
Abstract
Keywords
Fundamentals
The relationship between borderline personality disorder and bipolar affective disorder has been a topic of debate since at least 1979 (Boyce and Wilson, 2011; Siever and Gunderson, 1979; Stone, 1979). The presumed associations have been multiplied by increasing interest in patients who suffer less severe forms of mania but still suffer significant affective instability (the bipolar spectrum disorders) (Benazzi, 2009; Howland and Thase, 1993; Kwapil et al., 2011; Perugi et al., 2011; Thomas, 2004; Tiller and Schweitzer, 2010; Van Meter et al., 2011; Youngstrom et al., 2010). While such interest has captured recent attention, the concept of bipolar disorder with relatively mild forms of mania is not a recent development (Baethge et al., 2003; Brieger and Marneros, 1997; Slater and Roth, 1969). Our current major diagnostic systems have added to the confusion with long lists of criteria for each of these diagnostic groups, which permit the inclusion of a wide range of clinical presentations (Meares et al., 2011a). While bipolar disorder has been recognised as a diagnostic entity for a very long time (at least since Aretaeus of Cappadocia, circa AD 150–200) (Adams, 1972; Hornblower and Spawforth, 1996), borderline personality disorder as currently defined is a relatively more recent construct (Stern, 1938).
The problem of misdiagnosis of bipolar disorder has been well recognised and is the subject of considerable comment (Benazzi, 2000, 2006, 2008; Boyce and Wilson, 2011; Chilakamarri et al., 2011; George et al., 2003; Little and Richardson, 2010; Paris, 2010; Paris et al., 2007; Patfield, 2011; Ruggero et al., 2010a, 2010b; Smith et al., 2004; Tiller and Schweitzer, 2010; Yatham et al., 2009). One can readily appreciate that, among patients, a diagnosis of bipolar disorder gives a sense of optimism that treatment for their distressing illness is available. Conversely, in the context of our current service structure, a diagnosis of borderline personality disorder carries greater stigma and the implication that treatment may be unavailable (Aviram et al., 2006). A more biological diagnosis also externalises the locus of control, which is of appeal to some patients and therapists.
Nevertheless, bipolar disorder is both frequently over-diagnosed and frequently missed (Hadjipavlou and Yatham, 2009; Leboyer and Kupfer, 2010). Evidence is steadily accumulating that bipolar disorder is associated with significant risks to brain structure and function, making early and effective treatment particularly important (Berk et al., 2009, 2010a, 2010b, 2011; Macneil et al., 2011). On the other hand, the positive misdiagnosis of bipolar disorder brings significant potential adverse consequences, including inappropriate medication exposure, insurance complications, employment implications, stigma and a distorted perception of health status.
The failure to diagnose borderline personality disorder also has significant potential adverse consequences, as targeted psychotherapy and psychosocial management have proven efficacy. In the context of several shared elements, the complex phenomenological differences between the two disorders will emerge with greater clarity as they are examined in this paper (Berk et al., 2004).
It would seem helpful to begin by reflecting upon what might be considered the ‘core’ elements of each group of disorders. Meares et al. (2011a) used factor analysis to define four core elements for borderline personality disorder: ‘painful incoherence’ (highly intense emotional pain reflecting a fragmented sense of self; the most significant factor); ‘role absorption’ (loss of identity); ‘inconsistency’; and ‘lack of commitment’ (the least significant factor) (Meares et al., 2011a). Although other significant features of borderline personality disorder such as a fear of abandonment, impulsivity, recurrent self-injurious behaviour, affective instability (rapidly fluctuating moods provoked by life events), episodic explosive rage and episodic psychotic phenomena were clearly significant, they were not regarded as ‘core’ features. Previous factor analyses identified disturbed relatedness (identity disturbance, chronic perceptions of internal emptiness, unstable relationships), behavioural dysregulation (self-injurious behaviour, impulsivity) and affective dysregulation (inappropriate anger, efforts to avoid abandonment, affective instability) as the three prime features of borderline personality disorder (Clifton and Pilkonis, 2007). Significantly, Clifton and Pilkonis (2007) established that these latter factors correlated so highly together that they statistically reflected one comprehensive construct. It would be helpful to identify that construct in a clinically meaningful way.
Like Meares et al. (2011a), I suggest that an ‘emotionally noxious sense of self” (an emotionally painful disruption of self-identity, a recurring fear of abandonment and chronic emptiness) is that core entity. Zanarini et al. (2007) argue for a similar concept, and also suggest that the interaction of this core element with a ‘kindling’ life event converts this predisposition into a clinical syndrome. However, Trull et al. (2011), in their discussion of the proposed diagnostic criteria for DSM-V, maintain that there is no single ‘latent’ group identity for borderline personality disorder and therefore a categorical diagnostic structure is unsatisfactory. Instead, they argue for a combination of the dimensions of clinical signs and symptoms derived from factor analyses, combined with the core features of affective dysregulation, impulsivity, and interpersonal hypersensitivity. This seems consistent with the notion of a fundamental core element of a noxious sense of self.
Young et al. (2003), and Kellogg and Young (2006), have formulated the core elements of borderline personality disorder using a schema-based model. They describe these core schema elements as five modes which reflect the impact of childhood traumatic experiences: (1) ‘the abandoned and abused child’: fear of isolation and abandonment; (2) ‘the angry and impulsive child’: rage over perceived abuse, deprivation, rejection, subjugation and punishment; (3) ‘the detached protector’: emotional withdrawal, disconnection, isolation and behavioural avoidance; (4) ‘the punitive parent’: identification with a devaluing and rejecting parent; and (5) ‘the healthy adult mode’: the least common mode which allows the patient to meet essential needs and to seek containment of the recurring emotional pain. Their formulation is largely consistent with those described above, although they do not place emphasis upon self-observation and evaluation. However, their model has the added value of constructing a framework for a cognitive approach to psychotherapy.
Bipolar disorder would seem to have a very different nature when the fundamental features of this disorder are considered. These consist of elements of depressive disorder (dysphoric mood, anhedonia, psychomotor disorder) and elements of mania (unusually and significantly increased energy evident in several forms, impaired judgement with disinhibition, unusually elevated or irritable mood), with subjective experiences linked to these elements (emotional emptiness, irrational guilt, suicidal thoughts, grandiose thoughts, elevated or depressed mood, increased creativity or impaired cognitive function, and a number of other features) (Hosokawa et al., 2009; Parker, 2000, 2009; Parker et al., 2006). Importantly, disruption of a sense of self and an incapacity to maintain mutually satisfying relationships with others are not core features of bipolar disorder. As a consequence, the approach to effective psychotherapy for bipolar disorder is different to that for borderline personality disorder (Basco and Rush, 2005; Goodwin and Jamison, 2007d; Kellogg and Young, 2006; Linehan, 1993).
Matters of difference
Mania and hypomania in various ways define bipolarity, but some uncertainty arises when the milder forms of mania, such as those seen in cyclothymia, are considered (Akiskal and Benazzi, 2006; Alloy et al., 2011; Diagnostic and Statistical Manual of Mental Disorders, 2000; Goodwin and Jamison, 2007e; International Classification of Mental and Behaviour Disorders, 1994; Phelps, 2009; Smith et al., 2005).
Perugi et al. (2011) report evidence of cyclothymic temperament in patients diagnosed with bipolar disorder, borderline personality disorder and atypical major depressive disorder, although their criteria for cyclothymia were not clearly defined (Perugi et al., 2011). Further, they did not separate cyclothymia as a syndrome from cyclothymic temperament as an element of personality. Ghaemi et al. (2004) maintain that cyclical patterns of mood shifts are a common element of bipolar disorder, recurrent major depressive disorder and atypical major depressive disorder, but that atypical depressive features and early onset are more common in bipolar disorder. The absence of mania in major depressive disorder and atypical major depressive disorder would seem critically important, despite the cyclical nature of their symptom profiles. As noted previously, a family history of major mood disorders helps to reinforce the diagnosis of a bipolar disorder (Galione and Zimmerman, 2010; Ghaemi et al., 2004; Mitchell et al., 2008; Souery et al., 2012), and the life trajectories of disabling symptoms of bipolar disorder tend to be more prolonged than with borderline personality disorder (Paris, 2004; Paris et al., 2007). However, both disorders are associated with a significant incidence of childhood trauma (approximately 50% in bipolar disorder and 60–80% in borderline personality disorder) (Alvarez et al., 2011; Ball and Links, 2009; Conus et al., 2010; Etain et al., 2008; Fowke et al., 2011; Garno et al., 2005; Herman et al., 1989; Hyun et al., 2000), and early life trauma may play an aetiological role in both (Holmes, 2003; Joyce et al., 2003; Watson et al., 2006). Patients with bipolar disorders and borderline personality disorders may differ in the form of childhood trauma, or their vulnerability to such trauma, but the possible details of such differences remain uncertain.
Mackinnon and Pies (2006) offer support for the notion that rapid cycling of mood states is a common element of both bipolar and borderline states. The suggestion has some clinical support but appears inconsistent with the non-affective components, as well as the details of affective disruptions discussed later, observed in both disorders.
Self-mutilation has been observed with similar frequency in both bipolar disorder, particularly mixed states (Joyce et al., 2010), and borderline personality disorder. Therefore, such self-injury does not distinguish these disorders diagnostically. The separation of bipolar disorder and borderline personality disorder must then be achieved with criteria other than the presence of affective dysregulation and cyclicity of symptoms and signs alone. Importantly, however, the time course of the cyclicity is helpful: the presence of discrete, prolonged periods of affective symptoms, as opposed to rapidly shifting states, does suggest a bipolar diagnosis.
Differences have also been identified in thinking styles between bipolar and borderline patients, with implications for their emotional health and relationship quality. Wupperman et al. (2009) identified significant deficiencies in mindfulness (attention, awareness and acceptance of the moment) in patients with borderline personality disorder. These included reduced interpersonal effectiveness, as well as passive and impulsive emotion regulation, even when they controlled for neuroticism. Nilsson et al. (2010), using the Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire, and the Young Schema Questionnaire, found that bipolar patients exhibited a higher level of maladaptive schemas and affective temperaments compared with controls. In contrast, borderline patients exhibited a higher level of cyclothymic temperament and reduced self-control.
Quantitative clinical studies
There have been numerous attempts to quantify the similarities and differences between bipolar disorder and borderline personality disorder, as well as their comorbidity (Paris et al., 2007). Perugi et al. (2011) studied a population of patients diagnosed with atypical major depressive disorder, 32% of whom they subsequently found could be diagnosed with bipolar disorder (24% without antidepressant-induced bipolarity and increased to 78% if hyperthymia or cyclothymic temperaments were considered indicative of bipolarity). When these atypically depressed patients were divided into those who also suffered from borderline personality disorder (42%), the only significant differences in demographic and a range of clinical features were shorter durations of the current illness and a higher rate of suicide attempts. The presence of bipolar features, however, defined in their study, did not identify comorbid borderline personality disorder in these atypical major depressive disorder patients.
Galione and Zimmerman (2010) examined the clinical features of patients suffering depressive disorders (unipolar and bipolar), both with and without comorbid borderline personality disorder. They found the following differences when depressive disorders were comorbid with borderline personality disorder: earlier age of onset of depressive symptoms, greater frequency of depressive episodes, greater frequency of ‘atypical’ depressive symptoms, higher prevalence of comorbid anxiety disorders and substance abuse, and a greater number of suicide attempts. They also found that a history of bipolar disorder in first-degree relatives was not significantly associated with the presence of borderline personality disorder. They concluded that overall their data did not support the inclusion of borderline personality disorder as a component of the bipolar spectrum.
On the other hand, it is interesting that Mitchell et al. (2008) found that the probability of a depressive disorder being part of a bipolar disorder was increased by the presence of features of atypical major depressive disorder, an earlier age of onset of first depressive episode, a history of multiple and shorter depressive episodes, and/or a family history of bipolar disorder. While there is overlap in their findings with the probability of borderline personality disorder being present, the family history of bipolar disorder is again a prominent distinguishing feature.
Paris et al. (2007), in their review of the bipolar disorder/borderline personality disorder interface, also concluded that bipolar disorder and borderline personality disorder were most likely separate disorders. Specifically, they found that while episodes of mania in bipolar disorder contrasted with more affective instability in borderline personality disorder, there was a significantly higher frequency of bipolar disorder in first-degree relatives of bipolar disorder patients, the benefits of mood stabilizers were more predictable in bipolar disorder than borderline personality disorder, and the prognosis for borderline personality disorder was generally better than for bipolar disorder. They also reviewed the relative incidence of borderline personality disorder and bipolar disorder comorbidity in several studies (Paris et al., 2007). They record that after combining the data, the median incidence of bipolar disorder-I in patients with borderline personality disorder was 9%. Similarly, the median incidence of bipolar disorder-II in patients with borderline personality disorder was 11%. Cyclothymia was identified in 22% of patients with borderline personality disorder, but only one study was cited (Levitt et al., 1990). Conversely, borderline personality disorder was identified in 11% of patients with bipolar disorder-I and 16% of those with bipolar disorder-II. Perugi et al. (2003) found borderline personality disorder in 62% of patients with atypical major depressive disorder and cyclothymic temperament. These low rates of overlap argue in favour of the disorders being discrete entities.
Henry et al. (2001) found that while affective instability was evident in both bipolar disorder and borderline personality disorder, there were important differences. Significantly, the instability seen in bipolar disorder was more often between euthymia and depression, euthymia and elation, or depression and elation. In contrast, the lability seen in borderline personality disorder was more often between euthymia and anger. Indeed, there is an increasing consensus that the high ranking of irritability in the DSM-IV criteria for bipolar disorder is a problem, and this is likely to be amended in the DSM-V system (Ghaemi et al., 2008). Benazzi (2006), using a measure of personality factors, found borderline personality traits were significantly more common in bipolar disorder-II than in major depressive disorder. However, while the ‘affective instability’ factor did not separate bipolar disorder and borderline personality disorder, the ‘impulsivity’ factor was significantly more common in borderline personality disorder compared with bipolar disorder. Other personality disorders were also identified in patients with bipolar disorder, with histrionic personality disorder being the most common co-morbid subtype.
Yen et al. (2002) found that in women with borderline personality disorder, the level of affect intensity and affect control were significantly associated with the number of borderline traits. Both affect intensity (raised) and affect control (reduced) remained significant in association, even when controlled for depression. Affect control remained significant, even when controlled for affect intensity.
Reich et al. (2011) found several significant differences in affective lability between bipolar and borderline disorders. Bipolar patients exhibited higher scores on the Euthymia-Elation subscale of the Affective Lability Scale (ALS), as well as higher total scores using the Affect Intensity Measure. The latter scale also revealed higher Positive Emotion subscale scores in this group. In contrast, borderline personality disorder patients scored more highly on the Anxiety-Depression subscale of the ALS. They also found that, using the Affective Lability Interview for Borderline Personality Disorder Scale, borderline patients exhibited more frequent shifts between euthymia and anxiety, anger and depression, as well as depression and anxiety.
Becerra is currently conducting the first known study measuring emotional dysregulation using the Difficulties with Emotion Regulation Scale in patients with bipolar disorder. His preliminary data reveal a current mean score of 90 (maximum possible = 180) (Becerra R, 2011, unpublished data). This can be compared to a mean score of 126 in patients with borderline personality disorder (Gratz et al., 2006) and a mean of 80 in college students (Gratz and Roemer, 2004). While sufficient data is not yet available to permit a statistical analysis, the trend is toward a difference in scores between bipolar and borderline patients.
Altamura et al. (2011) reported lower rates of comorbidity of bipolar disorder and borderline personality disorder than, for example, of panic disorder, substance abuse and attention deficit hyperactivity disorder. Similarly, comorbidity of both disorders has been identified with atypical major depressive disorder and major depressive disorder. A family history of bipolar disorder tends to be more prominent in patients with bipolar disorder than borderline personality disorder. While affective dysregulation can be identified in both disorders, there appear to be qualitative as well as quantitative differences. Finally, similar forms of cognitive deficits can be identified in both disorders, but the severity tends to be greater in bipolar disorder.
Subtypes of bipolar disorder
The current DSM-IV and ICD-10 descriptions of criteria for bipolar disorder-I, bipolar disorder-II, and cyclothymia (with the added variants of mixed affective episodes, rapid cycling, psychotic affective symptoms and schizoaffective disorder), contain essentially the same criteria for manic and depressed episodes, separated only by severity and duration of episodes. This is a clumsy and largely meaningless exercise, in which arbitrary criteria of duration are cited and severity remains a subjective evaluation by the observer. Only the variants of mixed affective episodes, rapid cycling and affective psychosis can be said to have further objectivity, and even then the frequency of episodes to identify ‘rapid cycling’ is itself arbitrary. Indeed, the decision to admit to a hospital, with all its significant non-clinical variables, is regarded by many as an inappropriate criterion for separating bipolar disorder-I from bipolar disorder-II (Akiskal and Benazzi, 2006). The presence of affective psychosis is not even given its own separate subtype in current classifications, although clinically these bipolar disorder-I patients suffer from a particularly destructive illness and there may be significant differences in the nature of this form of bipolar disorder.
Cyclothymia is a useful, valid, but heterogeneous clinical entity (Akiskal and Benazzi, 2006; Akiskal et al., 2000; Howland and Thase, 1993). While cyclothymia can be considered a personality trait or temperament, it can also be defined as a form of bipolar disorder (DSM-IV and ICD-10). It is usefully considered as a disorder which includes a range of bipolar signs and symptoms (Phelps, 2009), but the manic features are of a severity which is only spontaneously evident to ‘significant others’ (such as family or friends), and often evident to the patient only through reflection. While many observers may notice various emotional, cognitive and behavioural features consistent with bipolar disorders, they will frequently consider these to be personality traits, and not recognise their significantly disabling quality. This may rely on a less than precise definition of ‘significant others’, but it carries at least some objectivity.
Patients rarely present with well-manicured illness syndromes and the interplay of significant bipolar features and numerous other disorders is considerable. In clinical practice, cyclothymia is diagnosed largely by historical review, collateral information from family and friends, current observation and self-report. Many patients suffering from cyclothymia are not spontaneously aware that their experience of pressured thoughts, fluctuating moods, bursts of expansive thinking, periods of heightened libido and significant fluctuations in sleeping habits, for example, are components of an illness. Yet these patients are usually well aware of the adverse consequences of their disorder, and are often perplexed by their own behaviour and internal experiences.
The intrusion of personality disorders (defined by the persistence of major disruption of the experience of self and interpersonal relationships), and a variety of other psychological disorders (such as anxiety disorders, eating disorders, attention deficit disorders and substance abuse), only obfuscate our understanding of bipolarity if included under the umbrella of bipolar spectrum disorders. It is more parsimonious to consider these as comorbid disorders, rather than forme frustes of bipolar disorders.
Neuropsychological studies
Neuropsychological studies have revealed deficits in cognitive function in both borderline personality disorder and euthymic bipolar disorder. The most prominent common features are defects in verbal learning and memory, and subtle impairment of executive functions have also been identified in both borderline personality disorder and bipolar disorder (Kurtz and Gerraty, 2009; Ruocco, 2005). However, Mann-Wrobel et al. (2011) report that the cognitive changes in bipolar disorder tend to be ‘generalized’ (evident in more brain regions) and potentially involve any cognitive functions. The precise deficits are modified by numerous illness and age-related factors. Only ‘crystallized’ verbal functions appeared relatively spared in their analysis. The severity of deficits from all of these studies tends to be greater in bipolar disorders and less generalized in borderline personality disorder (Kurtz and Gerraty, 2009; Ruocco, 2005).
Genetics
In 2000, Torgersen et al. (2000) reported a twin study of personality disorders, in which borderline personality disorder was revealed to be associated with a level of heritability of 0.7 (or 70%), consistent with measures of heritability in other personality disorders in that study. However, in 2008, he and his colleagues (Torgersen et al., 2008) reported a study of cluster B personality disorders, revealing a measure of heritability for borderline personality disorder traits of 0.35 (35%). Heritability in borderline personality disorder has been variously found in a number of studies to be between 0.35 and 0.8 (Torgersen et al., 2000, 2008). Kendler et al. (2011) also found significantly heritable personality traits in a large genetic study of personality disorders in general. Heritability in bipolar disorder has been estimated to be between 0.68 and 0.80 (Goodwin and Jamison, 2007a).
Familial coaggregation of borderline personality disorder and bipolar disorder has been identified, but similar coaggregation has been identified with other mood disorders (major depressive disorder and atypical major depressive disorder) as well as anxiety disorders, somatoform disorders and substance abuse (Zanarini et al., 2009). More rigorous measures of genetic linkage between bipolar disorders and borderline personality disorder have not yet been employed. The serotonin transporter gene ‘short’ polymorphism has been found to be significantly associated with both borderline personality disorder (Maurex et al., 2010; Wagner et al., 2009) and bipolar disorder (Daray et al., 2010; Levinson, 2006), but the associations are not strong. Joyce et al. (2006) found a significant association between the 9-repeat allele of the DAT1 dopamine transporter gene and borderline personality disorder. This association persisted when relevant developmental factors (childhood abuse or neglect, borderline temperament) were controlled. The association was larger in older patients, suggesting a possibly greater significance in ‘poorer prognosis’ patients. Nemoda et al. (2010) present similar evidence of an association between dopamine transporter polymorphisms and borderline personality disorder. However, dopamine transporter polymorphisms appear significant in bipolar disorders as well (Pinsonneault et al., 2011). The similarities and differences remain uncertain.
Neurobiology
While reduced suppression of corticotrophic releasing hormone production by dexamethasone (using the Dexamethasone Suppression Test) has been well observed in depressive disorders (unipolar and bipolar), increased suppression has been observed in borderline personality disorder (Carrasco et al., 2007; Goodman et al., 2010; Zimmerman and Choi-Kain, 2009). Post-traumatic stress disorder has also been associated with increased suppression, but the presence or absence of this disorder did not alter the findings in these studies. There may be a similar reduction in blunting of the suppression of thyrotropin-releasing hormone (thyroliberin) production by thyroxine in borderline personality disorder (Carrasco et al., 2007). Decreased serotonergic responsivity and increased cholinergic responsivity have been observed in borderline personality disorder and major depressive disorder, with suggestions that a similar pattern may be the case in bipolar disorder (Goodman et al., 2010).
Sleep architecture in borderline personality disorder is associated with a longer duration of rapid eye movement sleep, less slow-wave sleep and more stage 2 sleep than in major depressive disorder or healthy controls (De La Fuente et al., 2001, 2004). Similar disruptions of sleep architecture have been observed in bipolar disorder (Goodwin and Jamison, 2007e; Srinivasan et al., 2009), but more detailed research is required to clarify the similarities and differences which may be present in these two groups of disorders.
Hallahan et al. (2011) performed a very thorough mega-analysis of morphometric MRI studies in bipolar disorder and found evidence of increases in the volumes of the right lateral ventricle, left temporal lobe and right putamen, while a reduced size of right and left amygdalae and hippocampi have been observed in borderline personality disorder (Nunes et al., 2009). Previous studies in bipolar disorders found inconsistent evidence of changes in the volumes of the third ventricle, subgenual prefrontal cortex, hippocampal/amygdala complex, thalamus and caudate (Mcdonald et al., 2004). There is some evidence that adolescent females with borderline personality disorder may have reductions in dorsolateral prefrontal cortex and orbitofrontal gray matter, but the separation from healthy adolescent subjects is uncertain (Brunner et al., 2010).
Disruption of white matter integrity has been the subject of attention, with abnormalities detected in the internal capsules and adjacent areas of the striatum, thalamus and frontal white matter in bipolar spectrum disorders (Haznedar et al., 2005). Benedetti et al. (2011) found structural white matter injury in the pathways between the amygdala and a variety of regions, including the cingulate gyri (subgenual, anterior and posterior), the parahippocampal gyri, the orbitofrontal cortex and the dorsolateral prefrontal cortex, in patients with bipolar disorder. Of further interest, disruption of white matter integrity has been detected in the internal capsules and left temporal regions of unaffected first-degree relatives of patients with bipolar disorder (Sprooten et al., 2011). Altered white matter integrity in the inferior frontal lobes has also been described in females with borderline personality disorder and a history of self-injury (Grant et al., 2007). The significance and consistency of white matter changes are uncertain and await further clarification in both bipolar and borderline personality disorders.
Bandelow et al. (2010) suggest that many features of borderline personality disorder could potentially be explained as consequences of endogenous opioid dysfunction. These features include attention-seeking behaviours, over-activation of reward pathways with fear of abandonment, anhedonia and subjective emptiness as consequences of endogenous opioid deprivation and self-injury as an attempt to activate endogenous opioid function. They argue that the benefits of opioid receptor antagonists for self-injurious behaviour is supportive of their hypothesis. Unfortunately, the supportive evidence appears scant and confirmation of their hypothesis is lacking at this time.
Vollm et al. (2004) found that, using a Go/No Go task in borderline personality disorder and antisocial personality disorder patients, metabolic activation measured by Functional Magnetic Resonance Imaging (fMRI) was distributed across the medial, superior and inferior frontal gyri extending to the anterior cingulate. This contrasted with healthy controls whose activation was mainly limited to the prefrontal cortex. Schulze et al. (2011) used fMRI to examine differences in metabolic activity associated with emotional reactivity in female patients with borderline personality disorder and healthy controls during a delayed reappraisal paradigm using aversive pictures and cognitive reappraisal strategies. They found that borderline personality disorder patients exhibited enhanced emotional reactivity as well as deficits in voluntarily reducing aversive emotions by cognitive reappraisal.
Reviews by Mauchnik and Schmahl (2010) for borderline personality disorder, and Kupferschmidt and Zakzanis (2011), as well as Chen et al. (2011) for bipolar disorders, examined the neuroimaging research for both of these disorders. They note reports of reduced hippocampal and corpus callosum size in both borderline and bipolar patients, increased size of the amygdala in borderline patients, but inconsistent reports of alteration in the size of the amygdala in bipolar patients. In addition, they report reduced size of gray matter in the rostral and ventral regions of the anterior cingulate gyri in borderline patients, but no consistent reports of change in the anterior cingulate size of bipolar patients. Amygdala activity (measured by fMRI or Positron Emission Tomography scans) was reported to be increased in both borderline and bipolar patients, while hippocampal activity has been variously altered in bipolar patients. Activity of the anterior cingulate gyri and insular cortices were reportedly increased in borderline patients, but the reports of altered activity in these regions in bipolar patients have not been consistent. The reported failure of the activity of the insular cortices to increase when under emotional stress in borderline patients is of interest given their difficulty regulating emotional responses to such challenges. Bipolar patients have been reported to show reduced activity in the dorsolateral prefrontal cortices, the dorsomedial prefrontal cortices, the orbitofrontal cortices, the inferior frontal cortices and in the cuneus as well as lingual gyri. These changes in activity are of interest, given the evidence of fronto-limbic dysregulation and dorsoventral dysregulation in bipolar patients. The precise nature of morphological and metabolic changes in the brains of patients with bipolar and borderline personality disorders remains clouded by clinical heterogeneity, variations in technical assessment and the complexity of the neurobiology in these disorders.
The physiological response to facially expressed emotion, as measured by cerebral blood flow, has been studied in both bipolar disorder and borderline personality disorder. The findings reveal complex variations related to the nature of the expressed emotion, but possible differences between bipolar disorder and borderline personality disorder were difficult to define (Minzenberg et al., 2007; Wessa and Linke, 2009).
Meares et al. (2011b) report neurophysiological evidence of reduced inhibitory activity in the right hemisphere from fronto-medial structures in borderline personality disorder. However, similar defects in evoked potentials have been observed in bipolar disorder and schizophrenia, and may represent a marker of a broad neurophysiological dysfunction (Bestelmeyer et al., 2009). Indeed, one of the difficulties of biological markers in general is their broad failure to respect our current diagnostic systems. This is not really a surprise, since in no other branch of medicine does phenomenology accurately reflect pathophysiology. Importantly, however, all of these studies have provided further evidence of fronto-limbic dysregulation in both bipolar disorder and borderline personality disorder, compared with healthy controls.
The finding that the sensitivity of glucocorticoid receptors is reduced in bipolar disorder and increased in borderline personality disorder is of considerable interest, as it suggests a major separation in the neuroendocrine response to stress (Goodwin and Jamison, 2007c; Zimmerman and Choi-Kain, 2009). There is also some evidence that there may be reduced responsivity in serotonergic and acetylcholinergic circuits in both disorders. Altered function of endogenous opioid systems is a tempting hypothesis for some features of borderline personality disorder but is poorly supported. Dysregulation of neural circuits in the prefrontal regions, with disruption of some executive cognitive functions and reduced modulation by fronto-limbic pathways, appears supported in borderline personality disorder and in bipolar disorder (Berdahl, 2010). The differences in both structural and functional activity of neural circuits in both disorders remain uncertain, but exhibit similarities to changes in mental state and interpersonal functions.
Andreazza et al. (2010) and Berk et al. (2011) note the significance of mitochondrial dysfunction in bipolar disorders, with likely relevance to the disruption of energy evident in the clinical states of these disorders. There are no reports of mitochondrial dysfunction in borderline personality disorders.
Pharmacology
It is evident that antidepressants, anticonvulsant-mood stabilizers and atypical antipsychotic medications have value in the management of both bipolar disorder and borderline personality disorder. However, the benefits in bipolar disorder appear significantly more prominent than in borderline personality disorder, and their use in the latter remains limited (Ripoll et al., 2011). Given the broad utility of antidepressants, antipsychotics and anticonvulsants across a wide range of disorders, treatment response does not appear to have diagnostic implications. The only exception appears to be lithium, which does not show efficacy in non-affective psychoses nor display clear utility in personality disorders (Bellino et al., 2008).
Clinical observations
Clinical observation and documentation by many clinicians suggest that borderline personality disorder is associated with an emotionally painful disruption of the sense of self, as well as rapidly changing affective instability, high impulsivity and a pattern of severely unsatisfactory interpersonal relationships (Meares et al., 2011a, 2011b; Paris et al., 2007). Bipolar disorder is much less commonly associated with such disruption of self-experience, and is less often associated with high impulsivity and repeatedly unsatisfactory relationships. Patients with bipolar disorder are more often observed to have a positive family history of bipolar disorder, and their experience of affective instability is characterised by less rapid changes and less reactivity to environmental events than patients with borderline personality disorder.
Psychosis can arise in both bipolar disorder and borderline personality disorder. The form of psychosis in bipolar disorder is most frequently mood congruent, but mood incongruent psychotic phenomena can arise. The psychotic episodes are almost always limited in duration and rarely extend beyond several months (Goodwin and Jamison, 2007b). The content of the psychotic episodes is usually dominated by delusional thinking, but a variety of perceptual disorders are common and severe disorganisation (delirious mania and catatonia) may develop (Goodwin and Jamison, 2007b). Psychotic phenomena in borderline personality disorder are less consistent in content, may be linked to early life trauma, and may persist for many years. However, severe psychotic disorganization is rare and usually very brief (mainly hours) (Adams and Sanders, 2011; Barnow et al., 2010).
Acute psychiatric illness of many forms can test underlying personality structures, and the temporary emergence of behaviours suggestive of underlying personality disorder is common. During episodes of acute illness, patients with bipolar disorder (particularly mixed states) sometimes exhibit prominent affective instability, high impulsivity, self-injury, manipulative interpersonal behaviour and explosive rage. This may lead to an incorrect diagnosis of borderline personality disorder. Tiller has named this phenomenon ‘state borderline’ (Tiller J, 2002, personal communication). Longitudinal observation of the patient through historical assessment and personal observation by therapists is vitally important for accurate diagnosis. These observations chime with experience.
Conclusions
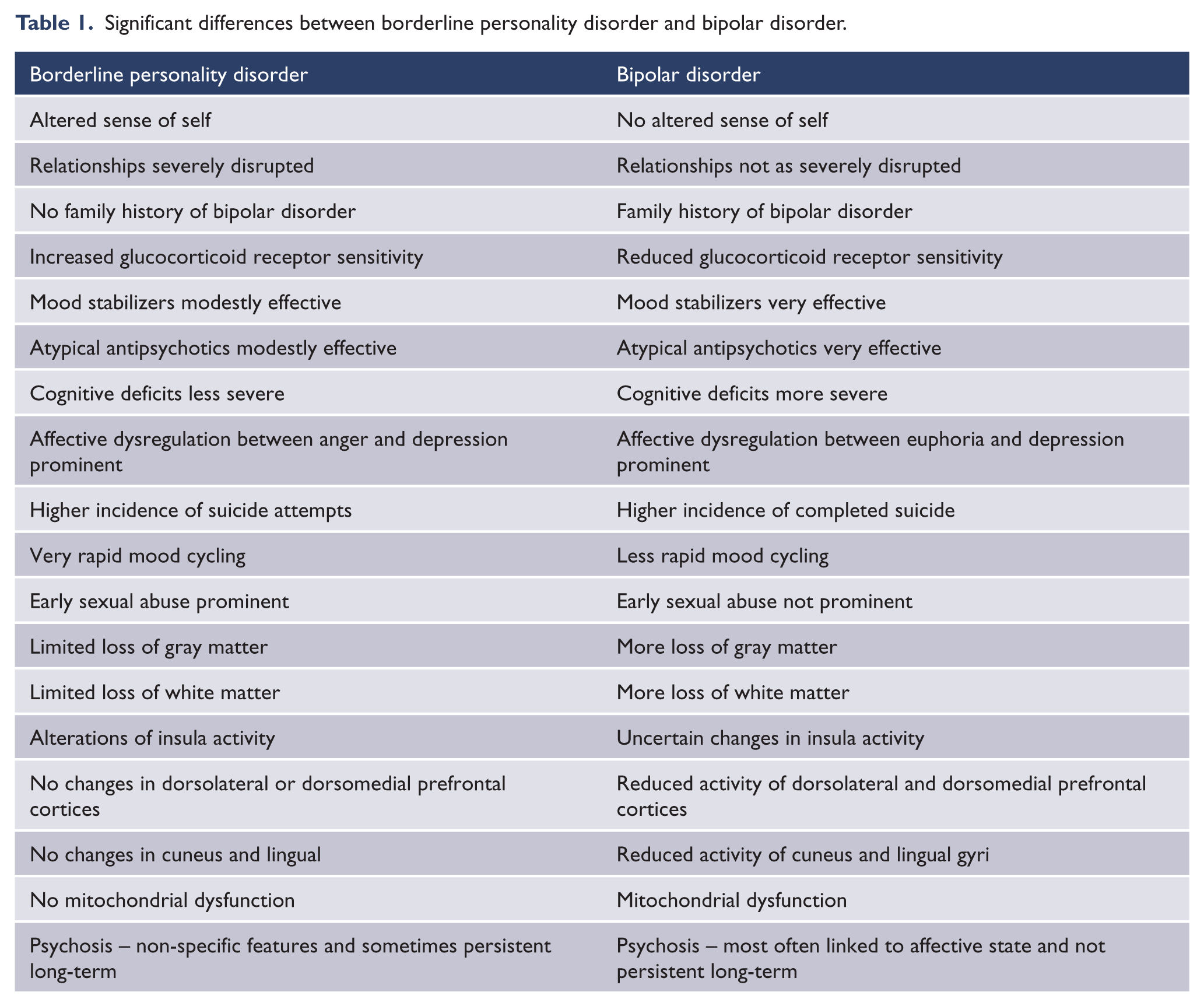
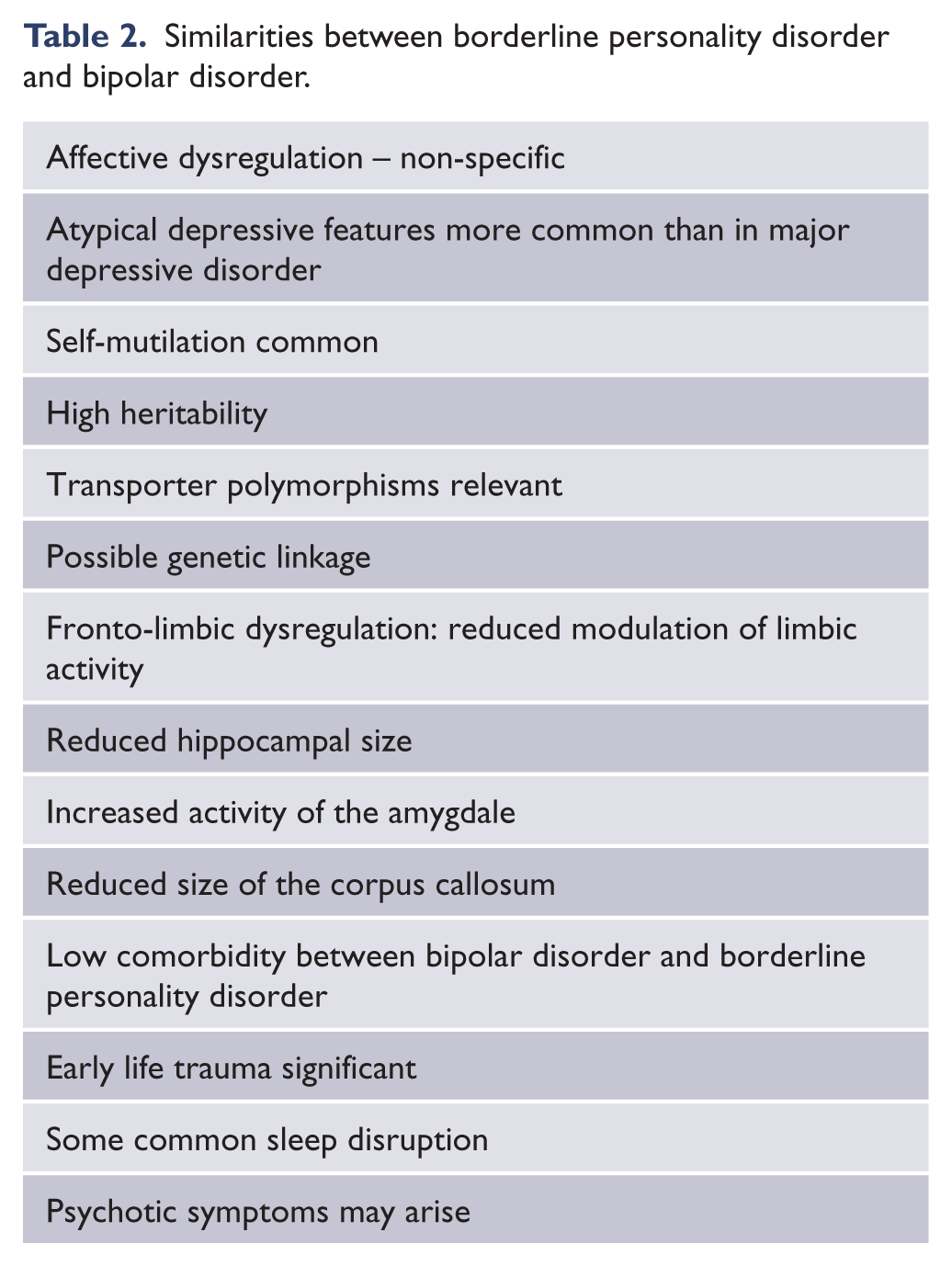
While bipolar disorder and borderline personality disorder have many clinical and biological features in common, the evidence suggests that they remain essentially distinct entities which may occur together or separately (see Tables 1 and 2). They share some elements of psychopathology and pathophysiology, but their differences are more significant.
Significant differences between borderline personality disorder and bipolar disorder.
Similarities between borderline personality disorder and bipolar disorder.
Footnotes
Acknowledgements
I am indebted to several colleagues, who have given very generously of their time and expertise to critically comment upon the preparation of this paper. Professors Michael Berk and Sean Hood have been of considerable assistance. My good friends Drs Robert Segal and Nick de Felice have also provided invaluable comment. Dr Sherylee Bassett has given expert advice, assisted generously with literature searches, provided professional editing and tireless devotion to the quality of presentation. Their contributions are gratefully acknowledged.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.