
Abstract
Objective:
Psychotic versus non-psychotic patients with bipolar disorder have been traditionally associated with different unfavorable clinical features. In this study on bipolar Italian patients, we aimed to compare clinical and demographic differences between psychotic and non-psychotic individuals, exploring clinical factors that may favor early diagnosis and personalized treatment.
Methods:
A total of 1671 patients (males: n = 712 and females: n = 959; bipolar type 1: n = 1038 and bipolar type 2: n = 633) from different psychiatric departments were compared according to the lifetime presence of psychotic symptoms in terms of socio-demographic and clinical variables. Chi-square tests for qualitative variables and Student’s t-tests for quantitative variables were performed for group comparison, and a multivariable logistic regression was performed, considering the lifetime psychotic symptoms as dependent variables and socio-demographic/clinical characteristics as independent variables.
Results:
Psychotic versus non-psychotic bipolar subjects resulted to: be more frequently unemployed (p < 0.01) and never married/partnered (p < 0.01); have an earlier age at onset (p < 0.01); more frequently receive a first diagnosis different from a mood disorder (p < 0.01); have a shorter duration of untreated illness (p < 0.01); have a more frequently hypomanic/manic prevalent polarity (p < 0.01) and a prevalent manic–depressive type of cycling (p < 0.01); present a lower lifetime number of depressive episodes (p < 0.01), but have more manic episodes (p < 0.01); and less insight (p < 0.01) and more hospitalizations in the last year (p < 0.01). Multivariable regression analysis showed that psychotic versus non-psychotic bipolar patients received more frequently a first diagnosis different from bipolar disorder (odds ratio = 0.64, 95% confidence interval = [0.46, 0.90], p = 0.02) or major depressive disorder (odds ratio = 0.66, 95% confidence interval = [0.48, 0.91], p = 0.02), had more frequently a prevalent manic polarity (odds ratio = 1.84, 95% confidence interval = [1.14, 2.98], p < 0.01) and had a higher number of lifetime manic episodes (more than six) (odds ratio = 8.79, 95% confidence interval = [5.93, 13.05], p < 0.01).
Conclusion:
Lifetime psychotic symptoms in bipolar disorder are associated with unfavorable socio-demographic and clinical features as well as with a more frequent initial misdiagnosis.
Introduction
Bipolar disorder (BD) is a prevalent psychiatric condition, frequently associated with prominent disability and social dysfunction (Martino et al., 2017). Long-term stabilization of bipolar subjects may be challenging for clinicians (Malhi et al., 2018), and different clinical factors have been associated with insufficient response to pharmacological treatment and poor outcome (Alda and Manchia, 2018), including early age at onset (Dell’Osso et al., 2009), advanced age (Sajatovic et al., 2015), long duration of illness (Altamura et al., 2015b), presence of rapid-cycling (Buoli et al., 2017), comorbidity with substance-use disorders (Strakowski et al., 2007) and psychotic symptoms (Altamura et al., 2015a; Ostergaard et al.,2013). Indeed, psychotic symptoms are frequently reported by subjects suffering from BD, being experienced by at least 68% of them (Keck et al., 2003). Of note, up to 50% of patients with a manic episode can manifest psychotic symptoms (Azorin et al., 2007) and more than half of the patients with bipolar depression may report delusions or hallucinations (Dilsaver et al., 1997). In a recent Italian study, the lifetime presence of psychotic symptoms in BD was found to be associated with worse clinical features, including early age at onset, more substance abuse and lifetime hospitalizations (Dell’Osso et al., 2017), consistently with other previously published data (Coryell et al., 2001; Kessing, 2004). Furthermore, psychotic bipolar patients were found to have more working impairment and social dysfunction than non-psychotic ones (Van Rossum et al., 2008). In light of their clinical severity, the treatment of psychotic bipolar patients may be particularly challenging and require combined pharmacotherapy both in the acute phase (Bjørklund et al., 2017) and in the long term (Buoli et al., 2014).
Different factors may contribute to a greater severity of illness and to a poorer prognosis for psychotic versus non-psychotic bipolar subjects. For instance, patients with a psychotic BD often receive a delayed proper treatment, as a consequence of misdiagnosis with other psychotic disorders, in particular with delusional disorder and schizophrenia (Altamura et al., 2015a). In addition, more pronounced biological abnormalities might be responsible for a greater clinical severity of psychotic versus non-psychotic bipolar subjects (Buoli et al., 2016a). Specifically, psychotic bipolar patients were found to have higher kynurenic acid levels in the cerebrospinal fluid, more hormonal abnormalities and brain changes (Ong et al., 2012) than non-psychotic bipolar subjects (Buoli et al., 2016a, 2016b).
In light of these considerations, the purpose of this study was to investigate, in a large multicenter sample of Italian bipolar patients, the possible clinical and demographic differences between psychotic and non-psychotic individuals with the aim of identifying clinical factors that may favor an early diagnosis and a personalized treatment for this subtype of patients. Of note, we assessed the generalizability of the results of a preliminary single-center Italian study (Dell’Osso et al., 2017) in a multicenter national study with a much larger sample size.
Methods
An overall sample of 1671 bipolar subjects was enrolled from different Italian psychiatric clinics. The protocol was approved by the local Ethical Committees. Patients had a diagnosis of BD according to Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) criteria (American Psychiatry Association, 2000). Diagnoses were made by expert psychiatrists, who had regularly followed up the selected patients and confirmed by the Mini-International Neuropsychiatric Interview (MINI; Buoli et al., 2018; Sheehan et al., 1998). Patients consecutively afferent to outpatient or inpatient services were included in the study. We included the centers of which staff routinely uses structured interviews for psychiatric diagnosis. No restriction criteria have been established in relation to the presence of academic facilities or geographical aspects to limit confounding factors associated with the type of care (general hospitals versus academic hospitals) or territory specificities. Clinical information was extrapolated through a review of the clinical charts and clinical interviews with patients and available relatives. Data were entered into an electronic central database (electronic case report form [e-CRF]). Collected data included the following socio-demographic and clinical variables divided in three clusters:
Cluster 1 (socio-demographic variables): age, gender, education, employment, marital status (at least one marriage or partnership) and living alone;
Cluster 2 (lifetime clinical variables): age at onset of BD, age at first pharmacological prescription (including benzodiazepines), age at first contact with psychiatric services, first psychiatric diagnosis, age at first psychiatric diagnosis, age at first diagnosis of BD, age at first mood stabilizer/atypical antipsychotic, duration of illness, duration of untreated illness, polarity of first episode, lifetime number of manic episodes, lifetime number of depressive episodes, prevalent polarity and prevalent type of cycling;
Cluster 3 (clinical variables—last year of observation): type of current episode, number of hypomanic/manic episodes, number of depressive episodes, presence and number of attempted suicides and the degree of lethality, comorbidity with substance-use disorders, presence of hospitalizations, presence of insight, attribution of symptoms to a psychiatric disorder, treatment adherence, number of visits, administration of psychoeducational interventions (according to Colom’s model) (Vieta et al., 2009).
We did not include the type of BD (1 or 2) as predictor of lifetime history of psychotic symptoms because this analysis has been previously performed on the same sample with a slightly lower number of cases (N = 1500). Of note, patients with BD type 1 showed significantly higher probability to experience lifetime psychotic symptoms than BD type 2 patients (p < 0.01) (Altamura et al., 2018).
Duration of untreated illness was considered as the time elapsing between first episode of BD and the prescription of a proper pharmacological treatment (mood stabilizer or atypical antipsychotic with stabilizing effects) (Altamura et al., 2015a).
Prevalent polarity was calculated according to the Barcelona proposal, defined as at least two-thirds (2/3) of the total number of past episodes being from the same polarity (Colom et al., 2015).
Lethality of suicide attempts was rated according to global impression of Scale for Assessment of Lethality of Suicide Attempt (score 1–2: low; score 3: medium; score 4–5: high) (Kar et al., 2014).
Exclusion criteria were the following: (1) patients who had not been examined in the last 12 months for the impossibility to collect data of cluster 3 variables (last year of observation); (2) patients whose clinical information were incomplete; (3) patients with a diagnosis of dementia, mental retardation or other medical conditions (e.g. untreated endocrine disorders) associated with an increased risk of psychotic symptoms or other clinical features (e.g. suicidal attempts). Of note, a recent review highlighted that secondary psychotic symptoms may be due to a number of neurological conditions including stroke, Alzheimer’s disease, Parkinson’s disease, paraneoplastic encephalitis or traumatic brain injury (Arciniegas, 2015). Patients with current or history of these conditions as well as with main endocrine diseases associated with increased risk of psychotic symptoms (untreated thyroid diseases and Cushing’s syndrome) have been excluded in this analysis (Santos et al., 2017). In addition, the presence or history of the following medical comorbidities, which have been associated with largely increased risk of suicide, was considered as exclusion criteria: myocardial infarction, previously mentioned neurological conditions and diagnosis of malignant cancer (Fässberg et al., 2016).
Descriptive analyses of the total sample were performed. The total sample was then divided in two groups according to the presence of lifetime psychotic symptoms. The two groups were compared for the above-mentioned variables by t-tests for quantitative variables and chi-square tests for qualitative ones.
Owing to the large number of variables statistically related to the dependent variable (the presence of lifetime psychotic symptoms) at the univariate analyses, preliminary multiple logistic regression analyses (one for each of the above-mentioned clusters) were performed including only statistically significant variables. Finally, statistically significant variables from these final models were inserted in a new global starting multivariable logistic regression model (adjusted for gender) in order to obtain the variables independently associated with the presence of lifetime psychotic symptoms. The choice to adjust the final model for gender was due to the fact that another analysis on the sample showed demographic and clinical differences according to this variable, although no statistically significant difference in gender distribution was found with regard to lifetime presence of psychotic symptoms (Buoli et al., in press). In addition, male hormones are hypothesized to be involved in the susceptibility to psychotic symptoms (Van Rijn et al., 2011). Finally, it is a standard statistical procedure ‘to adjust’ for some potential confounders in multivariable analyses, even independently from their statistical or not association with the dependent variable.
The selection of the variables was done according to a backward procedure; the goodness of fitting was assessed by the Hosmer–Lemeshow test. The level of statistical significance was set at p ⩽ 0.05. Statistical analyses have been performed by SAS® 9.2 version.
Results
The total sample included 1671 patients: 712 males (42.6%) and 959 females (57.4%); bipolar type 1: n = 1038 (62.1%) and bipolar type 2: n = 633 (37.9%). Patients had an age between 18 and 80 years (mean: 48.60 ± 13.36 years). Descriptive analyses of the total sample and groups divided according to the presence of lifetime psychotic symptoms are reported in Tables 1–3.
Socio-demographic variables of the total sample and of the two groups obtained according to the presence of lifetime psychotic symptoms.
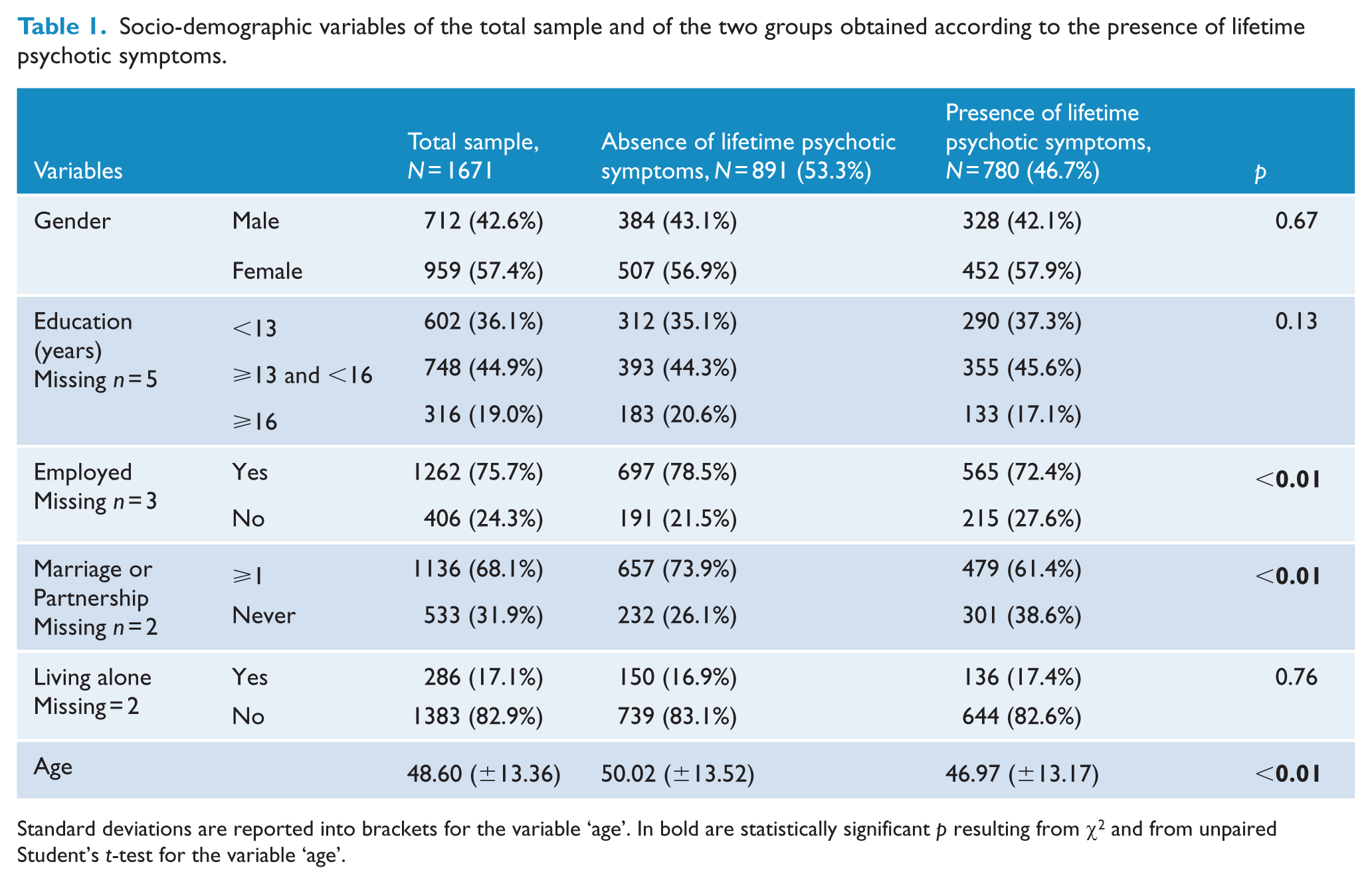
Standard deviations are reported into brackets for the variable ‘age’. In bold are statistically significant p resulting from χ2 and from unpaired Student’s t-test for the variable ‘age’.
Clinical variables of the total sample and of the two groups obtained according to the presence of lifetime psychotic symptoms.
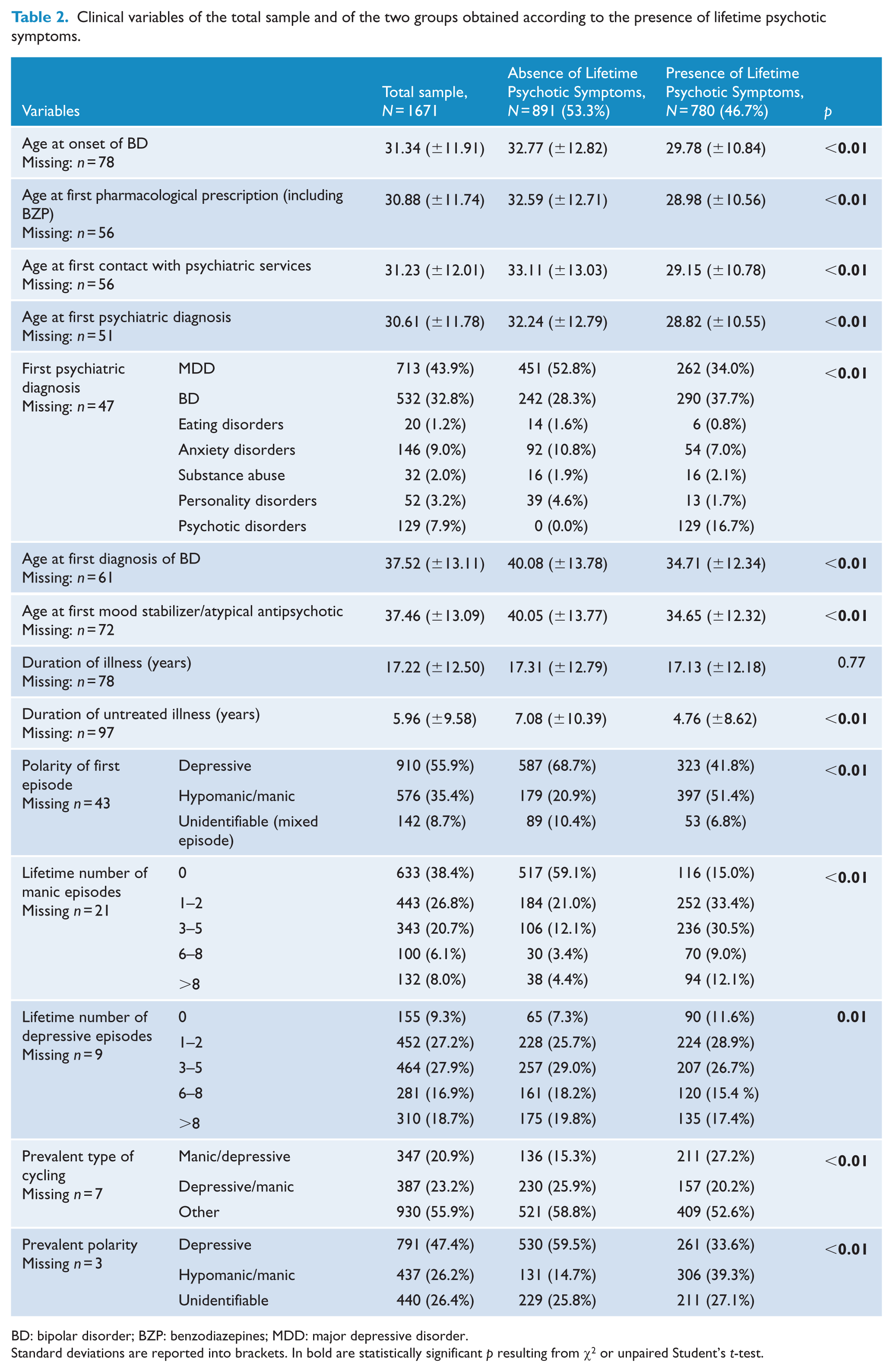
BD: bipolar disorder; BZP: benzodiazepines; MDD: major depressive disorder.
Standard deviations are reported into brackets. In bold are statistically significant p resulting from χ2 or unpaired Student’s t-test.
Clinical variables of the total sample and of the two groups obtained according to the presence of lifetime psychotic symptoms (last year of observation).
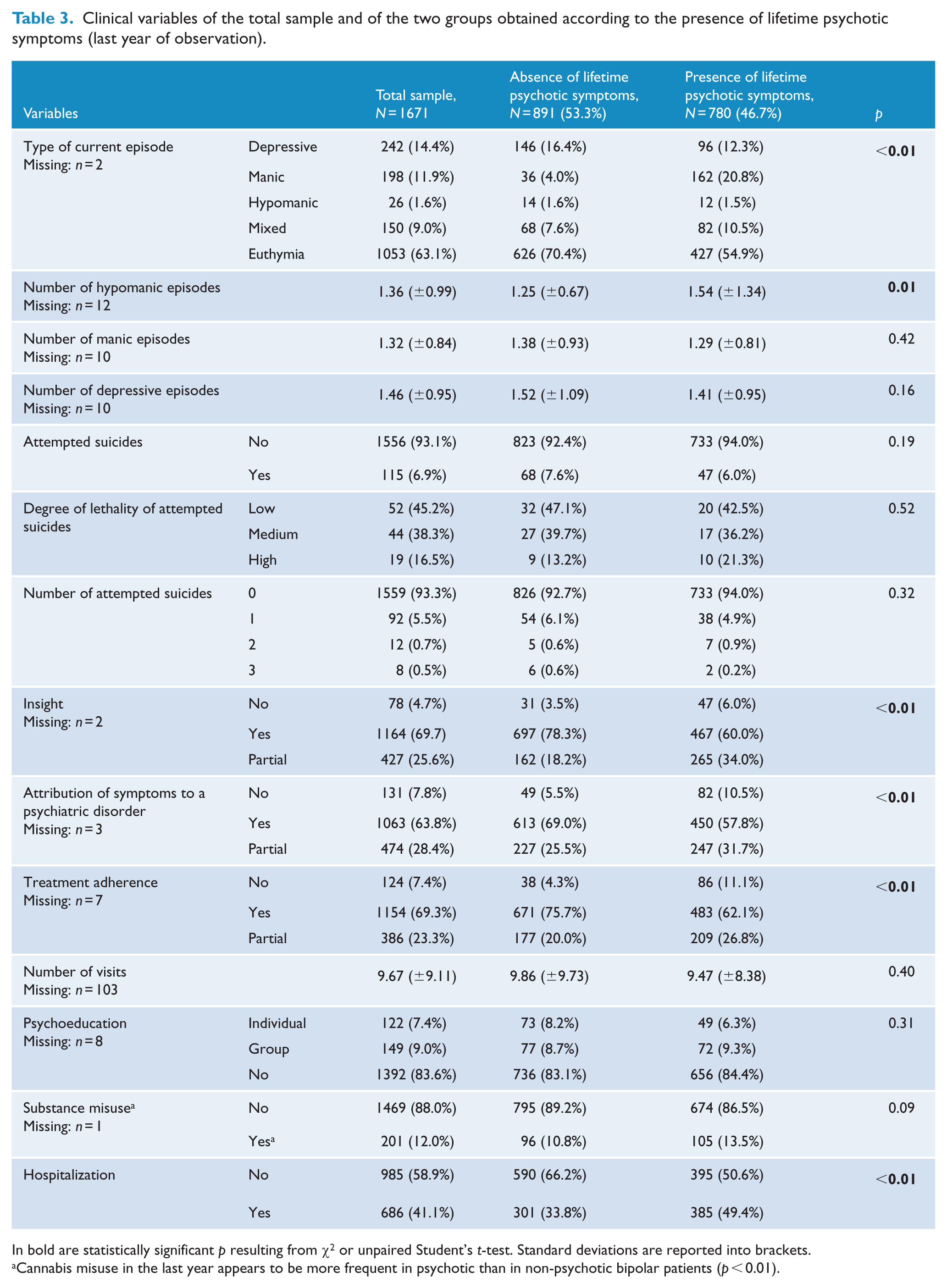
In bold are statistically significant p resulting from χ2 or unpaired Student’s t-test. Standard deviations are reported into brackets.
Cannabis misuse in the last year appears to be more frequent in psychotic than in non-psychotic bipolar patients (p < 0.01).
There were no significant differences between psychotic versus non-psychotic bipolar subjects in terms of gender distribution (p = 0.67), years of education (p = 0.13), living alone status (p = 0.76), duration of illness (p = 0.77), number of manic episodes in the last year (p = 0.42), number of depressive episodes in the last year (p = 0.16), presence of suicide attempts in the last year (p = 0.19), degree of lethality of suicide attempts in the last year (p = 0.52), number of suicide attempts in the last year (p = 0.32), number of psychiatric visits in the last year (p = 0.40), administration of psychoeducation interventions (p = 0.31) and presence of substance abuse in the last year (p = 0.09).
However, psychotic bipolar subjects (compared to non-psychotic ones) resulted to be younger (p < 0.01), more frequently unemployed (p < 0.01), to be never married or in partnership (p < 0.01), to have an earlier age at onset (p < 0.01), to have an earlier age at first pharmacological prescription (p < 0.01), to have an earlier age at first contact with psychiatric services (p < 0.01), to have an earlier age at first psychiatric diagnosis (p < 0.01), to have an earlier age at first diagnosis of BD (p < 0.01), to have an earlier age at first mood stabilizer or atypical antipsychotic prescription (p < 0.01), to have received more frequently a first diagnosis different from a mood disorder (in most of cases of a psychotic disorder) (p < 0.01), to have a shorter duration of untreated illness (p < 0.01), to have a more frequent hypomanic/manic polarity of first episode (p < 0.01), to have a more frequent hypomanic/manic prevalent polarity (p < 0.01), to have more frequently a prevalent manic-depressive type of cycling (p < 0.01), to present a lower lifetime number of depressive episodes (p < 0.01), to present more lifetime manic episodes (p < 0.01), to have a more frequent current manic episode (p < 0.01), to have a higher number of hypomanic episodes in the last year (p = 0.01), to be more frequently cannabis users in the last year (p < 0.01), to have more frequently no or partial insight (p < 0.01), to less frequently attribute symptoms to a psychiatric disorder (p < 0.01), to present less treatment adherence (p < 0.01) and to have more hospitalizations in the last year (p < 0.01).
The results of the goodness-of-fit test (Hosmer–Lemeshow test: χ2 = 7.52, df = 8, p = 0.48) showed that multivariable logistic regression model including socio-demographic/clinical variables as possible predictors of the lifetime presence of psychotic symptoms (adjusted for gender) was adequate. In particular, psychotic bipolar patients versus non-psychotic ones resulted to have received more frequently a first diagnosis different from BD (OR = 0.64, p = 0.02) or major depressive disorder (MDD) (OR = 0.66, p = 0.02) (Figure 1), to have a prevalent manic polarity (OR = 1.84, p < 0.01), to present a higher number of lifetime manic episodes (more than six) (OR = 8.79, p < 0.01) and to have less frequently at least one major depressive episode in the last year (OR = 0.66, p < 0.01) (Table 4).
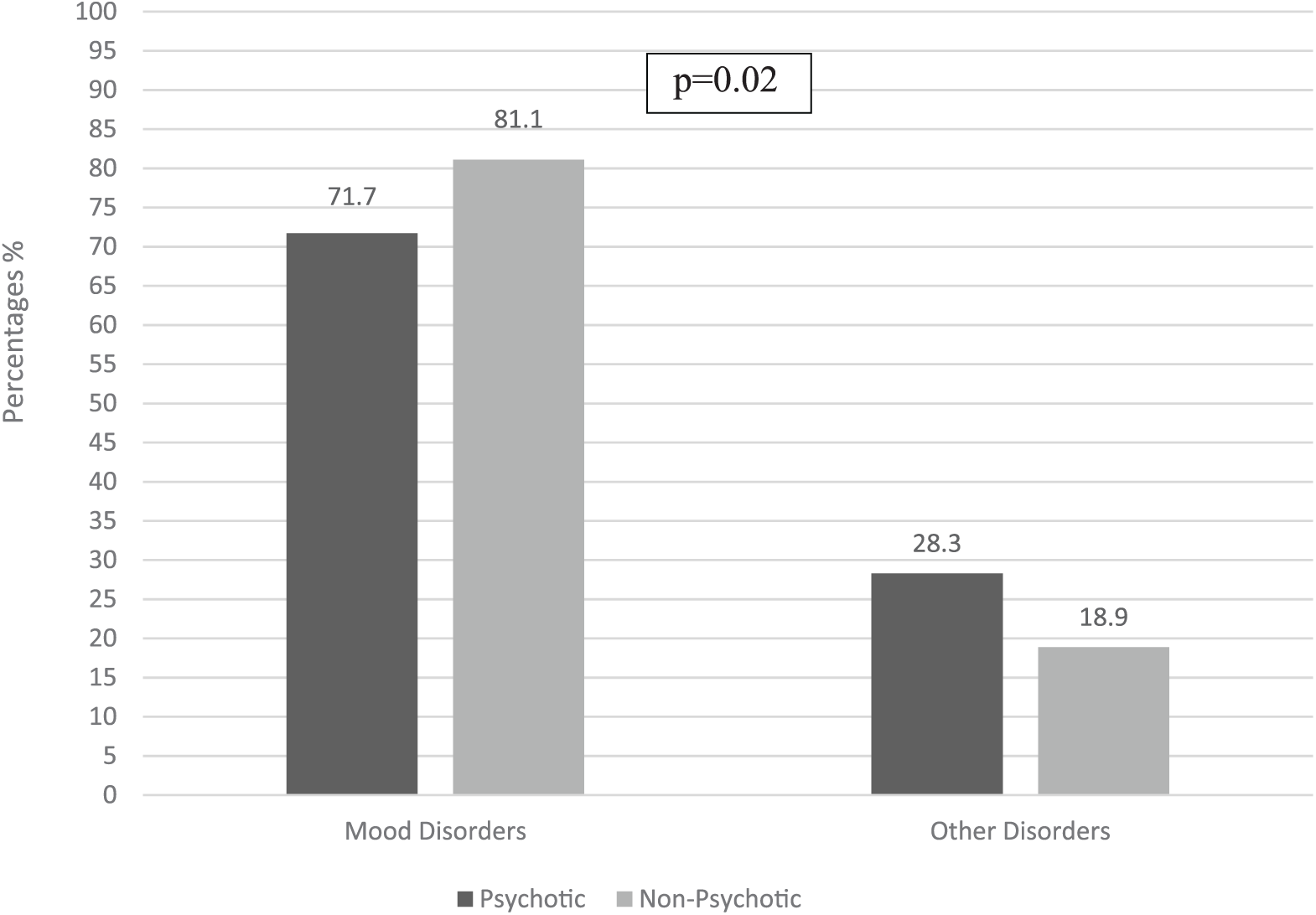
Type of first diagnosis in psychotic versus non-psychotic bipolar patients.
Summary of the statistics for the best-fit multivariable logistic regression model applied (adjusted for gender).
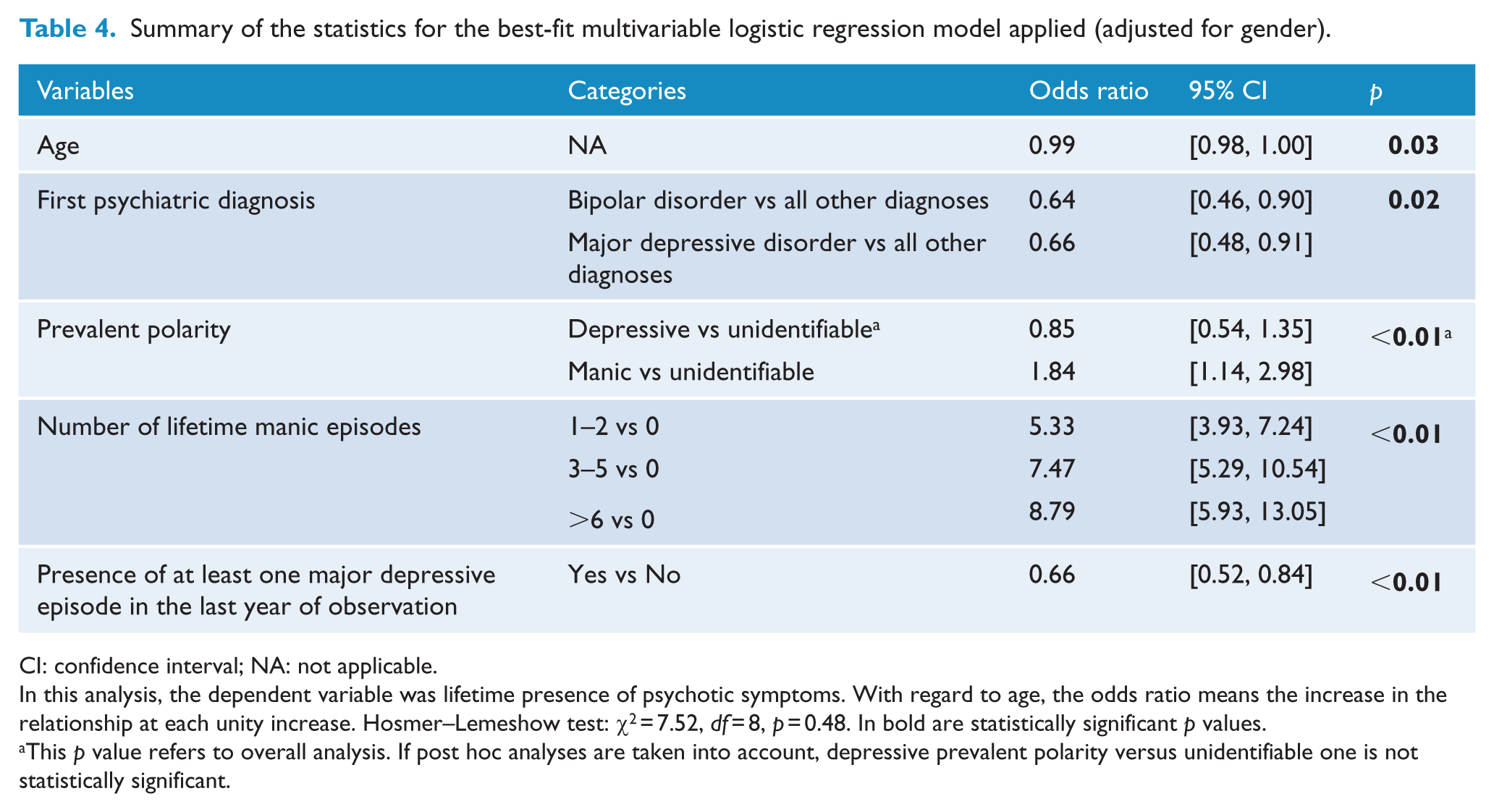
CI: confidence interval; NA: not applicable.
In this analysis, the dependent variable was lifetime presence of psychotic symptoms. With regard to age, the odds ratio means the increase in the relationship at each unity increase. Hosmer–Lemeshow test: χ2 = 7.52, df = 8, p = 0.48. In bold are statistically significant p values.
This p value refers to overall analysis. If post hoc analyses are taken into account, depressive prevalent polarity versus unidentifiable one is not statistically significant.
Discussion
The main results of this study, which according to authors’ knowledge has been conducted on one of the largest Italian multicenter samples, confirm the association of psychotic features in BD with several unfavorable socio-demographic and clinical features, including unemployment, unmarried/non-partnered status, an early age at onset with an early access to psychiatry services and pharmacological treatment, a higher probability of a first manic episode, of recent hospitalization, of manic/depressive cycle and less insight. In addition, even more robust findings (as the significance persisted in the final multivariate model) showed that psychotic versus non-psychotic bipolar patients have more frequently a first diagnosis of psychotic disorder, a more frequent manic prevalent polarity and more lifetime manic episodes.
Some of the results of this article confirm findings of previous studies. With regard to the lower chance of employment and of having a relationship in psychotic versus non-psychotic BD patients, a previous study showed patients suffering from psychotic mania (with respect to typical mania) had less probability to be partnered and more work impairment (Van Rossum et al., 2008). Also, the association between psychotic symptoms in BD and early age at onset has been previously reported by other investigations conducted in different countries (Belteczki et al., 2017; Dell’Osso et al., 2017). Early age at onset is generally considered as a clinical marker of poor outcome in BD (Carter et al., 2003), but it is not totally clarified whether this clinical feature in psychotic bipolar patients may indicate a major biological vulnerability to BD (Buoli et al., 2016a; Leboyer et al., 2005). Finally, also a higher probability of recent cannabis misuse in psychotic versus non-psychotic bipolar patients, especially after the onset of the disorder, has been previously reported (Strakowski et al., 2007).
Similarly to what has been reported in this study, previous data have been published about the higher frequency of hospitalizations in psychotic versus non-psychotic bipolar patients (Mazzarini et al., 2010; Ozyildirim et al., 2010). This result is understandable in light of more frequent manic episodes (Özyıldırım et al., 2010), more frequent manic prevalent polarity (Özyıldırım et al., 2010) and, above all, the lower insight level of psychotic bipolar subjects than non-psychotic ones (Hartung et al., 2017). This implies the absolute necessity of interventions aimed at improving the insight and treatment adherence of bipolar patients, particularly when presenting lifetime psychotic symptoms (Hartung et al., 2017).
One of the most interesting results of this study is that psychotic bipolar patients frequently receive an initial diagnosis of psychotic disorder. This has been noted in other studies reporting high rates of misdiagnosis in psychotic bipolar patients with other psychotic disorders (e.g. schizophrenia or delusional disorder) (Altamura et al., 2015a; Gonzalez-Pinto et al., 1998; Meyer and Meyer, 2009), despite, in some countries, this trend is changing with more cases of correct diagnosis of BD (Sara and Malhi, 2015). In relation to this aspect, two considerations can be formulated. The first is that the duration of untreated illness, one of the most important outcome factors in psychiatric disorders (Altamura et al., 2011), is significantly shorter in psychotic than non-psychotic bipolar patients, and this could be due to severe and urgent-to-treat nature of psychotic symptoms as well as the spread of second-generation antipsychotics that have a stabilizing effect and are able to change the course of BD (Altamura and Dragogna, 2013). In this sense, even though psychotic bipolar patients may receive a first incorrect diagnosis (e.g. schizophrenia or delusional disorder) (Altamura et al., 2015a), they might have a high chance to receive a proper treatment (e.g. with olanzapine) with respect to the past when first-generation antipsychotics were the unique option (Tohen et al., 2013). Consequently, the second consideration is that the greater clinical severity and poorer prognosis of psychotic versus non-psychotic bipolar patients could be attenuated by a correct earlier diagnosis and a better clinical management. This framework is supported by the fact that recent publications have not found important differences between psychotic and non-psychotic bipolar patients on a series of clinical features (e.g. suicidal behavior) (Gesi et al., 2016; Jiménez-López et al., 2018) associated with an unfavorable prognosis. Taken as a whole, the results of this article confirm the association between some unfavorable clinical aspects and the presence of psychotic symptoms in BD, but they also emphasize that proper management of psychotic bipolar patients consisting of an early diagnosis and tailored treatment (e.g. psychoeducation aimed to improve insight) may perhaps make the prognosis of these subjects similar to that of bipolar subjects without psychotic symptoms. Lifetime psychotic symptoms probably characterize a group of bipolar patients that need personalized interventions more than or not just a subgroup of bipolar subjects with a significantly more severe outcome (Leopold et al., 2013). Expertise and resources for early recognition and management of psychotic BD should be therefore considerably implemented (Leopold et al., 2013).
Finally, the following limitations of this research need to be mentioned:
Patients were treated with different drugs, which might have influenced some clinical features (e.g. the prescription of lithium may mask the differences in suicidal behavior between psychotic and non-psychotic bipolar patients);
The different settings of care (in several Italian regions) may have influenced the clinical and demographic features of the sample (e.g. the availability of psychoeducation to improve insight of bipolar patients);
Even though some of the patients were selected in community primary care services, others have been treated in tertiary academic care units with a potential influence of some clinical features (e.g. more severe patients are usually treated in secondary or tertiary care units);
Some data were collected retrospectively (e.g. number of mood episodes) so that they might have not been always as accurate as in controlled studies;
Referring to the point above, the number of depressive and manic/hypomanic episodes has been recorded as a categorical variable on the e-CRF (four classes, and particularly, 1–2, 3–5, 6–8 and >8), then it was not possible to consider these variables as continuous ones (it is necessary to specify that, in the light of the retrospective collection of these data, it is difficult to record very accurate information about the exact number of episodes);
The lack of a follow-up period due to the cross-sectional nature of the study.
Future research will have to establish if the presence of lifetime psychotic symptoms is a specifier of poor prognosis in BD or it identifies the need of specific interventions (e.g. long-term combined pharmacotherapy or target psychoeducation) aimed to improve the outcome of psychotic bipolar patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.