
Abstract
Objective:
This study examined the prescribing patterns of several first- (FGAs) and second-generation antipsychotic (SGAs) medications administered to older Asian patients with schizophrenia during the period between 2001 and 2009.
Method:
Information on hospitalized patients with schizophrenia aged 65 or older was extracted from the database of the Research on Asian Psychotropic Prescription Patterns (REAP) study (2001–2009). There were no older patients in Thailand, therefore data on 467 patients in eight Asian countries and territories including China, Hong Kong SAR, India, Japan, Korea, Malaysia, Singapore, and Taiwan were analysed. Cross-sectional socio-demographic data, clinical characteristics and antipsychotic prescriptions were assessed using a standardized protocol and data collection procedure.
Results:
Of the 467 patients, 192 patients (41.1%) received FGAs only, 166 (35.5%) received SGAs only and 109 (23.3%) received a combination of FGAs and SGAs. Of the FGAs, haloperidol was the most commonly used (31.3%; mean 9.4 ± 6.7 mg/day), followed by chlorpromazine (15.4%; mean 126.4 ± 156.4 mg/day) and sulpiride (6.6%; mean 375.0 ± 287.0 mg/day). Of the SGAs, risperidone was the most commonly used (31.5%; mean 4.5 ± 2.7 mg/day), followed by olanzapine (13.1%; mean 13.6 ± 6.5 mg/day), quetiapine (7.3%; mean 325.0 ± 237.3 mg/day) and aripiprazole (1.9%; mean 17.6 ± 7.7 mg/day).
Conclusions:
FGAs and higher doses of certain SGAs (risperidone, olanzapine and quetiapine) were still commonly dispensed to older Asian patients with schizophrenia. Considering older patients’ reduced tolerability of potentially severe side effects associated with FGAs and higher doses of certain SGAs, continuing education and training addressing the rational use of antipsychotics in this population is clearly needed.
Introduction
Many patients with schizophrenia live into older adulthood (Kohen et al., 2010). In contrast to younger patients, older patients with schizophrenia are a special population characterized by higher likelihood of drug-induced side effects, poorer general health and the need for lower doses of psychotropic medications (Meyers and Jeste, 2010; Uchida et al., 2009). Therefore, guidelines for the treatment of schizophrenia in younger adult patients cannot be reliably applied to older patients (Uchida et al., 2009). For example, the US ‘geriatric use’ rule of 1997 (US Food and Drug Administration, 1997) asked that the drug industry should provide supplemental data on specific classes of medications, including psychotropic drugs, for geriatric patients. To obtain approval for standard indications, however, phase 3 drug trials usually focus on those patients who would be most likely to benefit from the drug and who are least likely to suffer any drug-related adverse events. Consequently, it is difficult for the drug industry to conduct studies on ‘special populations’, such as older patients, to minimize the risk for adverse events (Meyers and Jeste, 2010). As a result, unlike the many treatment guidelines for younger adult patients with schizophrenia, to date there have been few guidelines for older patients. To provide rational guidelines, Alexopoulos et al. (2004) surveyed expert opinions for recommendations on indications for antipsychotics for patients aged 65 years and older. For those with schizophrenia, the expert consensus guidelines suggested that the first-line choice should be risperidone (1.25–3.5 mg/day), followed by quetiapine (100–300 mg/day), olanzapine (7.5–15 mg/day) and aripiprazole (15–30 mg/day). In contrast, first-generation antipsychotics (FGAs) were not recommended as first-line choices for this population.
To date, there have been no international studies investigating the prescribing patterns of antipsychotic medications in older Asian patients with schizophrenia. In our study, we conducted a secondary analysis of the data of the Research on Asian Psychotropic Prescription Patterns (REAP) project, which sought to examine the use of major FGAs and second-generation antipsychotics (SGAs), including aripiprazole, chlorpromazine, haloperidol, olanzapine, quetiapine, risperidone and sulpiride in older Asian patients with schizophrenia during the period between 2001 and 2009.
Methods
Settings, study design and subjects
The study was part of the REAP project, a psycho-pharmaco-epidemiological project on psychotropic drug prescription trends in hospitalized patients with schizophrenia in Asia. The REAP project was initially conducted in July 2001 followed by two waves of studies in July 2004 and then October 2008–March 2009 using the same design and standardized protocol. Consensus meetings on data collection and uniformity of data entry were held prior to each survey. The participating countries and territories included mainland China, Hong Kong, Japan, Korea, Singapore and Taiwan. Centres in India, Malaysia and Thailand joined the surveys in 2009. Details of the REAP project have been described elsewhere (Chong et al., 2004) and are summarized as follows. Patients were included in the analysis of data if they had a diagnosis of schizophrenia, as defined by the criteria of the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) or the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), were aged 65 years or older, took antipsychotic medications and were willing to provide written or oral consent according to the requirements of the Clinical Research Ethics Committee in the respective study sites. Patients having clinically significant medical illnesses were excluded.
Eligible patients were enrolled consecutively, their socio-demographic characteristics were recorded and cross-sectional clinical data including age, sex, length of illness, the presence or absence of significant psychiatric symptoms within the past month and the prescription of antipsychotics were collected by reviewing case notes in 2001, and by either a review of case notes only or a review of case notes supplemented by a clinical interview in both 2004 and 2009 using a questionnaire designed for the study. Data were collected by the psychiatrist treating the patient or by members of the research team with the agreement of the patient’s psychiatrist.
The study was approved by the Clinical Research Ethics Committees in the respective study sites. Given the anonymous nature of this observational study and the minimal risk to patients, patients’ informed consent was exempted in some participating study sites according to the requirements of the local Clinical Research Ethics Committee (Shinfuku and Tan, 2008) if only a review of case notes was used. The requirements of the Clinical Research Ethics Committee usually varied on a local basis across different study sites.
Statistical analysis
Descriptive statistics were used in this study. Continuous variables are reported as means ± standard deviations (SDs), and dichotomous variables are reported as numbers and percentages (%).
Results
Altogether, 31 psychiatric institutions were involved in 2001, 25 in 2004 and 50 in 2009. A total of 467 patients satisfied the study criteria; 159 in 2001, 161 in 2004 and 147 in 2009. Table 1 summarizes the socio-demographic and clinical characteristics of the study population and the use of major antipsychotic drugs for the whole sample and also separately for patients by study period. In total, 192 patients (41.1%) received FGAs only, whereas 166 (35.5%) received SGAs only and 109 (23.3%) received a combination of FGAs and SGAs. Of the FGAs, haloperidol was the most commonly used (31.3%; mean 9.4 ± 6.7 mg/day), followed by chlorpromazine (15.4%; mean 126.4 ± 156.4 mg/day) and sulpiride (6.6%; mean 375.0 ± 287.0 mg/day). Of the SGAs, risperidone was the most commonly used (31.5%; mean 4.5 ± 2.7 mg/day), followed by olanzapine (13.1%; mean 13.6 ± 6.5 mg/day), quetiapine (7.3%; mean 325.0 ± 237.3 mg/day) and aripiprazole (1.9%; mean 17.6 ± 7.7 mg/day). Table 2 shows the dose ranges for the SGAs.
Basic demographic and clinical characteristics of older Asian patients with schizophrenia in REAP surveys (2001–2009) and the most commonly prescribed antipsychotic drugs.
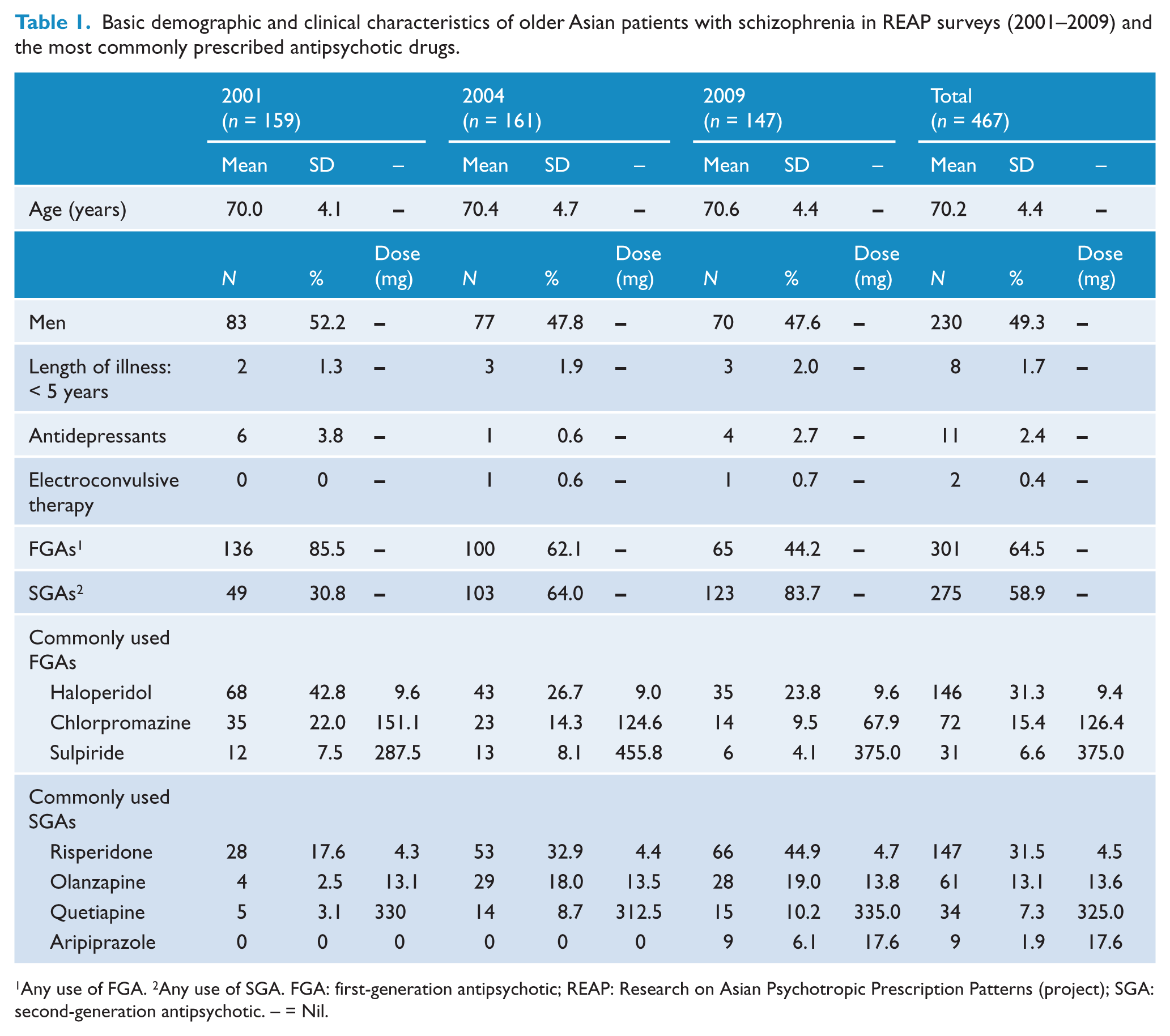
Any use of FGA. 2Any use of SGA. FGA: first-generation antipsychotic; REAP: Research on Asian Psychotropic Prescription Patterns (project); SGA: second-generation antipsychotic. – = Nil.
Dose range of major second-generation antipsychotics in older Asian patients with schizophrenia between 2001 and 2009 (n = 467).
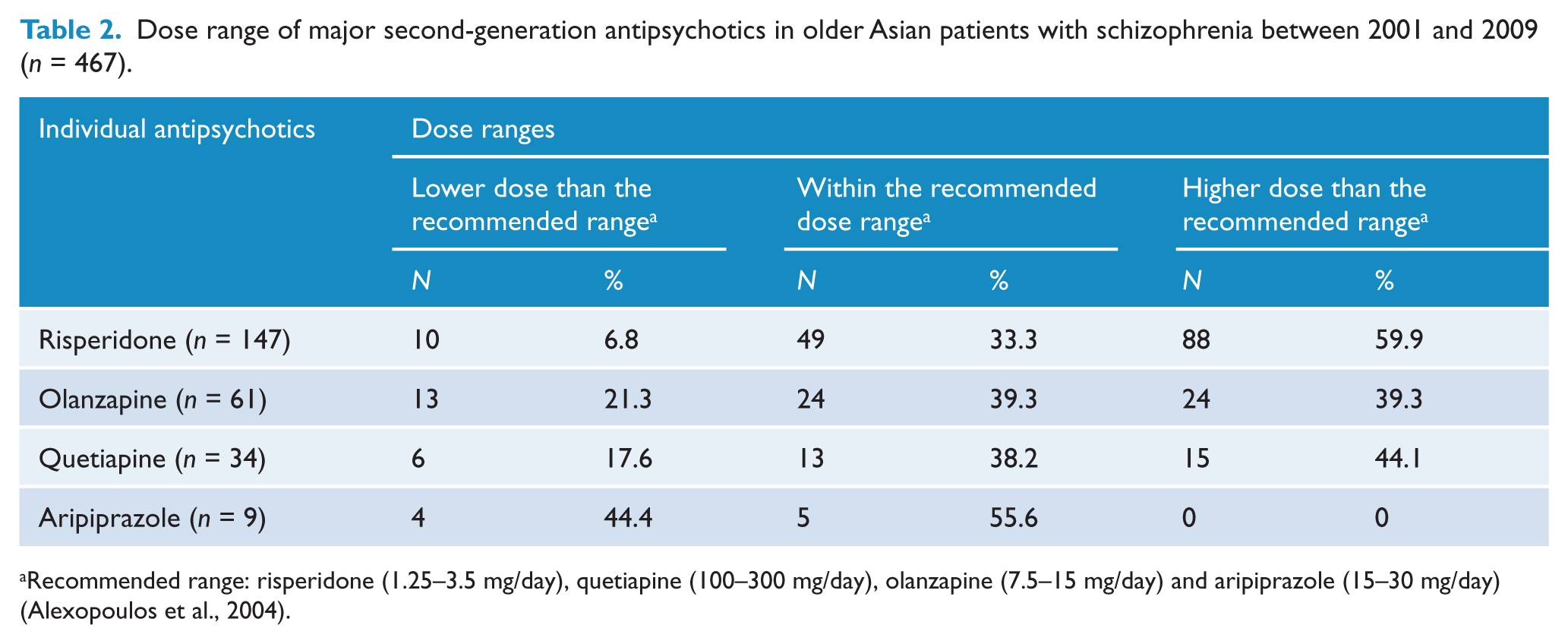
Recommended range: risperidone (1.25–3.5 mg/day), quetiapine (100–300 mg/day), olanzapine (7.5–15 mg/day) and aripiprazole (15–30 mg/day) (Alexopoulos et al., 2004).
Discussion
The major finding of this study was that risperidone was the most commonly used antipsychotic in older Asian patients with schizophrenia (31.5%), followed by haloperidol (31.3%), chlorpromazine (15.4%) and olanzapine (13.1%) in the pooled sample for the period between 2001 and 2009. These prescribing patterns are not entirely consistent with a previously published expert consensus guideline for treating older patients (65 years and older) with schizophrenia (Alexopoulos et al., 2004), which suggested that risperidone should be used as the first-line choice followed by quetiapine, olanzapine and aripiprazole. In the past decade, numerous studies have reported the advantages of risperidone, quetiapine and olanzapine in terms of safety, tolerability and efficacy compared to FGAs in the treatment of older patients with schizophrenia (Barak et al., 2002; Hwang et al., 2001; Hwang et al., 2003; Madhusoodanan et al., 2000; Ritchie et al., 2003), which supports the expert consensus guideline for the use of antipsychotic drugs in older patients. Surprisingly, we found that 64.5% of older patients received at least one type of FGA in the current sample. Although the figure decreased over time (85.5% in 2001, 62.1% in 2004 and 44.2% in 2009), approximately 50% of older patients were still on FGAs in 2009. The underlying reasons for this unexpected finding cannot be identified based on the cross-sectional design of this study. We speculate that a number of biological and socio-economic/cultural factors, including prior antipsychotic drug treatment, psychopharmacological traditions, variable access to different antipsychotic drugs, cost, insurance coverage and health policy, might all contribute to the frequent use of FGAs in older Asian patients with schizophrenia. A large-scale, retrospective cohort study (Wang et al., 2005) suggested FGAs were associated with a significantly higher risk of death (relative risk: 1.37; 95% CI: 1.27–1.49) compared to SGAs in older patients. Considering the increased susceptibility for antipsychotic-induced adverse events, such as extrapyramidal symptoms (EPS), and low tolerability to FGAs in older patients, in the absence of a clearly documented rationale, the use of FGAs should be discouraged in this population.
It should be noted that almost a quarter of older patients in this study were receiving a combination of SGAs and FGAs. To date, however, this practice has not been recommended by any treatment guidelines for either older or younger patients due to lack of improved efficacy, increased drug interactions, risk of side effects, non-adherence and cost (Kreyenbuhl et al., 2010; Mojtabai and Olfson, 2010; Zink et al., 2010).
In the expert consensus guideline (Alexopoulos et al., 2004), the recommended dose range for risperidone was 1.25–3.5 mg/day, while the ranges for quetiapine, olanzapine and aripiprazole were 100–300 mg/day, 7.5–15 mg/day and 15–30 mg/day, respectively. In this study, of the patients on risperidone, 59.9% received a dose that was higher than the recommended range. The corresponding figure for those on olanzapine and quetiapine was 39.3% and 44.1%, respectively. High doses of antipsychotic drugs are used both to enhance treatment response and for sedation and behavioral control; yet, data on the effectiveness and safety of this practice in older patients are limited. High doses of antipsychotic drugs may be associated with dose-response side effects, which are of particular concern in older patients who are more sensitive to them (Meyers and Jeste, 2010).
We also found that 6.8% of patients on risperidone received a dose that was lower than the recommended range. The corresponding figures for those on olanzapine, quetiapine and aripiprazole were 21.2%, 17.6% and 44.4%, respectively. We speculate that the possible reasons for the lower doses include the following:
Asian patients usually require lower doses of antipsychotics and they are more sensitive to side effects, such as EPS, than their Western counterparts (Chiu et al., 1991; Frackiewicz et al., 1997).
A combination of SGAs and FGAs may lead to the use of lower doses of the individual antipsychotics (although the combination may lead to higher antipsychotic doses overall).
The expert consensus guideline (Alexopoulos et al., 2004) used in this study was released in 2004 and we were unable to locate an up-to-date version or other guidelines for the use of antipsychotics in older patients.
Therefore we cannot exclude the possibility that lower (or higher) SGA dose ranges administered to older patients with schizophrenia have become accepted in clinical practice and would replace previous recommendations as research and experience with these drugs evolves.
Limitations of the study
The limitations of this study include the following:
The study targeted only hospitalized older patients in selected psychiatric institutions in eight Asian countries and territories with non-random sampling, therefore the results cannot be applied to all older schizophrenia patients in Asia.
Some important factors likely to influence antipsychotic prescription, such as the use of prior antipsychotics, antipsychotic response, patients’ contraindications to certain antipsychotics, local prescription guidelines, type of psychiatric facilities (e.g. chronic vs. acute) and reimbursement olicies were not evaluated. Additionally, augmentation strategies such as electroconvulsive therapy and adjunctive benzodiazepines and antidepressants were likely to influence the choice and doses of antipsychotic drugs. As only the treatment of a few patients was augmented in this study (Table 1), the potential influence of adjunct treatment was minimal.
The exclusion of patients with significant medical conditions might have affected the results.
Due to the cross-sectional nature of the study, we could not examine patients’ previous history of antipsychotic treatment or any other determinant of current antipsychotic treatment.
Sample sizes varied among participating countries/territories.
The limitations of this study, however, cannot offset its striking findings. In conclusion, the results suggest that the prescription of FGAs for older schizophrenia inpatients in Asia is very common. A considerable proportion of patients received higher doses of SGAs, which is not consistent with earlier expert consensus recommendations (Alexopoulos et al., 2004). Considering the potentially hazardous side effects of FGAs and higher doses of SGAs for this population, continuing education and training addressing the rational use of antipsychotics is clearly needed. In addition, local treatment guidelines for older Asian patients with schizophrenia need to be developed.
The increased risk of metabolic syndrome for patients on SGAs remains a great concern. Metabolic syndrome contributes to a number of troublesome psychological and physical co-morbidities, such as depression (Herva et al., 2006), diabetes mellitus (Mukherjee et al., 1996) and cardiovascular disease (Robinson et al., 2005).
There are no ‘gold-standard’ treatment guidelines for the use of antipsychotic drugs for the population of schizophrenia patients. Antipsychotic treatment should be individualized carefully, considering each patient’s preferences and their clinical condition.
Footnotes
Acknowledgements
The authors are grateful to the following clinicians involved in the data collection: Hong Deng and Wei Hao in China; Ajit Avasthi, Dipesh Bhagabati, Roy Abraham Kallivayalil, Shubhangi R Parkar and YC Janardhan Reddy in India; Tateno Masaru, Masamune Yayoi, Akiyama Tsuyoshi, Sato Soichirou, Nakagome Kazuyuki, Nakamura Jun and Kuroki Toshihide in Japan; Tae-Yeon Hwang, Seok Hyeon Kim, Yo Wang Lee and Jong- Il Lee in Korea; Tung-ping Su, Shih-ku Lin,Tzu-ting Chen, Chieh-hsin Chang, Hong-chieh Hsu, Chi-Fa Hung and Cheng-chung Chen in Taiwan; Krisakorn Sukavatvibul, Jittima Kleawtanong, Tantawan Suradechasakul, Manote Lotrakul and Usaree Srisutudsanavong in Thailand; and Norharlina Bahar in Malaysia. The authors would also like to thank the clinicians who helped to organize the study in each study site.
Funding
This study was supported in part by grants from the National Natural Science Foundation of China (81171270, 30800367, 30770776), the Beijing Nova Program of the Beijing Municipal Science & Technology Commission (2008B59), the Chinese University of Hong Kong (Direct Grant for Research; Project 2041454), the Institute of Mental Health research grant (CRC 249/2008) in Singapore, the Bureau of National Health Insurance (DOH92-NH-1025) in Taiwan, Chang Gung Memorial Hospital (CMRPG83043) and the Taipei City Government (97001-62-010), Taiwan.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.