
Abstract
Background
Ethylene glycol (EG) poisoning, if not diagnosed rapidly, can lead to poor patient outcomes. Gas chromatography (GC) is primarily used for EG quantitation which is rarely available, and the turn-around time may be prolonged. Most lactate results from point-of-care (POCT) methods are falsely elevated in EG poisoning compared with automated chemistry analyser results. In combination, the lactate gap (POCT-Automated chemistry) can be used as surrogate marker in just about all laboratories to indicate likely EG toxicity and guide treatment.
Case Report
A man presented by ambulance to hospital with severe agitation requiring mechanical ventilation to facilitate ongoing management. Venous blood gas analysis confirmed a high anion gap metabolic acidosis (HAGMA) with an elevated lactate. The lactate and osmolarity measured in the laboratory showed a normal lactate and high osmolarity, giving a large osmolar gap. The patient was immediately commenced on renal replacement therapy for presumed EG poisoning to minimize kidney injury, and the treatment continued for 19 hours. A very high EG concentration was confirmed by GC the next day.
Conclusion
An elevated lactate gap along with a HAGMA and osmolar gap can provide rapid surrogate laboratory data indicating EG poisoning enabling timely treatment and better patient outcomes.
Introduction
EG poisoning is an uncommon presentation posing a diagnostic challenge that requires prompt treatment with antidotal therapy (fomepizole and ethanol) and dialysis to prevent severe complications, renal failure, and neurotoxicity. Confirmation primarily by GC methods is very rarely available or unable to be provided in a timely manner; hence, widely available surrogate markers are utilized when managing likely EG poisoning. The CARE checklist guidelines were utilized in the write-up of the case in line with our local ethics approval HREC/14/QPAH/308.
Case history and results
Most Notable Pathology Results on Presentation.
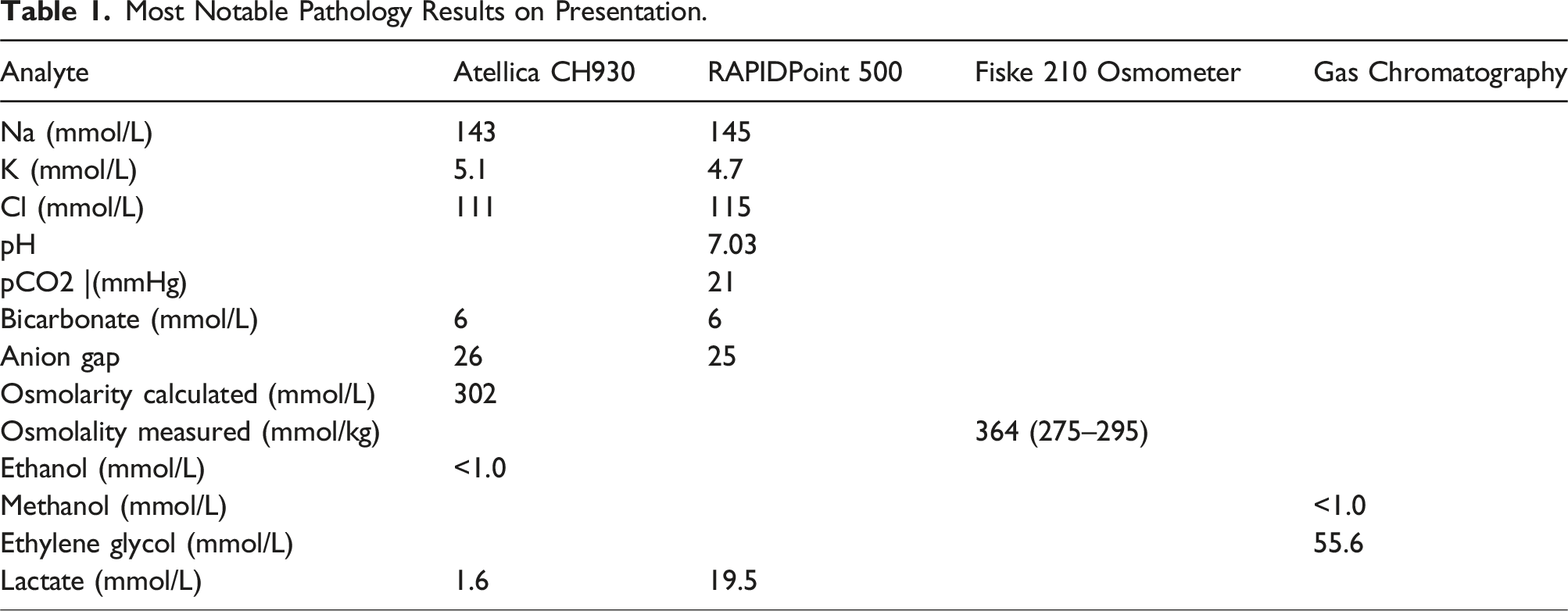
The remnant of the first laboratory serum sample was analysed for lactate on three POCT systems: i-Stat (Abbott Diagnostics, East Windsor, NJ, USA), RAPIDPoint 500 (Siemens Healthineers, Tarrytown, NY, USA), and ABL 835 (Radiometer, Bronshoj, Denmark), and re-analysed on the Atellica CH930 automated chemistry analyser (Siemens Healthineers, Tarrytown, NY, USA). The results were i-Stat 8.7 mmol/L, RAPIDPoint 500 23.0 mmol/L, ABL 835 25.0 mmol/L, and the Atellica 1.7 mmol/L, indicating the POCT methods were not equally affected. During the treatment period, the POCT lactate decreased by ∼0.8 mmol/L (50 mg/L) per hour.
Discussion
Ethylene glycol, propylene glycol, and diethylene glycol are widely used as components of antifreeze and coolant solutions for automobiles. 1 EG has a sweet taste which can be ingested as alcohol substitute and self-harm agent or accidentally by children and animals especially if such fluid is left in open containers. EG is rapidly absorbed reaching peak level in blood at 1–2 hours post ingestion. 2 It is then metabolized by alcohol dehydrogenase and aldehyde dehydrogenase to glycolic acid which in turn is oxidized to oxalic acid which forms crystals with calcium in the kidneys leading to acute kidney injury. 3 Glycolic acid inhibits cellular uptake of oxygen, causing increase in lactate level leading to reduced pH. 2 The presence of glycolate, a toxic metabolite of EG, is known to interfere with POCT measurement of lactate producing artefactual elevation. 3
Treatment guidelines recommend decisions for extracorporeal treatment are based on EG concentrations, despite the availability of these being limited. Traditionally, dialysis was recommended when EG is >8 mmol/L (>500 mg/L) 4 ; more recently, the EXTRIP group recommends extracorporeal treatment combined with antidote when the EG concentration is >50 mmol/L (>3150 mg/L). 5 There are no direct EG methods or markers in blood or urine readily and rapidly available to measure the concentration. The presence of EG is reliant on biochemistry tests, clinical signs and symptoms, and potentially patient disclosure for timely and appropriate diagnosis and management. The most valuable biochemistry markers are the presence of a HAGMA, an osmolar gap (noting not all labs possess osmometers) that is not explained by ethanol and most significantly a lactate gap, where there is an elevated lactate by POCT methods but normal levels on automated chemistry analysers. 6 The artefactual elevation is due to cross-reaction from glycolate due to its structural similarity with lactate making it a very specific surrogate indicating EG toxicity. 6 Due to the very high EG concentrations in our patient, over a 28-hour period, 11 of 12 blood gas samples had a lactate gap >8 mmol/L. Laboratories should establish an acceptable lactate gap based on local verification/validation data between their POCT and general chemistry methods using normal samples. In our hospital, the acceptable difference in results between our own systems is <10%.
The POCT analysers utilize amperometric methods where
Not all POCT methods are equally affected. Karon et al. compared the i-Stat, Nova Lactate Plus analyser, and Radiometer ABL 725 blood gas analyser with two laboratory analysers Vitros and Roche Cobas Integra 400 analyser lactate methods (range tested 1–14 mmol/L) showing lactate concentration decreased on the Radiometer and i-Stat analysers but increased on the Nova in comparison with the laboratory assays. 7 Indrasari et al. reported similar findings where 7 of the results with lactate >8 mmol/L were significantly higher on the Nova pHOx blood gas analyser versus the i-Stat analyser. 8 Our observed difference in the serum sample lactate results confirmed the i-Stat results produce lower results even in the presence or absence of EG in samples. The differences in POCT methods are likely to be due to method differences, in particular the sources of lactate oxidase enzymes. Thus, it is recommended in suspected EG ingestion lactate be measured concurrently on the same POCT and laboratory methods until EG is ruled in or out and the patient is stabilized during treatment with fomepizole or ethanol (with a target of ∼25–40 mmol/L). 9 The META study estimated the apparent half-life of EG with fomepizole to be ∼20 hours. 10 This will allow for saturation of the alcohol dehydrogenase enzyme system while EG is dialysed. EG half-life is 3–9 hours, but with ethanol treatment, this can be extended to 17–18 hours 6 requiring prolonged treatment as was in our case, 19 hours. The AACT guidelines suggest ADH blockade should continue until ED is <20 mmol/L (<1260 mg/L) and the patient is asymptomatic with normal pH. 4
Conclusion
The lactate gap can be a strong surrogate, along with a HAGMA and osmolar gap, of EG poisoning. Due to POCT method differences in lactate concentration, it is important lactate is measured on the same POCT and laboratory methods throughout diagnosis and treatment. Equally, false lactate elevations with POCT can be observed due to other alcohols and/or medication containing propylene glycol.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
Not applicable.
Contributorship
Goce Dimeski, Amanda Holford, and Katherine Isoardi collected and analysed the data. Goce Dimeski wrote the manuscript.