
Abstract
Objective:
Given the burden of common psychiatric disorders and their consequent service and planning requirements, it is important to have a thorough knowledge of their distribution and characteristics in the population. Thus, we aimed to report the prevalence and age of onset of mood, anxiety and substance-use disorders in an age-stratified representative sample of Australian men.
Method:
Psychiatric disorders (mood, anxiety and substance-use disorders) were diagnosed utilising a structured clinical interview (Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition, Non-Patient Edition) for 961 men aged 24–98 years enrolled in the Geelong Osteoporosis Study. The lifetime and current prevalence of these disorders was determined from the study population and standardised to 2006 census data for Australia.
Results:
Approximately one in three men (28.8%, 95% confidence interval [CI] = [26.8%, 30.8%]) reported a lifetime history of any psychiatric disorder, with mood disorders (18.2%, 95% CI = [15.2%, 21.2%]) being more prevalent than anxiety (7.2%, 95% CI = [5.0%, 9.4%]) and substance-use disorders (12.9%, 95% CI = [9.7%, 16.0%]). Approximately 8.7% (95% CI = [7.5%, 10.0%]) were identified as having a current disorder, with 3.8% (95% interquartile range [IQR] = [2.2%, 5.4%]), 2.4% (95% CI = [1.1%, 3.8%]) and 3.4% (95% CI = [1.8%, 4.9%]) meeting criteria for current mood, anxiety and substance-use disorders, respectively. The median age of onset for mood disorders was 37.5 years (IQR = 27.0–48.0 years), 25.0 years (IQR = 20.0–40.3 years) for anxiety and 22.0 years (IQR = 18.0–34.3 years) for substance-use disorders.
Conclusion:
This study reports the lifetime and current prevalence of psychiatric disorders in the Australian male population. These findings emphasise the extent of the burden of these disorders in the community.
Keywords
Introduction
Mental and substance-use disorders are impairing, disabling and highly prevalent (Steel et al., 2014) and are a leading contributor to the global disease burden (Whiteford et al., 2013). The impact on the economy is vast, with over AUD$7.6 billion, or AUD$332 per person, estimated to be spent on mental health–related services in Australia during 2012–2013 alone (Australian Institute of Health and Welfare, 2014). Poor mental health has broader societal implications, with mental disorders leading to significant additional indirect costs, such as lost productivity and premature mortality. Although traditionally considered to be more prevalent in women, the evidence suggests that there are notable sex differences in how mental illness manifests, with women more likely to suffer from mood and anxiety disorders and men from substance-use disorders (Seedat et al., 2009).
Despite the efforts dedicated to early recognition of psychiatric disorders in public and clinical healthcare settings, an accurate representation of the true population burden is difficult to obtain due to widely varying population prevalence estimates, likely due to differing assessment tools, cultural norms and issues relating to confounding. Previous surveys conducted worldwide have estimated the lifetime prevalence of mood, anxiety and substance-use disorders in men and women to range between 3.3% and 21.4% (interquartile range [IQR] = 9.8–15.8%), 4.8% and 31.0% (IQR = 9.9–16.7%) and between 1.3% and 15% (IQR = 4.8–9.6%), respectively (Kessler et al., 2007b). In Australia, much of the available literature is restricted to clinical samples, limited by the use of self-reported data, or focused on specific age brackets, thus limiting insights into the burden of these disorders among the broader population. The best data currently available come from the 2007 National Survey of Mental Health and Wellbeing (NSMHW), which reported that almost half of the population (45.5%, 95% confidence interval [CI] = [44.1%, 46.9%]) aged between 16–85 years had experienced a mental disorder at some point in their lives, with 6.2% (95% CI = [5.5%, 6.9%]), 14.5% (95% CI = [13.4%, 15.3%]) and 5.1% (95% CI = [4.5%, 5.8%]) meeting criteria for 12-month mood, anxiety or substance-use disorder, respectively (Slade et al., 2009). The NSMHW used the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview to assess mental disorder prevalence. Limitations of this tool included lay administration and potential for under estimating lifetime prevalence in particular among the elderly (Haro et al., 2006; Snowdon et al., 2015), with a restricted range of mental disorders assessed, certain subgroups of the population not surveyed, and a lower than expected response rate being further limitations of the survey (Slade et al., 2009).
When planning public health interventions and managing disease, it is essential that we have a thorough knowledge of the distribution and characteristics of health in the population, in order to better target those at risk, allocate resources and to develop well-informed health-related plans. Optimally, these investigations should span the adult age range including the elderly, utilise gold-standard measures to aid in the correct identification of affected individuals and explore sex differences. Following on from our previous study describing the prevalence of mood and anxiety disorders in women utilising data collected between 2004 and 2008 (Williams et al., 2010), we thus aimed to investigate the prevalence and age of onset of mood, anxiety and substance-use disorders in an age-stratified, representative sample of Australian men using a gold-standard assessment tool.
Methods
Participants
This study examined data collected from men enrolled in the Geelong Osteoporosis Study (GOS) – a large cohort study involving an age-stratified, random population-based sample of women and men, developed to investigate the epidemiology of osteoporosis and other common diseases including mental disorders (Pasco et al., 2012). Participants were selected at random, irrespective of disease status, from the Commonwealth of Australia Electoral Rolls for the Barwon Statistical Division (BSD), which is a geographically well-defined area surrounding Geelong and located in south-eastern Australia. The total population according to the 2006 census for this area was 259,013. Of these, 126,889 were males, with 91,078 aged over 20 years. The BSD has been shown to be comparable to the Australian population in terms of age distribution, country of birth, school leavers’ age, marital status and weekly income, allowing findings from this sample to be extrapolated to national levels (Pasco et al., 2012).
Between 2001 and 2006, 1540 men (aged 20–93 years) agreed to participate in the GOS, with a response of 67.0%. Of this group, 978 men from the original sample returned for a 5-year follow-up appointment between 2006 and 2011 (81.0% response of those who were alive, capable of informed consent and still residing in the region). Reasons for non-participation are provided elsewhere (Pasco et al., 2012). From a potential pool of 978 men, participants for whom psychiatric data were not available (n = 17) were excluded from the analyses, resulting in a sample of 961 men aged 24–98 years eligible for inclusion. The study was approved by the Barwon Health Human Research Ethics Committee and written informed consent was obtained from all participants.
Assessments
At the 5-year follow-up appointment, the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition, Non-Patient Edition (SCID-I/NP) was used to assess the presence of past or current mood disorders, including major depressive disorder (MDD), minor depression, bipolar disorder (I, II and not otherwise specified [NOS]), dysthymia (current only), mood disorder due to a general medical condition (GMC) and substance-induced mood disorder; anxiety disorders, including panic disorder, agoraphobia, social phobia, specific phobia, obsessive-compulsive disorder (OCD), post-traumatic stress disorder, generalised anxiety disorder (current only), anxiety disorders due to a GMC, substance-induced anxiety disorder and anxiety disorders NOS; and substance-use disorders, including alcohol, amphetamine, cannabis, hallucinogen, opioid, phencyclidine and sedative/hypnotic/anxiolytic abuse and dependence (First et al., 2002). Further information regarding age of onset, hospitalisation and previous diagnoses was also gathered. All interviews were conducted by personnel with qualifications in psychology, who were trained using live and videotaped interviews under the supervision of a psychiatrist.
Height and weight were measured to the nearest 0.1 cm and 0.1 kg, respectively, and body mass index (BMI) calculated in kg/m2. Area-based socio-economic status (SES) was ascertained using Socio-Economic Index For Areas (SEIFA) index scores, based on the 2006 Australian Bureau of Statistics Census data, and then used to derive an Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) score accounting for high and low income and type of occupation. A low score identifies the most disadvantaged (quintile 1), while a high score identifies the most advantaged (quintile 5) (Brennan et al., 2009). Education (highest level completed) and country of birth were self-reported.
Statistical analyses
Statistical analyses were performed using Minitab (Version 16; Minitab, State College, PA). Differences in characteristics between the groups were determined using t-tests for continuous parametric variables, Kruskal–Wallis for non-parametric continuous variables and chi-square tests for discrete variables. The lifetime and current prevalence of psychiatric disorders was determined from the study population and direct standardisation applied using the 2006 census data from the Australian Bureau of Statistics population figures for Australia (Australian Bureau of Statistics, 2007). Median age of onset was also determined.
Results
Characteristics of the whole group (n = 961) and men with and without a lifetime psychiatric disorder are described in Table 1. There was no difference between those with and without a lifetime psychiatric disorder in regards to BMI, SES, education attainment and country of birth; however, those with a lifetime psychiatric disorder were younger. Approximately, one in three men (28.8%, 95% CI = [26.8%, 30.8%]) reported a lifetime history of any psychiatric disorder and one in 11 men (8.7%, 95% CI = [7.5%, 10.0%]) reported a current disorder at the time of interview. Of the total sample, 15.4% self-reported being previously diagnosed with a psychiatric disorder by a clinician (general practitioner, psychologist or psychiatrist), and 1.1% reported being hospitalised for a psychiatric disorder. At the time of interview, 10.5% were current users of psychotropic medications.
Characteristics of the whole group and men with and without a lifetime psychiatric disorder. Values are given as median (interquartile range), mean (standard deviation) or n (%).
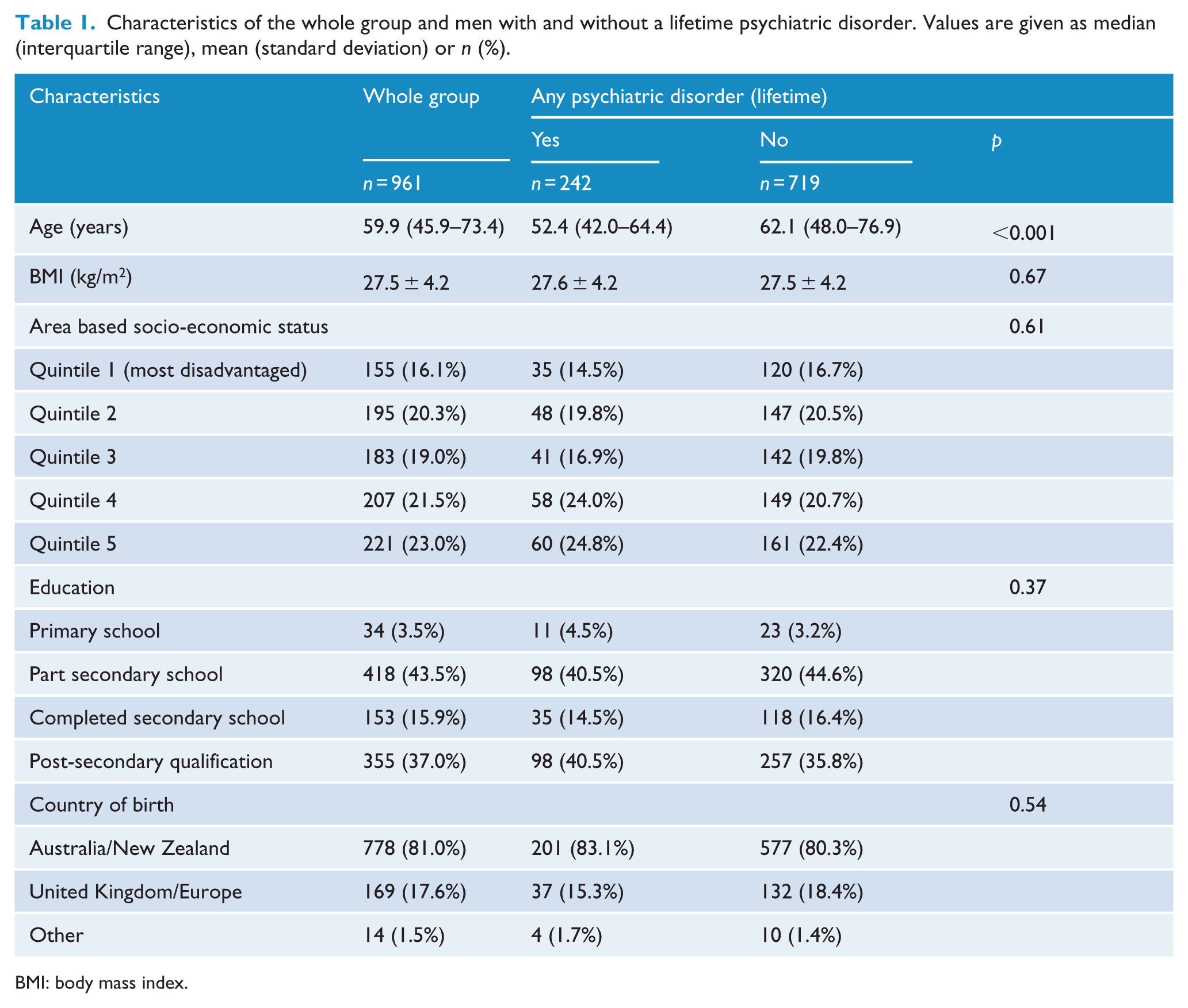
BMI: body mass index.
Mood disorders
The lifetime prevalence of any mood disorder was 18.2% (95% CI = [15.2%, 21.2%]). The most prevalent mood disorder was MDD, with 16.1% (95% CI = [13.2%, 18.9%]) of respondents reporting a lifetime history. Other mood disorders were less common; approximately 0.7% (95% CI = [0.2%, 1.1%]), 0.7% (95% CI = [0.3%, 1.7%]), 0.2% (95% CI = [0.02%, 0.4%]) and 0.1% (95% CI = [0.05%, 0.3%]) met criteria for a lifetime history of minor depression, bipolar disorder, mood disorder due to a GMC and substance-induced mood disorder, respectively (Figure 1). The median age of onset for any mood disorder was 37.5 years (IQR = 27.0–48.0 years) (Figure 2).
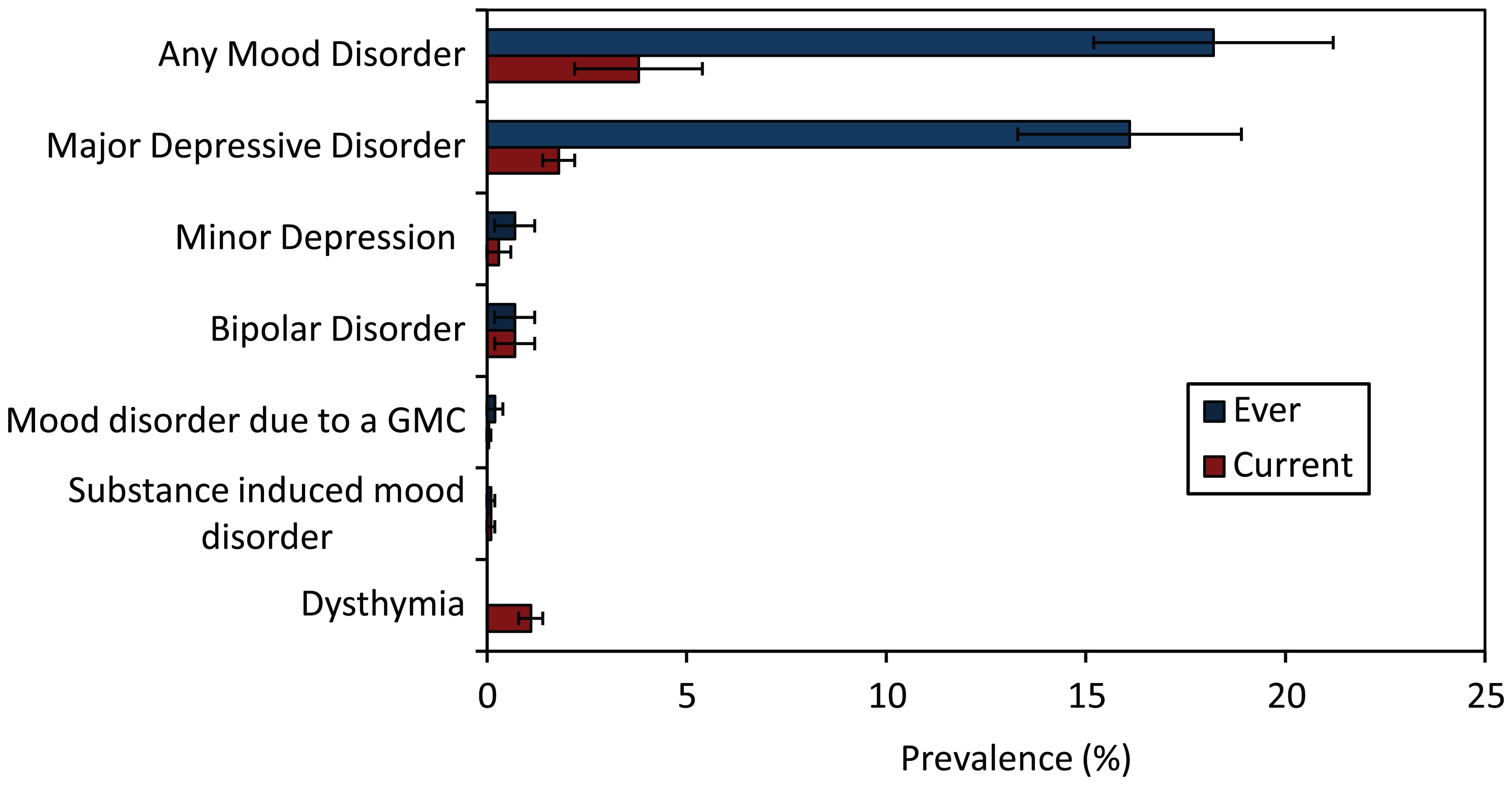
Lifetime and current prevalence of mood disorders standardised to Australian population (2006) (error bars represent 95% CI).
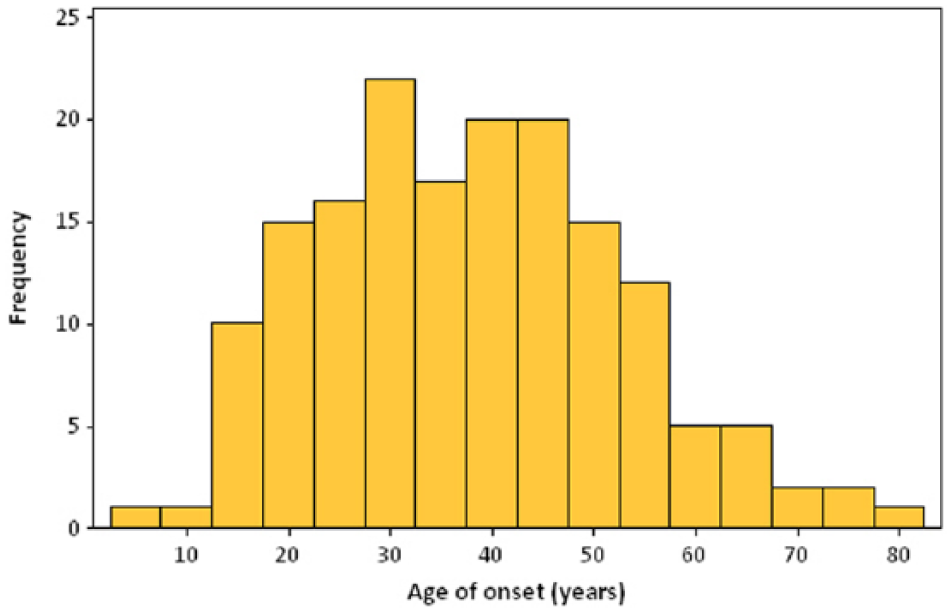
Age of onset distribution for any mood disorder.
Overall, 3.8% (95% CI = [2.2%, 5.4%]) of participants were identified as suffering from a current mood disorder. MDD was the most common current disorder, with 1.8% (95% CI = [1.4%, 2.3%]) meeting criteria at the time of interview, followed by dysthymia (1.1%, 95% CI = [0.7%, 1.4%]). The prevalence of the remaining mood disorders was low (Figure 1).
Anxiety disorders
The lifetime prevalence of any anxiety disorder at 7.2% (95% CI = [5.0%, 9.4%]) was considerably lower than the lifetime prevalence of any mood disorder. Panic disorder was the most common disorder, with 2.8% (95% CI = [1.3%, 4.2%]) meeting lifetime criteria, while post-traumatic stress disorder (1.3%, 95% CI = [0.6%, 2.1%]), specific (1.1%, 95% CI = [0.3%, 2.0%]) and social phobia (1.1%, 95% CI = [0.3%, 2.0%]) were the next most prevalent anxiety disorders. The other anxiety disorders were less common; approximately 0.9% (95% CI = [0.2%, 2.0%]) and 0.2% (95% CI = [0.02%, 0.4%]) met criteria for a lifetime history of OCD and anxiety disorder (NOS), respectively (Figure 3). No men met criteria for agoraphobia, anxiety disorders due to a GMC or substance-induced anxiety disorder The median age of onset for any anxiety disorder was 25.0 years (IQR = 20.0–40.3) (Figure 4).
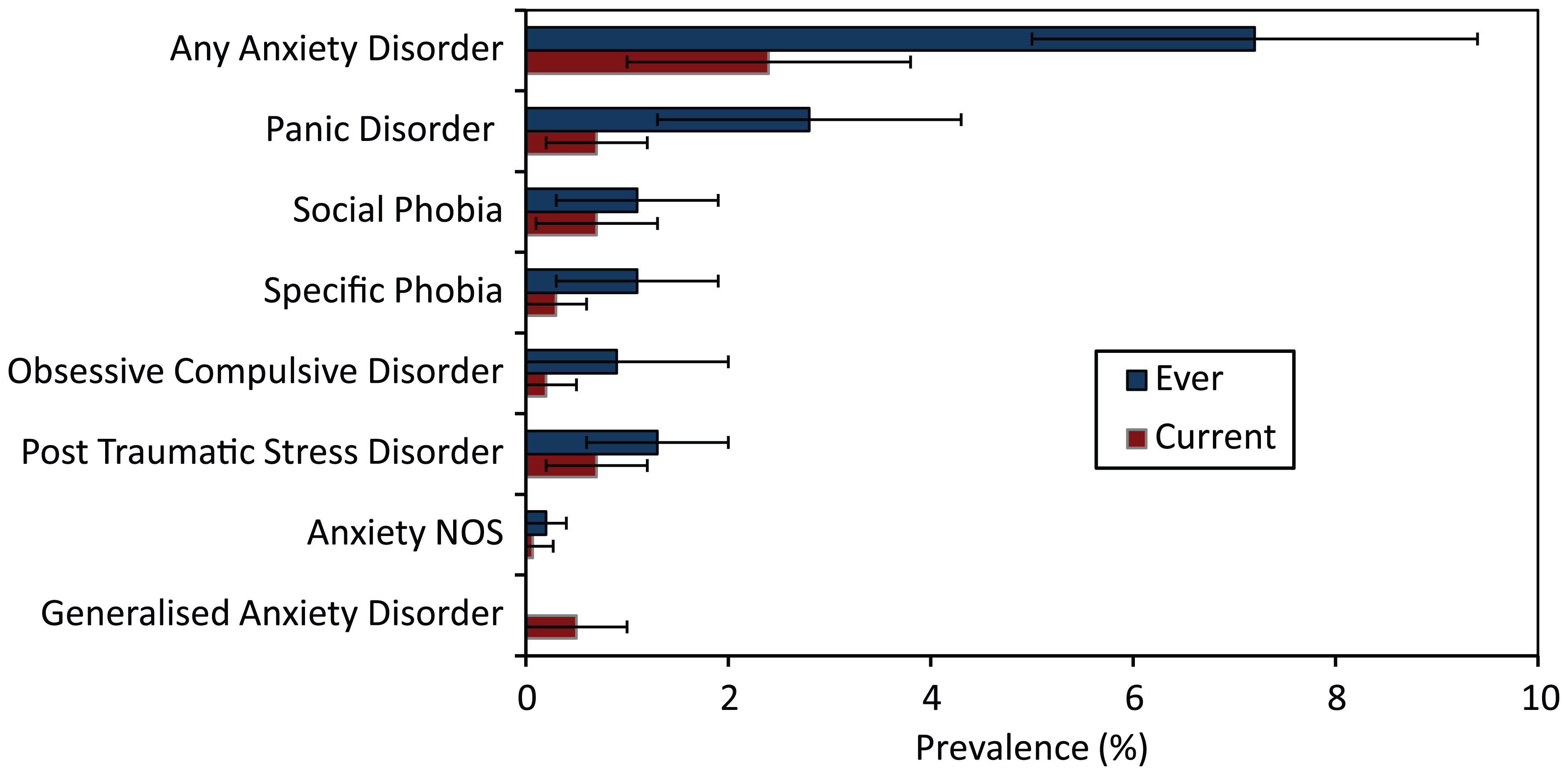
Lifetime and current prevalence of anxiety disorders standardised to Australian population (2006) (error bars represent 95% CI).
Age of onset distribution for any anxiety disorder.
The overall prevalence of current anxiety disorders was 2.4% (95% CI = [1.1%, 3.8%]), with the prevalence of each of the specific anxiety disorders being under 1.0% (Figure 3).
Substance-use disorders
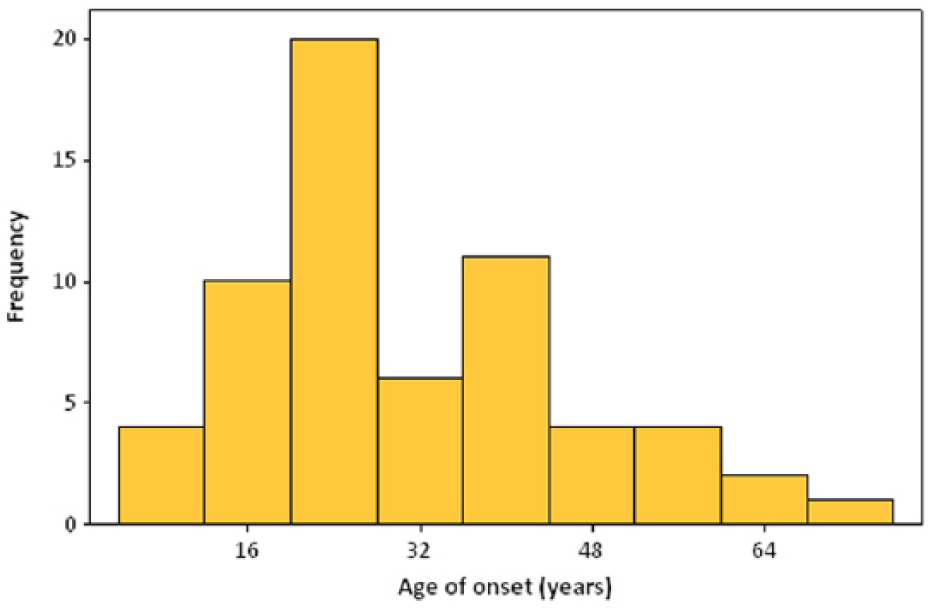
The lifetime prevalence of any substance-use disorder was 12.9% (95% CI = [9.7%, 16.0%]). In this sample, 4.7% (95% CI = [2.9%, 6.7%]) and 4.7% (95% CI = [2.9%, 6.7%]) met criteria for a lifetime history of alcohol abuse and dependence, respectively. The prevalence of drug use was considerably lower, with 1.5% (95% CI = [0.6%, 2.4%]) meeting lifetime criteria for drug abuse and 5.9% (95% CI = [3.4%, 8.4%]) for drug dependence (Figure 5). The median age of onset for any substance-use disorder was 22.0 years (IQR = 18.0–34.3) (Figure 6).
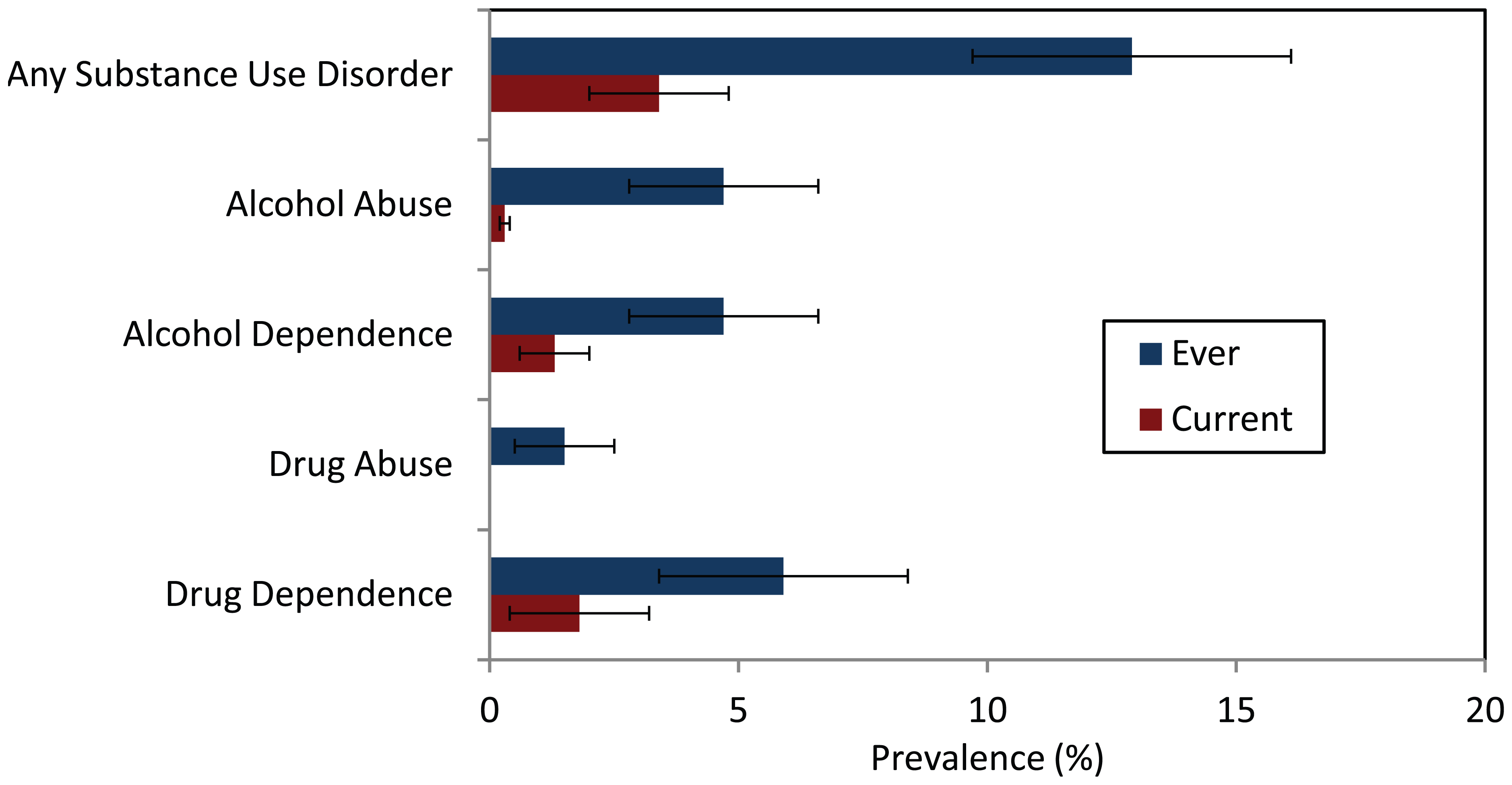
Lifetime and current prevalence of substance-use disorders standardised to Australian population (2006) (error bars represent 95% CI).
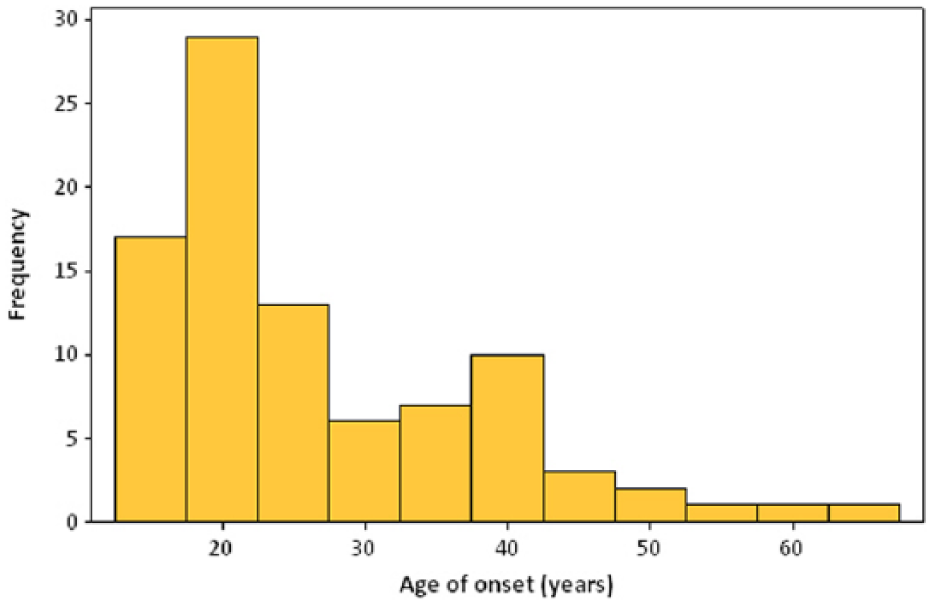
Age of onset distribution for any substance-use disorder.
The prevalence for any current substance-use disorder was 3.4% (95% CI = [1.8%, 4.9%]), with 0.3% (95% CI = [0.06%, 0.7%]) meeting criteria for current alcohol abuse, 1.3% (95% CI = [0.6%, 2.0%]) for alcohol dependence, 0% for drug abuse and 1.8% (95% CI = [0.5%, 3.2%]) for drug dependence (Figure 5).
Discussion
These findings are consistent with those of other epidemiological studies conducted worldwide in demonstrating that mood, anxiety and substance-use disorders are common in men (Boyd et al., 2015). Approximately, one in three men reported a lifetime history of any psychiatric disorder, with mood disorders being the most common, followed by substance-use disorders and then anxiety disorders. Approximately, one in 11 men reported a current disorder at the time of interview. The median age of onset varied for each of the disorders.
These data are also consistent in highlighting the discordance in the prevalence of psychiatric disorders between males and females. In our previous study in women, undertaken using the same methodology but nearly a decade earlier, we reported a lifetime prevalence of 30.0% (95% CI = [27.2%, 32.8%]) for any mood disorder (Williams et al., 2010), which is nearly double the rate we observed in men. Similarly, 13.5% (95% CI = [11.4%, 15.6%]) of women reported a lifetime history of anxiety disorder – again, nearly double that reported for men in this study. The age of onset for mood and anxiety disorders also varied between women and men, with a median age of onset of 27 years reported for mood disorders in women, which is a full decade younger than that reported for men. Women also experienced the onset of anxiety disorders several years earlier (18.5 years) than men. We cannot compare substance-use disorder prevalence between the sexes as we did not assess these disorders in the female study; however, it is commonly the case that these disorders are more prevalent in men (Seedat et al., 2009).
As part of the World Mental Health Survey Initiative, the lifetime prevalence of internalising (mood, anxiety) and externalising disorders (addictive disorders) was determined for the 10 participating European countries (Boyd et al., 2015). The lifetime prevalence of any mental disorder for men ranged between 11.6% and 39.3%, with prevalence of 2.6–13.9% for mood disorders, 4.1–16.2% for anxiety disorders and 2.4–21.2% for alcohol use disorders. Consistent with our findings, sex discrepancies were evident and consistent across the countries, with internalising disorders being more common among women and externalising disorders more common in men. A systematic review and meta-analysis incorporating 174 surveys worldwide, totalling 829,673 respondents, was recently conducted providing aggregated estimates of the lifetime prevalence of the common mental disorders (Steel et al., 2014). For men, the pooled lifetime prevalence of any mental disorder was 31.6% (95% CI = [28.6%, 34.8%]), 7.3% (95% CI = [6.3%, 8.5%]) for mood disorder, 10.1% (95% CI = [8.8%, 11.6%]) for anxiety disorder and 17.1% (95% CI = [14.4%, 20.3%]) for substance-use disorder. The lifetime prevalence of mental disorders among older Australians (65–85 years) participating in the NSMHW has been documented by sex (Sunderland et al., 2015). The lifetime prevalence of any mental disorder was 31.6% and 6.9% for mood disorders, 8.5% for anxiety disorders and 22.8% for substance-use disorders. Men were more likely to meet criteria for a mental disorder overall and substance-use disorders, and women, anxiety disorders. Our findings concur broadly with the aforementioned studies investigating lifetime prevalence rates in men, although the prevalence of mood disorders was somewhat higher in our current study; the inclusion of all mood disorders including those associated with organic pathology and the sensitivity of the tool used is likely to explain some of the discrepancies.
Also consistent with previous studies is the reported earlier age of onset for substance-use disorders compared with mood and anxiety disorders. Information concerning age of onset is important in aiding the understanding of causes and mechanisms and in guiding public health interventions. A review of epidemiological research investigating age of onset reported the median age of onset for mood disorders ranged between 25 and 45 years (IQR = 17–65 years), 18 and 29 years (IQR = 16–43 years) for substance disorders, 7 and 14 years (IQR = 4–20 years) for phobias and between 25 and 53 years (IQR = 15–75 years) for other anxiety disorders – panic disorder, generalised anxiety disorder and post-traumatic stress disorder (Kessler et al., 2007a). Summarised in a report by Jones, the median age of onset for mood, anxiety and substance-use disorders for those participating in the National Comorbidity Survey Replication (NCS-R) was 30, 11 and 20 years, respectively, with the age of onset range being somewhat concentrated for substance use (IQR = 18–27 years) and anxiety disorders (IQR = 6–21 years), compared to 25 years (IQR = 18–43 years) for mood disorders (Jones, 2013). In our study, the age of onset range for each of the disorders was similar.
Overall, our findings indicate the prevalence of psychiatric disorders among men in the general population and provide up-to-date data that are needed for targeting population healthcare planning and service provision. While it is understood that men are as likely as women to suffer from a psychiatric disorder, they are less likely to utilise health services and have a higher mortality rate associated with suicide; why such differences exist remains unclear. Lack of awareness and understanding, stigma and help-seeking barriers are a few of the many reasons used to explain the difference (Barney et al., 2006; Smith et al., 2006). Highlighting the magnitude of a problem and using such information as a tool to increase awareness is essential when attempting to improve health and bring about change.
There are both strengths and potential weaknesses that need to be taken into consideration when interpreting the findings. First, when measuring lifetime prevalence, recall bias is likely to be an issue. This could also be expected to affect the accuracy of age of onset data, with age at interview, in combination with the length of time between onset and recall, being potentially important factors influencing the accuracy of our data. However, the use of a gold-standard semi-structured clinical interview, wherein participants were encouraged to actively recall previous illnesses in great detail, may have reduced the impact of such biases. Second, the psychiatric profile of GOS non-respondents may have differed from responders; thus, it is not unrealistic to suggest that reported rates are underestimated. As this is a cohort study, we cannot exclude the possibility of differential loss to follow-up associated with psychopathology. Moreover, low prevalence disorders such as schizophrenia or other psychotic disorders were not identified and data on health service utilisation, disability or help-seeking behaviours were not available. Last, direct comparison to other studies in the literature was limited due to inter-survey heterogeneity including different tools, time periods, included disorders and a failure to distinguish prevalence rates between the sexes.
In summary, these findings provide important epidemiological data in men derived from the use of a gold-standard psychiatric assessment tool. The highly representative nature of the GOS sample affords extrapolation of these findings to the wider Australian population. The results reinforce our understanding of the high prevalence of these psychiatric disorders in men and provide important information that can be utilised in public health and clinical initiatives and for economic and service planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.J.W. has received Grant/Research support from Eli Lilly, Pfizer, The University of Melbourne, Deakin University and the National Health and Medical Research Council (NHMRC). F.N.J. has received Grant/Research support from the Brain and Behaviour Research Institute, the NHMRC, Australian Rotary Health, the Geelong Medical Research Foundation, the Ian Potter Foundation, Eli Lilly, the Meat and Livestock Board and The University of Melbourne and has been a paid speaker for Sanofi-Synthelabo, Janssen Cilag, Servier, Pfizer, Health Ed, Network Nutrition, Angelini Farmaceutica and Eli Lilly. J.A.P. has received grant/research support from the NHMRC, BUPA Foundation, Deakin University, Barwon Health and the Western Alliance. C.E.C., S.E.Q. and A.L.S. have no conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript. M.B. has received Grant/Research Support from the Stanley Medical Research Foundation, MBF, NHMRC, Beyond Blue, Geelong Medical Research Foundation, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Organon, Novartis, Mayne Pharma, Servier and Astra Zeneca. He has been a paid consultant for Astra Zeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Janssen Cilag, Lundbeck and Pfizer and a paid speaker for Astra Zeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Janssen Cilag, Lundbeck, Organon, Pfizer, Sanofi-Synthelabo, Solvay and Wyeth.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the National Health and Medical Research Council (NHMRC), Australia (projects 299831, 628582, 1026265, 1021345). L.J.W. is supported by a NHMRC Career Development Fellowship (1064272). S.E.Q. is supported by a NHMRC Public Health and Health Services Research Postgraduate Scholarship (1076347). M.B. is supported by a NHMRC Senior Principal Research Fellowship (1059660). The funding providers played no role in the design or conduct of the study; collection, management, analysis and interpretation of the data; or in preparation, review, or approval of the manuscript.