
Abstract
Context:
Attention deficit hyperactivity disorder and stimulant use disorder commonly co-exist, and appropriate treatments have not been well established.
Objective:
To provide guidance for treatment of co-existing attention deficit hyperactivity disorder and stimulant use disorder.
Data sources:
A systematic review of published English articles using MEDLINE, EMBASE, CINAHL, PsycINFO and Cochrane, utilising consistent search terms.
Study selection:
Randomised controlled trials, comparing any treatment arm with a control group, for participants meeting Diagnostic and Statistical Manual of Mental Disorders or equivalent criteria for both attention deficit hyperactivity disorder and stimulant use disorder.
Results:
Eight trials were identified for inclusion in this review. Four of eight studies showed improvement in attention deficit hyperactivity disorder outcome measures compared with placebo. Two of six studies that reported substance use outcomes showed improvement in treatment arms compared with placebo. Studies to show effect tended to be those with the highest treatment dosage.
Conclusion:
Evidence for the efficacy of treatment of patients with comorbid stimulant use disorder and attention deficit hyperactivity disorder is limited. Promising outcomes need replication in further studies utilising higher treatment dosage.
Case example
Adam is a 19-year-old young man with a diagnosis of attention deficit hyperactivity disorder (ADHD) since age 7, treated with methylphenidate from age 7 to age 13. He commenced polysubstance use at age 14 and left school in year 10. He transitioned to daily methamphetamine use and trafficking at age 17, with limited ongoing cannabis and illicit benzodiazepine use. He has accrued significant forensic system contact. He reports frequent impulsive behaviour, constant fidgeting and difficulty sitting still, and difficulty maintaining concentration at school. He finds that methamphetamine has a calming and stabilising effect on his mental state and requests support in recommencing ADHD treatment.
Introduction
Attention deficit hyperactivity disorder (ADHD) is common in populations of adults with substance use disorder. A meta-analysis indicated 23.1% of subjects with substance use disorder met Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for comorbid ADHD (Van Emmerik-van Oortmerssen et al., 2012). A childhood diagnosis of ADHD (particularly with hyperactive-impulsive symptoms) is recognised as a risk factor for development of substance use disorder and is related to more severe outcomes (Ameringer and Leventhal, 2013; Arias et al., 2008; Groenman et al., 2013; Kaye et al., 2016; Wilens, 2004). There is evidence that treatment of childhood ADHD with stimulants may reduce the risk of development of later substance use disorder, although results are mixed (Humphreys et al., 2013; Wilens et al., 2003).
The comorbidity of ADHD and substance use disorder likely relates to a constellation of factors, including common genetic vulnerability (Pettersson et al., 2016); the independent association of the two disorders with mood, anxiety and personality disorders (Van Emmerik-van Oortmerssen et al., 2014); developmental pathways and social impairments (Molina and Pelham Jr, 2014); and possible neurocognitive deficits (Groenman et al., 2015). The combination of ADHD and substance use disorders results in high risk of severe emotional and interpersonal problems (Van Emmerik-van Oortmerssen et al., 2014).
Several reviews have examined treatment of co-existing ADHD and any substance use disorder, again with mixed results (Cunill et al., 2015; Perez de los Cobos et al., 2014; Wilens and Morrison, 2012). These reviews assessed studies with a range of substance use disorders, different population groups and varying interventions. Results have indicated generally mild to moderate improvement in outcomes on ADHD measures but not in substance use outcomes. Authors conclude that a moderate reduction in ADHD symptoms that is not accompanied by reduction in substance use is of ‘limited clinical interest’ (Cunill et al., 2015) and that pharmacological treatment is ‘not particularly useful’ for the treatment of either condition (Wilens and Morrison, 2012). Stimulant medication has also been investigated as substitution pharmacotherapy for treatment of stimulant use disorder, with mixed results but some promise (Castells et al., 2010; Dursteler et al., 2015; Herin et al., 2010; Mariani and Levin, 2012).
This review focuses on the treatment of co-existing stimulant use disorder and ADHD – a specific case due to pharmacological similarities between illicit amphetamine-type stimulants and prescribed stimulant medications. Stimulants facilitate the activity of monoamine neurotransmitters (dopamine, norepinephrine and serotonin), in the central and peripheral nervous systems (Ciccarone, 2011). Cocaine, amphetamine, methamphetamine and methylphenidate elevate synaptic monoamines via varying mechanisms in facilitating secretion and inhibiting uptake (Sulzer et al., 2005; Svetlov et al., 2007). Methylphenidate has an action similar to cocaine, with comparable affinity to the dopamine transporter, rate of brain uptake and levels of synaptic dopamine, but differing markedly in their rate of clearance, half-life and mechanism of effect on the dopamine transporter (Calipari et al., 2014; Kollins et al., 2001; Volkow et al., 1995).
Stimulant medications are used in the treatment of childhood ADHD, with good effect (Punja et al., 2016; Storebø et al., 2015). The self-medication hypothesis has been raised by some authors as an explanatory model for stimulant use in individuals with untreated ADHD, with individuals reporting either relief of distress or improved function from illicit stimulant use (Mariani et al., 2014; Wilens, 2004; Zulauf et al., 2014).
On the other hand, misuse and diversion of prescription stimulants are common, especially in people who use illicit substances (Darredeau et al., 2007; Sweeney et al., 2013), creating challenges for safe prescribing. A Canadian study found 44% of adults prescribed methylphenidate admitted diversion and 29% admitted inappropriate use (Darredeau et al., 2007). A US community-based survey identified 6.2% of the population admitting lifetime non-medical use of prescriptions stimulants (Center for Behavioral Health Statistics and Quality, 2015). While the Australian National Drug Strategy Household Survey does not obtain data regarding non-medical use of prescription stimulants for equivalent Australian Data (Australian Institute of Health and Welfare, 2014), the NSW Poisons Information Centre reported increased contact for intentional exposures to ADHD medication over the past decade (Cairns et al., 2016).
This systematic review of randomised controlled trials aims to identify effective treatment of co-existing adult ADHD and stimulant use disorder, reviewing outcomes related to either ADHD measures or non-sanctioned stimulant use.
Methods
Eligibility criteria
Studies were selected to satisfy the following inclusion criteria: (1) randomised controlled trials comparing any treatment arm with a control group, (2) participants including adult humans, (3) participants meeting DSM or equivalent criteria for adult ADHD, (4) a majority of participants meeting DSM or equivalent diagnostic criteria for stimulant use disorder, (5) data measuring outcomes for either ADHD or substance use measures and (6) published in English language. No sample size or publication date restrictions were imposed.
Broad inclusion criteria were adopted in order to identify all potentially relevant studies.
Information sources
This search was applied to MEDLINE (1946–present), EMBASE (1947–present), CINAHL (1981–present), PsycINFO (1806–present) and Cochrane. Each search was run on 29 November 2016.
Search
The following search terms were used to search all databases, utilising exploded Medical Subject Headings (MeSH) terms combined with title and abstract searches: Attention Deficit Disorder with Hyperactivity or ADHD; Amphetamines, Cocaine, Central Nervous System Stimulants, methamphetamine or methylphenidate; and Substance-Related Disorders, substance use disorder, dependence, addiction, abuse or misuse. The Medline search terms are included in Supplementary Appendix 1. These search terms were adapted for other database systems. Screening was performed by one author.
To ascertain the quality of eligible randomised trials, adequacy of randomisation and concealment of allocation, and blinding of participants, health care providers and data collectors were determined.
Synthesis of results
Because the study designs, participants, interventions and reported outcomes measures varied markedly, a quantitative synthesis could not be undertaken.
Results
Study selection
A total of eight trials including a total of 511 participants were identified for inclusion in this review (Carpentier et al., 2005; Ginsberg and Lindefors, 2012; Konstenius et al., 2010, 2014; Levin et al., 2006, 2007, 2015; Schubiner et al., 2002) (see Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] diagram).
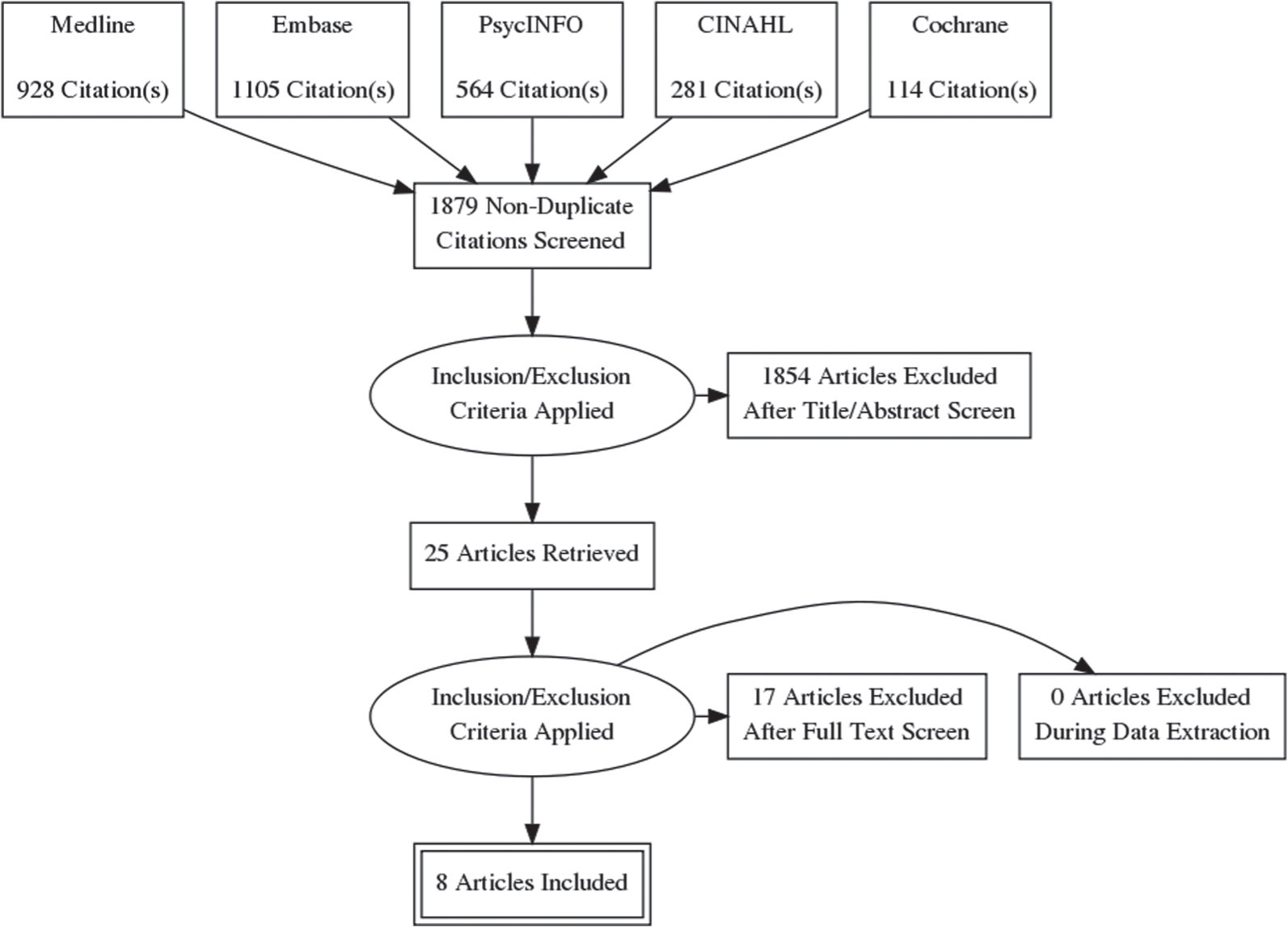
PRISMA study selection flow diagram.
Study characteristics
All of the studies compared stimulant treatment to placebo (Table 1). Seven studies compared formulations of methylphenidate to placebo (Carpentier et al., 2005; Ginsberg and Lindefors, 2012; Konstenius et al., 2010, 2014; Levin et al., 2006, 2007; Schubiner et al., 2002), with one of these studies also including a bupropion treatment arm (Levin et al., 2006). The eighth study compared extended-release mixed amphetamine salts with placebo (Levin et al., 2015).
Characteristics of included studies.
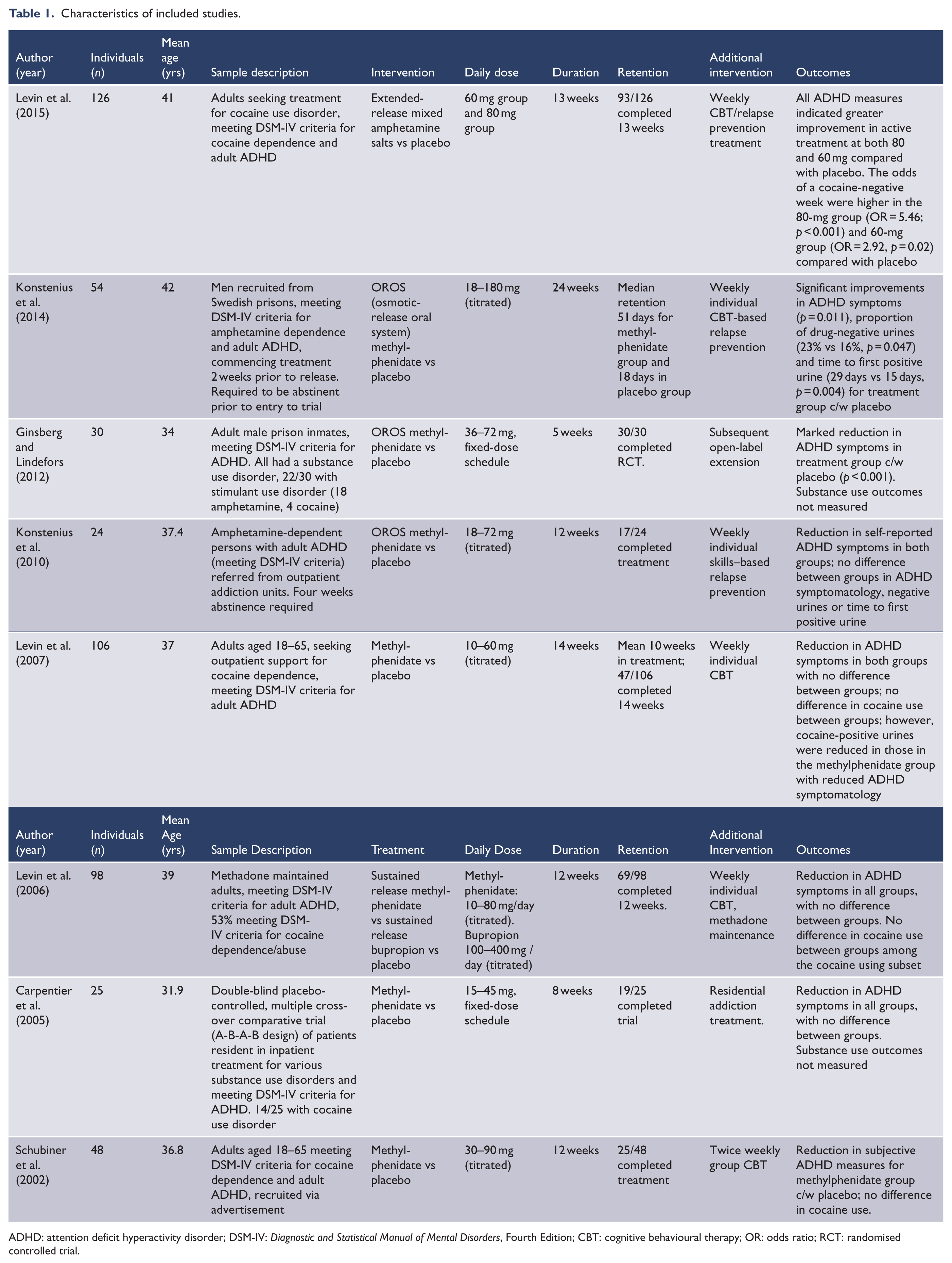
ADHD: attention deficit hyperactivity disorder; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; CBT: cognitive behavioural therapy; OR: odds ratio; RCT: randomised controlled trial.
There was significant variation in daily dosage of methylphenidate, with maximum dosage varying between 45 and 180 mg. Five studies titrated the doses to effect or side effect (Konstenius et al., 2010, 2014; Levin et al., 2006, 2007; Schubiner et al., 2002), and three studies used fixed-dose regimens (Carpentier et al., 2005; Ginsberg and Lindefors, 2012; Levin et al., 2015).
Three studies required a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnosis of cocaine dependence (Levin et al., 2006, 2007, 2015), and two studies required a DSM-IV diagnosis of amphetamine dependence (Konstenius et al., 2010, 2014). Three other studies were included that accepted subjects primarily dependent on other substances, but a majority of subjects in these studies met DSM-IV criteria for cocaine or amphetamine dependence (Carpentier et al., 2005; Ginsberg and Lindefors, 2012; Schubiner et al., 2002).
All studies included outcome measures of ADHD, and six of eight also included substance use outcomes (Konstenius et al., 2010, 2014; Levin et al., 2006, 2007, 2015; Schubiner et al., 2002). ADHD outcome measures varied, utilising the ADHD Rating Scale-IV, physician-rated and self-rated efficacy indexes, the ADHD Symptom Checklist, Adult ADHD Investigator Symptom Rating Scale, Conners’ Adult ADHD Self-Rating Scale–Screening Version (CAARS-SV), Clinical Global Impression Scale (CGI), the Adult ADHD Investigator Symptom Rating Scale (AISRS) and the Adult ADHD Rating Scale (AARS). Substance use outcomes measures included urine drug screens, self-report and craving scales.
All of these studies included adults only (mean age range: 31.9–42 years), and two of the studies were restricted to males (Ginsberg and Lindefors, 2012; Konstenius et al., 2014). Study duration varied between 5 and 24 weeks. All studies included additional psychosocial intervention, most commonly cognitive behavioural therapy. Four studies were carried out in the United States (Levin et al., 2006, 2007, 2015; Schubiner et al., 2002), three in Sweden (Ginsberg and Lindefors, 2012; Konstenius et al., 2010, 2014) and one in the Netherlands (Carpentier et al., 2005). Subjects were drawn from outpatient addiction treatment centres in three studies (Konstenius et al., 2010; Levin et al., 2007, 2015), from prison in two studies (Ginsberg and Lindefors, 2012; Konstenius et al., 2014) and one study each from an opiate substitution programme (Levin et al., 2006), a residential addiction treatment facility (Carpentier et al., 2005) and non-treatment-seeking community participants (Schubiner et al., 2002). Four studies occurred with currently abstinent subjects (Carpentier et al., 2005; Ginsberg and Lindefors, 2012; Konstenius et al., 2010, 2014) and four with currently substance-using subjects (Levin et al., 2006, 2007, 2015; Schubiner et al., 2002).
Risk of bias
Quality assessment is based on PRISMA guidelines (Liberati et al., 2009), with results indicated in Table 2. All studies are reported as randomised controlled trials. The majority of studies reported the process of randomisation and concealment and clarified that blinding was not broken. Question marks (?) indicated inadequate reporting within the article on a particular criterion. No study explicitly failed to fulfil the markers of validity. As this review only includes published studies, risk of publication bias is relevant.
Quality of included studies.
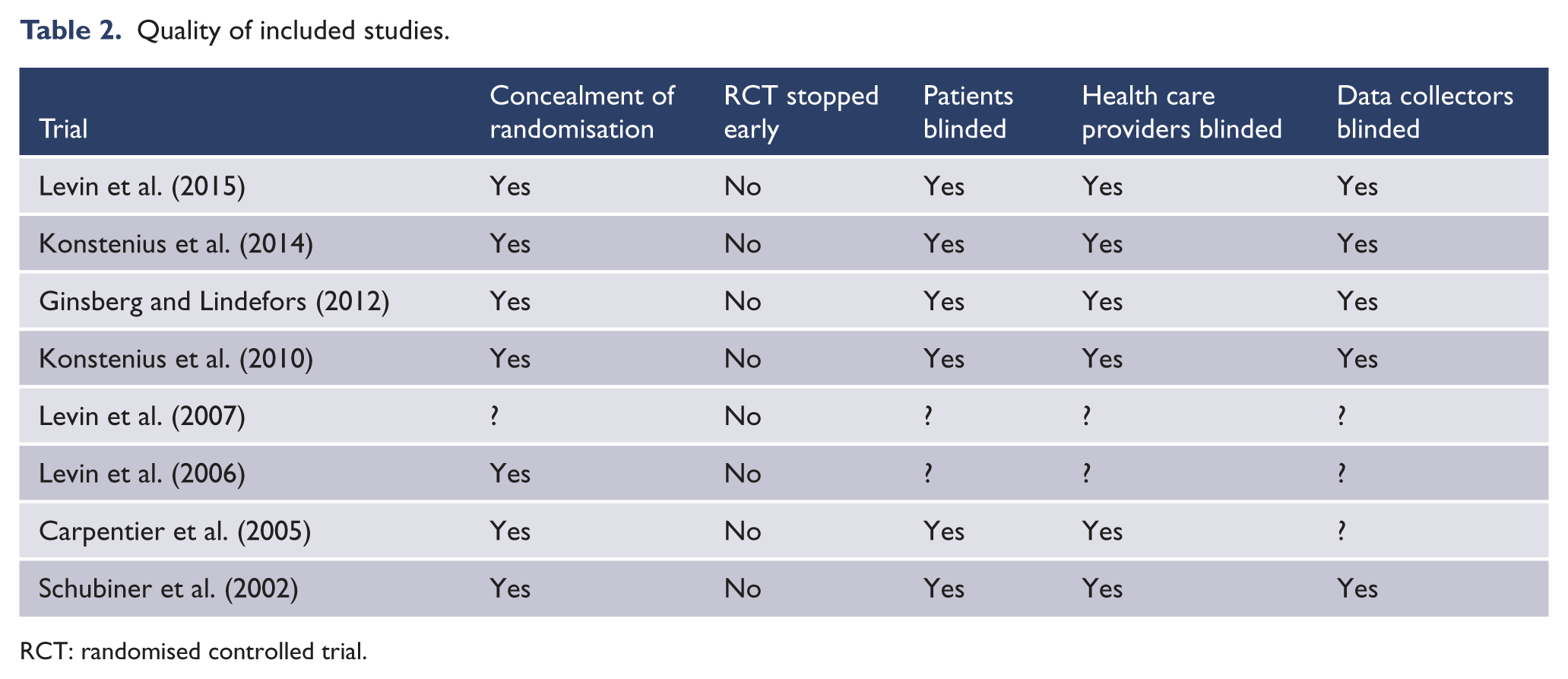
RCT: randomised controlled trial.
Results of individual studies
Substance use measures
Two of six studies that reported substance use outcomes showed significant improvement for treatment arms compared with placebo (Konstenius et al., 2014; Levin et al., 2015).
Levin et al. (2015) found (for extended-release mixed amphetamine salt) the odds of a cocaine-negative week (by urine drug screen) were higher in the 80-mg group (odds ratio [OR] = 5.46; 95% confidence interval (CI) = [2.25, 13.27]; p < 0.001) and 60-mg group (OR = 2.92; 95% CI = [1.15, 7.42]; p = 0.02) compared with placebo. Rates of continuous abstinence in the last 3 weeks were greater for the medication groups than the placebo group: 30.2% for the 80-mg group (p = 0.004) and 17.5% for the 60-mg group (p = 0.04) vs 7.0% for placebo.
Konstenius et al. (2014) found a significant difference in the proportion of drug-negative urines in the methylphenidate group (Md = 23%, n = 27) compared to the placebo group (Md = 16%, n = 27) (p = 0.047).
Four other studies (Konstenius et al., 2010; Levin et al., 2006, 2007; Schubiner et al., 2002) found no decrease in substance use measured by urine drug screen for methylphenidate compared with placebo. Levin et al. (2006) also found no difference in substance use measures for bupropion compared with placebo.
ADHD outcome measures
Four of eight studies reporting ADHD outcome measures showed significant improvement in ADHD outcome measures compared with placebo (Ginsberg and Lindefors, 2012; Konstenius et al., 2014; Levin et al., 2015; Schubiner et al., 2002).
Levin et al. (2015), in the one study of extended-release mixed amphetamine salt, found improvement in the proportion of subjects achieving clinically significant 30% reduction in AISRS score at the last enrolment week compared with week 0 for both treatment groups. Results showed proportions achieving 30% reduction of 58.1% for the 80-mg group, 75.0% for the 60-mg group and 39.5% for the placebo group. ORs were 2.27 (p = 0.07) for the 80-mg group vs placebo and 5.23 (p < 0.001) for the 60-mg group versus placebo.
Konstenius et al. (2014) found that the methylphenidate group showed significantly greater improvement in CAARS-SV score for all ADHD symptoms (95% CI = [−14.18, −3.28], p = 0.002) compared with placebo.
Schubiner et al. (2002) found the physician rated 21% of the placebo group as having moderate improvement versus 77% of the methylphenidate group, and the methylphenidate group rated themselves as significantly better than the placebo group (p < 0.02). No statistically significant differences were found for inattentive or hyperactive symptoms on the ADHD checklist.
Ginsberg and Lindefors (2012) found mean scores for the primary outcome measure, CAARS-SV, were significantly decreased by 19.6 in the methylphenidate group compared with a non-significant decrease of 1.9 in the placebo group (p < 0.001).
Four studies found no difference in ADHD outcome measures for formulations of methylphenidate compared with placebo (Carpentier et al., 2005; Konstenius et al., 2010; Levin et al., 2006, 2007). Each of these studies showed reduction in ADHD outcome measures in both methylphenidate and placebo groups, with no significant difference between groups.
Levin et al. (2006) also found no difference in ADHD outcome measures for bupropion compared with placebo.
Adverse effects and adverse events
Dry mouth was the only adverse event that occurred significantly more frequently in the group receiving extended-release mixed amphetamine salts compared with placebo (Levin et al., 2015).
In trials involving methylphenidate, adverse events were generally of mild–moderate severity (Konstenius et al., 2014; Levin et al., 2015), except for one event of blurred vision (Konstenius et al., 2010) and two severe events of hypertension and disorientation, both of which resolved with a reduction in dose (Schubiner et al., 2002).
Significant adverse effects were not recorded for bupropion compared with placebo (Levin et al., 2006).
Discussion
Based on the results of this review, there is limited evidence of benefit of treatment for comorbid ADHD and substance use for both outcomes. The majority of randomised controlled trials published for the treatment of co-existing ADHD and stimulant use disorder relates to stimulant medication (predominantly methylphenidate). Four of eight studies included in this review found treatment was no better than placebo for ADHD measures, and four of six found treatment was no better than placebo for substance use measures.
Notably, studies to show effect included those with the highest treatment dosage (Konstenius et al., 2014; Levin et al., 2015; Schubiner et al., 2002). The two studies showing effect in reducing substance use were the two studies utilising higher than usual ADHD treatment dosage (Konstenius et al., 2014; Levin et al., 2015). Substitution pharmacotherapy is effective for opioid and nicotine dependence, and is a plausible strategy for treating stimulant dependence, but similar to opioid substitution is likely to require robust doses (Mariani et al., 2014). Similarly, individuals with a long history of daily illicit stimulant use are likely to have increased tolerance to stimulants, and may need a higher dose of prescribed stimulants to reduce ADHD symptoms than previously stimulant-naive individuals (Konstenius et al., 2014).
The main limitation of this review arises from the paucity of evidence in this area, given that only eight RCTs (with a total of 511 participants) met inclusion criteria, despite a broad and inclusive search protocol. There was significant heterogeneity in the included studies, both in terms of study populations and in the study design and treatment(s) trialled. That evidence supporting stimulant treatment is limited reflects that studies generally included limited numbers, specific populations, short duration and high dropout rates. Studies included a range of subjective measures, which can cross over different diagnoses and may not be validated in some populations.
Significant improvement in ADHD measures was found in the placebo group in seven of eight studies, in addition to improvement occurring in the treatment group in all studies. All studies included psychosocial intervention, usually based on cognitive behavioural therapy or targeted at substance use and relapse prevention. These interventions may have been effective and may explain some of the improvement in the placebo groups (Van der Oord et al., 2008).
Limitations
Studies were included only if published in English Language. Non-published studies were not included, leading to possible publication bias. The majority of studies reviewed investigated effect of methylphenidate, with evidence limited for other interventions.
Case discussion: clinical implications
The clinical assessment and treatment of clients with co-existing ADHD and stimulant use disorder involve a range of challenges. There are inherent difficulties in making a valid diagnosis of ADHD in this population. Features associated with intoxication or withdrawal may mimic ADHD symptoms; cognitive deficits arising from substance abuse can hinder the ability to recall ADHD symptoms for appropriate diagnostic purposes or may be attributed to ADHD itself; it can be difficult to access appropriate longitudinal data to confirm a diagnosis; patients may feign ADHD symptoms in order to obtain stimulant medication (Levin, 2007), and ADHD symptoms overlap a range of other psychiatric diagnoses (Vergne et al., 2011). Once a diagnosis of ADHD can be established, there may be particular risks related to prescribing of stimulant medication, such as diversion and abuse (Cairns et al., 2016; Weyandt et al., 2013), psychosis and cardiac complications (Lakhan and Kirchgessner, 2012).
The case example illustrates the difficulty in using the available data to guide treatment. Only four of the studies included subjects currently using stimulants; all of these related to cocaine use disorder (whereas Adam is currently using methamphetamine), and only one found that treatment reduced substance use.
Adam reports a childhood diagnosis of ADHD. His request to recommence ADHD treatment in adulthood raises a number of clinical issues. First, he presents with daily methamphetamine use and is likely to have methamphetamine dependence. In terms of establishing his childhood ADHD diagnosis, a thorough history and collateral information would be required to support this. Further clarification of the current nature and extent of ADHD symptoms, and the impact of this on his level of function, will assist in determining whether he continues to experience impairment, as the diagnosis resolves prior to adulthood in a majority of cases (Barbaresi et al., 2013). Caution is needed in making a diagnosis in the population (Levin, 2007), and it can often be extremely difficult to delineate symptoms arising from substance dependence (or other comorbidities) from ADHD itself.
If a diagnosis of ADHD is considered valid, then a treatment plan may potentially include stimulant medication. However, the prescribing of drugs of dependence to individuals with a history of substance use disorder needs careful consideration. If this course of action is deemed appropriate, then prescribing should occur with due regard to ensuring compliance and minimising misuse and diversion of such medication (Cairns et al., 2016). Monitoring strategies can include regular review, examination for injection sites or for signs of intoxication or withdrawal, frequent collection of medication from the pharmacy and urine drug screening with gas chromatography/mass spectrometry (GC/MS) or liquid chromatography/tandem mass spectrometry (LC/MS) confirmation. There is a theoretical benefit of using a slow release product, such as lisdexamfetamine, which might have a lower abuse potential than alternatives, but further studies are needed to see whether this is the case.
The use of any stimulant medication should be considered a trial of treatment requiring significant functional gains in order for this treatment to be continued, in a similar manner to which a trial of opioids might be attempted in a patient with chronic non-malignant pain.
Conclusion
Implications for practice
This study found limited results for the efficacy of treatment of patients with comorbid stimulant use disorder and ADHD. Reduction in ADHD symptoms was identified in four of eight studies, and reduction in illicit stimulant use was identified in two of six studies. It is not possible on this basis to give clear recommendation for treatment.
The most promising results related to two studies utilising higher dosage of prescribed stimulants (Konstenius et al., 2014; Levin et al., 2015). Both of these studies are recent studies and have not been included in previous reviews.
While findings that higher doses of prescribed stimulants may reduce both ADHD symptoms and illicit stimulant use, this needs to be viewed cautiously in the context of the extant literature, and the results require replication to clarify potential benefits. Prescription stimulant treatment should follow cautious diagnosis, clear functional goals for treatment, and containment strategies to reduce risks of diversion or misuse.
Implications for research
Future research is required to continue to examine treatment strategies to address comorbid ADHD and stimulant use disorder. Recent promising results need to be repeated with clarification of which stimulant medications are likely to be effective, whether treatments are more effective for cocaine or amphetamine use disorder and which non-pharmacological treatments are effective. Further research would also be beneficial in examining whether improvements in substance use are correlated with improvements in ADHD measures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.