
Abstract
Keywords
Traditional estimates of the lifetime prevalence of bipolar disorder have usually been approximately 1–2% [1]. Typically these estimates have included only bipolar I and bipolar II disorders as currently defined by DSM-IV. Although controversial [2], there is substantive interest in broadening the spectrum of bipolar disorders beyond that defined as bipolar I or bipolar II [3]. In Europe Angst has reported prevalence rates of 8.3% for a broader bipolar spectrum [4], while a re-analysis of the USA Epidemiological Catchment Area database reported a 1.3% lifetime prevalence for bipolar I and II disorders, but an additional 5.1% reported subsyndromal manic symptoms [5]. One of the key contributors to this broadening of the bipolar spectrum appears to be the duration criteria for a manic episode, which has traditionally been set at 1 week. Angst reported that brief recurrent hypomania was validated by family history of mood disorders, a history of suicide attempts and treatment for depression [4]. Judd and Akiskal reported that the subsyndromal bipolar subjects had higher rates of suicide attempts and of adverse psychosocial outcomes [5].
Despite the clinical and epidemiological interest in broadening the bipolar spectrum, there is a paucity of data on the characteristics of subjects within this newly recognized bipolar spectrum. In DSM-IV, most of these subjects would be diagnosed as having bipolar disorder not otherwise specified (BDNOS).
In the present paper, using data from a family study on the molecular genetics of depression and personality, we examine whether BDNOS is more similar to bipolar I and II disorders or to major depressive disorder as regards clinical features, suicide attempt histories, personality traits and disorders, and axis I comorbidity.
Methods
Subjects
Probands were recruited from a wide variety of sources mainly by advertising in newspapers and on the radio. To be eligible for inclusion the proband must have received treatment for a major depressive episode, and be willing to participate in a family study on the molecular genetics of depression and personality. Bipolar disorder was not specifically mentioned in any of the recruiting/advertising material. Exclusion criteria were age <18 years, and not having first-degree biological relatives who would also participate in the research study.
The study was designed to obtain trios. Whenever possible we preferred to obtain consent from the proband's two parents, but if one or more parents were not available we recruited siblings in lieu of parents.
The study was approved by the Canterbury (New Zealand) Ethics Committee.
Screening
Probands or family members who had seen advertisements would usually make initial contact with interviewers/research assistants by telephone. Over the telephone the nature of the study was explained, a proband treated for depression within the family was identified, and the availability of proband and family members was confirmed. Potentially suitable probands and family members would then be sent more detailed information sheets about the study. If the proband and family members consented to participate, subjects would be offered the options of being interviewed in their home or within the university department conducting the study.
Questionnaires
Prior to, or following, the interviews and obtaining a blood sample for DNA extraction, all probands and family members completed two self-report questionnaires. This included a 240-item, 5-point Likert scale version of the Temperament and Character Inventory (TCI) to assess the four temperament measures and three character measures, inclusive of subscales, in Cloninger's psychobiological model of personality [6]. The other questionnaire was the General Behaviour Inventory (GBI), which assesses depressive, manic and biphasic mood swings [7].
Interviews
All consenting subjects were interviewed by trained interviewers/research assistants who had degrees in psychology. All interviews were reviewed by a psychiatrist (PRJ) and DSM-IV diagnosis were assigned. If the interview yielded insufficient information to enable confidence about diagnoses, we would utilize further information obtained from family members or, with consent, from medical records. The interview was based upon the Mini-International Neuropsychiatric Interview (MINI) [8], but with expansions in the areas of alcohol and drug dependence and bipolar disorder. Of particular relevance to this paper were the adaptations for bipolar disorder. If after the MINI probe for a history of mania or hypomania subjects had not screened positive, they were then asked the questions in the Mood Disorder Questionnaire (MDQ) [9]. If subjects affirmed three or more manic symptoms occurring at the same time, they were then asked about the nature of these manic episodes according to the MINI diagnostic criteria including duration, impairment, hospitalization and psychosis. Considerable care was taken to enquire about the longest duration of manic episodes and age of onset. BDNOS required a history of major depressive episode(s) plus two or more 1–3 day manic episodes without hospitalization, psychosis or impairment.
After the completion of the interview for Axis I disorders, subjects were then screened for personality traits and associated difficulties related to these traits. The first screener consisted of 12 questions. For each trait a subject was asked whether they would consider themselves to be not at all (score = 0), somewhat (score = 1) or very much (score = 2) a perfectionist, conscientious, stubborn (obsessive–compulsive screener); a loner, content without friends, didn't care what others thought about them (schizoid screener); a worrier, shy or unconfident (avoidant screener); or impulsive, easily angered or having unstable and erratic relationships (borderline screener). These questions had been derived from earlier research on the structure of personality disorder symptoms [10]. If they identified traits as being present they were then asked whether these had caused difficulties for them.
Subjects were then asked, in a similar format, 20 questions about their affective temperament [11]. Following these screening questions the interviewer followed up any potentially positive personality disorder traits by completing the Structured Clinical Interview for DSM Personality Disorders (SCID-II) [12].
Analyses
All data from interviews and questionnaires were entered into a relational database and then transferred to SYSTAT for statistical analysis. For the purposes of the present paper we were interested only in probands or family members who received a consensus diagnosis of BDNOS, bipolar I or II disorder, or major depressive disorder.
These three groups were then compared using χ2 tests for categorical variables or analysis of variance with post-hoc Tukey tests for continuous variables. Because the sample consisted of 197 unrelated probands and 200 first-degree relatives with mood disorders, statistical analyses did not adjust for potential family clustering effects because they would be minimal.
Results
The subjects consisted of 197 probands (77% female), 81 mothers of the proband, 28 fathers, 60 sisters and 31 brothers; all of whom were diagnosed as having suffered from a lifetime major depressive disorder, BDNOS or bipolar I or II disorder. The mean ages of the probands was 38.2±12.4 years, mothers 59.4±10.7 years, fathers 59.2±10.1 years, sisters 38.4±11.0 years, and brothers 41.8±12.6 years. Of the 297 subjects with lifetime major depression, 80% had recurrent episodes, and 139 were probands. Of the 75 subjects with bipolar I or II disorder, 45 were probands. Of the 25 subjects with BDNOS, 13 were probands.
From Table 1, which compares the BDNOS subjects with the bipolar I or II disorder and major depressive disorder subjects, it can be seen that the BDNOS subjects are marginally younger than the subjects in the other two diagnostic groups but are comparable in relationship to gender, likelihood of ever receiving treatment, likelihood of being in a current episode of depression, and age of onset. However, the three diagnostic groups differ by history of suicide attempts, self-mutilation and ever having had an episode of melancholic depression or psychotic depression. In all these instances the bipolar I/II group has the highest rates with the BDNOS being intermediate, but usually closer to the depressed group.
Subject details
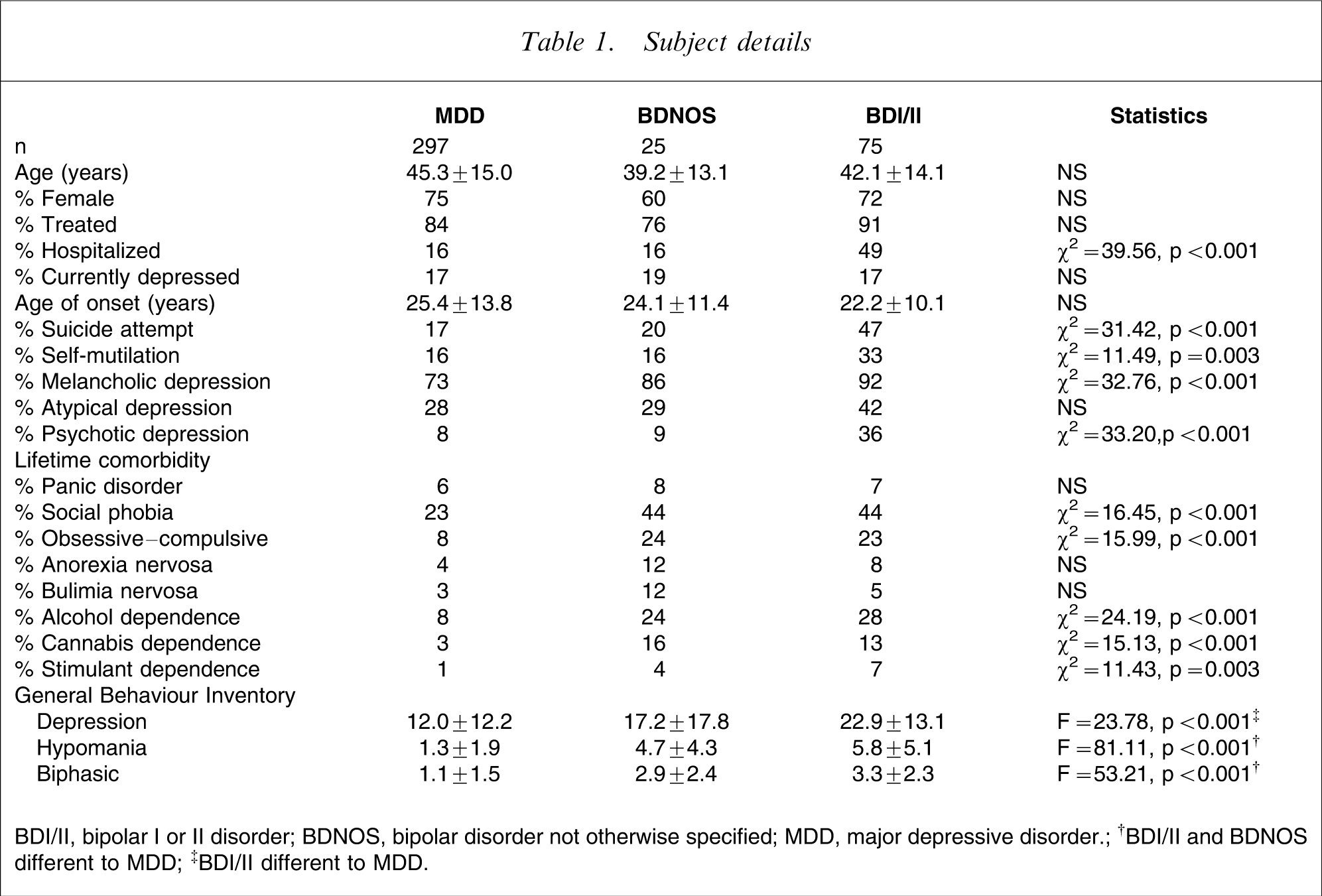
BDI/II, bipolar I or II disorder; BDNOS, bipolar disorder not otherwise specified; MDD, major depressive disorder.
†BDI/II and BDNOS different to MDD
‡BDI/II different to MDD.
In comparing rates of comorbidity across the three diagnostic groups it can be seen that there are significant differences with respect to social phobia, obsessive–compulsive disorder, alcohol dependence, cannabis dependence and stimulant dependence. In most instances the BDNOS group is comparable to the bipolar I/II group, and with higher rates of comorbidity than the major depression group. For stimulant dependence the BDNOS group is intermediate between the major depression and bipolar I/II groups.
Table 2 compares the three diagnostic groups on personality screening questions, personality disorder symptoms, personality disorder diagnoses and on temperament and character. While the three diagnostic groups did not differ on six of 12 personality traits, the bipolar I/II and BDNOS groups scored higher on the scales of being a loner and being impulsive. The bipolar I/II group scored higher on being content without friends, easily angered and having unstable and erratic relationships, with the BDNOS group intermediate. The bipolar I/II group scored higher on being socially unconfident.
Personality traits and disorders
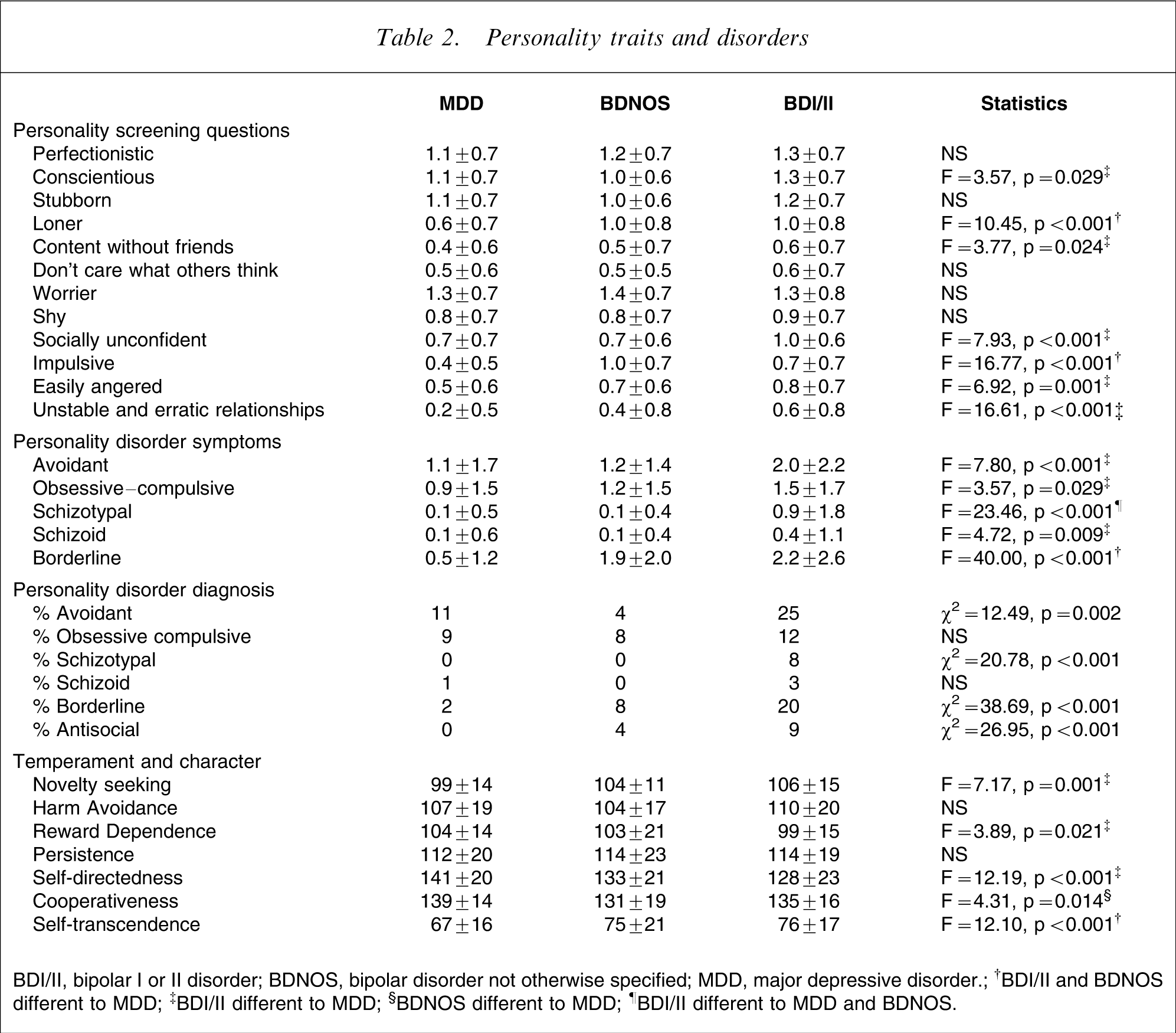
BDI/II, bipolar I or II disorder; BDNOS, bipolar disorder not otherwise specified; MDD, major depressive disorder.
†BDI/II and BDNOS different to MDD; ‡BDI/II different to MDD; §BDNOS different to MDD; ¶BDI/II different to MDD and BDNOS.
The bipolar I/II group were assessed as having more avoidant, obsessive–compulsive schizoid and schizotypal personality disorder symptoms, while both the BDNOS and bipolar I/II groups had more borderline personality disorder symptoms. The bipolar I/II group had the highest rates of all personality disorders, but with regard to borderline and antisocial personality disorders the BDNOS group were clearly intermediate between the other two diagnostic groups.
On self-reported temperament and character the bipolar I/II group had higher novelty seeking, lower reward dependence and lower self-directedness. The BDNOS group had the lowest cooperativeness. Interestingly both the BDNOS and bipolar I/II groups had higher self-transcendence than the MDD group.
Discussion
In the present paper, in which we have compared personality and clinical characteristics of subjects with BDNOS to those with bipolar I/II disorder or major depression, we have shown that BDNOS is often different to major depression and more akin to bipolar I/II disorder. These data add further evidence for broadening the bipolar spectrum to include BDNOS, which in this paper was defined as recurrent 1–3 day hypomanias.
Before discussing the personality findings it is relevant to discuss the clinical and comorbidity differences between the three mood disorder diagnostic groups. On clinical features the bipolar I/II subjects differed from those with major depression, with the BDNOS subjects intermediate but generally closer to the major depression subjects. Significant ways in which bipolar I/II were different from major depression included a higher likelihood of ever having been hospitalized, higher rates of suicide attempts and self-mutilation, and higher rates of psychotic depressive episodes. The present findings as regards high rates of psychotic depression in bipolar I/II disorder are consistent with many other studies [13–15]. However, BDNOS did not show the same high rate of psychotic depression. The high rate of suicide attempts in the bipolar I/II subjects is consistent with many other studies [16, 17]. The high rates of self-mutilation in the bipolar I/II subjects may be a surprise to some readers but it has previously been reported [18]. Although self-mutilation has likely genetic, developmental and personality correlates [19], mixed mood states may also be an important risk factor for self-harm [20].
Although with regard to clinical differences the BDNOS subjects were more similar to major depression than bipolar I/II, for comorbidity BDNOS tended to be similar to bipolar I/II, especially as regards anxiety and substance dependence comorbidity. Both BDNOS and bipolar I/II subjects had higher rates of social phobia and obsessive–compulsive disorder. Issues of the comorbidity of anxiety disorders with bipolar disorder have been previously reviewed [21], and there are suggestions that a broadly defined cyclothymia has considerable potential to enhance our understanding of obsessive–compulsive disorder [22]. The high rates of alcohol, cannabis and stimulant dependence in both BDNOS and bipolar I/II subjects are consistent with other studies in bipolar I/II disorder [23], and extend this comorbidity finding into the broader bipolar spectrum.
In relation to personality disorders, the bipolar I/II group had higher rates of avoidant and schizotypal personality disorders than the depressed or BDNOS groups. The high rate of avoidant personality disorder in bipolar I/II disorder is not consistent with other studies, in which avoidant personality disorder is either more common in unipolar depression [24] or not different [25]. The increased rate of schizotypal personality disorder in bipolar I/II disorder has been previously noted, and in major depression the presence of schizotypal traits predicts the later development of bipolar disorder [26]. The bipolar I/II group also had higher rates of avoidant and schizotypal personality disorder symptoms.
For borderline personality disorder there is a stepwise increase in the rate of borderline personality disorder from major depression to BDNOS to bipolar I/II disorder. For borderline personality disorder symptoms both bipolar I/II and BDNOS subjects have higher rates. The 20% prevalence of borderline personality disorder in bipolar I/II disorder is consistent with other studies [24–26]. The rate of 2% for borderline personality disorder in those with major depression is lower than in studies recruiting currently depressed patients [27, 28], which typically may find approximately 10%. However, the depressed subjects in the present study were approximately 10 years older and <20% were currently in a depressive episode. Both of these factors reduce the rate of borderline personality disorder, which may be less stable than traditionally believed [29]. The overlap between bipolar disorder and borderline personality disorder is well recognized, although the interpretation of the importance of this comorbidity is controversial [30]. The elevated rate of borderline symptomatology in BDNOS, compared with major depression, suggests that even brief 1–3 day hypomanias may increase the risk of borderline personality disorder.
On the personality screening questions it is of note that the BDNOS subjects were most likely to endorse themselves as impulsive and scored non-significantly higher than the bipolar I/II subjects, and significantly higher than the major depression subjects. For the personality screening questions on being angry and having unstable and erratic relationship, the BDNOS subjects were intermediate.
On Cloninger's temperament and character inventory the BDNOS subjects were between the bipolar I/II and major depression subjects on elevated novelty seeking, lower reward dependence and lower self-directedness. For co-cooperativeness the BDNOS subjects had the lowest score, which was significantly lower than those with major depression. Perhaps most interestingly, both the BDNOS and bipolar I/II subjects scored significantly higher on self transcendence than the major depression subjects. High self-transcendence, especially if combined with low self-directedness and co-cooperativeness, is associated with schizotypal traits [31, 32]. Although the BDNOS subjects did not have the increased rate of psychotic depressive episodes and of schizotypal personality disorder seen in the bipolar I/II subjects, the higher self-transcendence score in the BDNOS subjects suggests that they share some of the psychosis-prone characteristics of the bipolar I/II subjects.
The present findings, which provide some support for BDNOS being included as part of a broader bipolar spectrum, need to be considered in relationship to the strengths and limitations of the present study. A first critical issue is that we have compared three groups of subjects, all with mood disorders, on the basis of their reported history of hypomania or mania. The BDNOS group reported a history of hypomanic symptoms for 1–3 days, compared to the bipolar I/II subjects who had hypomanic/manic symptoms of ≥4 days, or the major depression subjects who reported no history of hypomanic symptoms. Any single interview by trained interviewers, but without extensive clinical experience, will have limitations even though the interviewers were closely supervised and trained by a psychiatrist (PRJ) with a long history of interest in bipolar disorder [26, 33–35]. In obtaining a history of hypomania the interviewers did not limit their enquiries to the traditional probe questions about elevated, expansive or irritable mood as used in the MINI and other structured interviews, because when subjects denied the probe questions they were then asked all the questions of the MDQ. Indeed eight (of 25) BDNOS subjects and six (of 75) bipolar I/II subjects denied the mania probe questions but affirmed items on the MDQ, and on further questioning were considered to have experienced hypomanic episodes. Even with this additional approach to eliciting a history of hypomania it is likely that there was still have some underreporting of hypomania, because single interviews may have low sensitivity but satisfactory specificity [36]. It is reassuring that the BDNOS subjects, like the bipolar I/II subjects, scored significantly higher on the hypomanic and biphasic scales of the GBI. Because the interviewers were blind to the results of the questionnaires, these data provide further evidence for the bipolarity diagnosis of the present BDNOS group.
A second limitation could possibly include the method of sampling, which was by advertising. This may be a reason for the high percentage of female subjects across all diagnostic groups. Because we used trio sampling this also restricts subjects to those with living and accessible first-degree relatives, but also means that subjects are not strictly independent. However, because the sample consisted of 197 probands, and usually three from any family, clustering is extremely unlikely to account for any of the findings.
A third limitation is the assessment of personality traits and disorders. One issue of relevance is the mood state of subjects when they were assessed, but >80% of subjects across all three diagnostic groups were not considered to be suffering from a current mood episode when interviewed. This may account for a somewhat lower rate of personality disorder in the depressed group compared to clinical studies, which assess for personality disorders when subjects are in current mood episodes. A second issue is that trained interviewers, not clinicians, administered the SCID-II interview. Furthermore, we did not use the self-report SCID-PQ screener, but developed a new personality trait screener in which every subject was asked about traits relevant to key personality disorders. We consider that this is an equally rigorous introduction to the SCID-II interview, and any methodological weaknesses would not explain differences between the three diagnostic groups.
In summary, we have compared BDNOS subjects, defined by a history of depression plus 1–3 day hypomanias, with subjects who reported just major depression or traditionally defined bipolar I/II disorder. In a number of aspects related to personality features and comorbidity the BDNOS subjects share features with the bipolar I/II subjects and differ from those with major depression. This supports broadening the bipolar spectrum to include those with recurrent brief hypomanias, as suggested by Akiskal [3] and Angst [4]. Although these data support the broadening of the bipolar spectrum, clinicians should be cautious in assuming that mood stabilizers [26, 37, 38] are necessary for all bipolar spectrum patients [39, 40]. The broadening of the bipolar spectrum diagnosis is also of relevance to defining the prevalence of bipolar disorders, which are more prevalent than the traditional 1–2%, when broader diagnostic definitions are used [41].
Footnotes
Acknowledgements
This research was funded by the Health Research Council of New Zealand.