
Abstract
Objective:
Access to adequate housing consistent with personal preferences and needs is a human right and supports recovery from psychosis. This study aimed to: (1) describe people with psychosis living in different housing types, and their preferences and needs; (2) explore selected demographic and social inclusion correlates in relation to housing; and (3) compare two subgroups – participants living in supported group accommodation and supported housing – on key demographic, functional, clinical and social inclusion variables.
Method:
Current housing, preferences, needs and assistance, and housing-related social inclusion variables were assessed in a two-phase prevalence survey conducted within seven catchment areas across five Australian states. Two supported housing models were compared: supported group accommodation and supported housing (rental accommodation with in-reach support). Descriptive statistics were used.
Results:
Of the total participants (n = 1825), one half were living in public or private rented housing (48.6%) and 22.7% were waiting for public housing. Despite being the preferred form of housing, only 13.1% were living in their own home. One in 20 participants (5.2%) was currently homeless; 12.8% had been homeless in the previous 12 months. Residents of supported group accommodation felt safer in their locality than those in supported housing, but experienced less privacy and choice.
Conclusions:
Although fewer participants were homeless compared with the first Australian survey of psychosis, the proportion remains high. Housing difficulties are experienced by people with psychoses living in various accommodation and concern housing adequacy and safety as well as autonomy and choice. Access to public housing is restricted compared with the identified need. Since residents of supported group accommodation felt safer in their locality than those in supported housing, but experienced less privacy and choice, each supported housing model may offer different advantages to people with psychosis, and contribute to services that support and maintain recovery.
Introduction
According to article 11 of the International Covenant on Economic, Social and Cultural Rights (Office of the United Nations High Commissioner for Human Rights, 1976), everyone has the right to an adequate standard of living, including decent housing. Various factors are involved in deciding whether housing is adequate, including legal security of tenure, affordability, accessibility, habitability, location and cultural adequacy (Australian Human Rights Commission, 2011). In addition, as recovery from psychosis is multidimensional (Herrman and Harvey, 2005), many individual and environmental factors, including housing, affect the wellbeing of people living with severe mental illnesses (SMI), including psychoses (State Government of Victoria, 2011).
Research has increasingly demonstrated the therapeutic benefits of adequate supported housing to people with SMI (Sylvestre et al., 2007). Increased choice, control and quality of housing and the extent to which housing creates opportunities for people with psychoses to develop meaningful relationships in their dwellings and the community (community integration) are associated with decreased symptomatology, enhanced wellbeing and quality of life, and decreased service use (Nelson et al., 2007; Sylvestre et al., 2007). Few studies have considered the citizenship dimension of housing for people with psychosis; that is, whether housing supports their participation in broader systems such as programs, mental health systems and society more generally (Sylvestre et al., 2007). However, assisting people to live in accordance with their values and preferences, and promoting their social inclusion and citizenship is entirely consistent with a recovery-oriented approach to mental health care (Chopra et al., 2011; Commonwealth Government of Australia, 2009a; Slade, 2009; State Government of Victoria, 2011).
People with a psychotic illness have always lived in a range of accommodation, including with their families of origin in the family home. Although early developments in community-based mental health services included setting up group homes, hostels, and halfway houses (e.g. Thornicroft and Bebbington, 1989), housing for people with psychotic disorders did not become a priority until the deinstitutionalisation of mental health services occurred in many countries (Chopra et al., 2011). This led to the development of group housing with on-site support staff, often as part of a residential rehabilitation continuum in the community (Leff et al., 2009). Permanent, independent housing is usually positioned at the end point of this continuum (Henwood et al., 2011). Former long-stay patients experienced increased satisfaction and quality of life when moving to these forms of housing, although improvements in symptomatology and functioning were less consistent (Chopra et al., 2011; Hobbs et al., 2000; Leff and Trieman, 2000; Trauer et al., 2001). However, both here and overseas, concern has been expressed about the disruption to recovery and risk of reinstitutionalisation that may be experienced by some residents following discharge to alternative housing (Carling, 1993; Chopra and Herrman, 2011).
A concerning subgroup of people with psychotic disorders is either homeless or living in marginal accommodation (insecure housing with shared bathroom and kitchen and living space) (Chamberlain, 1999). Homelessness amongst people with psychotic disorders has been recognised for some time and is associated with substance use, poor physical health, social isolation and exclusion, disability, and poor access to effective treatment and rehabilitation (e.g. Scott, 1993). These problems are largely related to discontinuity of service provision (Chopra et al., 2011). Supported housing – that is, regular housing (i.e. available to the general population) coupled with separate in-reach flexible mental health support – has been developed, particularly for people with mental illness who are homeless or at risk of becoming homeless (Ridgway and Zipple, 1990; Tsemberis et al., 2004). Supported housing (commonly referred to as the Housing First model) can reduce homelessness and hospitalisation and enhance residential stability (Rog, 2004; Rosenheck et al., 2003; Tsemberis et al., 2004). Less consistent effects include symptom reduction and improved functioning, physical health and quality of life (Ridgway and Rapp, 1997). Not only is this housing and support model effective for homeless people with mental illness (Nelson et al., 2007), it is also more consistent with the preferences of most people with psychotic illnesses and with the recovery model, although living in supported housing may be associated with loneliness (Sylvestre et al., 2007). Nonetheless, supported housing is increasingly an integral component of mental health services.
Most research on housing models has been carried out in the USA, but there are similar findings in Australia (Chopra and Herrman, 2011; Hobbs et al., 2000; Trauer et al., 2001). Thus, homeless Australians with mental illness suffer from a high rate of physical and mental health problems and a shortage of accessible and appropriate housing and support services (Grigg et al., 2004; Mental Health Council of Australia, 2005).
The first Australian survey of psychosis, conducted in 1997–1998, reported high levels of persisting disability and needs amongst homeless people living with psychotic disorders (Herrman et al., 2004). Further, meaningful activity and the social needs of people with psychotic disorders living in group housing were often overlooked, according to this first national survey and other Australian research (Freeman et al., 2004; Harvey et al., 2002). Consequently, the first national survey concluded that there was a need for better access to public housing, flexible supports linked to accommodation, and a range of residential disability support services (Jablensky et al., 2000).
As deinstitutionalisation progressed around Australia, different programs have been developed that aim to provide a partnership between housing, disability and mental health service providers to enable people with psychosis to live in society with greater access to the full range of opportunities experienced by all Australians. From the mid-1990s, Australian state and territory governments have expanded these programs to keep pace with increasing need as more people with psychosis live in the community. The Housing And Support Initiative (HASI) in New South Wales (New South Wales Health, 2006), Psychiatric Disability Rehabilitation and Support Services (PDRSS) in Victoria (State Government of Victoria, 2003), Project 300 and Housing and Support Program (HASP) in Queensland (State of Queensland (Queensland Health), 2011), Independent Living Program (ILP) in Western Australia (Government of Western Australia, 2004) and Housing and Accommodation Support Partnership (HASP) program in South Australia (South Australia Health, 2010), represent some of these programs. They typically consist of home-based outreach support for people with severe mental illnesses and significant disability who are living in regular housing. Access to clinical mental health services is from Assertive Community Treatment (ACT) teams (Harvey et al., 2011) or a range of disability and recovery-based support services may be provided by the non-government sector. In 2008, the National Mental Health Policy was updated to reflect the changed service system, with greater emphasis placed on recovery as a core aim of mental health services and the stronger partnership needed for access to support and housing (Commonwealth Government of Australia, 2009a). Further, the federal government’s national approach to reducing homelessness (Commonwealth Government of Australia, 2008) included an expansion of the Personal Helpers and Mentors (PHaMs) program to assist people with a mental illness who are homeless or at risk of homelessness and a ‘no discharge into homelessness’ policy. The latter aims to ensure that appropriate accommodation and support plans are put in place before a person is discharged from psychiatric care. The National Affordable Housing Agreement (Commonwealth Government of Australia, 2009b) is tackling the provision of more affordable housing together with support for people with mental illness, and new social housing has been constructed under the current federal government’s National Building and Economic Stimulus Plan funding. Thus, the expansion of supported housing is one of the major changes in housing options for Australians with psychosis in the last decade and, like elsewhere (Carling, 1993), has led to increasing debate about the value of the alternative supported group accommodation model (Chopra et al., 2011).
A second national survey of psychosis was conducted in 2010. It was designed to cover a wider range of aspects of life than the aforementioned first survey. Within this second national survey, this study aimed to: (1) describe the proportions of people with psychosis living in different housing types, including the homeless and those living in marginal accommodation, together with their housing preferences and needs; (2) explore selected demographic and social inclusion correlates in relation to these housing types; and (3) compare two subgroups – participants living in supported group accommodation and supported housing (i.e. public or private rental accommodation with in-reach support) – with respect to key demographic, functional, clinical and social inclusion variables. This comparison is important because of recent increased availability of both types of housing and support in Australia. However, their relative advantages in this context have not been examined.
Materials and methods
Survey and participants
All participants took part in the Survey of High Impact Psychosis (SHIP). This second Australian national survey of psychosis covered seven catchment areas with a total area of 62,000 square kilometres and a population of 1.5 million people aged 18–64 years, approximately 10% of the Australian population in this age group. A two-phase design was used (Pickles et al., 1995). In Phase 1, screening for psychosis took place in public specialised mental health services and in non-government organisations supporting people with a mental illness. In Phase 2, people who screened positive for psychosis in Phase 1 were randomly selected, stratified by age group (18–34 years and 35–64 years), for interview and assessment. The census month was March 2010. Of 7955 people who were screen positive for psychosis and eligible, 1825 were interviewed in Phase 2. Data were collected on symptomatology, substance use, cognitive ability, functioning, disability, physical health, mental health service utilisation, medication use, education, employment and housing. The study was approved by institutional human research ethics committees at each of the seven study sites and all participants provided written, informed consent. Full details of the survey methodology are given in Morgan et al. (2011; 2012).
Measures and data handling
Within the second national survey of psychosis, data on current housing, changes of housing in the previous 12 months, housing preferences, needs and assistance, and housing-related social inclusion variables (e.g. accessibility of shops and public transport) were collected. Diagnoses were derived from the 10th edition of the International Classification of Disease (ICD-10) (World Health Organization, 2010).
Housing was categorised as: public rented house/unit/apartment (in Australia, public and private rented house/unit/apartment is typically independent accommodation; in-reach support may be provided, but this is allocated to the individual and not the accommodation); private rented house/unit/apartment (as before); family home; own house/unit (that is, owned by self or others and no rent paid); supported group accommodation (that is, group accommodation with on-site support staff including hostels, group homes, non-government organisation (NGO)-operated residences and clinical residential rehabilitation settings such as community care units; some group accommodation offers a permanent home – those that do not typically offer residential rehabilitation on a time-limited basis); homeless (primary, secondary or tertiary); institution (such as lodges or nursing homes) or hospital; other (including caravans or prison). Primary homelessness was defined as living on the streets, in parks, in deserted buildings; secondary homelessness was defined as living in temporary shelters such as refuges, emergency accommodation or sleeping on a friend’s couch; and tertiary homelessness was living in a boarding room (Chamberlain, 1999).
As people with psychosis are known to move in and out of homelessness, the survey collected detailed information on periods of homelessness in the 12 months prior to interview. Participants were asked about their housing over the previous 12 months as well as separately reporting any episodes of primary or secondary homelessness or residence in marginal housing.
In order to compare residents in supported group accommodation and supported housing, two subgroups were created. Supported group accommodation was defined as any group accommodation with on-site staff support. Supported housing was public or private rental accommodation combined with in-reach staff support, either in the form of ACT or home visits by an NGO at least weekly. We chose to exclude those living in their family or own home from the supported housing subgroup, since they were likely to differ with respect to other material and personal support available to them. Since the variable concerning housing type referred to current housing, whereas the support variables concerned support received in the preceding 12 months, participants were only selected for their respective subgroups if they had been resident in the appropriate housing type for the preceding 365 days. This had the added advantage of selecting only participants who had been stably accommodated in their respective housing in order that the comparison between these subgroups was more likely to reflect real differences between them. These two subgroups were compared on selected demographic and clinical variables, together with key variables (functioning, social inclusion and recovery) consistent with the literature (Sylvestre et al., 2007).
Descriptive statistics were employed, and subgroup comparisons were assessed using the chi-squared test or Student’s t-tests, as appropriate. All analyses were conducted with SPSS for Windows, version 19 (Chicago, IL: SPSS Inc., 2009)
Results
Demographic and diagnostic profile of participants
Of the 1825 participants with psychotic disorders, most were male (59.6 %), not currently partnered (82.9%), born in Australia (82.2%) and in the older group aged 35–64 years (57.6%). All participants met screening criteria for psychosis. The majority met ICD-10 research diagnostic criteria (World Health Organization, 2010) for schizophrenia (46.7%), schizoaffective disorder (16.1%) and bipolar affective disorder (17.5%). Further details on demography, diagnosis, course of illness and recent service usage of participants are provided in Morgan et al. (2011; 2012).
Current housing, housing preferences and satisfaction
Current and preferred housing of Australians living with psychosis who were interviewed in the second national survey are presented in Table 1. Comparing participants’ current and preferred accommodation types, the main discrepancies were: living in one’s own home or unit (which was the current form of housing for 13.1% compared with the preferred form of housing for 39.8%), living in a family residence (current housing for 19.1% and preferred housing for 10.4%), and living in supported group accommodation (current housing for 11.0% and preferred housing for 2.8%). Examining the number and proportion of those not currently living in a particular accommodation type but preferring to do so (column 3, Table 1), the largest discrepancy in numerical terms again concerned those participants who were not living in their own home or unit but expressed such a preference (n = 506). This examination also revealed that amongst the relatively small numbers preferring to be homeless (whether primary, secondary or tertiary; 44 participants), three-quarters was not currently homeless.
Current and preferred housing of Australians living with psychosis.
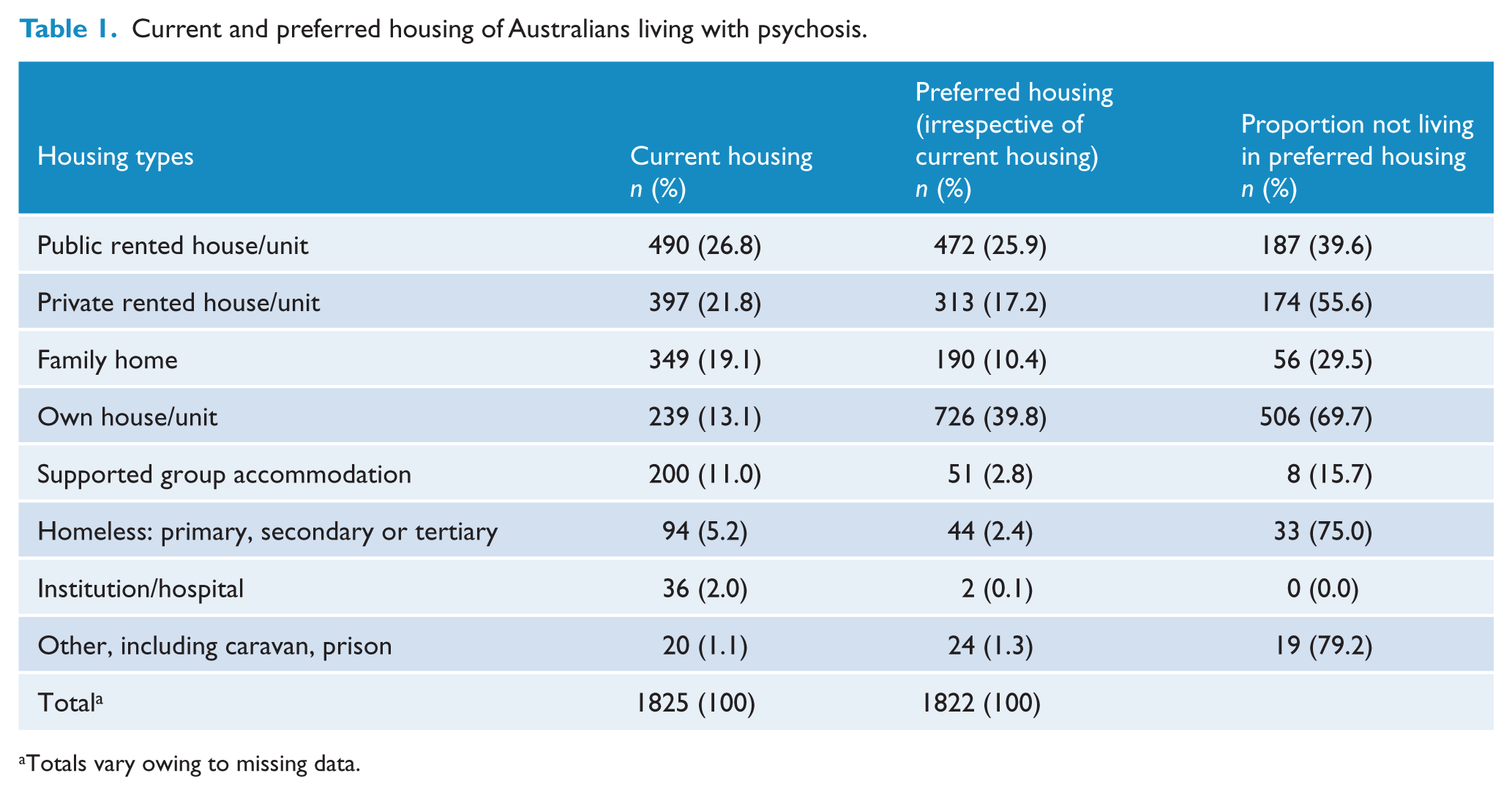
Totals vary owing to missing data.
Half the sample (52.6%) said they were very satisfied with their current living situation, with a further three in ten somewhat satisfied (28.4%); 8.3% were somewhat dissatisfied and 4.4% very dissatisfied. Significantly more of the ‘very dissatisfied’ group reported that they had no choice about their current residence (69.6% vs 28.9%, χ2 = 58.76, p < 0.001) and did not have their own room (15.5% vs 5.6%, χ2 = 9.62, p = 0.002) as compared with other participants. They were more often living in publicly rented accommodation (34.2%) or were homeless (16.5%). The major reasons cited for dissatisfaction with their current housing were a preference for living independently (24.1%) or unsatisfactory practical circumstances such as lack of safety due to crime or vandalism (15.2%), unsuitability (12.9%) or substandard conditions (12.5%) of their current accommodation.
Housing needs and assistance
A total of 414 participants (22.7%) were on a waiting list for public independent housing (see previous definition). Compared with the rest of the participants, a higher proportion of those waiting for public housing was either living in privately rented accommodation (28.3%) or supported group accommodation (16.4%), or were homeless (11.1%).
Just over one in five (21.9%) of participants reported receiving some assistance with their housing in the context of having moved house, such as acquiring and settling into their housing, in the previous 12 months. Of these, most (85.9%) reported their housing needs were adequately met. Only 41 individuals (2.2% of the total) expressed an unmet need for housing assistance. The majority of those identifying unmet housing needs were either living in privately rented accommodation (15 individuals, 36.6%) or were homeless (10 individuals, 24.4%).
Participants who had a psychiatric inpatient admission in the year prior to interview were asked if staff had talked to them about where they were going to stay on discharge. Over half (58.2%) recollected discussing accommodation options with staff at the time. Two-thirds (69.4%) reported not needing further help as they already had somewhere to live, 23.2% needed and received help finding accommodation, and 7.5% reported that they had not been given any help and had nowhere to live on discharge.
Homelessness and housing instability
At the time of interview, 5.2% of participants were homeless. Further, 12.8% had experienced at least one period of homelessness in the past year and a quarter (25.2%) had been fearful of homelessness in the previous year. On average, those who had been homeless reported 155 days of homelessness in the past year (SD = 141 days; median = 98 days). Eight individuals (3.4%) had been homeless for the entire year. The percentage of those experiencing homelessness was significantly higher for males than for females (15.4% vs 8.9%, χ2 = 16.27, p < 0.001), as was the mean days homeless (170 days vs 117 days, t = 2.66, df = 231, p = 0.008). Significantly more of those aged 18–34 years (16.4%) experienced a period of homelessness in the past year, compared with the older age group (35–64 years; 10.1%, χ2 = 16.15, p < 0.001). However, older participants were homeless for slightly (but not significantly) longer than those who were younger (mean of 167 days vs 146 days, respectively). As expected, participants who were never married were more likely to have experienced homelessness (15.0% vs 11.1% separated/divorced/widowed and 7.1% married/de facto, χ2 = 14.91, p = 0.001). There were no differences according to whether participants were born in Australia or not.
Concerning changes of accommodation, over a quarter of participants (27.4%) had changed accommodation at least once in the past year, not including admissions in and out of hospital; 3.7% of all participants moved twice and 6.7% moved three or more times. A range of reasons was identified by participants for moving out of stable accommodation in the past year. The most common main reason identified by participants was: conflict with parents/partner or housemates (19.6%); desire for independence or adventure (12.1%); own mental health problems (excluding anxiety or depression) (11.7%); non-renewal of lease or rental (10.9%); and financial troubles (6.3%). Almost 5% (4.6%) moved out of stable accommodation in the past year as a result of hospitalisation.
Comparison between residents in supported group accommodation and supported housing
One hundred participants were living in supported group accommodation and 98 were living in supported housing (regular housing with in-reach support) for the entire year prior to interview. In the latter subgroup, 53 participants received ACT and 54 were visited by an NGO case manager and saw their case manager at least weekly. Thus, nine participants in the supported housing group received both types of outreach support service.
Participants living in supported group accommodation and those living in supported housing were similar concerning proportions of Australian-born individuals (88.0% vs 83.7%, χ2 = 0.76, p = 0.38) and the younger group (aged 18–34 years) (30.0% vs 31.6%, χ2 = 0.06, p = 0.80). However, residents in supported group accommodation were more likely to be male (77.0% vs 45.9%, χ2 = 20.22, p < 0.001) and to have never married (78.0% vs 54.1%, χ2 = 17.94, p < 0.001) (Table 2).
Demographic and clinical characteristics of residents in supported group accommodation and supported housing.
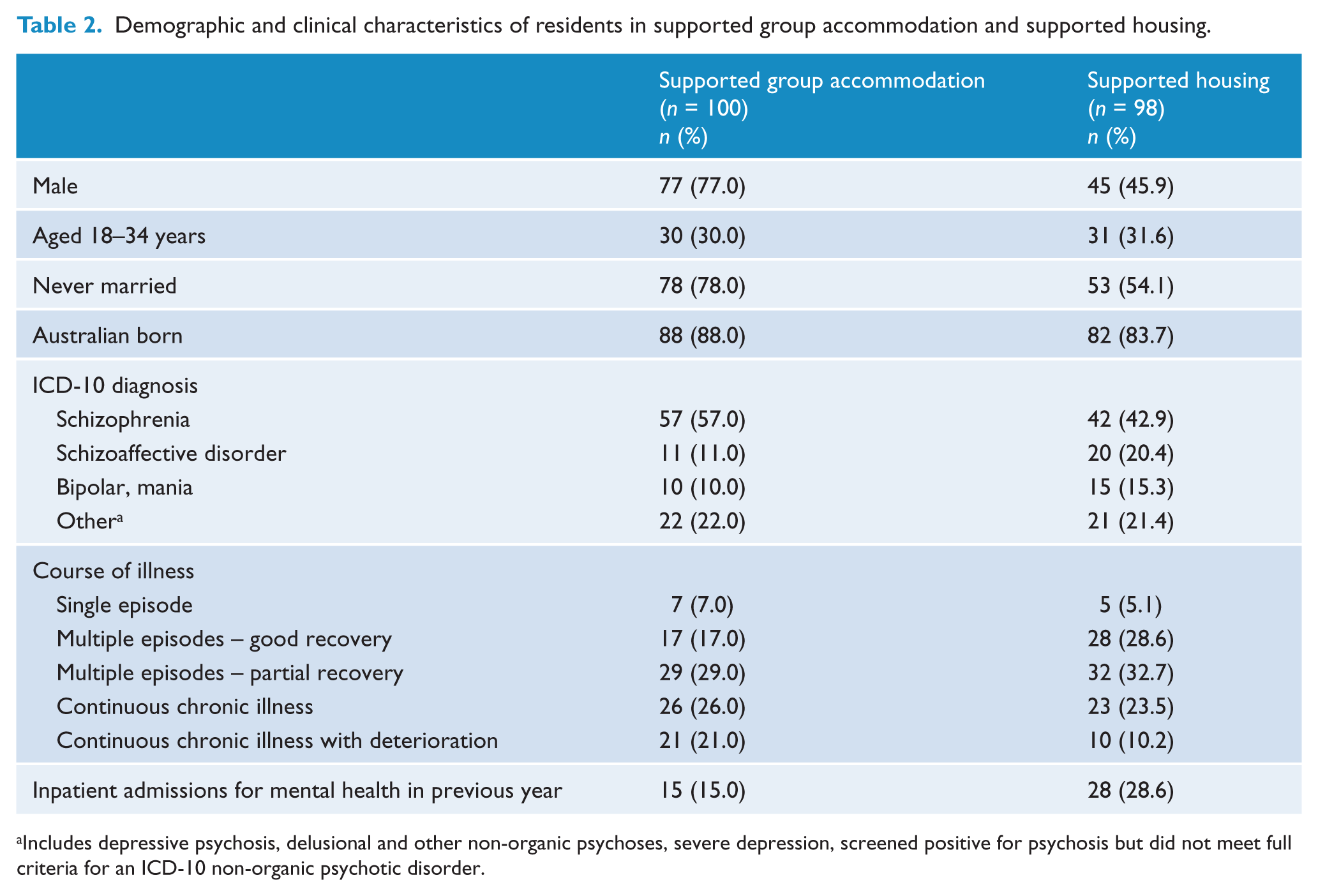
Includes depressive psychosis, delusional and other non-organic psychoses, severe depression, screened positive for psychosis but did not meet full criteria for an ICD-10 non-organic psychotic disorder.
Overall, participants in these two housing types did not vary significantly by diagnostic category (χ2 = 5.89, p = 0.12), duration (t = −1.92, p = 0.06) or course (χ2 = 7.24, p = 0.12) of illness (see Table 2). Nonetheless, more participants living in supported group accommodation were diagnosed with schizophrenia (57.0% vs 42.9%) and fewer with schizoaffective disorder (11.0% vs 20.4%) and bipolar affective disorder (10.0% vs 15.3%). On average, this subgroup also had longer illness duration (19.7 vs 16.9 years) and more participants with continuous chronic illness with deterioration (21.0% vs 10.2%) rather than multiple episodes with good inter-episode recovery (17.0% vs 28.6%). Fewer residents in supported group accommodation, however, had inpatient admissions for mental health in the previous year (15.0% vs 28.6%, χ2 = 5.36, p = 0.02).
Selected social functioning indicators were examined across the two subgroups. Those in supported group accommodation were significantly more disabled according to the Personal and Social Performance (PSP) scale (Morosini et al., 2000) (Table 3). There were 22.0% classified as having poor functioning sufficient to require intensive support and supervision, compared with only 6.1% in supported housing (Fisher’s exact test, χ2 = 13.23, p = 0.001). Residents of supported housing reported significantly greater frequency of face-to-face contact with family and other relatives (daily/almost daily: 41.2% vs 8.0%, χ2 = 31.67, p < 0.001), yet were rather more isolated and lonely (43.6% vs 34.3%, χ2 = 1.75, p = 0.186).
Comparison of residents in supported group accommodation and supported housing: social functioning, social inclusion and recovery indicators.
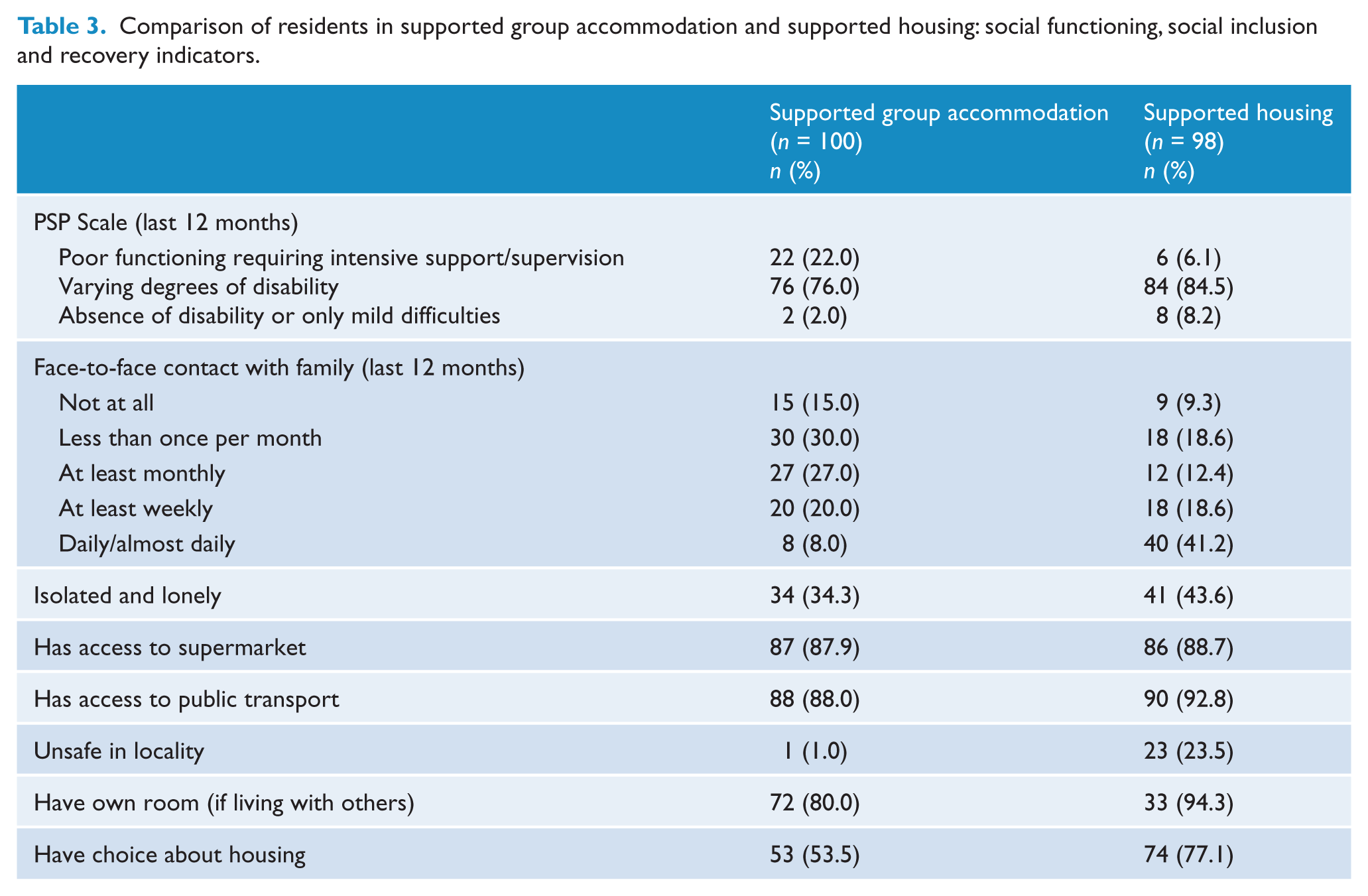
The two subgroups were compared on key social inclusion and recovery indicators related to their housing (Table 3). Whether in supported group accommodation or supported housing, most individuals had easy access to a supermarket (87.9% and 88.7%, respectively) and public transport (88.0% and 92.8%, respectively). However, more supported housing residents felt unsafe in their locality (23.5% vs 1.0%, χ2 = 22.74, p < 0.001). In contrast, fewer residents of supported group accommodation were likely to have their own room if living with others (80.0% vs 94.3%, χ2 = 3.83, p = 0.05) or reported having a choice about where they currently lived (53.5% vs 77.1%, χ2 = 11.90, p = 0.001). Finally, the majority in both supported housing and supported group accommodation preferred to live in rental accommodation (61.2% and 43.4%, respectively) or their own home (31.6% and 21.2%, respectively); however, one in four (25.3%) of those in supported group accommodation preferred to live there.
Discussion
Our key findings are that many Australians living with psychosis continue to experience homelessness, a mismatch between their actual and preferred form of housing and unaddressed housing needs. However, comparisons of those receiving services through state-run specialised mental health services in a given month have revealed important improvements in their housing circumstances since the first survey in 1997–1998 (see Jablensky et al., 1999, 2000; Morgan et al., 2011 for further details). These include an increased proportion of people living in rented accommodation (from 34.2% to 49.2%) and supported group housing (from 5.2% to 10.9%) and a drop in homelessness (from 13.0% to 5.0%) (Morgan et al., 2011; 2012). These welcome improvements are likely to be linked with mental health service delivery changes such as deinstitutionalisation, and the further development of community-based mental health services including treatment and support provided through ACT (Harvey et al., 2011) and disability and recovery-based support services provided by NGOs within people’s homes. They are also likely to have resulted from broader policy developments that have targeted homelessness and the increased provision of affordable housing and support services for people with severe mental illnesses, such as psychoses, so that they may gain and maintain housing (Commonwealth Government of Australia, 2008, 2009b).
Need is complex and difficult to adequately define and elicit. A particular strength of this second national survey was that various enquiries were made of participants concerning their housing needs. Notwithstanding the above positive findings, these revealed unaddressed housing issues. Further, our findings suggest that housing difficulties are experienced by people with psychoses living in a variety of accommodation types. As expected, the subgroup of participants who were very dissatisfied with their current living situation contained a higher proportion of the homeless, although those in publicly rented accommodation were also over-represented. In line with existing literature about beneficial housing features as well as consumer preferences (e.g. Sylvestre et al., 2007), underlying reasons concerned practical issues of housing adequacy and safety as well as preferences for greater choice, privacy and independence. Whilst access to ‘regular’ housing such as publicly rented property is broadly consistent with citizenship rights and a recovery-oriented approach to mental health (Chopra et al., 2011; Commonwealth Government of Australia, 2009a; Slade, 2009), our findings suggest that not all such accommodation can be defined as being of adequate quality. Further, although few of the participants (2.2%) expressed unmet needs for housing assistance, perhaps because housing needs may not be readily identified or expressed by this group, those who did express needs were predominantly homeless or living in privately rented housing. In addition, underscoring the complexity of expressed preferences and needs with regard to housing, only 10 (of 94) homeless participants expressed an unmet need for housing assistance and an additional 33 individuals were not homeless (however defined) but expressed such a preference. These data challenge the common assumption that no one wants to be homeless and suggest that some people with psychosis may prefer to live on the streets, in temporary shelters or in a boarding room rather than in some other types of accommodation. This finding warrants closer examination in future analyses. A plausible explanation may be perceived advantages with respect to greater independence compared with institutional and supported group accommodation, as identified within the first national survey (Harvey et al., 2002).
Almost one-quarter of all survey participants was on the public housing waiting list. This suggests that, whilst substantial progress has been made in improving the access of people living with psychoses to adequate housing, there is still more that could be done. In particular, considerably more investment is needed to meet unmet preferences for own housing as well as alternatives to institutional living and living in the family home. Availability of housing stock is a general issue (Grigg et al., 2004; Herrman et al., 2004). However, wider availability of, and access to, services offering housing assistance could be helpful (New South Wales Health, 2006). Only one in five survey participants were asked if they received these services if they had moved house in the previous 12 months, but most of these reported that their needs were adequately met. A particularly important gap is identified by the participants (7.5%) who reported that they had not been offered any help with accommodation when inpatients and yet had nowhere to live on discharge. This finding is concerning given the agreement by all states and territories to adopt a policy of ‘no discharge into homelessness’ as part of the National Affordable Housing Agreement (Commonwealth Government of Australia, 2008). With continuing pressure on inpatient beds and emergency departments and clear evidence that lack of appropriate and affordable supported accommodation is a significant contributor to length of stay (Zhang et al., 2011), it is imperative that the housing needs of inpatients are better addressed.
Although fewer participants were homeless compared with the first survey of Australians with psychosis, the proportion remains high and is a matter of public concern. Homelessness affects the lives of a substantial minority of people with psychoses, with one in eight having experienced homelessness and one in four fearful of this possibility. Our data also highlight the linked phenomenon of housing instability, which is more prevalent than in a comparable group of the general population (18.6% of those aged 15–64 years) (Australian Bureau of Statistics, 2007). Further, although homelessness is often considered an older person’s problem, our data underscore the importance of the growing recognition of youth homelessness (16.4% of participants aged 18–34 years in this survey) (e.g. Victorian Homelessness Strategy Ministerial Advisory Committee, 2001) and the corresponding need for youth-specific interventions (National Youth Commission, 2008). As a more general response to homelessness, the ACT model, and particularly the supported housing model (which similarly incorporates home-based support), have been shown to be effective (Rog, 2004; Rosenheck et al., 2003; Tsemberis et al., 2004) and could be made more widely available for people with psychoses who are homeless or at risk of homelessness. In addition, it may be useful for mental health services to identify and target ‘frequent movers’ for outreach interventions where available. Further, since moving out of stable accommodation was commonly precipitated by interpersonal conflict at home, wider availability of effective interventions to improve relationships with significant others, such as family interventions, is warranted (Pharaoh et al., 2006).
Our findings highlight that many people with psychosis experience a mismatch between their housing preference and their current living situation. From a rights perspective, this suggests that the development of a full range of services is needed to adequately address this disparity. This would also be consistent with existing evidence concerning the therapeutic value of attending to housing choice (e.g. Sylvestre et al., 2007) as part of the recovery paradigm (Commonwealth Government of Australia, 2009a). However, as suggested by Sylvestre et al., further work is required to understand how programs and policies can be re-modelled to adequately address choice, take appropriate account of factors such as diminished expectations and adaptation among people with psychosis (Herrman et al., 2002), titrate support to changing needs, and balance the best interests of the individual and community.
Supported housing is not only an effective intervention for homelessness, but also has wider benefits for people with psychoses (Nelson et al., 2007; Sylvestre et al., 2007). These have led to growing adoption of this model both in Australia and overseas. This study compared two participant subgroups within the national survey with different types of housing and support: supported group accommodation and supported housing (regular housing with in-reach support). The subgroups resembled each other with respect to diagnosis and course of illness, although there was a tendency for greater disability among those in supported group accommodation that was also reflected in their social functioning ratings. This may be a selection effect due to residential assignments being matched with applicants’ characteristics (Wong and Solomon, 2002) and cannot be used to draw conclusions about the relative effectiveness of the models. Key differences emerged between the two subgroups with respect to social inclusion and recovery indicators that are consistent with the literature (Leff et al., 2009; Sylvestre et al., 2007). Whilst supported housing appears more consistent with recovery-oriented practice, it may exact a cost in the increased likelihood that participants feel unsafe in their locality as well as more isolated and lonely, despite greater contact with relatives. Conversely, the opportunity to live in housing of choice is still an unmet need for a greater proportion of those in supported group accommodation. Given that recovery is a complex and individualised process (Slade, 2009), it may be better to view these two models as complementary, rather than one leading to or replacing the other. Whilst not as overtly consistent with recovery values, there is evidence that supported group accommodation can support people’s recovery and may be required to maintain this recovery (Chopra and Herrman, 2011). Without sufficient diversity of housing types available to support and maintain recovery, and sufficient flexibility of policy and practice, some of the most disadvantaged groups among those living with psychosis will become or remain socially isolated, and more rather than less disabled, over time.
Limitations
The survey method was likely to underestimate the homeless with psychosis. This is because they are less often in contact with services and were not specifically targeted for this survey (Harvey et al., 2002; Herrman et al., 2004). The survey was cross-sectional and so cannot be used to draw conclusions about effectiveness of housing models. There was relatively little data collected on neighbourhood characteristics in this survey – despite growing recognition of the importance of neighbourhood characteristics in relation to housing outcomes and satisfaction. The limitations of satisfaction data in this population are also noted given the possibility of diminished expectations or adaptive preferences. Some of the variables used to inform the subgroup comparison may have been imprecisely rated: for example, ACT is a complex service model which is difficult to define briefly in the context of a lengthy survey interview and may have been poorly understood by participants. In addition, this survey did not collect data on model fidelity of ACT and other outreach support and the extent and content of NGO outreach support provided to participants was unknown. Finally, although the subgroups were restricted to participants residing for the previous year in the relevant housing in order to select well-defined and stable subgroups, participants could have spent brief unaccounted-for periods of time elsewhere, such as in transitional accommodation or respite. Further, this approach may have introduced selection bias due to differential rates of housing tenure in these two housing models.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethics approvals for the study were obtained from the relevant institutional human research ethics committees.
This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
The study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.