
Abstract
Objective:
Amphetamine use and availability have increased in Australia and there are concerns that this has led to more frequent hospital admissions with amphetamine-related psychosis. This study examines whether amphetamine-related admissions to mental health units are more common at times of greater amphetamine availability.
Methods:
We conducted an ecological study using aggregate crime and health service data for NSW, Australia, from January 2000 to March 2015. Amphetamine-related criminal incidents (arrests or cautions for possession or use) were used as an indirect measure of amphetamine availability. Semiparametric time series analysis was used to compare monthly arrest rates to monthly hospitalisation rates for (1) amphetamine abuse or dependence, (2) amphetamine-related psychosis and (3) any psychosis.
Results:
Amphetamine-related admissions to NSW mental health units have increased four- to fivefold since 2009 and comprised approximately 10% of all admissions to these units in early 2015. There was a significant association between arrests and amphetamine-related admissions. After adjustment for seasonal variation, this effect demonstrated a time lag of 1–2 months. There was no relationship between amphetamine arrests and overall admissions for psychosis.
Conclusion:
Greater amphetamine availability significantly predicts admissions for amphetamine use disorders and amphetamine-related psychosis. Better treatment strategies are needed to break the nexus between drug availability and drug-related harm.
Introduction
Methamphetamine availability and use has increased substantially in Australia over the last 5 years (Degenhardt et al., 2017). Psychotic disorders are among the most serious harms associated with amphetamine misuse (Darke et al., 2008; McKetin et al., 2013) and have significant impacts for individuals, families and the health system. Around half of injecting amphetamine users meet the criteria for a current or lifetime psychotic disorder (Hides et al., 2015). More than 16% of Australians with a first hospitalisation for psychosis have comorbid amphetamine misuse, 10 times the rate of the age-matched Australian population (Sara et al., 2013). Amphetamine misuse is associated with more frequent hospital admissions and greater social disruption in people with enduring psychotic disorders such as schizophrenia (Sara et al., 2014). Therefore, it is important to understand the extent to which changes in amphetamine availability and use contribute to an increased burden of psychosis in Australian populations and health services.
This study examines whether hospital admissions with amphetamine-related psychoses are more common at times of greater amphetamine availability. We use arrests for amphetamine possession or use as a measure of amphetamine availability in the community. Drug-related arrests have been shown to be an indirect but valid measure of drug availability and to correlate with other measures including changes in purity and drug-related harms (Rosenfeld and Decker, 1999; Snowball et al., 2008). We have previously reported that fluctuations in amphetamine availability explained 50% of the variation in admissions to NSW public hospital mental health units with amphetamine-related psychosis between 2000 and 2009 (Sara et al., 2011). The increased amphetamine availability and use in Australia since 2010 (Degenhardt et al., 2017) and the change towards greater use of more potent forms such as crystal methamphetamine (Australian Institute of Health and Welfare, 2017) suggest that this evidence should be updated. This study examines NSW police and hospital data from 2000 to 2015 and applies a time series analysis approach to examining the relationship between availability (arrests) and harm (hospital admissions).
Methods
Aggregated data were obtained from routinely collected crime and health datasets and used with permission of the relevant data custodians. Amphetamine use and possession data (‘Amphetamine Arrests’) were provided by NSW Bureau of Crime Statistics. This comprised the total number of ‘criminal incidents’ of amphetamine possession and/or use detected by or reported to NSW Police. In addition to arrests, ‘criminal incidents’ include some cautions and persons diverted from court through the use of infringement notices or youth justice conferences.
Mental Health admissions data were extracted from the NSW Health Information Exchange (HIE). Same day or overnight inpatient episodes of people aged 14–65 years in designated adult acute mental health units were included. To ensure that the timing of admission reflected the timing of possible community exposure to amphetamines, the following were excluded: (1) acute adult units with a tertiary referral role (e.g. forensic units, neuropsychiatry units, day programmes, ECT suites); (2) admissions following transfer from another hospital, a nursing home or due to statistical type-change within a facility; and (3) episodes where greater than 1 week elapsed between admission to hospital and transfer to an acute mental health unit. Psychosis was defined by a primary diagnosis with an International Classification of Diseases, 10th Revision (ICD-10) diagnosis code of psychotic disorder (F20-29), specific drug-induced psychoses (F1x.5, F1x.7) or affective psychoses where psychotic symptoms were specified (F30.2, F31.2, F31.5, F32.3, F33.3). Amphetamine use disorders were identified by primary or additional diagnosis codes for amphetamine abuse, dependence, intoxication or withdrawal. Amphetamine-induced psychosis diagnoses were recorded as both psychoses and amphetamine disorders. All diagnoses were routine clinical diagnoses as made and recorded by the team responsible for the clinical care of that hospital episode.
Statistical analysis
Monthly police and health data were compared using semi-parametric time series analysis. Three outcome variables were examined separately: (1) hospital admissions with amphetamine abuse or dependence (‘Amphetamine Abuse’), (2) hospital admissions with amphetamine-related psychosis (‘Amphetamine Psychosis’) and (3) all hospital admissions with psychosis (‘All Psychosis’). Generalised additive models (GAM; Wood, 2006) were used, comparing each outcome variable (Abuse or Psychosis) to the independent variable of amphetamine possession and use, after adjusting for seasonal variation and unmeasured factors via a smooth function s(t). The GAM model takes the form
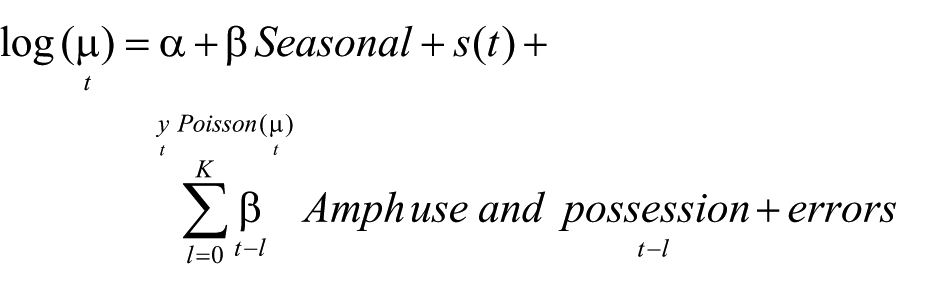
where α is the model’s intercept, β = (January, …, November) measures the monthly seasonal effects and
The errors were assumed to follow an autoregressive model of order 1. The cumulative percentage increase in either Abuse or Psychosis associated with a unit increase in amphetamine use and possession on a given month was calculated, including lag effects by examining cumulative or total effect

To account for possible unmeasured confounders affecting the response variable, the model includes a smooth varying temporal function s(t), which was estimated based on generalised cross-validation (Peng et al., 2005, 2006). Finally, the errors in the models include an autoregressive process of order one (AR1) to account for the autocorrelation due to the time series nature of the measurements.
Results
Monthly data were available for 61 months from January 2000 to March 2015 inclusive. On average, there were 2482 eligible admissions to mental health units per month, of which 887 (36%) had a diagnosis of psychosis and 128 (5%) had any amphetamine-related diagnosis. There were an average of 39 admissions per month with Amphetamine Psychosis (1.6% of all admissions, 4.4% of All Psychosis). There was a steady increase in arrests and admission indicators from 2009 to 2015 (Figure 1). In 2009, there were 844 amphetamine-related admissions (2.7% of total), including 198 Amphetamine Psychosis admissions (1.8% of all psychosis admissions). By contrast, in the first quarter of 2015, amphetamine-related admissions comprised 9.9% of all mental health admissions, and Amphetamine Psychosis admissions comprised 10.0% of All Psychosis admissions. In the same period, there were on average 250 Amphetamine Arrests per month, increasing from 153 per month in 2009 to 607 per month in the first quarter of 2015.
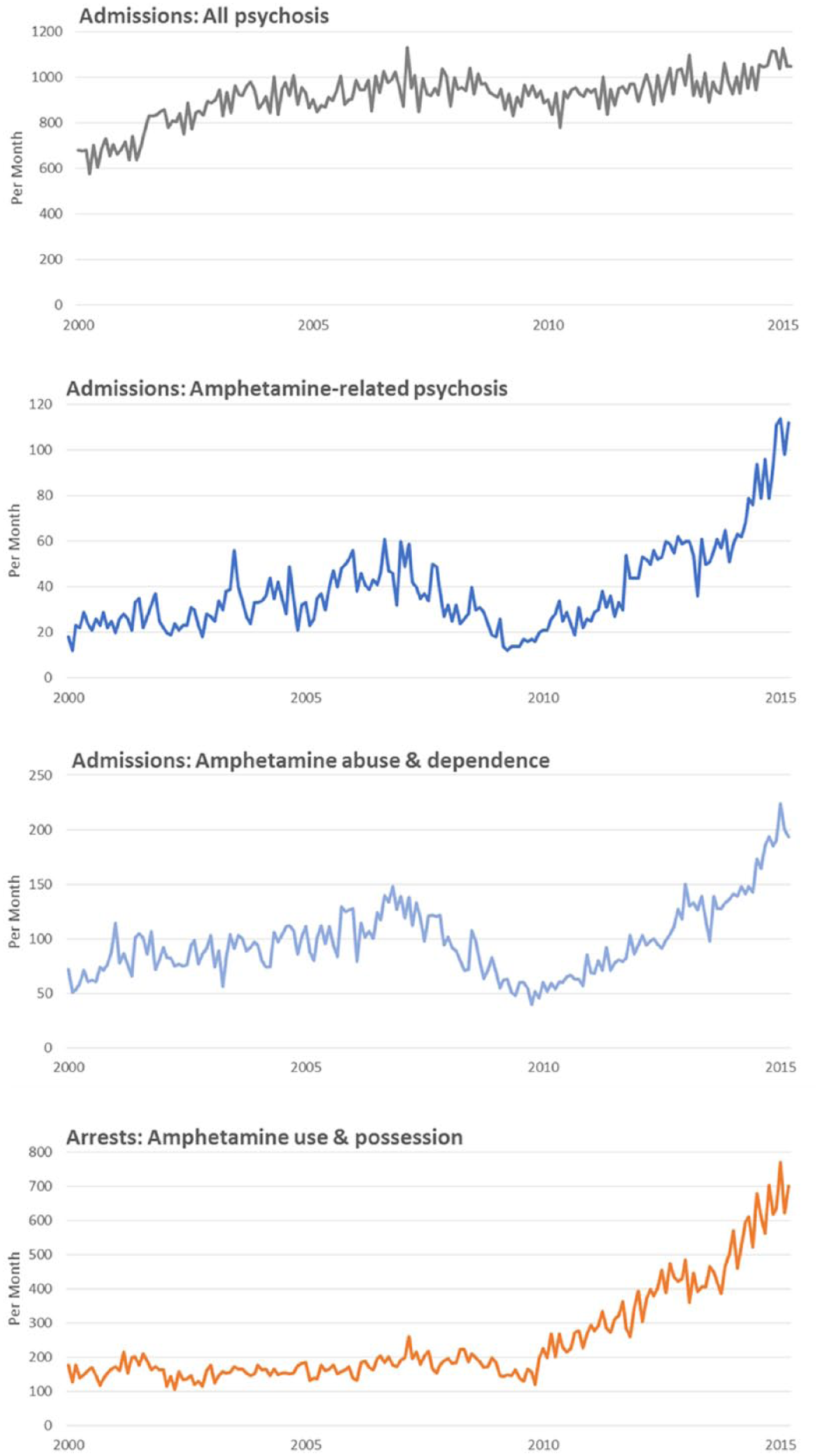
Monthly measures of amphetamine availability (Arrests for amphetamine use and possession) and amphetamine-related admissions to mental NSW mental health units, January 2000–March 2015.
Table 1 summarises the time series analysis. There was a seasonal trend in admissions for Amphetamine Abuse, which were more common in summer months (December, January). The same trend was not seen for Amphetamine Psychosis. After controlling for seasonal trends, there was a significant positive relationship between Amphetamine Arrests and hospital admissions for Amphetamine Abuse and Amphetamine Psychosis. This association demonstrated a time lag, with Amphetamine Abuse and Amphetamine Psychosis admissions being significantly increased at 1 and 2 months following an increase in Amphetamine Arrests.
Generalised additive model examining the association between amphetamine availability (Amphetamine Arrests) and admission to a NSW mental health unit with amphetamine-related harms or psychosis, 2000–2015.
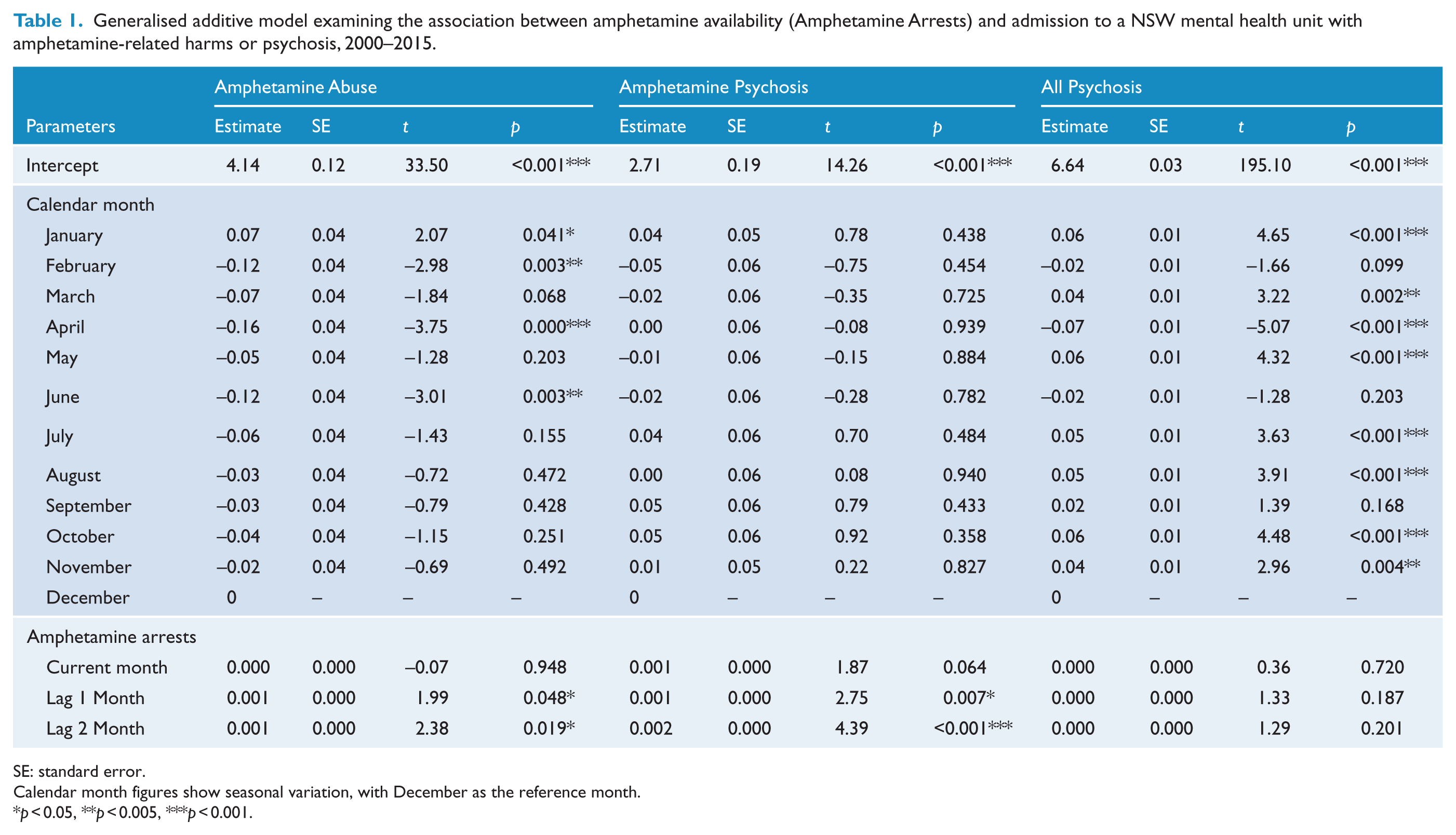
SE: standard error.
Calendar month figures show seasonal variation, with December as the reference month.
p < 0.05, **p < 0.005, ***p < 0.001.
Based on the estimated cumulative effects, each 10 unit (approximately 4%) increase in Amphetamine Arrests was associated with a 3% increase in admissions to mental health units with Amphetamine Abuse and a 4% increase in admissions for Amphetamine Psychosis. There was no significant relationship between Amphetamine Arrests and All Psychosis admissions.
Conclusion
We found a strong relationship between an indirect measure of amphetamine availability (criminal incidents of amphetamine possession and use) and rates of amphetamine-related admission to mental health units. In NSW, from 2000 to 2015, measures of amphetamine availability and amphetamine-related hospitalisation both increased four- to fivefold, rising steadily from a low in 2009 to the end of the observation period in 2015. These were large relative increases; however, amphetamine-related admissions to mental health units comprised a small minority of total mental health admissions. During the study period, less than 5% of admissions to mental health units included an amphetamine-related diagnosis.
The timing and scale of our findings are consistent with other Australian evidence. Since 2009 there have been steady increases in measures of amphetamine availability, including border seizures, clandestine laboratory detections and amphetamine seizure purity (Australian Crime Commission, 2017; Degenhardt et al., 2017). These have been mirrored by increases in amphetamine-related drug helpline calls, drug and alcohol treatment episodes and amphetamine-related hospitalisations (Degenhardt et al., 2017). Additional evidence is provided by waste-water analysis, which has emerged as a sensitive mechanism for monitoring spatial and temporal trends in illicit drug use (Australian Criminal Intelligence Commission, 2017). These studies estimate that amphetamine use increased 3.4- to 4.8-fold in South East Queensland from 2009 to 2015 (Lai et al., 2016) and more than doubled in South Australia from 2011 to 2015 (Tscharke et al., 2016).
The National Drug Strategy Household Survey (NDSHDS) provides three-yearly measures of drug use in the Australian population. Self-reported amphetamine use has declined steadily since 2001, being overtaken by the use of cocaine and 3,4-methylenedioxy-methamphetamine (MDMA or ‘ecstasy’) (Australian Institute of Health and Welfare, 2017). However, among amphetamine users, there is a continued trend towards greater frequency of daily or weekly use, greater frequency of injecting use and the use of crystal methamphetamine in place of powder or base forms (Australian Institute of Health and Welfare, 2017). These patterns of use are all associated with greater harms and specifically with an increased risk of psychosis (Hides et al., 2015; Lappin et al., 2016; McKetin et al., 2013).
There was a small but significant time lag in our findings: increased amphetamine availability preceded increased amphetamine-related admissions by 1–2 months. This time lag is consistent with the typical time course of amphetamine-related psychoses. Brief or transient psychotic symptoms may occur within hours of amphetamine use (Curran et al., 2004), but symptoms sufficient to require hospital admission often occur in the context of prolonged or dependent use (Lappin et al., 2016; McKetin et al., 2013). This consistent time lag also makes some other possible explanations for our findings less likely, such as greater awareness and data capture by both police and health staff, or greater diversion of people from police to hospital at the time of amphetamine-related arrests.
This study has a number of limitations. First, we have used the number of amphetamine-related arrests as our primary independent variable and treated this as an indirect measure of amphetamine availability. There is evidence supporting the validity of drug-related arrests as a measure of drug availability (Rosenfeld and Decker, 1999; Snowball et al., 2008; Warner and Coomer, 2016). However, variations in arrests may also be influenced by changes in the prioritisation of policing activities or changes in awareness and data collection regarding amphetamines. The use of arrest figures in this way has been debated because of evidence that police activity may be more focused on disadvantaged or marginalised groups (Warner and Coomer, 2016). While acknowledging the limitations of the measure used, it is important to note that there is no perfect measure of the community availability of illicit drugs. Household surveys are open to response bias, are insensitive to hotspots and marginalised groups, and have insufficient temporal resolution for this type of analysis. Drug purity data is also influenced by changes in police activity or practice. Drug price data is primarily obtained from sentinel drug user surveys, and unit drug prices often remain relatively stable despite changes in drug availability (Caulkins, 2007). The consistency of the NSW arrests data with other Australian data on drug seizures, purity and harms provides some convergent validation of the measure used.
Second, we used routinely recorded clinical diagnoses of amphetamine abuse, dependence or psychosis as our primary dependent variables. Diagnoses recorded in routine clinical care are likely to underestimate the true prevalence of substance use disorders and may be influenced by changing awareness among clinicians or clinical coders. It is possible that the increase in Amphetamine Psychosis admissions without a corresponding increase in All Psychosis admissions is consistent with changes in awareness and diagnostic practice rather than a true increase in amphetamine-related psychoses. However, the high occupancy and fixed bed numbers of typical acute mental health units mean that genuine increases in demand may be reflected in a change in diagnostic mix rather than an increase in the total number of admissions.
Third, the study used an ecological design, comparing aggregate state-wide data on arrests and admissions. We cannot demonstrate a link between availability and harms in individuals or specific geographical regions. We cannot identify whether increased arrests or admissions reflect a greater number of individuals or merely a greater number of events per individual. The changing pattern of amphetamine use in Australia (Australian Institute of Health and Welfare, 2017) suggests that the increased harms may be occurring in the smaller group of individuals with more frequent or dependent amphetamine use.
While acknowledging these limitations, the apparent link between greater amphetamine availability and more frequent admissions has implications for clinical care and for policy. It has been argued that amphetamines have been a major factor in increasing demand and acuity in mental health inpatient services (Australian Senate Select Committee on Mental Health, 2006). We found a substantial relative increase, but a modest absolute increase in amphetamine-related admissions. Admissions with amphetamine-related psychoses accounted for 5–10% of all psychosis admissions, and changes in amphetamine availability were not associated with an increase in overall admissions for psychosis. However, when bed occupancy is high, even modest increases in demand may have a major impact on service capacity.
Rates of substance use are influenced by personal, cultural and economic factors, including market signals such as availability and price (Johnson and Golub, 2007). Do our findings therefore provide an argument for a greater focus on strategies to reduce amphetamine availability, in order to reduce psychosis and other harms? We would argue that they do not. Amphetamine availability in Australia has continued to increase despite significant investments in precursor controls, border interceptions and policing (Australian Crime Commission, 2017). Large amphetamine seizures have not been associated with any reduction in amphetamine-related harms (Wan et al., 2016). If arrests for amphetamine possession led to reductions in amphetamine use, our study should have found an inverse correlation between arrests and admissions rather than the positive correlation observed.
Instead, our findings underline the challenge of limiting or reducing drug-related harms at a time of greater drug availability. Possible interventions may include early education and harm reduction strategies which facilitate engagement and treatment of at-risk individuals as early as possible in their substance use histories. Cognitive behavioural therapy (CBT) and contingency management have been shown to be effective psychological treatments for amphetamine dependence (Lee and Rawson, 2008). Long-term residential rehabilitation can reduce amphetamine use and harm (McKetin et al., 2012). There are no proven pharmacotherapies for people with established amphetamine dependence (Darke and Farrell, 2016); however, supply control with prescription amphetamines has been proposed as a less harmful alternative with potential to regulate purity and reduce policing costs (Dobry and Sher, 2012).
In conclusion, this study has demonstrated a strong correlation between fluctuations in amphetamine availability (as measured by arrests) and amphetamine-related admissions to mental health units. Hospital admission for amphetamine-related psychosis has increased four- to fivefold during a period of apparently increasing amphetamine availability. Globally, amphetamine use continues to rise. Strategies are needed to break the nexus between amphetamine availability and amphetamine-related harms, including psychosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.