
Abstract
Objective
As part of a strategy to consider the options for preventing the developmental entrenchment of expressed emotion (EE), we examine the early ontogeny of EE in a first-episode sample of individuals with psychosis and its links with the process of adaptation to change.
Methods
The key relatives of 50 first-episode psychosis patients from two locations were interviewed soon after patient referral and again 9 months later using measures of expressed emotion and loss.
Results
The developmental pathways of components of expressed emotion, particularly criticism and emotional over-involvement, were independent despite having a similar effect on outcome for patients. Initially, high levels of emotional over-involvement were reduced by follow up, with 37% resolving into high criticism. Overall expressed emotion status changed in 28.2% of key relatives (all parental), predominantly from high to low. High emotional over-involvement and low criticism are associated with significantly high levels of perceived loss in relatives. The metamorphosis of emotional over-involvement to criticism was linked to a reduction in perceived loss.
Conclusions
Expressed emotion is not a stable index in relatives of first-episode psychosis samples. Appraisals of loss by relatives may be driving high emotional over-involvement with implications for family intervention programs. Attachment theory may help to explain some of the processes underlying resistance to change in some of the high-EE behaviours measured by expressed emotion.
Research into expressed emotion (EE) is now well into its fourth decade with a large body of work continuing to emphasise a robust association of high EE in carers and relatives with poor outcome in patients for numerous organic and psychological health problems [1–3]. Despite this understanding, comparatively little emphasis has been placed on tracing the separate developmental pathways of criticism and emotional over-involvement (EOI) for the purposes of targeting early intervention and support. Although EE is taken to reflect fairly stable qualities in individuals for intervention purposes, the high percentage of change in EE status over relatively short periods of time reported in many studies [4] does provide cause for thought. This phenomenon can be partly explained by noting that most of the EE studies have assessed relatives while the patient was either in the midst of or had very recently been in a state of psychosis, and the prevailing reactions at this time may reflect some enduring characteristic of relatives' coping responses to a breakdown in a family member.
Expressed emotion as a clinical concept has three components that are predictive of outcome: (i) emotional over-involvement, a breakdown of the natural boundaries in the family situation; (ii) critical comments (CC), critical attitudes and condemnation of behaviours in the patient by carers; and (iii) hostility (H), which involves a generalisation of criticism of the patient's personality and/or elements of rejection on the part of carers. Family intervention studies have shown that if the frequency of critical, over-involved and hostile interactions can be reduced, this leads to a secondary reduction of the risk of relapse over time [4,5]. To assume that high EE is a stable factor built into families would allow us to direct standard interventions at ‘critical periods’, however, the evidence suggests that EE is unstable, particularly during the early phase [4,5]. For this reason it is therefore important not to simply see EE as a risk factor in itself, but rather as the outcome of an adjustment and adaptation process, which needs to be appropriately modelled.
It has been found that, even within chronic populations, EE is not stable over time. Kuipers and Scazufca found that 36% of patients had changed EE status over 9 months and even more over a longer period of time [6]. Examining the ontogeny of EE, they also found that changes in EE were linked to changes in subjective burden and perception of clients' functioning. The idea that EE is not a trait characteristic but a thermometer of patient and relative transactions at a particular point in time is important for what happens after the onset of the first psychotic symptoms and, therefore, also for what happens before the first presentation [7].
Existing family intervention methods, designed as they were for use with families experiencing longer-term psychosis in a relative, appear less useful in first-episode samples. A study of behavioural family therapy in first-episode psychosis found no impact on relapse and for some families it actually increased distress [8]. Expressed emotion in first-episode samples seems to be particularly mutable and this may be considered to be a critical period for adjustment before EE response styles are established, which makes it an ideal period to prevent the entrenchment of high-EE behaviours.
Emotional over-involvement and criticism
Hooley has suggested that emotional over-involvement and criticism are both strategies reflecting a common need to control the home situation [9]. Critical and hostile statements, often directed at behaviours thought to be under the control of the patient rather than illness-caused [10], are perhaps more clearly understood than the processes underlying high EOI. Criticism is seen in both spouses and parents of patients with schizophrenia, while EOI is more often seen in parents. Emotional over-involvement has been more often linked to poor premorbid functioning [11,12] and burden. Bentsen et al. found that anxiety and depression were more prevalent in households where there are high levels of EOI displayed [13]. Stirling et al., looking at a first-episode psychosis sample, contradict many of the previous findings concerning the association of high EE with relapse rates, but are in agreement with a model that takes reactive components of the patient/illness/relative dynamic into account [14,15]. They found that a very large proportion of their high EE group reached threshold in EOI (14/16) at index but this was greatly reduced by follow up. Kavanagh writes:
In an interactive model, patients' symptoms and other problem behaviours elicit frustration, distress and concern from other people, and prompt attempts to cope. Unfortunately, these attempts at coping sometimes involve critical or intrusive interactions. The resultant negative emotions exacerbate patients' symptoms and make it more difficult for them to function effectively. [3]
Loss and grief as a response to severe mental illness
Miller examined the role of loss in relatives of individuals with serious mental illness and found that grief is a key reaction, with many relatives longing for a return of the quality of their former relationship with their ill relative [16,17]. Miller used a modified version of the Texas Revised Inventory of Grief [18] to measure levels of grieving that relatives of individuals with severe mental illness were experiencing. He found levels of grief similar to those displayed by recently bereaved individuals even years after the family member had first become mentally ill. Miller speculated that such high levels of grief may be due to
… the difficulty some relatives had in identifying and openly talking about their loss either because of the stigma of mental illness or because of the abstract nature of ‘psychic loss’ in which the person lives on but the relationship changes profoundly [16]
and suggests that the grief that needs to be addressed in this population is resulting ‘from the loss of specific hopes and aspirations rather than loss through death’. Clearly, the perception of loss will interact with the prior level of attachment or bonding between relative and patient.
Birchwood has argued that the perception of loss and change may be a prime motivator of criticism and EOI, starting before the formal onset of positive symptoms [4,5]. The longitudinal links between criticism and EOI observed by Stirling et al. might suggest that criticism is a coping strategy to deal with the pain of loss [16]. This explanation is entirely consistent with attachment theory. Bowlby argued that criticism is an ego-involving response to bring the errant individual ‘back into line’ through an activation of attachment behaviours [19,20].
Sample characteristics
Descriptive characteristics of patients and relatives are shown in Table 1. Patients and relatives were selected at the time of the patient's first presentation for acute psychosis conforming to ICD-10 schizophrenia or a related disorder. Patients were recruited from acute hospital admissions and direct referrals to home-treatment teams in the North Birmingham and Gloucestershire health regions. Inclusion in the study was requested if they had lived with or had been in regular contact with their relatives for one of the 3 months prior to admission; had engaged with the health services for the first time for the treatment of psychosis; and had no comorbid major neurological disorders. Fifty patients and 50 key relatives were initially recruited, with six relatives refusing to participate in the follow up, two patients and one relative having left the area and a further two patients not returning to the relatives' household, leaving 39 relative/patient pairs. The drop-out group did not differ significantly from the remainder on demographic measures or symptom indices.
Descriptive characteristics of patients and relatives (n = 39)
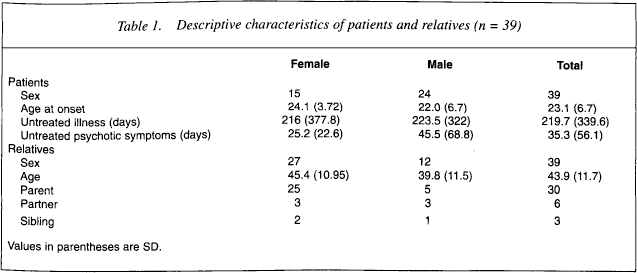
As shown in Table 1, 30 of the relatives were parents (77%), of whom 17 represented single-parent households. The remaining relatives were six partners (15%) and three siblings (8%). The patient sample included white (28; 72%), Asian (6; 15%) and black/mixed race (5; 13%) individuals.
Assessment
The EE levels of the relatives were assessed by using the Camberwell Family Interview (CFI) [21]. All interviews were carried out either in the family home or in a mental health centre and relatives were rated as high in EE if they scored 6 or higher in the criticism (CC) subscale; 3 or higher in the emotional over-involvement (EOI) scale or had any score for hostility (H). Follow-up interviews were carried out 9 months after first testing (median = 9.5 months). The expressed emotion ratings of the relatives were assessed by a researcher trained to reliability in rating the CFI. A sample of interviews were also rated blindly by another trained CFI rater with acceptable levels of reliability.
Loss was assessed in relatives and patients by using the mental illness version of the Texas Inventory of Grief [16,18], a two-part questionnaire measuring initial reactions at the time of loss and levels of ongoing grieving. Demographic data were collected by using standard forms at interviews for both patients and relatives. Several other instruments were employed in the assessment procedure.
The majority of patients (34, 86%) returned to live in the family household for the duration of the follow-up period, with the other five remaining in high (several times weekly) contact with their key relative.
Results
Ontogeny of expressed emotion
Expressed emotion status at index and follow-up were significantly but moderately correlated (r = 0.48, P < 0.01), as were CC (r = 0.55) and EOI (r = 0.66) but not H (r = 0.13), suggesting considerable intraindividual change. The period of untreated psychotic symptoms for patients differentiated high and low CC relatives at first testing, with high CC relatives having longer reported exposure to untreated symptoms prior to medical intervention (low CC = 26.4 days, high CC = 75.4 days, F1,37 = 5.99, P < 0.05). No other differences were found in EE or subscale status for this or untreated illness measures.
There was a considerable change in overall EE status over the follow-up period, with 28% of the relatives obtaining a different EE rating from the initial measure (Fig. 1) and 42% of the initially high EE relatives resolving to low EE. The individual subscales of the CFI show clear differences in the resolution of EOI and CC over time. The rate of high EOI at first testing was 41% (n = 16) while 9 months later this had reduced to 18% (7) (Fig. 2).
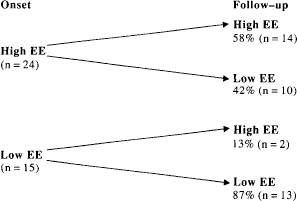
Stability and change in expressed emotion in first-episode psychosis
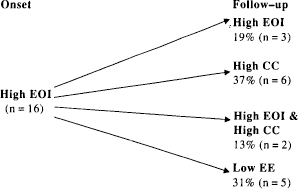
Ontogeny of relatives initially high in emotional over-involvement over 9 months
The number of participants rating above threshold for criticism also changed markedly over the 9 months with an initial group of 9 (23%) increasing to 12 (31%) over the follow-up period (Fig. 3).
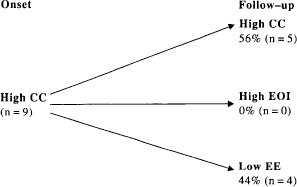
Ontogeny of relatives initially high in critical comments over 9 months
Loss appraisals
The present findings show a significant difference in loss perceived by relatives high or low in EOI (Fig. 4). Conversely, it was also found that those high in criticism had a lower appraisal of loss (Fig. 5). In those relatives where initial high EOI changed to high criticism (n = 6), loss appraisal has reduced significantly over time (t = 8.84, P < 0.001).
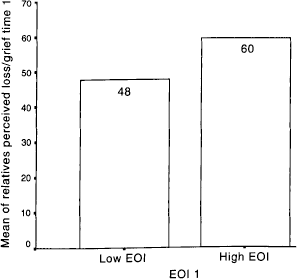
Comparison of present grief levels in relatives high or low in emotional over-involvement [t(1,37) = −3.571, P < 0.001]
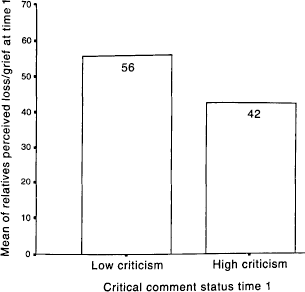
Comparison of present grief levels in relatives high or low in criticism [t(1,37) = 3.543, P < 0.001]
Discussion
The present findings suggest that, in the early stage of a psychotic episode, a significant proportion of key relatives will experience an emotional reaction to the appraisals of loss that can best be described as a process of grieving. This may generate some of the over-involved behaviours found in relatives high in EOI and may be particularly resistant to certain forms of family intervention. Miller suggests that, for these relatives, interventions containing specific grief work such as reminiscence and loss-accommodation may be more appropriate and beneficial in preventing long-term denial and distancing that, for a proportion of relatives, is likely to lead to the later entrenchment of critical attitudes [16,17]. Relatives experiencing initially high levels of grief in response to psychosis may be at a particular risk of ‘sealing-over’ [22] affective elements of the relationship with the patient and remaining distant. The other potential pathway would appear to be an ‘integrating’ response, where the loss is acknowledged but no distancing occurs. That the EOI response would seem to be specific to familial experiences of loss is supported by the observation that no above-threshold EOI was found in studies of EE in key workers of mentally ill patients in institutional settings [23,24]. Some of these processes can be understood from research that has examined the evolution of loss appraisals in response to illness, such as Burke et al., who differentiate chronic sorrow from pathological grief [25]. Chronic sorrow, a pervasive sadness, which, however, allows for functional behaviour and good reality testing, has been found in parents of mentally retarded children. This is occasioned by the chronic nature of the losses experienced and differs from acute grief, which is time-limited. The experience of psychosis within a family holds many similarities to this as the cycle of relapse and wellness generate a continuing cycle of grieving. Eakes, in a small study, found that eight of ten parents of seriously mentally ill children suffered from chronic sorrow [26]. This would suggest a partial integration and acceptance of the loss leading to a capacity to function as well as possible under the circumstances and may mirror the level of functioning stability found in low-EE family members.
Bowlby has drawn attention to the pervasiveness of angry coercive behaviour acting in the service of an affectional bond, describing it as the behaviour seen when a mother, whose child has run foolishly across the road, berates and punishes him with an anger born of fear, or, in some families, when a member becomes angry whenever his approaches to another family member are met by an unresponsive silence [20]. If angry coercion is seen as a ‘natural’ adaptive response to discourage individuals from ‘stepping out of line’, it may help to explain some of the origins of high levels of criticism in studies of EE. Highly critical attitudes toward family members with psychosis have been associated with attributions of patients' responsibility for symptoms from relatives [10] as well as subjective burdens experienced by the caregiver [6]. If the patient does not recover over time, the coercive criticisms may be employed as an attempt to establish more normative behaviours. These can soon escalate into hostility if the hoped-for improvements do not occur. Bowlby suggests that dysfunctional anger occurs whenever people (children or adults) become so intensely and/or persistently angry with their partner that the bond between them is weakened instead of strengthened and the partner is alienated. Anger with a partner also becomes dysfunctional whenever aggressive thoughts or acts cross the narrow boundary between being deterrent and being revengeful. It is at this point, too, that feeling ceases to be the ‘hot displeasure’ of anger and may become, instead, the ‘malice of hatred’ [20]. Family interventions may need to take these critical ‘default’ mechanisms into account when attempting to reduce EE in family relationships. Perhaps the low-criticism relatives have simply reached the insight, either through empathy or experience, that coercive criticism does not work for the behaviours associated with psychosis.
If, as attachment theory suggests, a normal reaction to loss involves coercive anger or criticism, we might expect a resolution of EOI behaviour to criticism over a period of time, once some issues of guilt and insecurity [27] in the carer had been worked through. Using this model, we would expect that in most cases, the high EOI of relatives should gradually resolve into high-CC or low-EE responses and we should seldom see a low-EE relative change status to a high-EOI relative except where there is an acute deterioration in the patient's condition.
Contributing issues to the grieving process
The length of time over which grief processes may be occurring in families with an ill member can be vast. Davis and Schultz [28] detected grief in older parents of children with schizophrenia, for 43% of whom the duration of diagnosed schizophrenia was more than 10 years. Grief was conceptualised here as a cognitive, behavioural and emotional reaction to loss. This shows that the intensity of this process may be contributing to other family dynamics such as subjective burden and EE for much greater periods of time than previously realised. In a small qualitative study exploring the experience of caring for an adult child with schizophrenia, Tuck et al. suggest that the changed dynamics involve both the loss of an imagined, idealised child and a transformation of the physically present child into a needy stranger [29], which is emphasised by a finding that parents display significantly more warmth to well children and EOI to a schizophrenic child [30]. This may give some clue as to the protracted nature of the grieving response in carers, as it is not just the loss of a healthy child with associated loss of positive aspirations for the future but also, in periods of psychosis, the intrusion of a demanding ‘stranger’ who must complicate the intensity of the already traumatic experience.
Conclusion
An examination of the ontogeny of EE in first-episode samples with emphasis on the subscales of criticism and EOI can provide a deeper understanding of the processes involved in the development of high-EE behaviours in the relatives of individuals with psychosis. An appreciation of the influence that appraisals of loss and associated grief reactions can play in the establishment of new patterns of behaviour with the patient may help in the design and targeting of specific interventions for this period in order to prevent the entrenchment of high-EE behaviours in carers. Attachment theory allows us to recognise coercive criticism as an adaptive mechanism in response to an errant family member and may explain the lack of long-term effectiveness of some of the previous family intervention trials. Early intervention at this crucial stage is likely to show the greatest benefit for individuals with psychosis and their relatives in terms of long-term improvements in outcome.