
Abstract
Introduction
Psychotic disorders including schizophrenia are severe mental illnesses causing enormous burden to patients, carers and society (Knapp et al., 2004). The literature has shown that, despite advances in pharmacological and psychosocial interventions, a significant proportion of patients with psychotic disorders exhibit persistent functional impairment even in the presence of clinical remission (Andreasen et al., 2005). Recently, there has been a shift of therapeutic focus from symptom control to improved functioning and pursuit of recovery (Harvey and Bellack, 2009). Although there is a lack of consensus or standardised criteria in defining recovery, it is generally agreed that recovery should be conceptualised as a multi-dimensional construct embracing both symptom and functional domains (Harvey and Bellack, 2009). It is also recognised that different perspectives are adopted by clinicians and patients regarding how to view the recovery concept, with the former perceiving recovery as an outcome measure (recovered versus non-recovered) and the latter a process (being in recovery) (Bellack, 2006).
Thus far, data on recovery in psychotic disorders is relatively scarce as few studies have employed both symptomatic and functional remission criteria for outcome evaluation. Among these few studies, some only applied the severity criterion without taking into consideration the duration component (Bobes et al., 2009; Boden et al., 2009; Henry et al., 2010). Additionally, participants recruited by previous research were mainly derived from chronic samples which were clinically heterogeneous (Bobes et al., 2009; Novick et al., 2009). Conversely, examining patients with first-episode psychosis can, first of all, ensure the cohort to be more homogeneous with respect to illness chronicity and treatment exposure; and secondly, allow the course of illness from its onset to be better elucidated.
We have previously examined perceptions of first- episode patients on recovery, with achievement of adequate functioning being regarded as a key element signifying recovery (Lam et al., 2010). In this study, we sought to investigate the prevalence and predictors of symptomatic remission and recovery in a large representative cohort of Chinese young people presenting with first-episode psychosis in Hong Kong 3 years after entry to a territory-wide early intervention service. The operational criteria adopted for recovery were based on clinical definitions incorporating both symptom and functional dimensions. To the best of our knowledge, this study was the largest evaluating remission and recovery in patients with first-onset psychosis in non-Western countries.
Materials and methods
Participants and setting
The initial sample comprised 839 patients who were consecutively enrolled in the EASY programme (Early Assessment Service for Young People with Psychosis) from July 2001 to August 2003. Since 2001, this publicly-funded specialised programme has been providing early assessment and phase-specific intervention for all individuals aged 15 to 25 years experiencing first-episode psychosis in Hong Kong (Tang et al., 2010). The service adopts a case-management approach and assertively follows up patients for the first 3 years after their initial episodes (including follow-up in transitional step-down clinic in year 3). Standardised clinical assessments evaluating onset and development of psychosis, symptom profiles, and psychosocial functioning are performed on each patient. Multi-disciplinary case reviews are held regularly to closely monitor each patient’s clinical progress and treatment outcome. Patients are discharged to general psychiatric service at the end of the programme.
In this study, we excluded patients who had mental retardation, psychotic disorders due to a general medical condition or substance-induced psychosis. Individuals with more than 1 month of psychiatric treatment before service entry were not recruited. Of the initial cohort, 700 participants fulfilled the inclusion criteria and 539 (77%) completed 3-year follow-up.
Assessments and procedure
The baseline and follow-up variables of all participants were obtained via systematic record review. For each participant, outpatient and inpatient medical records, and computerised clinical information were retrieved from medical databases. Trained research assistants acquired the data from medical files according to a protocol designed specifically for data collection in the current study. Standardised data entry forms were used to systematically extract information on intake, treatment and follow-up variables from consecutive medical files. Weekly consensus meetings were held throughout the period of data collection to ensure strict adherence to protocol and to resolve any ambiguity in clinical information during the data acquisition process. Only data that could be reliably extracted from records were targeted for retrieval and analysis. Outcome measures were determined for each month in the 3 years following first contact. The study was part of a large-scale first-episode psychosis outcome study (Chen et al., in press) and was approved by the local research and ethics committee.
Baseline data included sociodemographics, age and mode of onset of first psychotic episode, and duration of untreated psychosis (DUP), defined as the time interval between onset of positive psychotic symptoms and first contact with the psychiatric service. Psychopathological evaluation included positive and negative symptom levels assessed individually from the Clinical Global Impression – Severity of Illness Scale (CGI-S) (Guy, 1976). Past records of suicide attempts and substance abuse were also ascertained. Service utilisation characteristics included number and length of psychiatric hospitalisations, use of second-generation antipsychotic (SGA) medications, and receipt of welfare allowance. Functional outcome was evaluated by the Social Occupational Functioning Assessment Scale (SOFAS) (American Psychiatric Association, 1994) and vocational status. Diagnostic assignment of individual participants was based on a longitudinal approach taking into consideration that diagnostic change may take place over time (Chang et al., 2009). In the EASY programme, diagnosis of each case was derived from the consensus results of an inter-disciplinary conference utilising multiple sources of information, and regular diagnostic reviews were undertaken to incorporate additional clinical information that emerged during the course of illness. In this study, the final 3-year clinical diagnosis based on ICD-10 criteria (World Health Organization, 1992) was thus ascertained as a participant’s research diagnosis.
Participants were classified as achieving symptomatic remission if they maintained CGI-S scores < 3 for both positive and negative symptoms in the last 6 months of the 3-year follow-up. Functional remission was defined as attaining both sustained employment (full-time or part-time work/study) and SOFAS score > 60 in the last 12 months of the follow-up period. Recovery was defined as simultaneous fulfilment of the following criteria in the last 12 months of study period: (i) CGI-S scores < 3 for both positive and negative symptoms; (ii) no psychiatric admission; (iii) achieving functional remission.
Validity and inter-reliability for major variables including DUP and outcome measures were evaluated based on 12 cases using intra-class correlation coefficient (ICC). Validity compared ratings between an experienced psychiatrist and research staff (ranged from 0.78 to 1.00). Inter-rater reliability compared ratings between research staff (ranged from 0.70 to 1.00). Both validity and inter-rater reliability exercises yielded a satisfactory level of concordance.
Statistical analysis
To assess potential attrition bias, baseline differences between completer and non-completer groups were evaluated using a chi-square test and independent t-test as appropriate. Subsequent analyses were performed only on participants who completed 3-year follow-up. Group differences (i.e. remitted versus non-remitted patients; recovered versus non-recovered patients) with regard to sociodemographics and baseline clinical characteristics were examined using chi-square test for categorical variables and independent t-test for continuous measures. Those variables that were found to be statistically significant in bivariate analyses were then included into stepwise binary logistic regression models to identify predictors of symptomatic remission and recovery. We also assessed the differences in 3-year outcome between patients achieving symptomatic remission and those who did not. The level of statistical significance for all analyses was set at p < 0.05.
Results
Characteristics of the sample
Of 700 first-episode patients who fulfilled inclusion criteria at baseline, 539 (77%) completed 3-year follow-up. There was no significant difference between completers and non-completers on sociodemographics, DUP and other baseline characteristics, with the exception of diagnosis. Participants who completed follow-up were more likely to have schizophrenia spectrum disorder (schizophrenia and schizoaffective disorder) when compared with those who disengaged from service (χ2 = 18.9, p < 0.001). Of these 539 participants, 51.6% were male (n = 278) and 28.6% (n = 154) were employed or studying at entry. The mean age at entry was 21 years (SD = 3.4). The mean DUP was 226.3 days (SD = 360.0; median DUP = 91 days), with 49.7% less than 3 months. Schizophrenia spectrum disorder was the most common diagnosis, accounting for 73.3% of the completer sample, followed by other psychoses (acute and transient psychotic disorders, delusional disorder and unspecified non-organic psychosis; 16.3%) and affective psychosis (bipolar disorder and depression with psychotic features; 10.4%).
Prevalence of remission and recovery
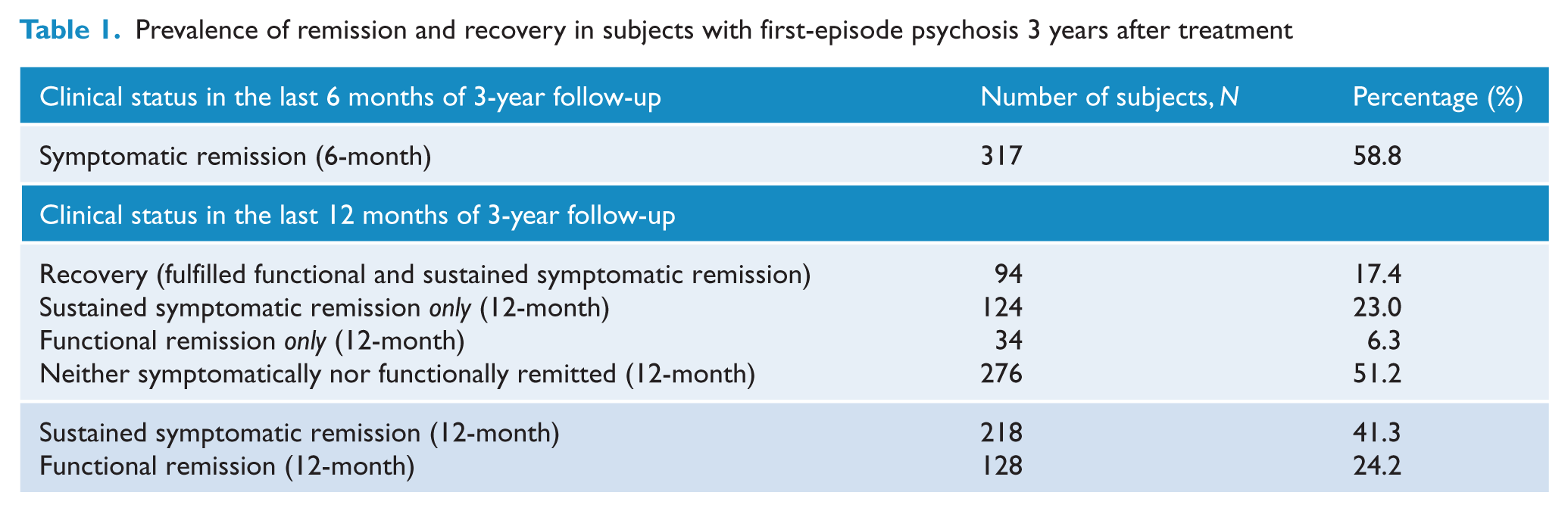
As shown in Table 1, by the end of 3-year follow-up, 317 (58.8%) and 128 (23.7%) participants met criteria for symptomatic and functional remission, respectively. Ninety-four patients (17.4%) achieved recovery at year 3, while 276 (51.2%) were classified as non-remitters in both symptomatic and functional domains over the period of the last 12 months of follow-up.
Prevalence of remission and recovery in subjects with first-episode psychosis 3 years after treatment
Predictors of symptomatic remission and recovery
Table 2 summarises the differences between symptom remitters and non-remitters on a range of sociodemographics, baseline and outcome characteristics. Remitted patients were significantly more likely to be female, to have higher educational attainment, older age of onset of psychosis, shorter DUP, acute development of psychotic symptoms, non-schizophrenia spectrum diagnosis, and early symptom resolution within the first 3 months of treatment. Besides, patients in remission spent less days in inpatient units, had fewer admissions and more favourable functional outcome (higher mean SOFAS score and higher likelihood to sustain stable employment in year 3) than non-remitters. Logistic regression analysis revealed that female sex, older age of onset, shorter DUP and early symptom resolution predicted symptomatic remission 3 years after service entry (χ2 = 29.1, p < 0.001, Nagelkerke R2 = 0.72) (Table 3).
Sociodemographic, baseline and outcome characteristics of patients in symptomatic remission and non-remission groups
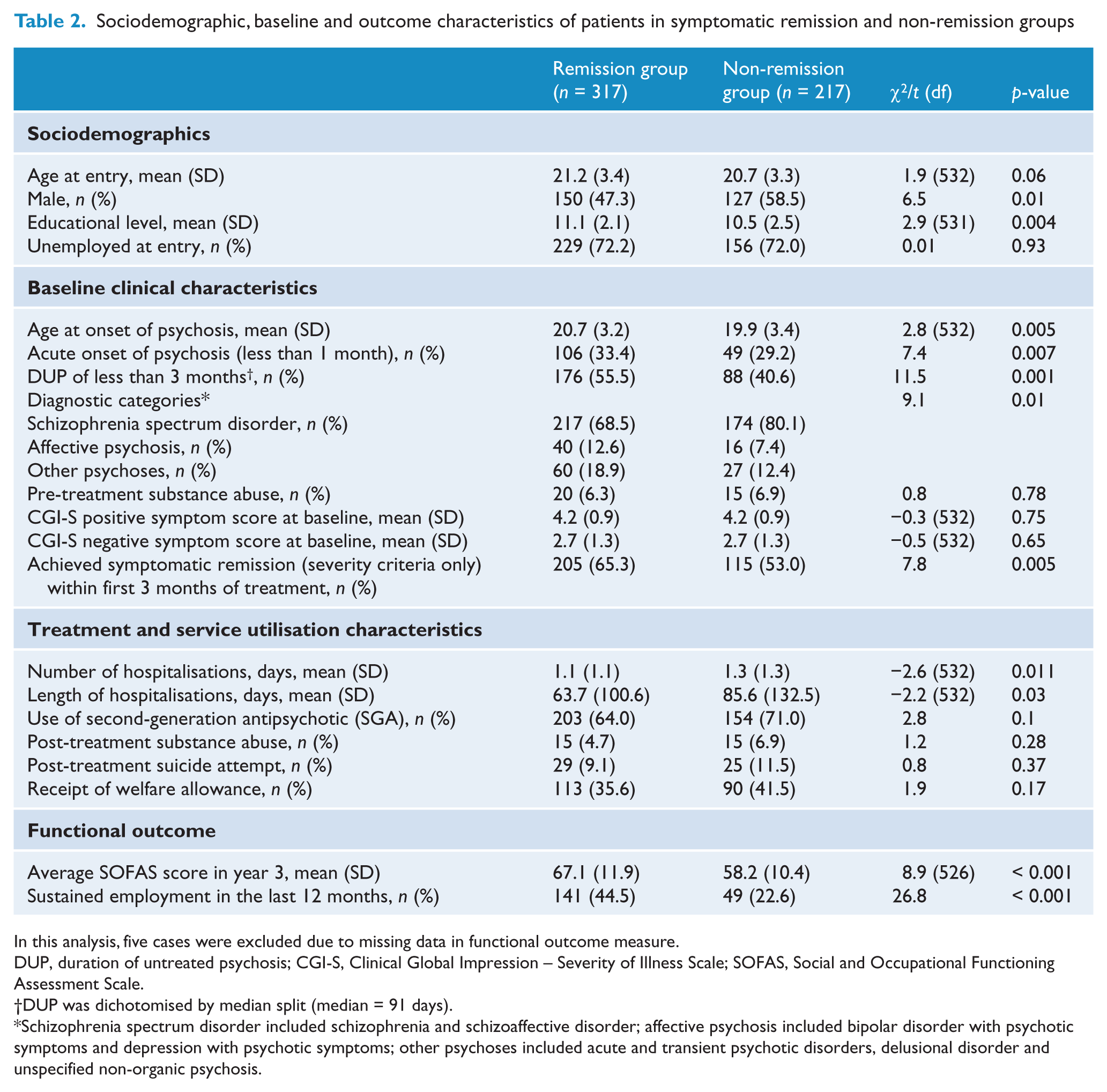
In this analysis, five cases were excluded due to missing data in functional outcome measure.
DUP, duration of untreated psychosis; CGI-S, Clinical Global Impression – Severity of Illness Scale; SOFAS, Social and Occupational Functioning Assessment Scale.
DUP was dichotomised by median split (median = 91 days).
Schizophrenia spectrum disorder included schizophrenia and schizoaffective disorder; affective psychosis included bipolar disorder with psychotic symptoms and depression with psychotic symptoms; other psychoses included acute and transient psychotic disorders, delusional disorder and unspecified non-organic psychosis.
Logistic regression analysis for predictors of symptomatic remission in patients with first-episode psychosis
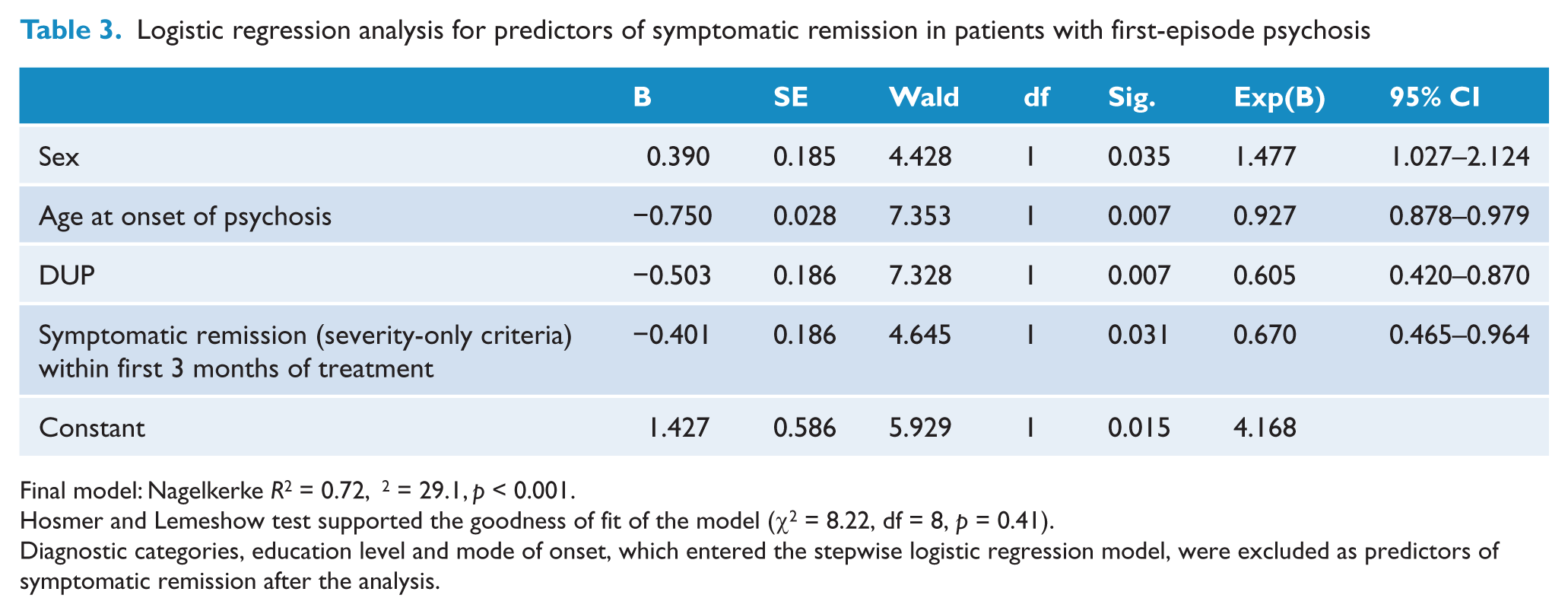
Final model: Nagelkerke R2 = 0.72, χ2 = 29.1, p < 0.001.
Hosmer and Lemeshow test supported the goodness of fit of the model (χ2 = 8.22, df = 8, p = 0.41).
Diagnostic categories, education level and mode of onset, which entered the stepwise logistic regression model, were excluded as predictors of symptomatic remission after the analysis.
Differences between participants who achieved recovery and those who did not are presented in Table 4. Patients in recovery were more likely to be female, to engage in work or study at intake, to have higher educational attainment, shorter DUP, acute onset of psychosis, non-schizophrenia spectrum diagnosis, and fewer negative symptoms at baseline. Compared to non-recovered patients, participants who met criteria for recovery had lower rate of admissions, shorter duration of inpatient stay, and a lower likelihood of receiving welfare allowance from the government. Logistic regression analysis showed that higher educational level, shorter DUP and superior baseline occupational status were predictive of recovery (χ2 = 33.9, p < 0.001, Nagelkerke R2 = 0.10) (Table 5).
Sociodemographic, baseline and treatment characteristics of patients in recovery and non-recovery groups
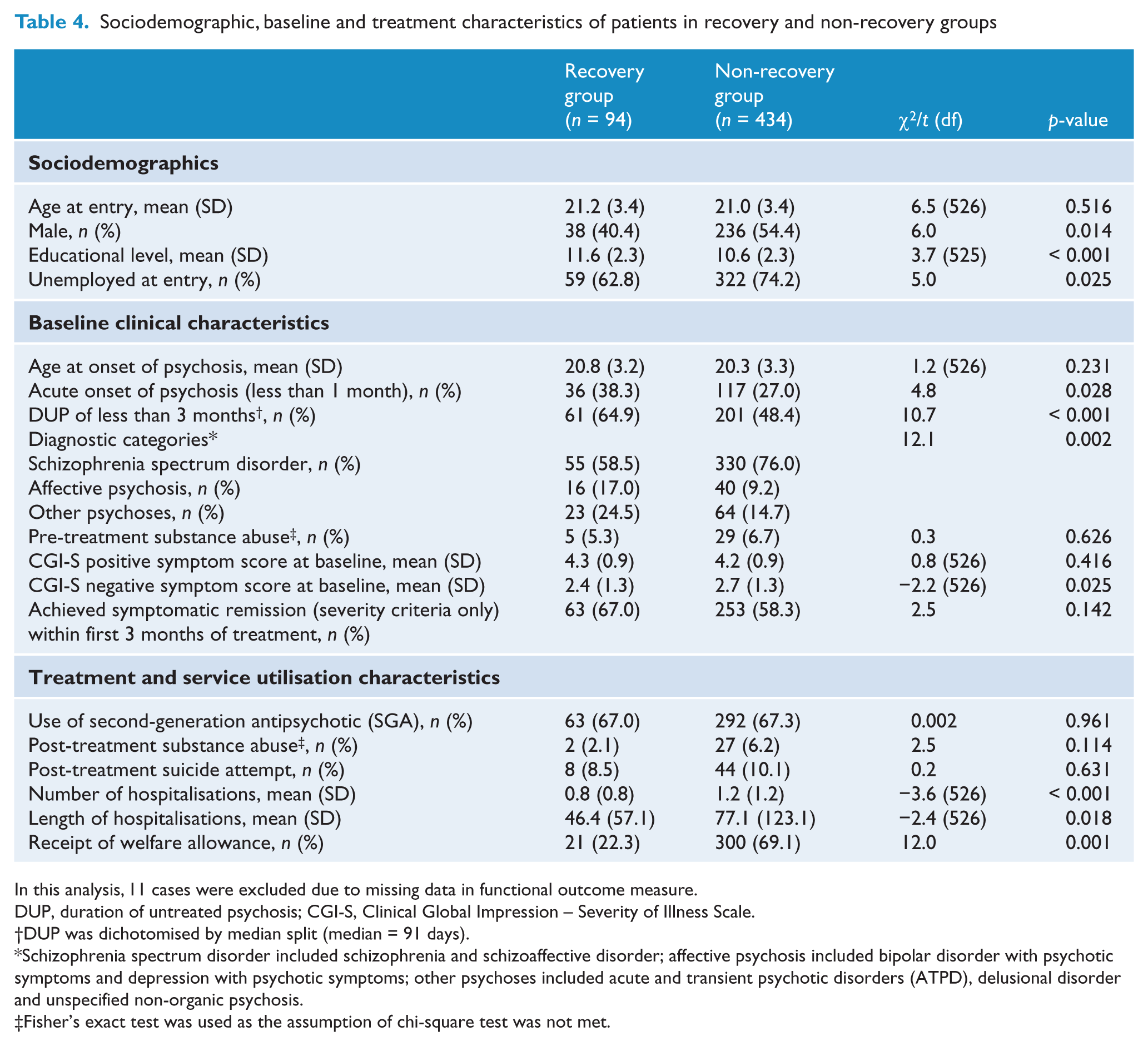
In this analysis, 11 cases were excluded due to missing data in functional outcome measure.
DUP, duration of untreated psychosis; CGI-S, Clinical Global Impression – Severity of Illness Scale.
DUP was dichotomised by median split (median = 91 days).
Schizophrenia spectrum disorder included schizophrenia and schizoaffective disorder; affective psychosis included bipolar disorder with psychotic symptoms and depression with psychotic symptoms; other psychoses included acute and transient psychotic disorders (ATPD), delusional disorder and unspecified non-organic psychosis.
Fisher’s exact test was used as the assumption of chi-square test was not met.
Logistic regression analysis for predictors of recovery in patients with first-episode psychosis
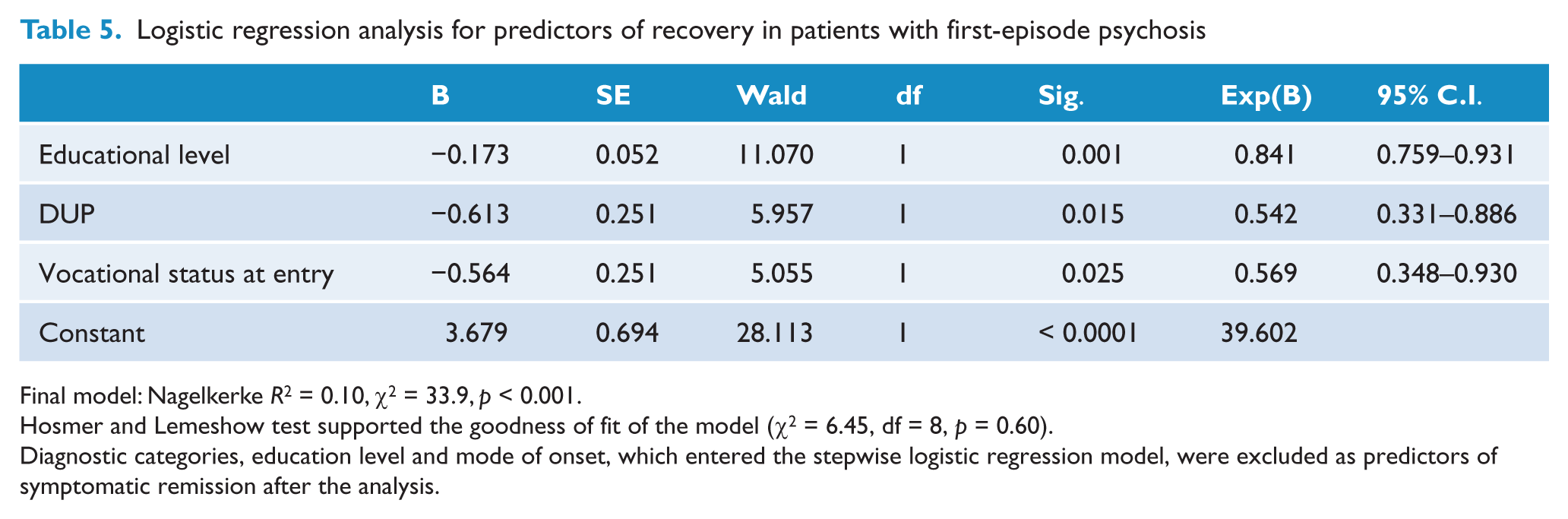
Final model: Nagelkerke R2 = 0.10, χ2 = 33.9, p < 0.001.
Hosmer and Lemeshow test supported the goodness of fit of the model (χ2 = 6.45, df = 8, p = 0.60).
Diagnostic categories, education level and mode of onset, which entered the stepwise logistic regression model, were excluded as predictors of symptomatic remission after the analysis.
Discussion
In the current analysis, we found that approximately 60% of participants presenting with first-episode psychosis achieved symptomatic remission 3 years after service entry. However, only a quarter of patients fulfilled criteria for functional remission, and less than one-fifth were recovered by the end of 3-year follow-up. Further, half of all patients were not remitted either symptomatically or functionally in the last 12 months of the study period. It should be noted that it may be difficult to directly compare our results with previous findings due to substantial methodological variations across studies and lack of consistent definitions regarding recovery (Harvey and Bellack, 2009). Nonetheless, literature revealed that the rate of symptomatic remission in first-episode psychosis ranged from 36% to 59%, with the majority above 50% irrespective of varying symptom criteria, timeframes and lengths of follow-up adopted among studies (Addington and Addington, 2008; Boden et al., 2009; Cassidy et al., 2010; Emsley et al., 2007; Henry et al., 2010; Petersen et al., 2008; Robinson et al., 2004; Saravanan et al., 2010; Wunderink et al., 2009). Our findings on prevalence of symptomatic remission were therefore largely consistent with previous results. The rates of functional remission and recovery in our first-episode sample were also in line with published reports (Albert et al., 2011; Henry et al., 2010; Petersen et al., 2008; Robinson et al., 2004; Wunderink et al., 2009).
In accordance with the results of earlier reports (Wunderink et al., 2009), our study showed that the majority of those who were functionally remitted also met criteria for sustained symptomatic remission (73.4%). Conversely, of those who achieved sustained symptomatic remission, only 43.1% were also in functional remission. It indicated that most patients who functioned properly were also free from symptoms but not the other way round. Thus, our results lend support to the proposition put forward by Andreasen et al. (2005) that remission of symptoms is a necessary but not sufficient step towards recovery. Moreover, our findings of 6.3% of participants being functionally remitted in the absence of sustained symptomatic remission suggested that functional improvement could occur in a small minority of patients who were not free from symptoms.
We replicated results from several past studies that shorter DUP was predictive of symptomatic remission (Addington and Addington, 2008; Emsley et al., 2006; Robinson et al., 2004; Wunderink et al., 2007) and recovery (Robinson et al., 2004; Wunderink et al., 2009). In fact, a substantial body of evidence has demonstrated that prolonged DUP was associated with poor clinical and functional outcomes independent of other potential confounders such as poor premorbid adjustment, at least in the short- to medium-term of illness course (Marshall et al., 2005). On the contrary, some researchers argued that it was duration of untreated illness (DUI) rather than DUP that strongly predicted psychosocial functioning (Crumlish et al., 2009), while others suggested that effect of DUP on longer-term outcome may be diluted by other factors such as comorbid substance abuse, treatment adherence (Addington et al., 2004), and environmental factors including social support, discrimination and job opportunities (Rinaldi et al., 2010). Although further research is required to either refute or confirm the neurotoxicity hypothesis of DUP (Wyatt, 1991), it is recognised that prolonged DUP would cause significant psychosocial disruptions in patients with psychotic illness. This is particularly relevant as onset of psychosis most frequently occurs in late adolescence or early adulthood, critical life stages for an individual’s scholastic and vocational development. In this regard, reducing treatment delay, i.e. DUP, which is one of the few potentially modifiable prognostic factors of psychotic disorders, may improve long-term outcome as achieving adequate functioning in the early phase of illness may serve as a foundation for building further and sustained functional gains.
Our findings that female sex and older age of onset predicted symptomatic remission, as well as superior baseline occupational functioning and higher educational attainment predicted recovery were in agreement with past studies (Harrison et al., 2001; Lambert et al., 2008; Novick et al., 2009; Torgalsboen, 1999; Wunderink et al., 2009). We also confirmed previous findings showing that early symptom resolution was predictive of symptomatic remission (Lambert et al., 2008). As early treatment response was shown to be closely related to later outcome, early detection of incomplete symptom remission or treatment resistance followed by subsequent adaptations of clinical management may further improve the overall prognosis of the illness (Emsley et al., 2006). Contrary to past findings suggesting that substance abuse was associated with poorer outcome in psychotic disorders, we failed to demonstrate any significant negative correlations of substance abuse with either symptomatic remission or recovery. Nonetheless, it should be noted that the prevalence of substance abuse in our first-episode sample was low when compared with that of Western countries. Thus, it may limit the generalisability of our results in this regard.
With regard to outcome difference between patients who attained symptomatic remission and those who did not, our results, which were in line with the literature, demonstrated that the remitter group had more favourable clinical and functional outcomes than non-remitted counterparts (Cassidy et al., 2010; Emsley et al., 2007; Henry et al., 2010; Wunderink et al., 2007). In particular, remitted participants were significantly more likely to maintain stable employment in the last year of follow-up. However, less than half of remitted patients (44.5%) attained sustained employment after 3 years of treatment, and the overall employment rate was low, with only around one-third (35.6%) of all participants being able to obtain a stable job at the end of follow-up. The findings thus highlighted the significance of unemployment problems in the first-episode population and an inadequacy of the current early intervention service in improving patients’ occupational functioning. In fact, one previous study revealed that young people with first-episode psychosis were 10 times more likely to be unemployed than their same-age peers in the general community (Killackey et al., 2006). We also found that recovered patients were less likely to receive welfare benefits from the government for their illness and social disability. Given that unemployment and lost productivity contribute significantly to the societal costs of psychotic disorders (Knapp et al., 2004), provision of intensive psychosocial interventions, including those specifically addressing vocational deficits such as individual placement and support (IPS), in the early stage of illness may be particularly cost-effective in minimising long-term psychosocial impairments (Killackey et al., 2008; Rinaldi et al., 2010). In a similar vein, the World Psychiatric Association has identified setting goals for employment and education as recommended roles for psychiatrists working with young people presenting with first-episode psychosis (Martindale et al., 2009).
There are several limitations in the study. First, the study was based on medical file review, which may be biased by varying degrees of documentation quality. As this specialised early intervention service adopted a case management approach in which the same clinical team followed through this cohort in the first 3 years, the quality of clinical documentation of this ‘first-contact-to-treatment’ sample is therefore relatively more homogeneous than other comparable retrospective record review studies using clinical data from a generic psychiatric service. Besides, as clinical presentation and illness progress of each individual enrolled in this programme was thoroughly assessed and closely monitored, and all available sources of information would be ascertained via multi-disciplinary input, the possibility of missing relevant clinical data for case notes documentation was thus minimised. Moreover, errors in data extraction may be further reduced via close scrutiny of data acquisition and rating processes by regular consensus meetings. Second, our criteria for symptomatic remission were based on the CGI-S scale, which has been employed in previous large-scale studies for defining clinical remission (Lambert et al., 2008; Novick et al., 2009), and is a less specific measure of symptom severity than psychopathological ratings proposed by Andreasen et al. (2005) in their definition of remission. Third, as we only focused on variables that could be reliably retrieved from medical records, information of some other important variables such as detailed premorbid functioning and quality of life could not be addressed in this study.
In conclusion, the current study showed that, in a large and clinically homogeneous cohort of Chinese young people experiencing first-episode psychosis, more than half achieved symptomatic remission 3 years after treatment initiation. However, our findings of a low rate of functional remission and recovery, along with similar results in the literature and a recent debate regarding sustained effectiveness of early intervention for psychosis (Bosanac et al., 2010; McGorry et al., 2010; McGorry, 2011; Rosenman and Anderson, 2011), indicated that early identification and prompt management of treatment non-responders and more intensive psychosocial interventions should be incorporated in early intervention programmes to further improve patients’ social and vocational outcomes. It is acknowledged that at present there is an inadequate knowledge base in guiding how to incorporate cognitive and psychosocial dysfunction into the definition of functional remission and recovery (Andreasen et al., 2005), and therefore more research should be conducted to explore the longitudinal relationship between cognitive deficits, functional impairments and remission of symptoms. Further studies are also needed to evaluate the trajectory of remission status and the potential prognostic role of early remission and recovery in predicting long-term outcome.
Footnotes
Acknowledgements
The authors would like to thank all coordinating clinicians and staff from the participating hospitals, clinics and medical records departments for their kind assistance.
Funding
The study was part of the historical case-controlled study of first-episode psychosis which was supported by a grant from the Health and Health Service Research Fund (03041041) of the Food and Health Bureau, the Government of Hong Kong Special Administrative Region. Author E.Y.H.C. has participated in the paid advisory board for Otsuka, has received educational grant support from Janssen-Cilag, and has received research funding from Astra-Zeneca, Janssen-Cilag, Eli Lilly, Sanofi-Aventis and Otsuka; Author M.M.L.L. has done consultancy for Otsuka and Eli Lilly.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.