
Abstract
Objective:
To describe the correlates of stimulant use disorders (abuse, dependence) in an Australian population sample, to compare the characteristics of stimulant users with and without stimulant use disorders and to describe the patterns of service use and help-seeking in people with stimulant use disorders.
Methods:
Data were drawn from the 2007 National Survey of Mental Health and Wellbeing, which sampled 8841 residents of private dwellings in Australia in 2007. Lifetime DSM-IV substance use and mental disorder diagnoses were obtained from interviews conducted by lay interviewers, using the Composite International Diagnostic Interview (CIDI). Socio-demographic, socio-economic and clinical correlates of stimulant use disorders were identified using binary logistic regression models. Stimulant users with and without stimulant use disorders were compared to non-stimulant users via multinomial logistic regression models.
Results:
Compared to Australians without stimulant use disorder, people with stimulant use disorders were younger, more likely to be male, of non-heterosexual orientation and born in Australia, but were not more socially disadvantaged. Lifetime comorbidity rates were high: 79% of persons with stimulant use disorders had a lifetime alcohol use disorder, 73% a lifetime cannabis use disorder, and more than one third a lifetime mood or anxiety disorder. Stimulant use disorders were associated with a family history of substance use, affective disorders and psychosis. One in five people with lifetime stimulant use disorders had been imprisoned, homeless or hospitalised for substance or mental health problems, and 13% reported at least one symptom of psychosis. Nearly half had sought help for substance or mental health problems, primarily from General Practitioners (GPs), psychologists or psychiatrists.
Conclusions:
Stimulant use disorders in a representative population sample are associated with significant comorbidity and harm. Many persons with stimulant use disorders had sought care and found this helpful. There is scope for screening and intervention in this group.
Keywords
Introduction
Stimulants may cause serious physical and mental health problems (Darke et al., 2008), more often in regular or dependent users than in those who use less frequently (McKetin et al., 2006a; Degenhardt et al., 2008). In Australia the 12 month prevalence of stimulant use disorders (abuse or dependence) is estimated to be around 0.6% (McKetin et al., 2005; Sara et al., 2011), a rate comparable to the prevalence of dependent heroin use at the height of Australia’s heroin ‘epidemic’ in the late 1990s (Hall et al., 2000). Understanding the characteristics and comorbidities of individuals with stimulant use disorders may assist in planning health system responses for this group.
The first aim of this study is to describe people with stimulant use disorders in a representative Australian population sample. Most descriptions of stimulant use disorders are based on treated or convenience samples such as injecting drug users or high risk populations. These studies find that stimulant use disorders are associated with very significant comorbidity. Dependent stimulant users are often dependent on other drugs, and have high rates of depression, anxiety, psychotic symptoms, suicidal ideation and suicide attempts (Glasner-Edwards et al., 2009; Kalechstein et al., 2000; Stafford and Burns, 2010; Wallace et al., 2009; Zweben et al., 2004; McKetin et al., 2010; McKetin et al., 2006b). Individuals with stimulant use disorders are significantly disabled or marginalised, with fewer years of education and significantly increased rates of unemployment, homelessness, criminal activity and imprisonment compared with those without stimulant use disorders (Copeland and Sorensen, 2001; Degenhardt et al., 2008; Korte et al., 2011; McKetin et al., 2006a; Stafford and Burns, 2010; Zweben et al., 2004; Farrell et al., 1998). However, treatment and convenience samples are likely to include a more severely dependent or disabled group, who may differ systematically from persons with stimulant use disorders in the general population.
Population surveys of drug use can complement studies based on treatment or convenience samples. Most population surveys report only on stimulant use, and do not apply diagnostic criteria for stimulant abuse or dependence. Surveys from the US, UK, Canada, Australia and New Zealand (Adlaf et al., 2005; Durell et al., 2008; Substance Use and Mental Health Services Administration, 2007, 2010; Wilkins and Sweetsur, 2008) find that stimulant use is more common in men, peaks in the 20s, and is usually preceded by the use of other drugs, particularly cannabis. Australia’s National Drug Strategy Household Survey (NDSHS) found that stimulant use is usually infrequent; only 36% of those who had used any stimulant in the preceding year had done so monthly or more often. Few population surveys have examined regular stimulant users or those diagnosed with stimulant use disorders. The US National Epidemiological Survey of Alcohol and Related Conditions (Conway et al., 2006) found high rates of lifetime depressive disorders (51%) and anxiety disorders (39%) in individuals with amphetamine abuse or dependence.
The second aim of this study is to compare stimulant users who do not have stimulant use disorders with those who do. We have previously reported that nearly half (46%) of people who have used stimulants on more than five occasions met criteria for a lifetime stimulant use disorder (Sara et al., 2011). For an individual, the vulnerability to develop abuse or dependence is likely to reflect a mix of genetic, psychological and environmental factors (Kendler et al., 2003; Yucel et al., 2007) along with drug-related factors (McKetin et al., 2006a). To our knowledge, no study has compared the personal, family and social correlates of persons with stimulant use disorders against those of stimulant users who do not have features of abuse or dependence.
The third aim of this study is to examine help-seeking in people with stimulant use disorders. Australians with substance use disorders seek help less often than people with other mental disorders, and rates of help seeking are lowest in younger adults and males (Burgess et al., 2009), who are the group most likely to have stimulant use disorders. Understanding the extent of unmet need for treatment in this group may assist in identifying opportunities for prevention or intervention.
This study addresses these three aims by examining stimulant use disorders in the 2007 Australian National Survey of Mental Health and Wellbeing (NSMHWB) (Australian Bureau of Statistics, 2008), which provided information about a representative sample of the Australian population. It collected diagnostic information on substance use and high prevalence mental disorders diagnosed using ICD-10 and DSM-IV criteria, along with information about personal and household characteristics and family history.
Setting and participants
The 2007 NSMHWB was conducted by the Australian Bureau of Statistics (ABS) in late 2007. Respondents aged 16 to 85 years were identified from private dwellings selected by the ABS using a stratified, multi-stage area sample. One individual was selected from the pool of eligible adults in each dwelling, using a randomising algorithm implemented by a computer-assisted interview schedule, and invited to participate in an interview. Younger (16-24 years) and older people (65-85 years) were over-sampled to improve the reliability of estimates for these groups. The sampling process yielded 8,841 fully-responding households, a response rate of 60%.
Methods
Measurements
Stimulant use variables
The 2007 NSMHWB reports the use of stimulant drugs in five categories: (i) Amphetamine/Speed, (ii) Methamphetamine/Base/Ice, (iii) Ecstasy, (iv) Cocaine and (v) Any stimulant (any of i – iv). For each of these drug types respondents were asked whether they had ever used, and if so their age at first use and whether they had used more than five times in their lifetime. Persons who reported using any stimulant more than five times in their lifetime were asked whether they had done so in the last twelve months.
Diagnostic variables
The 2007 NSMHWB used a modified version of the Composite International Diagnostic Interview (CIDI) to provide lifetime and twelve month diagnoses of stimulant abuse and stimulant dependence. The derived variable ‘any stimulant use disorder’ was positive if an individual met criteria for stimulant abuse or for stimulant dependence. NSMHWB did not report diagnoses of abuse or dependence for individual stimulants (e.g. methamphetamine, ecstasy, cocaine). DSM-IV criteria were used in this study.
Data analysis
Data from the 2007 NSMHWB Basic Confidentialised Unit Record File (CURF), April 2009 version (Australian Bureau of Statistics, 2009) were analysed using PASW Statistics Version 18 (IBM Corporation, 2009) and STATA version 11 (StataCorp, 2009). Data were weighted using factors within the CURF which adjust for the differential probability of survey selection and for the age and sex distribution of the Australian population. For all analyses standard errors and 95% confidence intervals (CIs) were calculated using jackknife repeated replication to take account of the complex survey design. Because of the low prevalence of stimulant use disorders in the past 12 months, analyses were conducted on correlates of lifetime stimulant use disorders only.
Analysis was conducted in two stages. Firstly, binary logistic regression was used to compare people with and without lifetime stimulant use disorders. Secondly, people without lifetime stimulant use disorders were divided into two groups; stimulant users and non-stimulant users. Multinomial logistic regression was then used to examine whether stimulant users with a lifetime disorder differed from stimulant users without disorder, when compared with people who had never used stimulants.
For the first analysis, personal correlates and comorbidities of stimulant use disorders were examined by comparing persons with a lifetime history of DSM-IV stimulant use disorder against those with no stimulant use disorder. Odds ratios and CIs were calculated using binary logistic regression analyses conducted separately for a range of potential predictors, which included demographic variables and lifetime mental health and substance (alcohol, cannabis) disorders. Lifetime harms were not included in the multivariate analysis, as these are consequences of rather than risk factors for stimulant use disorders. Where necessary, variables with low frequency values and high standard errors were dichotomised or categories were combined.
Multiple logistic regression was then performed using those variables with significant associations (p<=0.05) and acceptable standard errors of estimate in univariate associations. Multicollinearity was tested by examination of variance inflation factors and condition number. Highly collinear variables were removed to yield a final model with a condition number less than 30 and with no condition index loading more than 0.4 for any individual variable (Belsley, 1991).
The distributions of age at first reported use of alcohol, cannabis and stimulants were both skewed and censored. Therefore we examined the proportion using each drug, and the median and interquartile range of age at first use.
In a second analysis, to examine differential risk factors for stimulant use and stimulant disorders, we separated persons without stimulant use disorders into two groups; stimulant users and stimulant non-users, as described above. This produced an outcome variable with three mutually exclusive categories; (i) non users (lifetime stimulant use on five occasions or less), (ii) users without disorder (lifetime stimulant use but no stimulant use disorder) and (iii) users with disorder (lifetime stimulant use and stimulant use disorder). Multinomial logistic regression was used to compare these groups. Multicollinearity was tested using the approach described above. Because of high relative standard errors for many of the estimates, we limited the variables entered to those identified in the earlier multiple logistic regression. Odds ratios were considered to differ significantly from each other if their 95% confidence intervals did not overlap (Schenker and Gentleman, 2001).
To examine service use, persons with stimulant use disorders were compared with persons meeting criteria for any other lifetime DSM substance use disorder or mental health disorder. Lifetime rates of hospitalisation, consultation with health professionals and self-management were described.
Persons with stimulant disorders were also compared with those with other substance use disorders. Rates of seeking help for substance problems, and the perceived effectiveness of that help were described for those groups.
Results
Associations with lifetime stimulant use disorders
On the respondents to NSMHWB 263 of the 8841 met criteria for a lifetime DSM stimulant use disorder, yielding a weighted prevalence estimate of 3.3% (CI 2.8% - 3.9%).
Table 1 describes the correlates of lifetime DSM-IV stimulant use disorders. Compared to Australians without stimulant use disorders, those with a stimulant use disorder were younger - 76% (CI 75%-76%) were under 30 - and were more likely to be male (69%, CI 62%-76%). There were no significant associations between lifetime stimulant use disorders and education, household measures of income or disadvantage, or urban/rural location. Stimulant use disorders were more common in those who reported a non-heterosexual orientation (OR 3.8, CI 1.9-7.4) and less common in persons born outside Australia (OR 0.4, CI 0.3-0.8), but both estimates had a relative standard error (RSE) between 25% and 50% and so should be interpreted with caution.
Associations with lifetime DSM-IV stimulant use disorder, compared to persons with no lifetime stimulant use disorder.
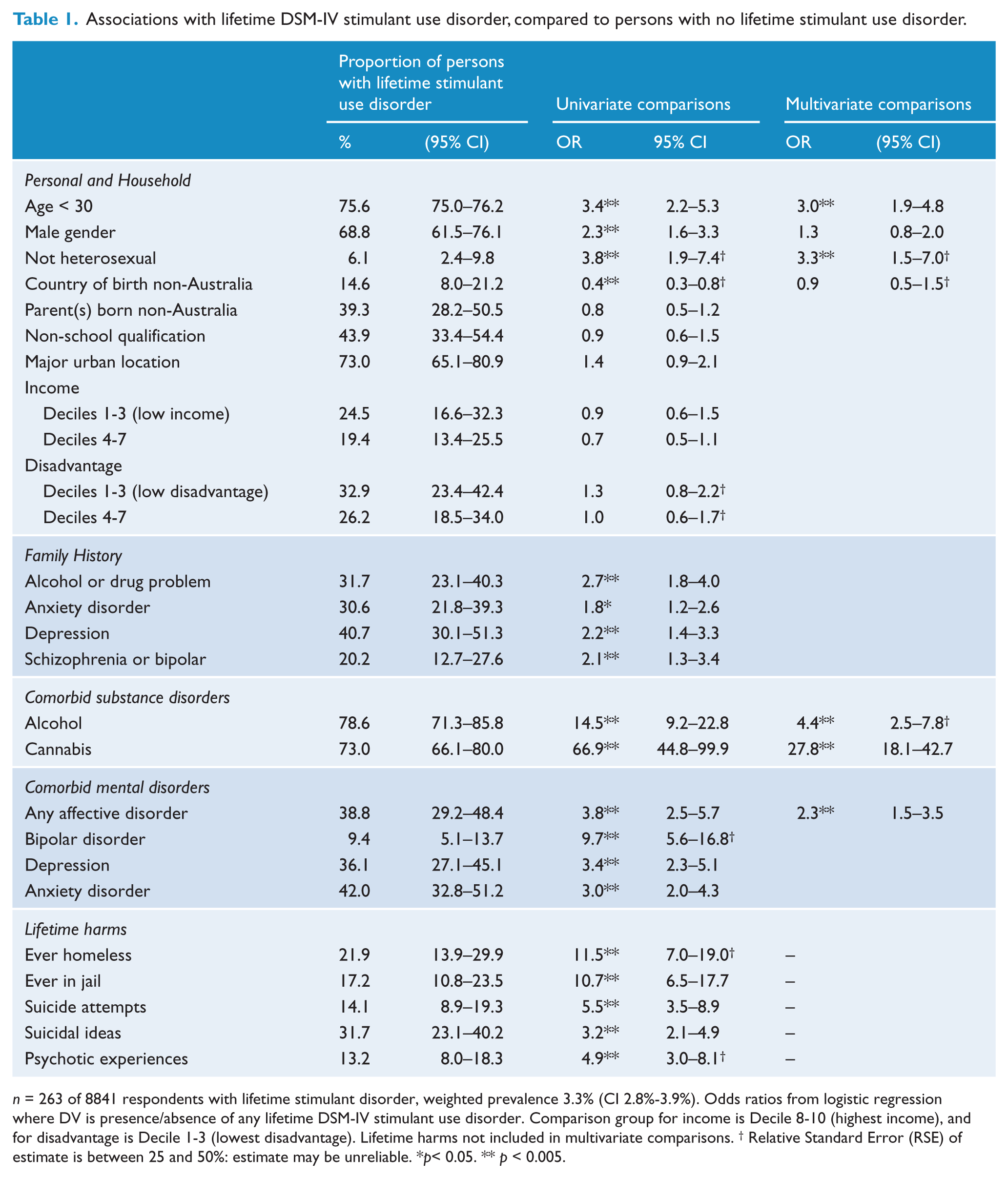
n = 263 of 8841 respondents with lifetime stimulant disorder, weighted prevalence 3.3% (CI 2.8%-3.9%). Odds ratios from logistic regression where DV is presence/absence of any lifetime DSM-IV stimulant use disorder. Comparison group for income is Decile 8-10 (highest income), and for disadvantage is Decile 1-3 (lowest disadvantage). Lifetime harms not included in multivariate comparisons. † Relative Standard Error (RSE) of estimate is between 25 and 50%: estimate may be unreliable. *p< 0.05. ** p < 0.005.
Lifetime stimulant use disorders were strongly associated with the diagnosis of another substance use disorder. Most people with lifetime stimulant use disorder also met criteria for lifetime alcohol use (79%, CI 71%-86%) or cannabis use disorders (73%, CI 66%-80%). They had more than a 60-fold higher risk of cannabis use disorders (OR 67, CI 45-100) and more than a 10-fold higher risk for alcohol use disorders (OR 15, CI 9-23) than people without lifetime stimulant disorders.
More than one third of those with a lifetime stimulant use disorder also had a lifetime history of an affective disorder (39%, CI 29%-48%) or anxiety disorder (42%, CI 33%-51%). These rates were three- to four-times higher than rates in those without a lifetime stimulant use disorder.
There were associations between lifetime stimulant use disorder and self-reported family history of substance use or psychiatric problems. There was an approximately two-fold higher risk of stimulant dependence in those with a family history of alcohol and drug problems (OR 2.7, CI 1.8-4.0), depression (OR 2.2, CI 1.4-3.3) or anxiety (OR 1.8, CI 1.2-2.6).
The final multivariate logistic regression model identified five variables that retained significant associations with lifetime stimulant use disorder after controlling for other variables. When compared to persons with no lifetime stimulant disorder, the strongest predictor of a stimulant disorder was a lifetime history of cannabis use disorder (OR 27.8, CI 18.1-42.7). There were also smaller but still significant associations with lifetime alcohol use disorder (OR 4.4, CI 2.5-7.8), being under 30 years of age (OR 3.0, CI 1.9-4.8) and a history of any affective disorder (OR 2.3, CI 1.5-3.8). The association with non-heterosexual sexual orientation also persisted after controlling for other variables (OR 3.3, CI 1.5-7.0) but the RSE of this estimate was between 25% and 50%. Family history variables were excluded from the final model because of their close covariation with individual substance, mood and anxiety disorders.
Persons with a lifetime history of stimulant use disorder reported significant psychosocial harms. One in five reported having been in prison (OR 10.7, CI 6.5-17.7) or homeless (OR 11.5, CI 7.0-19.0, RSE 25-50%). Around one third (32%, CI 23%-40%) reported suicidal ideation and nearly half of these (14%, CI 9%-19%) reported a suicide attempt.
Persons with stimulant disorders had increased rates of family history of schizophrenia or bipolar disorder (OR 2.1, CI 1.3-3.4) compared to those without stimulant disorders. Thirteen percent (13%, CI 8%-18%) reported one or more psychotic experiences on the NSMHWB psychosis screener, almost five times the rate of those without stimulant disorders (OR 4.9, CI 3.0-8.1, RSE 25%-50%).
Differentiating the correlates of stimulant use and lifetime stimulant use disorder
In the second set of analyses, multinomial logistic regression was used to compare the three outcome groups; (i) stimulant non-users, (ii) stimulant users without disorder and (iii) stimulant users with disorder. Table 2 shows the results of this regression; stimulant non-users were the comparison group and results for that group are not shown. Stimulant users without disorder comprised 322 of 8841 NSMHWB respondents (weighted prevalence 3.9%, CI 3.4%-4.5%). They did not differ from stimulant users with disorders on age, gender, sexual orientation or in the proportion with comorbid affective, anxiety or alcohol use disorders. Only comorbid lifetime cannabis disorder distinguished between stimulant users without disorder (OR 3.8, CI 2.1-6.6) and stimulant users with disorder (OR 33.2, CI 21.4-51.6).
Multinomial Logistic Regression comparing stimulant users with and without lifetime DSM-IV stimulant use disorder (abuse, dependence) to a reference group with no lifetime stimulant use.
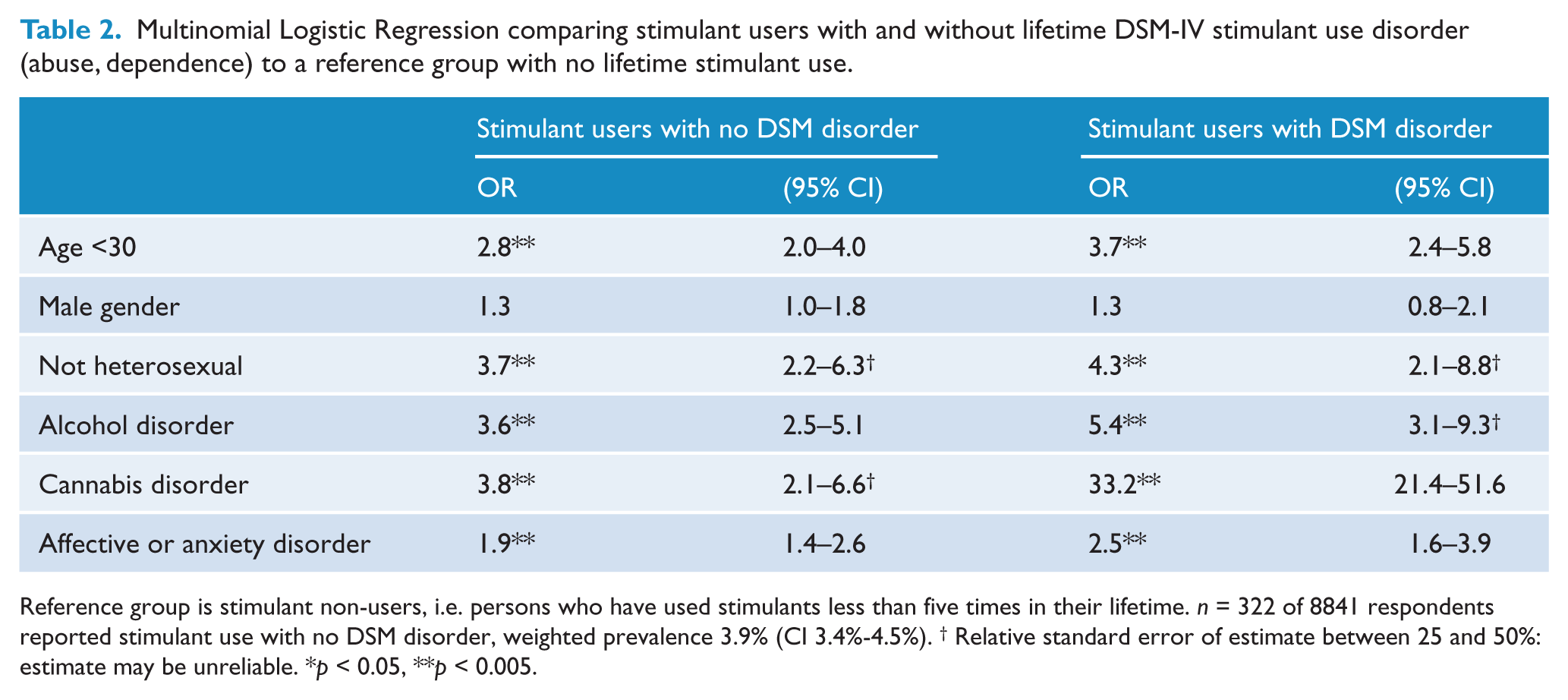
Reference group is stimulant non-users, i.e. persons who have used stimulants less than five times in their lifetime. n = 322 of 8841 respondents reported stimulant use with no DSM disorder, weighted prevalence 3.9% (CI 3.4%-4.5%). † Relative standard error of estimate between 25 and 50%: estimate may be unreliable. *p < 0.05, **p < 0.005.
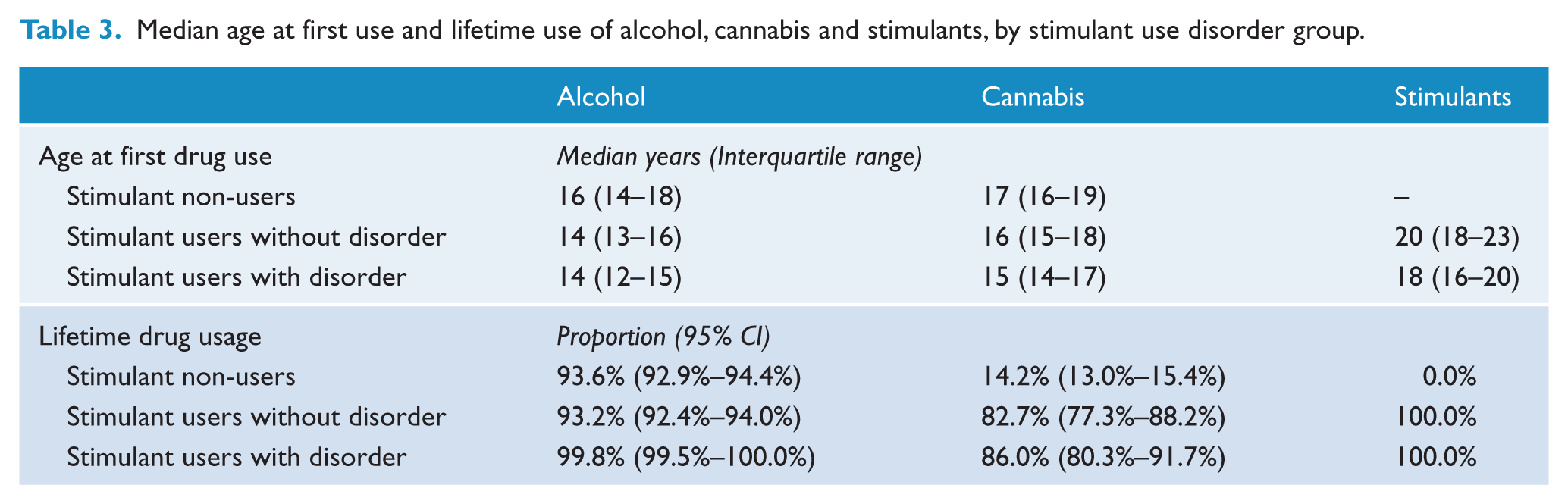
Table 3 summarises age at first use of alcohol, cannabis and stimulants. Rates of lifetime cannabis use were much higher for stimulant users, whether with disorder (86%, CI 80%-92%) or without disorder (83%, CI 77%-88%), when compared to stimulant non-users (14%, CI 13%-15%). For all groups the median age at first drug use was youngest for alcohol, intermediate for cannabis and oldest for stimulants. Stimulant users (with or without disorder) had a lower median age of first use of alcohol and cannabis than stimulant non-users. Stimulant users with disorder had a lower median age of first use of cannabis and stimulants than stimulant users without disorder.
Median age at first use and lifetime use of alcohol, cannabis and stimulants, by stimulant use disorder group.
Service use
Table 4 shows rates of help-seeking and service use. It includes help sought by stimulant users for any problem (i.e. stimulant use or any other mental health or drug and alcohol problem). The comparison group is persons with any DSM mental health or substance disorder other than stimulant use disorder. Nearly one in five persons (19%, CI 11%-27%) with a lifetime stimulant use disorder reported having been hospitalised for a mental health or substance use condition, approximately twice the rate of persons with other lifetime disorders (10%, CI 8%-11%).
Lifetime treatment rates of stimulant users with lifetime DSM-IV stimulant use disorders compared to persons with other lifetime DSM mental health disorders.
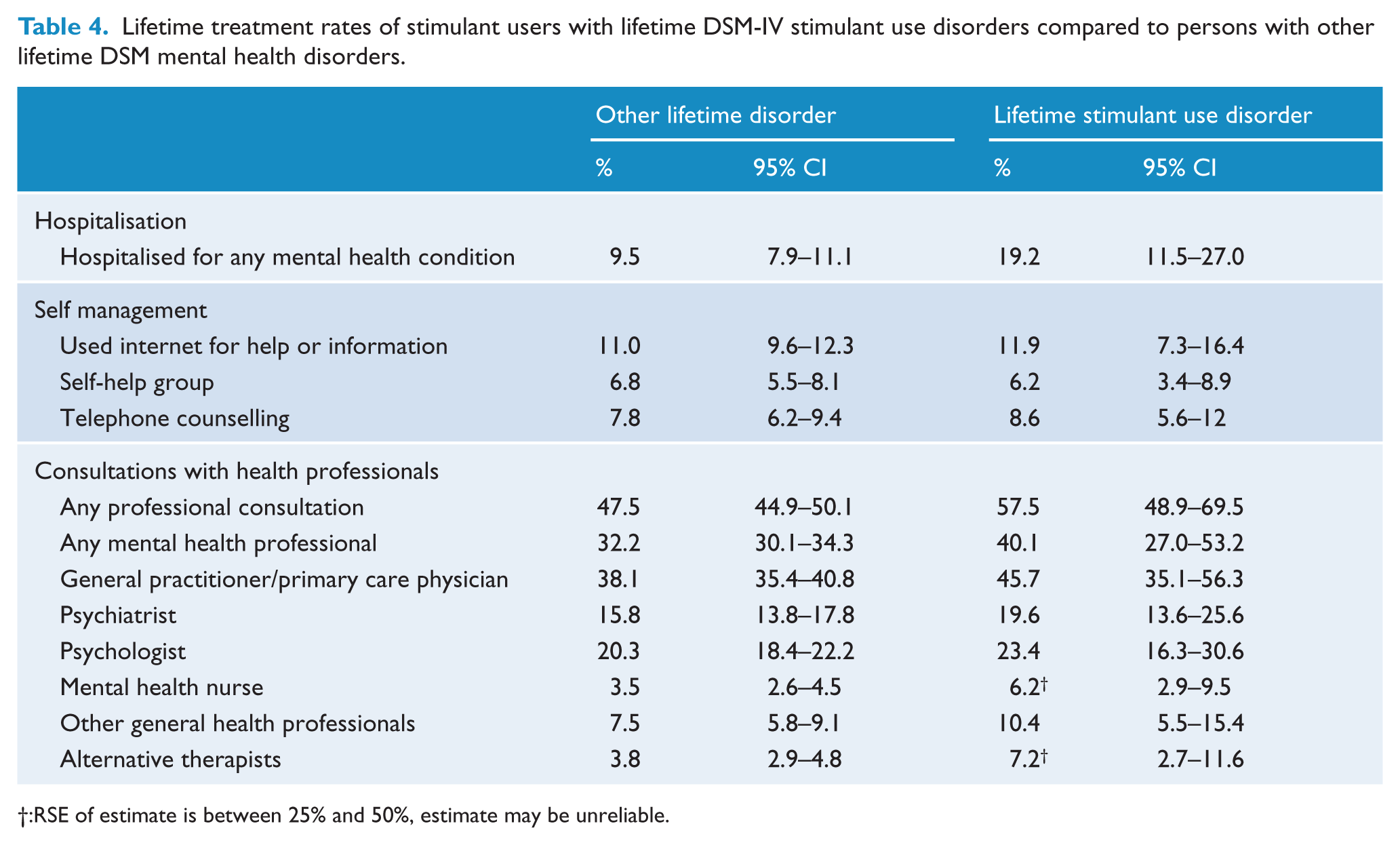
:RSE of estimate is between 25% and 50%, estimate may be unreliable.
More than half of those with a lifetime stimulant use disorder (57%, CI 47%-68%) reported a professional consultation for a mental health or substance use problem. The most common contacts were with General Practitioners (GPs) (46%, CI 35%-56%), followed by psychologists (23%, CI 16%-31%) and psychiatrists (20%, CI 14%-26%). The type of professionals did not differ substantially between those with lifetime stimulant use disorders and those with other disorders. Those with lifetime stimulant use disorders reported similar rates of use of internet information or self-help sites (12%, CI 7%-16%) and telephone counselling services (9%, CI 6%-12%) as persons with other disorders.
Stimulant users with disorder had sought help for drug and alcohol problems more often than persons with other specific drug and alcohol use disorders: nearly half (47%, CI 37%-58%) of stimulant users with disorder had talked to a medical practitioner or other health professional about drug and alcohol problems, compared to 16% (CI 14%-19%) of people with other alcohol or drug use disorders. Fifty eight percent (58%, CI 40%-76%) of stimulant users with disorder who had sought help considered that treatment had been effective, compared with 36% (CI 26%-44%) of those with other drug and alcohol problems. Only 6% (CI 3%-9 %) of those with lifetime stimulant use disorders had participated in self-help groups for alcohol and drug problems.
Discussion
This study is the first to report the correlates of diagnosed stimulant use disorders from a large, representative Australian population sample. We found high rates of comorbidity and harm in this group. Around three quarters of those with stimulant use disorders also had lifetime alcohol or cannabis use disorders. Depressive and anxiety disorders were common, and the risk of any affective disorder was more than twice that of the general population after controlling for age, gender and other disorders. The risk of suicide attempts, homelessness and imprisonment were between five and ten times greater than for the general population. These findings are consistent with those reported in treatment and convenience samples, and suggest that the high rates of comorbidity and harm found in treated samples are not solely due to selection issues. This study does not demonstrate any causal link: stimulant use disorders may be a cause of other problems (such as mood disturbance and legal problems), an effect of such problems, or part of a broader set of personal and social vulnerabilities.
As expected, lifetime stimulant use disorders were more common in younger adults and in men. They were less common in people born outside Australia but this was not significant after controlling for other variables. Contrary to a number of clinical and cohort studies (Akiyama, 2006; Degenhardt et al., 2007a, 2007b, 2008; Durell et al., 2008; Russell et al., 2008), we did not find a significant social gradient in the prevalence of stimulant use disorders. This may reflect limitations in NSMHWB which are discussed below. However, we note also that a recent analysis of the Australian National Drug Strategy Household Drug Survey (Roche et al., 2008) found that amphetamine use was almost twice as common in those in the paid workforce as those not in work. Therefore those at risk of harm from dependent stimulant use may also include a broader group, and prevention or treatment strategies may need to consider a more diverse range than high risk studies suggest.
There have been reports of increased rates of stimulant use in homosexual men in the US and UK (Bonell et al., 2010; Maxwell and Rutkowski, 2008). We found that stimulant disorders were more common in people reporting non-heterosexual sexual preference. This effect persisted after controlling for other variables but was based on small numbers of individuals and so should be interpreted with caution. In this sample, people reporting non-heterosexual orientation were more likely to use stimulants, but had the same risk as other stimulant users of developing abuse or dependence.
The second aim of this study was to compare stimulant users who do not have stimulant use disorders with those who do have such disorders. We found few differences between stimulant users with and without stimulant use disorders. Only comorbid cannabis use and younger age of first use of cannabis and stimulants distinguished the two groups. This finding is consistent with recent evidence for the role of early cannabis use as a gateway to later use of other illicit drugs (Degenhardt et al., 2009, 2010). It suggests that strategies for the prevention of stimulant use disorders need to be broad based.
In this population sample, individuals with stimulant use disorders were twice as likely to report a family history of bipolar disorder or schizophrenia than those without stimulant use disorders. The precipitation or worsening of psychosis is one of the most serious harms associated with stimulant use disorders (Curran et al., 2004; Darke et al., 2008). Many risk factors interact in the development of psychosis (McGrath et al., 2004) and the role of stimulants should not be overstated. However, for some individuals interactions between genetic liability and substance abuse, including stimulants, may increase the risk of psychosis (McGorry et al., 2008). Our findings suggest that those with stimulant use disorders may be vulnerable not only due to exposure to substances but also due to a higher rate of family history of psychosis.
This study’s third aim was to describe help-seeking and service use in people with stimulant disorders. Around half of those with a lifetime stimulant use disorder had sought help for a substance or mental health problem (although not necessarily for stimulant use). Most had done so by consulting a GP, a psychologist or psychiatrist. This suggests the importance of GPs and mental health professionals screening for comorbid stimulant use disorders. Intervention and information strategies often target internet and social media but only 12% of those with stimulant use disorder reported using those media for help or information. In this study people with stimulant disorders who sought care were more likely to report that this had been helpful than persons with other substance problems, underlining the opportunity for effective intervention in this group. The rate of help-seeking in those with lifetime stimulant disorders was higher than that reported from NSMHWB for people with any 12 month substance use disorder (24%) (Burgess et al., 2009). These higher rates partly reflect differences between lifetime and 12-month measurement periods, but may also reflect the high rate of comorbid conditions in people with stimulant use disorders. Help-seeking is more common where substance use disorders are comorbid with other mental disorders (Burgess et al., 2009).
This study has a number of limitations. Firstly, the NSMHWB 2007 had a response rate of 60%. Respondents to population surveys are more likely to be older, female, better educated, healthier and less socially disadvantaged than non-respondents (Knudsen et al., 2010; Galea and Tracy, 2007). Rates of illicit drug use may be particularly understated by population health surveys which may not recruit from unconventional households, marginalised groups or drug ‘hotspots’ (Degenhardt et al., 2011). The NSMHWB weights data for the age and gender distribution of the Australian population, but cannot correct for other sources of bias. These factors may contribute to the lack of association between stimulant use and measures of social disadvantage in this study.
Secondly, the NSMHWB was designed for the study of high prevalence conditions. Stimulant use disorders, being infrequent, are at the lower limit of the survey’s resolution. Therefore we have focused on lifetime rather than 12 month disorder. This limits the conclusions which can be drawn. Persons with comorbid lifetime conditions cannot be assumed to have had these disorders at the same time, or in any particular sequence. There was also insufficient power to allow examination of some potentially important issues, such as comparison of those with stimulant dependence and stimulant abuse separately. Furthermore, the NSMHWB did not report diagnoses of abuse or dependence for individual stimulant drugs. We therefore could not examine individual stimulant drugs, when there is evidence that personal correlates, harms and risks of dependence do differ amongst different types of stimulants (Conway et al., 2006; Grant, 1995; McKetin et al., 2006a).
Conclusions
Australians who met criteria for lifetime DSM-IV stimulant use disorders in the NSMHWB had high rates of comorbid substance use, mood and anxiety disorders, suicide attempts, homelessness and imprisonment. These findings from a representative population sample underline findings from treatment and convenience samples that stimulant use disorders are associated with significant comorbidity and harm.
Only comorbid cannabis disorders and earlier drug use distinguished stimulant users without disorder from those with abuse or dependence. Many people with stimulant use disorders had sought help, especially from GPs and mental health professionals, and many had found treatment helpful. Therefore health professionals need to be made aware of the scope for intervention. Prevention of stimulant use disorders may require a broad focus on younger people at risk, including those with cannabis use disorders. Treatment for stimulant use disorders may also need to address comorbid substance use disorders, mood and anxiety disorders as well as broader vulnerabilities.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.