
Abstract
Aims:
Young people with first-episode psychosis (FEP) or at ultra-high risk (UHR) of psychosis often have lower vocational engagement than their peers. This study examines the effect of treatment in early intervention for psychosis services in Australia on engagement in education and employment.
Methods:
This is a naturalistic sample of young people aged 12–25 with FEP (n = 1574) and UHR (n = 1515), accessing treatment in the headspace Early Psychosis (hEP) programme. Engagement in education and employment was assessed at baseline and every 90 days in treatment. Mixed effects logistic regression were used to analyse changes over time.
Results:
On entering the hEP programme, approximately 49% of the young people with FEP and 28% of the young people at UHR status identified as Not in Education, Employment or Training (NEET). The odds of being NEET were reduced by 27% (95% confidence interval = [14, 39]) for every 6 months treatment for the FEP group, but no change in NEET status was observed in the UHR group. In both groups, absence from daily activities was significantly reduced during time in treatment.
Conclusion:
While there are methodological challenges analysing real-world non-control group cohort data, the findings indicate positive effects of the hEP programme on vocational and daily activity engagement for young people with FEP and at UHR status. A large proportion of the young people still identified as NEET after receiving treatment services, suggesting further refinement to ensure targeted and consistent vocational support throughout care.
Introduction
The onset of psychotic disorders typically occurs in late adolescence or early adulthood (McGorry et al., 2011). This is a critical period in life, when most young people are beginning higher education or starting their first job. Being affected by mental ill-health in youth can interrupt the vocational development of the young person. For young people (aged 15–25) accessing mental health services for psychotic disorders, the proportion identifying as Not in Education, Employment or Training (NEET) is more than three times higher than the proportion identifying as NEET among their general population peers (Brown et al., 2020). Low engagement in employment is also observable in young people at ultra-high risk (UHR) of developing psychosis (Cotter et al., 2017).
Functional and vocational outcomes in youth with mental ill-health are a key domain to address due to its high personal and economic consequences. School absence is associated with lower academic achievement and lower earnings later in life (Cattan et al., 2022; Hancock et al., 2013) and lack of school qualifications may contribute to a sense of social exclusion for the young person (Filia et al., 2019). Similarly, unemployment has also been linked to reduced earnings (Brand, 2015) as well as reduced well-being and poor mental health (Modini et al., 2016; Mousteri et al., 2018; Reneflot and Evensen, 2014). These negative consequences of unemployment can be long lasting and affect the young person over the life course (Strandh et al., 2014). The low engagement in employment for persons affected by psychotic illness is one of the main factors leading to the high socio-economic costs of psychotic illnesses (Hastrup et al., 2020).
The potential to improve the lives of young people, as well as reduce the societal costs of mental illnesses, speaks to the benefits of supporting the vocational needs of young people with mental ill-health as early as possible. Importantly, young people with mental ill-health consistently report engagement in education and/or employment as one of their primary goals (Ramsay et al., 2011; Thomas et al., 2020). Vocational support for young people therefore forms a valuable component of mental health services but is frequently under-funded and under-prioritised.
Early intervention in psychosis (EIP) services, which deliver multi-component psychosocial interventions provided by a multidisciplinary team, have documented positive effects on symptom reduction and global functioning, including engagement in education and employment (Correll et al., 2018). In Correll et al.’s (2018) meta-analysis examining the effects of EIP services vs treatment as usual, six studies (with a total of 1743 individuals with first-episode psychosis [FEP]) examined vocational outcomes specifically. The meta-analysis showed that the proportion of individuals in school or employed was 53% for individuals in EIP, compared to 45% in treatment as usual. A systematic review and meta-analysis by Frawley et al. (2023) examines the effects of different psychosocial interventions (e.g. cognitive behavioural therapy, supported employment) on global functioning, including employment. The study concludes that multi-component psychosocial interventions, characteristic of EIP services, are effective in improving functioning in FEP. The authors also speculated a positive effect in individuals with UHR status, although this could not be sufficiently documented in the meta-analysis with further real-world data being required.
In Australia, a series of EIP services have been established that are delivered through the headspace Early Psychosis (hEP) programme in headspace centres across Australia (a national Commonwealth Government funded initiative to improve access to mental health care for 12–25 year olds). A recent study highlighted improvements in short- and medium-term clinical and functional outcomes in young people accessing these hEP services (Brown et al., 2022), but the vocational outcomes have not yet been assessed. The current study explores engagement in education and work for young people in the hEP programme by examining routinely collected information on education and employment status and information on absence from daily activities due to mental ill-health. In addition, this study aims to determine the effects of receiving treatment in the hEP programme on these vocational outcomes and examine whether symptom severity impacts the treatment effect.
Methods
Setting
The hEP programme is a comprehensive EIP service based on the evidence-based Early Psychosis Prevention and Intervention Clinic and Personal Assessment and Crisis Evaluation models which originated from Orygen in Melbourne in the 1990s (Stavely, 2013; Yung et al., 2007). Within the hEP programme, young people and their families are offered easy-access, recovery-oriented, community-based care delivered by clinically trained case managers (e.g. psychologists, social workers, occupational therapists, mental health nurses), psychiatrists, family workers and peer support workers. Depending on individual needs, the hEP programme can be accessed for 2–5 years for young people with FEP and 6–12 months for those with UHR criteria who do not go on to develop a psychotic disorder. The hEP programme is delivered at 15 headspace centres in Australia across six clusters (South East Melbourne, Western Sydney, North Perth, Adelaide, South East Queensland and Darwin).
In terms of vocational support at hEP services, all programmes ensure there is a focus on education and employment for young people wishing to address these goals through their time in the programme as it is one of the 16 core components of the service model (Hetrick et al., 2018). While each service differs based on local need, core parts of the hEP programme typically include vocational-focused group programmes, having Individual Placement and Support (IPS) workers embedded in the programme, and utilising established collaborations with local employment services. This inclusion of vocational support in the programme is monitored through annual fidelity assessments (Williams et al., 2021).
Participants
The study sample is a naturalistic cohort of young people aged 12–25 accessing treatment for FEP or UHR through the hEP programme. FEP status and UHR status were determined based on the criteria outlined in Comprehensive Assessment of At Risk Mental States (Yung et al., 2005). All young people accessing the service between 19 June 2017 and 22 March 2021 who consented to having their data used for service evaluation purposes were included in the current study.
Measures
Data were collected by hEP clinicians at the young person’s entry into the hEP programme and routinely every 90 days when in the programme into an electronic Minimum Data Set. Data are collected for each distinct time period the young person uses the service, referred to as ‘episodes of care’. In this study, only an individual’s first episode of care was used in the analyses.
Demographics
At entry into the hEP service, demographic data are collected on the young person’s age, gender, sexuality, ethnicity and First Nations status. A socio-economic index was assigned to each young person by matching their residential postcode to the Index of Relative Socio-economic Disadvantage (IRSD) score, derived from the 2016 Australian National Census (Australian Bureau of Statistics, 2016), with lower scores indicating greater disadvantage. Duration of untreated psychosis (DUP) was assessed by clinicians for individuals experiencing FEP at entry into the service. DUP is defined as the days between the date of first manifest symptom of psychosis at threshold for a psychotic disorder and the date of first treatment with antipsychotic medication or entry into the hEP programme.
Clinical measures
The 24-item Brief Psychiatric Rating Scale (BPRS; Overall and Gorham, 1962) is also completed by the clinician at each assessment as a measure of overall psychopathology. This covers 24 distinct psychiatric symptoms which are rated on a scale from 1 to 7, with the total score ranging from 24 to 168, and with higher scores representing more severe psychopathology (Shafer, 2005).
Vocational outcome measures
Young people report their current education and employment status at each assessment. NEET is defined as not being in full- or part-time education and not being in full- or part-time employment.
Absence from daily activities is measured using the two additional items collected as part of the Kessler Psychological Distress Scale (K10, Kessler et al., 2003). These two items, indicated by K10+, are measured in the Mental Health National Outcomes and Casemix Collection (www.amhocn.org/nocc-collection/nocc-measures), and explore absence from daily activities due to psychological distress, as measured by K10. The K10+ ‘days absent’ question reads ‘In the last four weeks, how many days were you TOTALLY UNABLE to work, study or manage your day to day activities because of these feelings?’ and the K10+ ‘reduced days’ question reads ‘[Aside from those days], in the last 4 weeks, how many days were you able to work or study or manage your day to day activities, but had to CUT DOWN on what you did because of these feelings?’.
In this study, responses on the first question are used to indicate number of ‘days absent’ in the last 4 weeks. To indicate number of ‘days impaired’, responses on the two questions are combined into one variable indicating fully or partly absence in the last 4 weeks. As the responses to the number of ‘days absent’ and the number of ‘days impaired’ were highly skewed with an inflated number of zeros, both responses were dichotomised. Cut-off scores were based on the distribution of the data for ‘days absent’ (⩾5 days), and cut-off scores used by the Australian Bureau of Statistics for ‘days impaired’ (⩾8 days; Mulder and Cashin, 2015). The two dichotomised variables were used for the primary analyses.
Statistical analysis
The same statistical approach was used to analyse each of the UHR and FEP cohorts separately. Demographic and clinical characteristics were described for each cohort using frequencies and percentages for categorical variables and means and standard deviations (SDs) for continuous variables.
Within each cohort, mixed effects logistic regression models were used to analyse the longitudinal effects of treatment time within the hEP programme on each of the vocational outcomes. Mixed effects models allow for correlated responses over time within individuals by including a participant identifier as a random effect in the model, while treatment time and potential confounders are included in the model as fixed effects. For both cohorts, data collected at 0 (baseline), 3, 6, 9 and 12 months were included in the regression models. The number of months in the programme was treated as a continuous variable, with one unit of treatment represented by 6 months in the programme. The treatment odds ratio (OR) may then be interpreted as the multiplicative change in the odds of experiencing the outcome of interest, for every 6 months of treatment for an individual. Each model was also adjusted for known confounders, age at entry to the programme, gender, IRSD score, First Nations status and the service cluster where the client attended the hEP programme. To assess the impact of clinical presentation when entering the hEP programme on the effect on treatment outcomes, a stratified analysis was undertaken for clients with a baseline BPRS score <50 and for clients with a baseline BPRS score ⩾50. This cut-off was chosen based on existing raw data median scores (Brown et al., 2022).
Missing data were addressed using multiple imputation procedures (Rubin, 1987). Fifty datasets were imputed in wide format to take account of multiple measurements per person using the R package MissRanger (Mayer, 2023), which uses a chained random forest algorithm. The imputed datasets were analysed in long format, and the results pooled using Rubin’s (1987) rules. The primary results are based on the imputed analyses; however, a complete case analysis was included for comparison.
Sensitivity analyses were conducted on the K10+ ‘days absent’ outcome, treating the data as counts and using mixed effects quasi-Poisson regression to model the effect of treatment in the hEP programme on the number of days absent in the last 4 weeks. The random and fixed effects in the model were the same as for the mixed effects logistic models; however, the treatment effect per 6 months is represented as a rate ratio (RR), interpreted as the multiplicative change in the expected number of days absent within the last 4 weeks. Additional sensitivity analyses of the outcomes were carried out separately within the first 6 months of treatment, to assess for any temporal treatment pattern in comparison to the treatment effects estimated over 12 months.
All analyses were undertaken using the R package (R Core Team, 2013) within RStudio (RStudio Team, 2020), with packages glmer (Bates et al., 2015) and glmmTMB (Brooks et al., 2017) used for the regression analyses.
Ethics
Included individuals in the current study provided verbal consent to have their data collected for service evaluation purposes. Ethical approval was obtained from the University of Melbourne Human Research Ethics Committee (2021-20371-13617-3).
Results
Sample characteristics
Characteristics of the cohorts are presented in Table 1. In total, 1574 young people with FEP and 1515 young people with UHR status accessed treatment in the hEP programme between June 2017 and March 2021 and are included in this analysis. In the FEP group, the majority identified as male (66.7%) and in the UHR group, a slightly higher proportion identified as female (52.7%). The FEP group was also slightly older (mean = 19.8; SD = 2.8) compared to the UHR group (mean = 17.7; SD = 3.1). The number of First Nations young people was similar in the FEP group (7.3%) and in the UHR group (9.3%).
Baseline demographic and clinical characteristics of individuals with FEP and with UHR status.
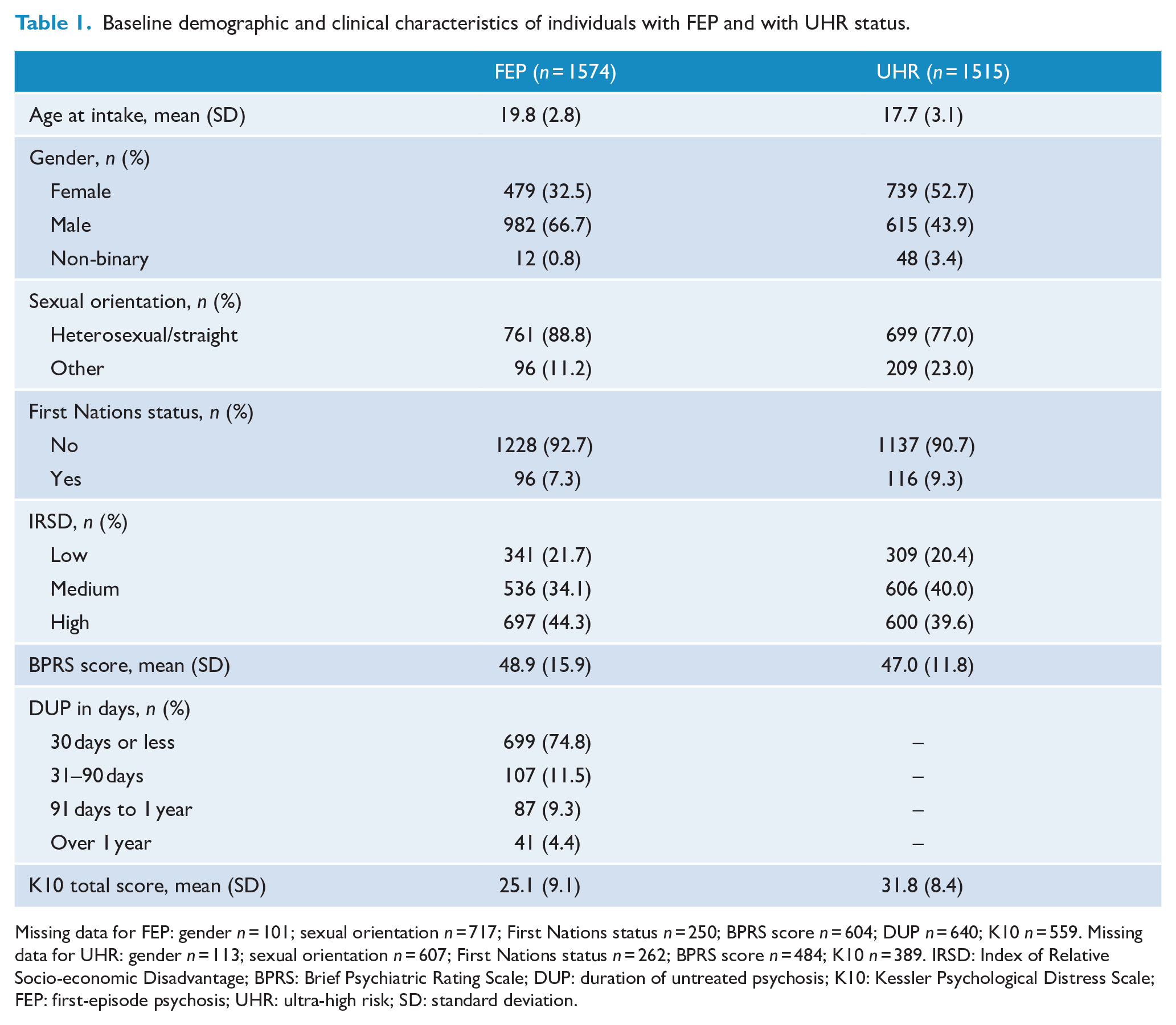
Missing data for FEP: gender n = 101; sexual orientation n = 717; First Nations status n = 250; BPRS score n = 604; DUP n = 640; K10 n = 559. Missing data for UHR: gender n = 113; sexual orientation n = 607; First Nations status n = 262; BPRS score n = 484; K10 n = 389. IRSD: Index of Relative Socio-economic Disadvantage; BPRS: Brief Psychiatric Rating Scale; DUP: duration of untreated psychosis; K10: Kessler Psychological Distress Scale; FEP: first-episode psychosis; UHR: ultra-high risk; SD: standard deviation.
Vocational outcome results
Table 2 presents a descriptive summary of the vocational outcomes at each time point for the FEP and UHR cohorts. Figure 1 presents the results of the mixed effects logistic regression models for the primary outcomes in each cohort using the imputed analyses. For each outcome, the treatment ORs are adjusted for confounders and presented (along with 95% confidence intervals [CIs]) for the overall analysis and for the stratified analysis. These results are also given in Table S1 for FEP and Table S2 for UHR, along with the unadjusted and complete case analyses for each cohort (see Supplemental Appendix 1). The primary results are summarised below. To gain insight into the absolute predictions of the outcomes using our models, Table S3 presents a modelled example of estimating average marginal predicted probabilities for each outcome at each follow-up time based on our cohort covariate data (see Supplemental Appendix 2).
Vocational engagement over time in treatment for individuals with FEP and at UHR status.
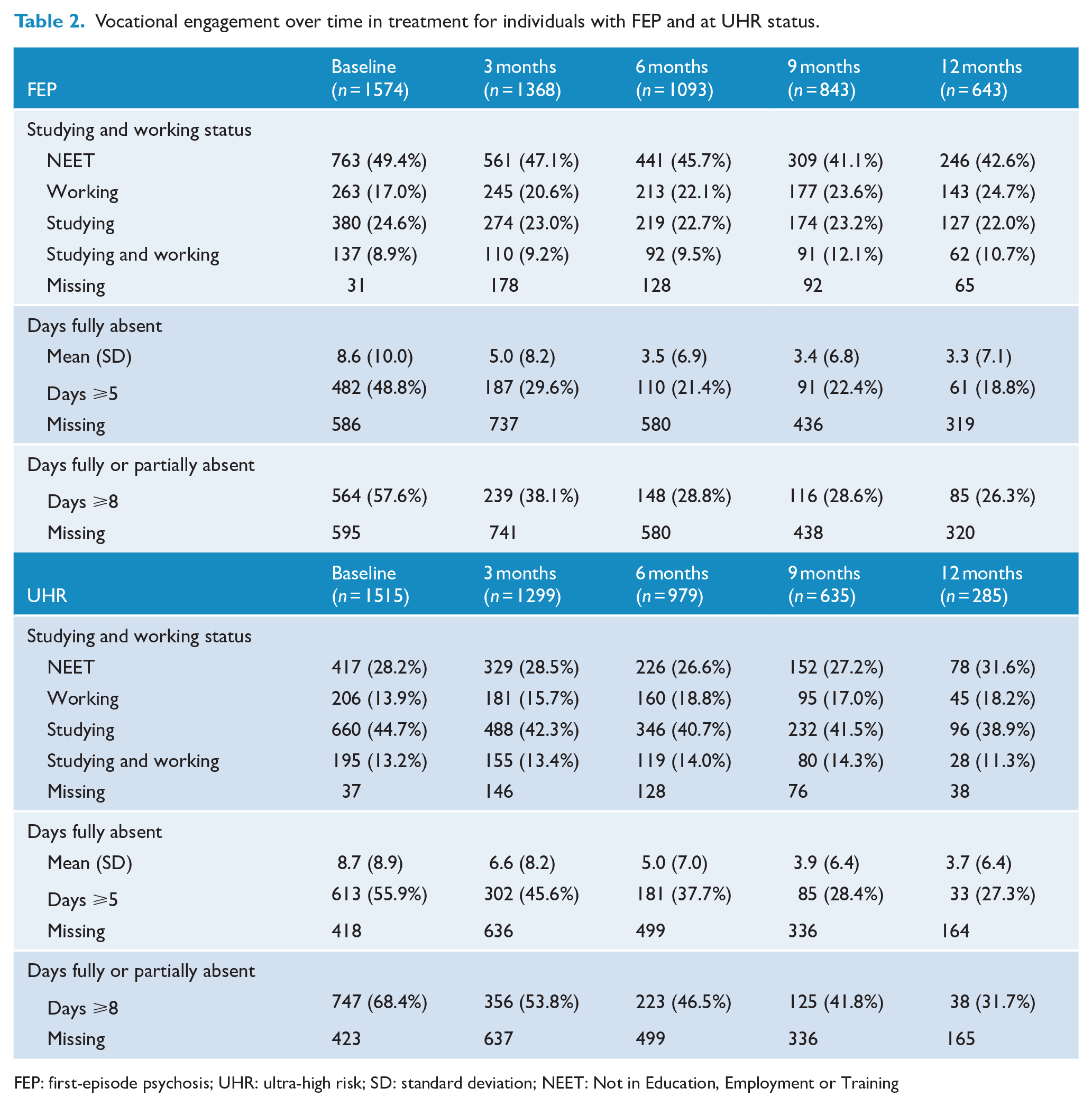
FEP: first-episode psychosis; UHR: ultra-high risk; SD: standard deviation; NEET: Not in Education, Employment or Training
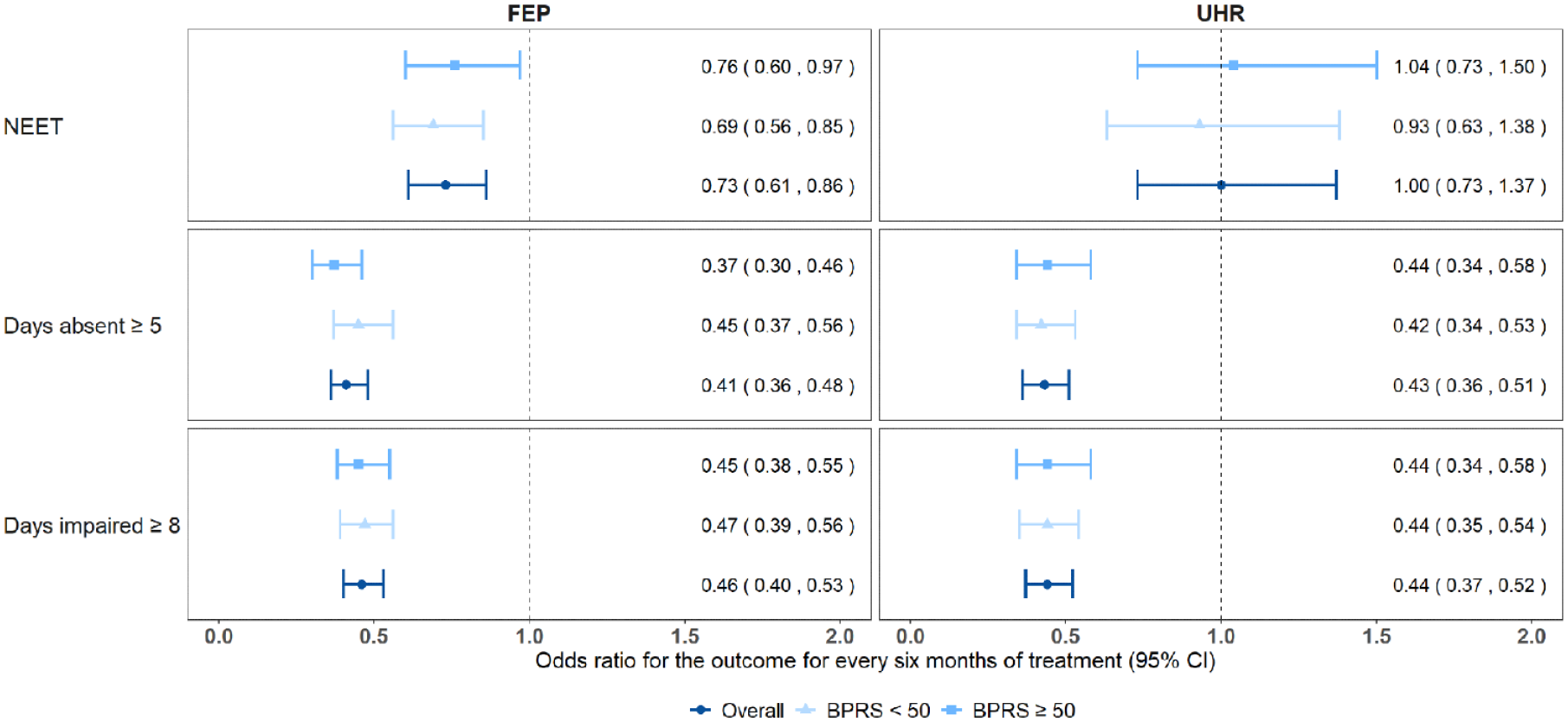
Odds ratio of vocational engagement outcomes per 6 months in treatment for individuals in FEP and UHR group (total cohort and stratified by baseline BPRS scores), using imputed mixed effects logistic models controlling for age, gender, IRSD score, First Nations status and service clusters.
FEP cohort
NEET status
Table 2 shows how the outcomes in each cohort changed over the course of treatment. Overall, 49.4% of the young people with FEP identified as NEET on entry to service. A further 17.0% were working; 24.6% were studying and 8.9% were both studying and working (n = 1543). The proportion identifying as NEET decreased over time in treatment. At 12 months of service, 42.6% were NEET; 24.7% working; 22.0% studying and 10.7% both studying and working (n = 578).
The results of the mixed effects logistic models (Figure 1) show that the odds of being NEET for the FEP group were reduced by 27% for every 6 months in treatment (OR = 0.73; 95% CI = [0.61, 0.86]). An estimate of the practical impact of this treatment effect on our FEP cohort (Table S3) would be a reduction in NEET status from around 51% at baseline to 41% at 12 months, an estimated 10% reduction.
Days absent from daily activities
At service entry (Table 2), the FEP cohort reported an average 8.6 (SD = 10) days absent from daily activities during the last 4 weeks (n = 988). When combining information on full and partial absence from daily activities, 57.6% of FEP individuals had 8 or more impaired days during the last 4 weeks (n = 978). Those still accessing the hEP service at 12 months had on average 3.3 (SD = 7.1) days absent during the last 4 weeks (n = 324). The proportion of individuals with 8 or more impaired days was reduced to 26.3% after 12 months (n = 323).
Mixed effects logistic models (Figure 1) found the odds of having 5 or more days absent during the last 4 weeks decreased by 59% for every 6 months in treatment (OR = 0.41; 95% CI =[ 0.36, 0.48]). The odds of having 8 or more impaired days decreased by 54% for every 6 months in treatment (OR = 0.46; 95% CI = [0.40, 0.53]).
Impact of symptom severity
Lower symptom severity (defined as a BPRS total score <50) was associated with a greater reduction in NEET status over time in treatment for individuals with FEP (see Figure 1 and Table S1). The odds of being NEET was reduced by 31% (OR = 0.69; 95% CI = [0.56, 0.85]) for every 6 months in treatment for individuals with lower symptom severity and by 24% (OR = 0.76; 95% CI = [0.60, 0.97]) for individuals with higher symptom severity (BPRS total score ⩾50).
The reduction in absence from daily activities over time in treatment was slightly higher in individuals with higher severity (see Figure 1 and Table S1). The odds of being absent from daily activities 5 or more days in the last 4 weeks reduced by 55% (OR = 0.45; 95% CI = [0.37, 0.56]) per 6 months treatment in individuals with milder symptom severity and by 63% (OR = 0.37; 95% CI = [0.30, 0.46]) in individuals with higher symptom severity. The odds of having 8 or more impaired days in the last 4 weeks were similar for both low and high levels of symptom severity.
UHR cohort
NEET status
From Table 2, in the UHR group (n = 1515), 28.2% identified as NEET when they first accessed treatment in the hEP programme, while 13.9% were working; 44.7% were studying and 13.2% were both working and studying (n = 1478). The proportion of young people with UHR status identifying as NEET did not change markedly over time in treatment. Among the young people with UHR status still accessing services after 12 months, the proportion identifying as NEET was 31.6%; 18.2% were working; 38.9% were studying and 11.3% were both studying and working (n = 247).
Mixed effects logistic models (Figure 1) showed that the odds of being NEET for the UHR group did not change over time in treatment (OR = 1.00; 95% CI = [0.73, 1.37]).
Days absent from daily activities
At service entry (Table 2), the UHR cohort had on average 8.7 (SD = 8.9) days absent from their daily activities in the last 4 weeks (n = 1097). Over two-thirds (68.4%) had 8 or more days of daily activity impaired in the last 4 weeks (n = 1092). After 12 months in treatment, absence from daily activities was markedly reduced with those accessing treatment having on average 3.7 (SD = 6.4) days absent during the last 4 weeks (n = 121) and the proportion with 8 or more days impaired in the last 4 weeks was 31.7% (n = 120).
Mixed effects logistic models (Figure 1) found the odds of having 5 or more days absent during the last 4 weeks decreased by 57% for every 6 months in treatment for the UHR cohort (OR = 0.43; 95% CI = [0.36, 0.51]). The odds of having 8 or more days impaired in the last 4 weeks decreased by 56% for every 6 months in treatment (OR = 0.44; 95% CI = [0.37, 0.52], Figure 1).
Impact of symptom severity
There was no evidence of a treatment effect on NEET status for either the low or high symptom severity groups. There was also no evidence that symptom severity impacted the treatment effects on days absent or days impaired.
Sensitivity analysis
Days fully absent
The Poisson regression analysis on number of days absent over time in treatment showed that for every 6 months in treatment, the number of days absent in the last 4 weeks for young people with FEP is expected to reduce by 40% (RR = 0.60; 95% CI = [0.55, 0.67]), after adjusting for age, socio-economic status, gender, First Nations status and service cluster (Table 3). Similar results were found for individuals in UHR, where the number of days absent in the last 4 weeks is expected to reduce by 34% per 6 months treatment (RR = 0.66; 95% CI = [0.60, 0.72]; Table 3). Similar effects were evident in the lower and higher symptom severity groups within both cohorts.
RR of expected number of days absent from daily activities in last 4 weeks, per 6 months in treatment, estimated using mixed effects quasi-Poisson regression for individuals in FEP and UHR cohorts and within symptom severity subgroups.
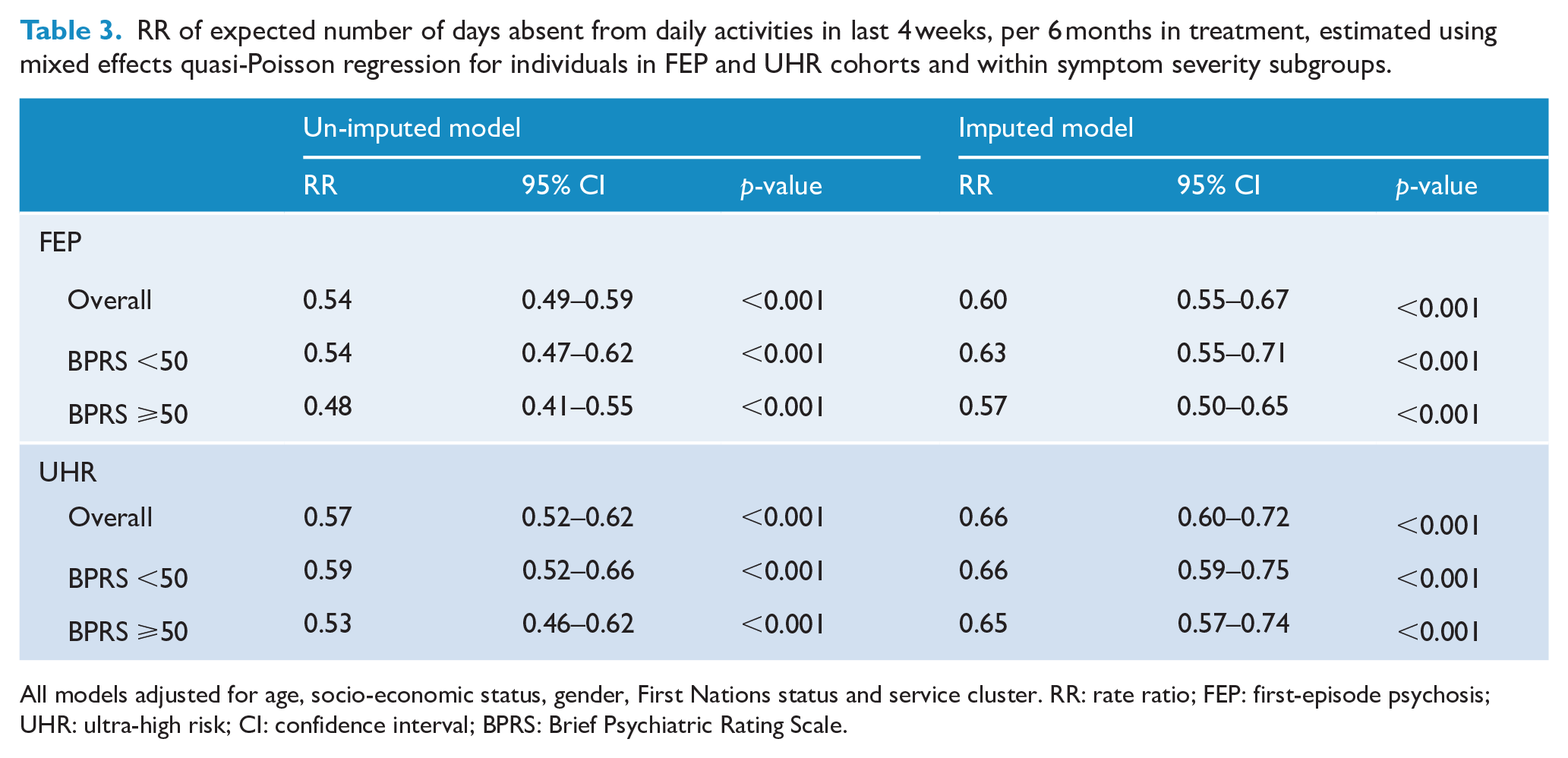
All models adjusted for age, socio-economic status, gender, First Nations status and service cluster. RR: rate ratio; FEP: first-episode psychosis; UHR: ultra-high risk; CI: confidence interval; BPRS: Brief Psychiatric Rating Scale.
Treatment effects within first 6 months
Figure S1 (see Supplemental Appendix 3) provides a comparison of treatment effects estimated within the first 6 months of treatment in the hEP programme to treatment effects averaged over 12 months. For the UHR cohort, the treatment effects were similar for all three outcomes and for the FEP cohort the effects were similar for NEET status. For the FEP cohort, the odds of each of the daily functioning outcomes were reduced by a further 20% within the first 6 months, compared to treatment effects estimated over 12 months, suggesting a greater benefit in the first 6 months of treatment.
Discussion
This analysis of 1574 young people experiencing a FEP and 1515 young people at UHR status is one of the largest naturalistic studies to look at the impact of engaging in real-world EIP services on a young person’s vocational outcomes. In our study, as many as half of the young people with FEP (49.4%) and more than a quarter of the young people with UHR status (28.2%) were NEET when they first accessed treatment in the hEP programme. The longitudinal analyses found that the odds of young people with NEET status were reduced every 6 months in treatment for the FEP group, but not for the UHR group. The number of days absent from daily activities and the number of days impaired (fully or partly from daily activities) were reduced for both the FEP and UHR groups suggesting increased engagement in education or employment during their time in the hEP services. The effect of receiving care on the number of days fully absent and impaired was similar for individuals with high and low symptom severity. However, our study indicates that the positive effect of treatment on NEET status is slightly larger for individuals with FEP with low symptom severity compared to high symptom severity.
While cohort studies that rely on real-time, real-world data collection with no control group have inherent methodological weaknesses, we argue that the current findings still provide valuable evidence of the positive effect of EIP services when treatment is provided in a naturalistic setting. The findings are in line with data published on the positive effect on symptoms, quality of life and social functioning (Brown et al., 2022) and suggest that the evidence regarding superior vocational outcomes for young people who engage with EIP services compared to treatment as usual in clinical trials (Correll et al., 2018) can be generalised to real-world clinical practice. While improvements in the number of individuals being classified as NEET at the beginning of care to later on in care may be relatively small (around 10% from modelling), we believe that it still reflects important gains in the trajectory of young people with early psychosis’ lives and is likely to have a flow on effect on lowering the economic ‘cost’ of the disease (Hastrup et al., 2020).
Despite these promising findings, it is important to note that vocational engagement continues to be low for a large group of young people with FEP and UHR compared to their peers, even after receiving EIP care, as seen in previous literature (Ajnakina et al., 2021; Cotter et al., 2017). The reasoning for low vocational recovery in these cohorts is still not clear, with this study not clearly showing that symptom severity has an impact. This current finding is consistent with another Australian study in a clinical sample of young people accessing treatment in headspace, which found no association between changes in depression and NEET status (O’Dea et al., 2016).
Clinical implications
The findings from this analysis of naturalistic data highlight that while services might be continuing to have a positive impact on the vocational outcomes of the young people they serve, there may be more they could be doing to support these young people to engage in education or work during their tenure of service, e.g. ensuring flexibility of clinical appointments around work/school as young people re-engage with these crucial parts of their life. Given that those with UHR status are in services for less time than those with FEP, and that this analysis shows currently lower gains made for this cohort, perhaps teams need to ensure that vocational support is prioritised earlier during their treatment.
The collection and use of the K10+ data utilised here highlight that tracking of the impact of treatment on a young person’s ability to engage in work or education could be better utilised by treating clinicians to ensure this critical element of functional recovery is adequately attended to throughout care. Utilising IPS (Allott et al., 2019) and vocational specialists within mental health services should remain a priority alongside symptom reduction and remission as it may not be sufficient to focus solely on symptom reduction to improve vocational outcomes (Ramsay et al., 2011; Thomas et al., 2020).
Study limitations
Several limitations affect the interpretation of the findings presented here. As the study is based on routinely collected clinical data, the data collection ended when the treatment was terminated. This can mean large variations in the duration of follow-up and fluctuating cohort size at time points. An important limitation is therefore the lack of knowledge on the vocational functioning of the young people who terminated treatment. The positive effect of treatment could be larger than observed if the young people who discontinued treatment did so due to feeling better. However, the naturalistic design of this study does not allow for this conclusion to be made, and it is also possible that the NEET status negatively influenced the engagement in treatment (Maraj et al., 2019). Treatment effects on NEET status estimated within the first 6 months were comparable to treatment effects averaged over 12 months, suggesting attrition was not a primary driver of NEET status results. The development of a comprehensive clinical registry with data linkage would allow for some of these unknowns to be addressed.
Another important limitation is the lack of a control group. We cannot firmly conclude that the increased vocational functioning across treatment can be directly attributed to the beneficial effects of the hEP programme, or which parts of the programme ultimately support these outcomes (e.g. the comprehensive case-management and multidisciplinary-team approach). Although clinicians had appropriate training in data collection, the study is vulnerable to typical limitations of naturalistically collected data, including variations in clinicians’ interpretations of items, missing data in some items and vulnerability to data entry errors.
Conclusion
This large naturalistic cohort of young people with FEP and at UHR status has outlined the impact that treatment in the hEP programme can have on vocational and daily activity engagement. After 12 months treatment, absence from daily activities was reduced to approximately half the level reported at programme entry for both individuals with FEP and in UHR. The proportion identifying as NEET was reduced for the FEP group, but not the UHR group. Although findings are limited by the unknown vocational engagement of the young people who dropped out of services early, the study supports real-world vocational improvements following initiation of treatment. Even so, too many young people continue to be excluded from education and employment. Given the large personal and socio-economic consequences of vocational exclusion, increased accessibility to employment and education and enhanced focus on vocational support are of key importance.
Supplemental Material
sj-docx-1-anp-10.1177_00048674241261778 – Supplemental material for Vocational functioning in young people accessing services for first-episode psychosis and ultra-high risk of psychosis: A longitudinal naturalistic cohort study
Supplemental material, sj-docx-1-anp-10.1177_00048674241261778 for Vocational functioning in young people accessing services for first-episode psychosis and ultra-high risk of psychosis: A longitudinal naturalistic cohort study by Naja Kirstine Andersen, Catherine L Smith, Caroline X Gao, Kate Filia, Magenta Simmons, Gina Chinnery, Eoin Killackey, Andrew Thompson and Ellie Brown in Australian & New Zealand Journal of Psychiatry
Footnotes
Authors’ Note
Catherine Smith and Caroline Gao are also affiliated to Monash University Public Health and Preventive Medicine, Monash University, Clayton, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.