
Abstract
Although current pharmacological treatments for psychotic illnesses are highly effective in achieving symptomatic remission, the recovering patient faces a number of complex issues as the psychotic symptoms subside [1–3]. These issues include the appraisal of the extent of recovery and the possibility of relapse, and of making sense of the illness episode and its treatment. These interconnected construals of the illness and its impact are potentially open to the influence of prior knowledge, personality, sociocultural influences, illness experience and psychoeducational messages that are delivered by the intervention team [3–7]. The outcome of these construals can have a significant effect on how the patient reacts to the illness and may consequently have an impact on the future course and outcome of the illness [4],[7–11].
In the early stages of psychosis, patients are confronted with an illness experience for the first time, and the optimal consideration of illness-related issues is crucial [10]. Contemporary programs for early psychosis often incorporate a significant component of psychoeducation and psychological intervention [12–14]. These approaches open up the possibility for a more refined assessment and management of experiential issues in the recovery period after a first psychotic episode. However, there is currently a lack of systematic knowledge in this important area. In previous research, most of these issues have been considered narrowly in separate domains such as insight or compliance [15] and are often oriented towards the perspective of the clinician, rather than that of the patient [16].
A patient's appraisal of their own illness experience has often been studied under the umbrella term of ‘insight impairment’. Until recently, insight impairment has been considered from the relatively narrow clinician-centred perspective as being a symptom of psychotic disorder, but more recent approaches to insight impairment have recognized its multidimensional nature [17–19]. Most of the recent rating scales address domains such as the awareness ofsymptoms, the attribution of illness and the attitude towards treatment. These assessments, however, define insight as a state of knowledge or appraisal and underemphasize the process by which such an appraisal is made, or to what extent information is actively sought and considered. An emphasis on ongoing processes, as opposed to a static outcome, would be more relevant in the understanding of how patients come to an appreciation of their illness during the early stages of a psychotic disorder.
Closely related to the understanding of an illness are the understanding and experiences of treatment. Currently, most assessments of attitude to treatment emphasize the measurements of side-effects [15], [20]. Psychoeducational approaches to enhancing patient understanding of treatment are often based on health-belief models that emphasize rationalist assumptions of the relationship between knowledge, belief and behaviour [21]. These approaches fail to recognize the importance of non-rational heuristic factors, such as the relationships between patients, carers and clinicians, in shaping the patient's experience and attitudes toward treatment. The implications of continuing medication after the first episode are also not well addressed.
There are other aspects of recovery from early psychosis that are not well covered by existing assessments and research, but which are nevertheless extremely important in shaping the response and reactions of patients to their illness, especially after the first psychotic episode. For instance, the patient's own judgment of the extent of their recovery, and the basis upon which this judgment has been made, are important issues that need to be considered in the formulation of a management plan. Likewise, the patient's appraisal of the risk of relapse and the action that might be taken in the event of a relapse, are significant issues that all recovering patients must face. Importantly, although underrecognition of the impact of an illness may lead to non-adherence, awareness of the full implications of an illness could overwhelm the coping capacity of the patient, which results in demoralization and feelings of hopelessness [22].
Currently, the systematic assessment of these interconnected domains is difficult. Established instruments usually focus narrowly on one of these domains in isolation [23], [24] and assessments are often constructed from the conceptual perspective of the clinician, rather than the patient. In addition, few of these instruments are specifically designed for people who are recovering from a first-episode illness [25]. As the issues that confront a patient early in the course of an illness are potentially different from those that confront chronic patients, these generic instruments may not be capable of emphasizing the issues that are of particular relevance in early psychosis. We aimed to develop a pragmatic assessment instrument, the Psychosis Recovery Inventory (PRI), which addresses these significant issues in the recovery stage of early psychosis. The themes of the instrument are generated from the accounts of patients and the instrument is comprehensive and addresses the relevant domains. Finally, to be more widely applicable, the instrument is self-administered and has a low administrative burden. We describe the development and validation ofthis instrument and present the initial results from the application of the instrument to a sample of recovering first-episode patients.
Method
Development of the Psychosis Recovery Inventory
Aims and target domains of the inventory
The PRI aims to assess a range of related experiences and attitudes in patients who are recovering from a first psychotic episode. These issues include perceptions of the illness and its treatment, and the appraisal of the extent of recovery and the risk of relapse. The inventory is not intended to measure symptom levels or side-effects, nor is it to be used as a specific tool for the measurement of narrowly defined ‘insight impairment’. It is also not intended to assess a broader sense of self-efficacy or psychosocial wellbeing. The aim of the inventory is to address a number of illness-related issues with which patients are confronted upon their recovery from the psychotic state and emphasizes their mutual interdependencies.
Item pool generation from qualitative interviews
The first step in the generation of a pool of items for the inventory involved a series of qualitative interviews with patients who were recovering from first-episode psychosis (n = 20). Patients were recruited from an early psychosis clinic, with illness durations of not less than 6months and not exceeding 2 years. They were diagnosed with schizophrenia according to the DSM-IV. These interviews were conducted using openended questions that encouraged the patients to reflect on aspects of the illness experience that they regarded as being significant in the recovery period. The interviews were transcribed. The transcriptions were studied for notable themes by an experienced clinician (E.Y.H. Chen). Potential items were identified from these themes and were formulated as statements. Care was taken to express these statements in clear, simple and relevant language. Forty-two items were generated in the initial pool, which then underwent translations between the English and Chinese versions. The validation was carried out based on the Chinese version.
After the generation of the pool of items, they were screened by two experienced clinicians for face validity. Theywere then offered for trial administration to patients, during which detailed feedback on the understandability and ease of use of the instrument was obtained. Items were evaluated for their clarity and specificity (i.e. they should not be open to many alternative interpretations); their length (longer items were shortened or removed); and their reading difficulty level (i.e. items that were found to be difficult to understand by patients were revised or discarded). In the initial stages of item construction, an attempt was made to formulate both positively and negatively worded items. However, even at the early pilot stage it was clear that for most patients the reversal of item polarity created considerable confusion. Subsequently, only positively framed statements were included. In addition, items in which patients tended to rate at one extreme were discarded and items with a poor test–retest reliability (an intraclass correlation of lower than 0.4) were also excluded.
Structure of the Psychosis Recovery Inventory
The final version of the PRI consists of 25 core items. Each item consists of a declarative statement to which a six-point Likert scale is applied that ranges from 1 (‘strongly disagree’) to 6 (‘strongly agree’), avoiding a neutral midpoint. Apart from the core items, there are two quantitative items that are measured by visual analogue scales, which address the perceived extent of recovery and perceived risk of relapse. There are also two sets of follow-up questions, one set addresses ‘misattributions for abnormal experiences’ (in case an abnormal experience is acknowledged) and the other set concerns ‘the perceived nature of non-recovery’ (in case non-recovery is perceived).
Validation study
For the assessment of convergent validity, we used two concurrent measures. Respondents were required to complete the Drug Attitude Inventory (DAI) and their clinicians completed the core items in the Scale to Assess Unawareness of Mental Disorder (SUMD) [19] on the same day. The SUMD assesses the patient's awareness of the mental disorder, the social consequences of illness and the effects of medication. The DAI addresses the thoughts of patients toward medication and the experiences they have had in taking antipsychotic drugs [20]. The test–retest reliability was evaluated by administering the PRI twice to the reliability study sample (n = 20) within 2–4 weeks. Although we understand that subjective appraisal about the illness can be subjectd to gradual changes over a longer time span, but we do not expect marked fluctuationover the test–retest interval.
Subjects
The validation study involved 48 outpatients who were attending the early intervention service at the Queen Mary Hospital and the Pamela Youde Nethersole Eastern Hospital in Hong Kong. These patients were diagnosed with schizophrenia according to DSM-IV, with an illness duration of not less than 6 months and not exceeding 2 years. They were judged to be competent to complete a self-administrated questionnaire. Patients with moderate to severe learning disability and comorbid substance-induced psychosis were excluded from the study.
Data analysis
Statistical analysis was carried out using the Statistical Package for Social Science (SPSS)V 12. The psychometric properties of the PRI items were explored by studying the distribution of the raw scores in each item in the inventory. Items in which subjects tended to score at one extreme were considered less useful. Factor analysis was carried out for each of the major domains (appraisal of relapse and recovery, reaction to illness and reaction to treatment) to explore the underlying structure of the instrument. The internal consistency was assessed by Cronbach's alpha for the instrument as a whole and its major domains. The intraclass coefficient was used to assess the test–retest reliability. The relationship between the DAI scores, SUMD scores and the relevant parts of the PRI were explored by correlation analysis.
Results
Subjects
Two patients refused participation since they did not regard themselves as suffering from any illness. Three other patients were excluded because of their low level of cooperation in completing the questionnaire. The sample consisted of 48 subjects with a mean age of 22.9 years (SD = 4.4). There were 27 men and 21 women. The education level was 11.9 years (SD = 2.4). The sample did not differ from the overall clinic population in terms of age, sex and education level (t-test and χ2 tests, NS) The mean duration of illness was 19 months (median 18 months), with a mean duration of untreated psychosis of 475 days (median 185 days). Eleven female and 9 male patients with a mean age of 22.3 years (SD = 4.4) participated further in the test–retest reliability study. The mean test–retest interval was 3 weeks. The subjects who took part in the study also participated in a more extensive first-episode study. The study was approvedbythe local ethics committees and all of the subjects gave written informed consent.
Descriptive results
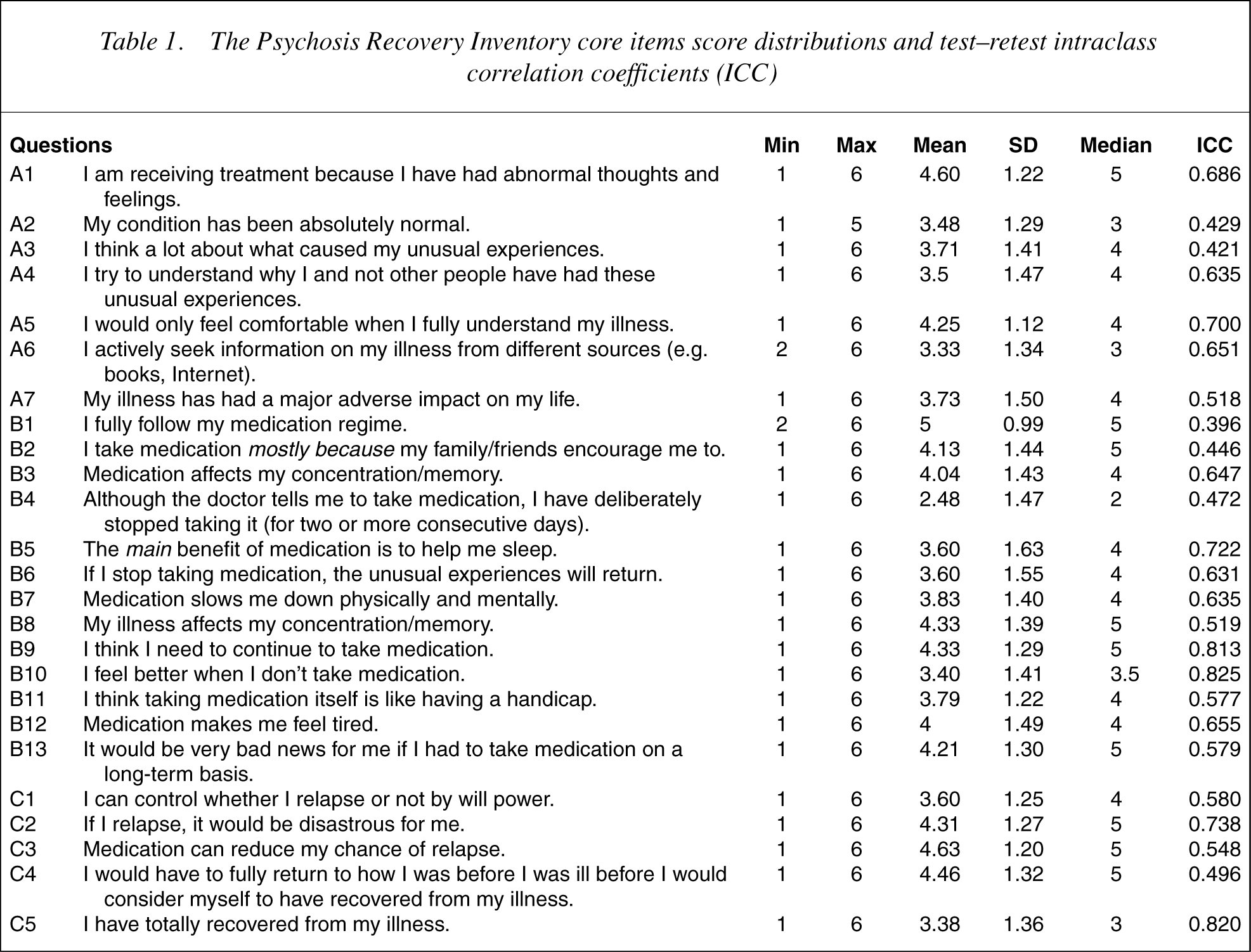
For each of the core items, the mean score, standard deviation, range, median and mode are shown in Table 1.
The Psychosis Recovery Inventory core items score distributions and test–retest intraclass correlation coefficients (ICC)
Perceived extent of recovery
Approximately 10% of the subjects considered themselves to have made a full recovery. Half the patients regarded themselves to have made a good recovery of 75% or more. Seventy-one per cent considered themselves to have made a recovery of more than 50%, and 19% of subjects regarded themselves as having made a limited recovery of less than 50%. Subjects who considered themselves to have made a less than full recovery rated four potential reasons for their non-recovery. The average scores on the six-point scale are as follows: ‘cognitive dysfunction’ (4.36, SD = 1.24), ‘social functioning impairment’ (3.24, SD = 1.42), ‘occupational functioning impairment’ (3.60, SD = 1.46) and ‘need to continue with medication’ (4.56, SD = 1.00). Significantly higher ratings were given for ‘cognitive dysfunction’ and ‘need to continue with medication’ as the major reasons for perceived non-recovery (repeated measure anova, df = 3, F = 16.1, p< 0.001).
Perceived risk of relapse
A majority of the subjects, 76.5%, judged their risk of relapse to be half or less than half, 52% regarded their risk of relapse to be 30% or less, and 20% considered that they were not at risk of relapse at all. The subjects were divided into two groups according to their perceived risk of relapse. When those who perceived their risk of relapse to be less than 30% (n = 25) were compared with the rest with regard to their scores on the PRI core items, they were found to have significantly less cognitive problems (Mann–Whitney U-test, z = −2.55, p = 0.011), had exercised less effort in understanding their illness(z = −3.36, p< 0.001), had perceived less impact of their illness (z = −2.07, p = 0.039) and reported more control over relapse and recovery (z = 3.03, p = 0.002). A similar profile is obtained for those who perceived their risk of relapse to be less than 50% (n = 27).
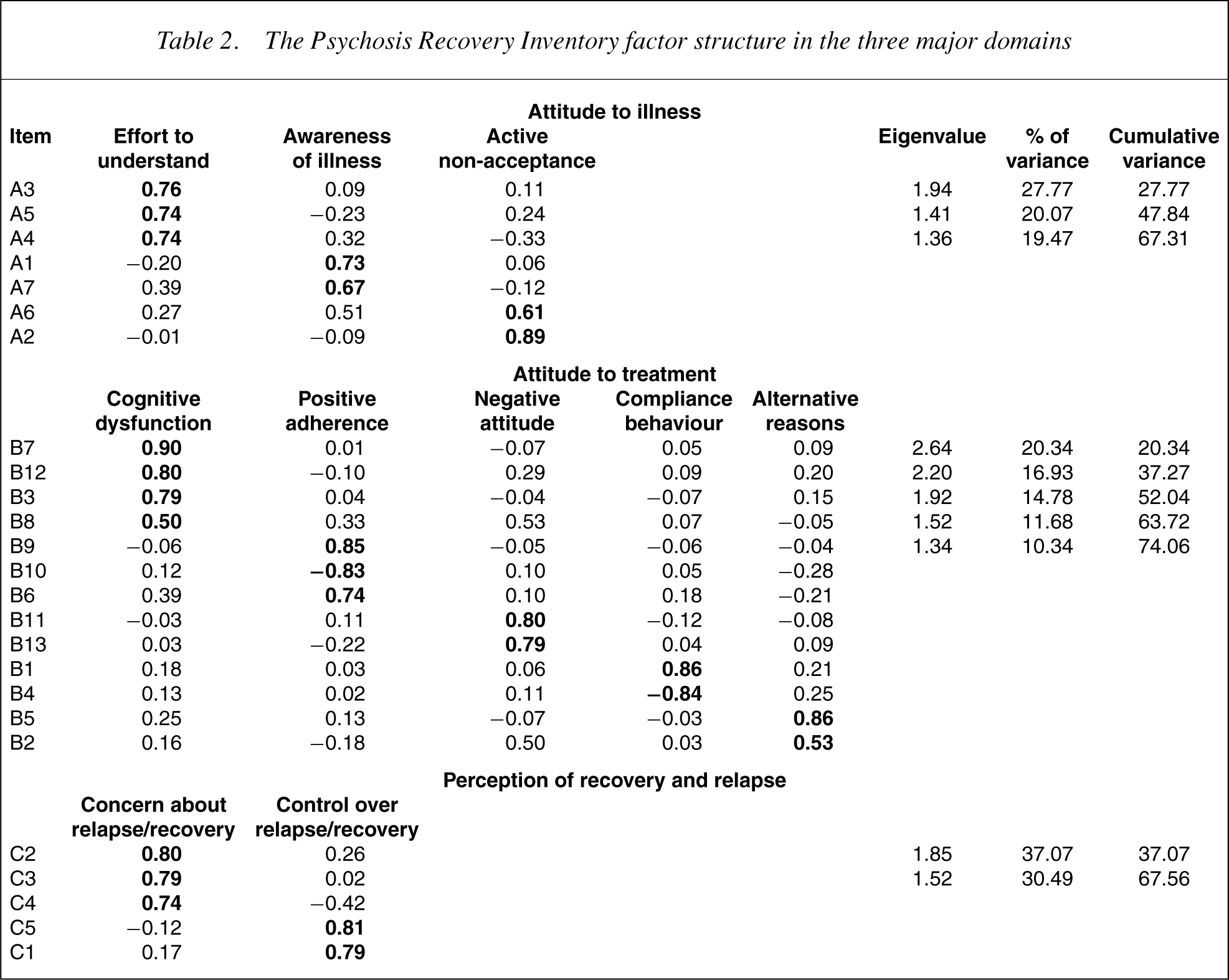
Factor structure ofthe Psychosis Recovery Inventory
A factor analysis (principal component analysis with varimax rotation) was carried out on the items in each of the three major domains in the inventory. For the ‘attitude to illness’ domain, three factors with eigenvalues greater than 1 emerged, which accounted for 67.3% of the variance. The ‘attitude to treatment’ domain was segregated into five factors and accounted for 74.1% of the variance, and in the ‘perception of recovery and relapse’ domain, two factors accounted for 67.6% of the variance (Table 2).
The Psychosis Recovery Inventory factor structure in the three major domains
Test–retest reliability
The intraclass correlation coefficients for the subscales ranged from 0.54 to 0.87, with a mean of 0.70. The test–retest intraclass correlation coefficient for the visual analogue scale items was 0.73 for perceived risk of relapse and 0.84 for perceived level of recovery.
Internal consistency
The Cronbach's alpha coefficient over the entire scale was 0.79.
Convergent validity
The misattribution subscale of the PRI showed a modest correlation with the SUMD (r = 0.280, p< 0.05). Subjects were divided into those who had impaired insight (SUMD score < 6) and those who had unimpaired insight (SUMD score = 3). The group with unimpaired insight was found to score significantly lower on the PRI misattribution subscale (mean = 1.36, SD = 2.31) than the group with impaired insight (mean = 2.82, SD = 1.74) (t = − 2.413, p < 0.05).
The correlation between the PRI treatment domain subscale scores and the DAIwas explored using correlation analysis. The positive adherence scores were correlated with the DAI scores (Spearman correlation coefficient = 0.482, p< 0.001).
Discussion
The PRI was developed and validated with the aim of capturing a range of interrelated attitudes and perceptions of patients who are recovering from a first psychotic episode. Most of the target areas are not systematically covered by existing rating instruments.
The construction of the PRI was based on first-hand material that was obtained from qualitative interviews with recovering patients. This method of item generation enabled the formulation and inclusion of items that are perceivedto be important by patients, and also enabled the items to be expressed as statements in a form that closely matches the way in which the patients themselves would articulatethem. This proximity to the perspective ofthe patient is a distinctive orientation of the PRI.
The PRI was conceived and developed as a self-administered questionnaire. Self-administration has several advantages. Apart from the low administrative burden, the subject is under less pressure to give socially desirable responses. The scale is also less dependent on the judgment and interview style of the rater. The construction of a self-administered scale, however, is more demanding in that items must be free from any possibility of misinterpretation. This requirement resulted in the extensive process of item selection, revision and testing that was employed in the construction of the PRI. The PRI can be conveniently completed by most patients in 10–15 minutes. It is supposed to be administered to patients in whom positive symptoms have largely subsided. It is not designed to replace instruments that are used in the assessment of more narrowly defined areas, such as insight.
The PRI had a good test–retest reliability over a 4-week period. A comparison of the DAI with the relevant items in the PRI provided convergent validity data. The PRI and SUMD target different domains. The SUMD is clinicianrated and targets the awareness of symptoms, and the PRI is self-administered and emphasizes the process of information-seeking.
One technical difficulty was experienced in the construction of the items. The normally desirable practice of including both positively and negatively framed questions to avoid acquiescence [26] was not feasible with this inventory, as the subjects generally found negatively phrased statements confusing to rate. This constraint resulted in our decision to present the items in a simpler positive framework. An examination of the item scores did not reveal a responding tendency that was suggestive of excessive acquiescence.
Although the use of a self-rated questionnaire necessarily involves a degree of bias in favour of patients who are cooperative and insightful, the extent of the bias is probably limited as only a small number of subjects declined participation because of impaired insight. In addition, the validation sample size (n = 48) is relatively modest in relation to the factor analysis procedure for the ‘attitude to treatment’ subscale, which contained 13 variables. The factor structure of the PRI should be explored with future studies involving additional samples from different populations.
The PRI is an efficient, reliable and valid instrument for the assessment of issues that confront patients upon recovery from an initial psychotic episode. These include the way in which the patient perceives abnormal experience and its treatment, and the appraisal of the risk of relapse and extent of recovery. The PRI enables clinicians to understand the perceptions of the patient in these interconnected domains, and makes possible the systematic exploration ofthese relationships in clinical practice and future research.