al., 2010). In relation to gender, however, previous research findings are not as clear. Males are generally considered to be ‘angrier’ than females; however, studies also indicate that while males are more likely to express anger, females are more likely to experience anger at higher levels than males (Bacskai et al., 2011; Campbell and Muncer, 2008). Given that the present study measured the experience of anger, it is not surprising that females reported more severe anger compared to males.
Diagnoses of MDD and BD were significantly associated with anger after controlling for demographics and comorbidity. These findings are consistent with clinical research demonstrating that individuals with these mood disorders are likely to report high levels of anger and experience anger attacks (Benazzi, 2003; Fava and Rosenbaum, 1998; Perlis et al., 2004; Sayar et al., 2000). Dysthymia, however, was not associated with anger severity in the present study. Although dysthymia is a chronic and disabling disorder, it is not as severe as MDD or BD (APA, 2000) and therefore may not be as strongly associated with anger compared to other more severe disorders.
A number of anxiety disorders were found to be independently associated with anger in the present study. Specifically, these were SP, GAD, OCD and PTSD. For PTSD these findings are not surprising, given the number of clinical studies evidencing an association between PTSD and anger. It has been proposed that individuals with PTSD have a lowered threshold for perceiving situations as threatening and that the perception of threat activates a biologically prepared survivor mode that induces anger reactions (survivor mode theory) (Chemtob et al., 1997). In relation to SP, it has been suggested that individuals develop heightened feelings of anger in response to perceived negative evaluation from others (Moscovitch et al., 2008). For GAD, on the other hand, it may be that individuals experience feelings of anger as a result of emotion regulation difficulties. It has been posited that they have deficits in their ability to soothe themselves when they experience negative emotions and avoid letting others know what they feel in order to prevent criticism and rejection, but they experience and express anger when their emotional needs are not met (Mennin et al., 2002). Lastly, for individuals with OCD, clinical research has argued that individuals with OCD experience anger as a result of frustration stemming from their beliefs of perfectionism and intolerance of uncertainty (Radomsky et al., 2007). The NCS-R did not assess for OCD and therefore Hawkins and Cougle (2011) did not include this disorder in their analyses. Given the findings of the present study and the dearth of literature in this area, future research exploring the associations between SP, GAD, OCD and anger is warranted.
There were no significant associations detected between anger severity and diagnoses of PD or agoraphobia after controlling for comorbid disorders. This suggests that any heightened anger detected among individuals with PD or agoraphobia may be attributable to the presence of other co-occurring disorders. Indeed, PD patients who report anger attacks also report more severe levels of depressive symptomatology compared to those without anger attacks (Gould et al., 1996).
Diagnoses of AUD and DUD, on the other hand, were significantly associated with anger severity after controlling for demographic characteristics and the presence of other comorbid disorders. The findings extend the clinical research that has consistently demonstrated associations between a variety of SUDs and elevated anger (Aharonovich et al., 2001; Easton et al., 2007). These findings also highlight the importance of including treatment approaches targeting anger in interventions for SUD. This is especially important given that anger has been shown to be associated with poor substance use treatment outcomes (Pekala et al., 2009; Witkiewitz and Villarroel, 2009).
Limitations
The findings in the present study should be considered in light of some limitations. First, the 2007 NSMHWB did not assess for personality disorders. Personality disorders such as BPD and ASPD often co-occur with a range of other mental health disorders and have been shown to be associated with anger (Baer and Sauer, 2011; Lobbestael et al., 2009; Tedlow et al., 1999). Future studies examining the correlates of anger should consider controlling for the influence of personality disorders in their analyses. Also, while this study identified demographic characteristics and specific mental health disorders that play a role in the severity of anger among individuals in the Australian general population, it is important to note that these accounted for only 13% of the total variance. Indeed, a number of other individual and situational factors not included in the present study could account for symptoms of anger in this sample.
It is also worth noting that the overall anger severity scores for those with mental health disorders appeared to be low. These scores, however, are consistent with those reported in Hawkins and Cougle’s (2011) analyses of the NCS-R. The anger items used in the 2007 NSMHWB and the NCS-R are relatively under-researched and it is not yet possible to calibrate total anger severity scores to any clinical reference point. It is therefore unclear whether the significant findings detected in the present study are of clinical significance. There is a need for further research on these anger items to establish such clinical cut-offs. Anger is a complex construct and, as such, a variety of instruments have been employed in research studies to measure clinically significant levels of anger. Future research investigating correlates of anger would benefit from studies that also utilise these validated measures. Finally, the data analysed in the present study are cross-sectional and therefore conclusions regarding causality cannot be determined. It is unclear whether the presence of a disorder plays a causal role in the experience of anger or whether individuals with a predisposition of trait anger are more susceptible to developing a mental health disorder. Given that levels of anger and psychiatric status can vary substantially for an individual over time, it is important for future research to carry out longitudinal studies to explore associations between the severity of mental health disorders and the severity of anger.
Conclusions
The current study is one of the first to employ population-level data to examine the associations between mental health disorders and anger. Although anger is a commonly experienced emotion, for some individuals anger can have extremely maladaptive effects on behaviour. The results of the present study suggest that individuals with common mental health disorders are prone to experiencing more severe levels of anger. As such, it is imperative that assessments of individuals presenting to mental health treatment services include a thorough assessment of anger symptomatology.
Footnotes
Acknowledgements
The 2007 NSMHWB was conducted by the Australian Bureau of Statistics and was funded by the Australian Government Department of Health and Ageing. The authors are responsible for the content and the writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.