
Abstract
Background
Most colorectal cancers (CRCs) occur in individuals aged over 50 years; however, the incidence in younger age groups is increasing. Diagnosis in younger patients is frequently delayed due to non-specific symptoms and the relative frequency of benign disease. There is a need to identify patients who warrant further investigation for CRC. This study reviewed whether a faecal haemoglobin (f-Hb) ≥10 μg Hb/g faeces measured by the faecal immunochemical test for f-Hb (FIT) was associated with CRC in a local primary care population aged under 50 years.
Methods
f-Hb results from symptomatic patients aged 18–49 years presenting to primary care during a 17-month period were extracted from local laboratory information systems. Colonoscopy lists were obtained from three local trusts. The Somerset Cancer Registry was searched to identify CRCs. f-Hb and outcomes were matched using NHS numbers.
Results
A total of 3119 patients were included (median age 41 years); 313 of 2682 patients with f-Hb <10 μg/g (11.7%) and 305 of 437 patients with f-Hb ≥10 μg/g (69.8%) underwent colonoscopy. Twelve CRCs were detected. At a cut-off of 10 μg/g, the positivity rate was 14.0%, sensitivity was 100% (75.8–100%), specificity was 86.3% (85.1–87.5%), positive predictive value (PPV) was 2.7% (2.5–3.0%) and negative predictive value (NPV) was 100%. At a cut-off of 150 μg/g, sensitivity was 83.3% (55.2–95.3%), specificity was 95.2% (94.4–95.9%), PPV was 6.2% (4.7–8.2%) and NPV was 99.9% (99.8–100%).
Conclusion
Our data supports the use of FIT to triage patients aged under 50 years presenting to primary care with symptoms suggestive of CRCs.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed cancer worldwide, accounting for 10% of global cancer incidence in 2020. 1 As with other cancers, the incidence of colorectal cancer increases with age, and 90% of cases are estimated to occur in individuals aged over 50 years. 2 While the absolute prevalence in younger age groups remains low, 3 a study from 2019 found significant increases in colorectal cancer incidence over a 10-year period in individuals under the age of 50 years in a number of countries including the UK, 4 where over 2500 people aged under 50 are diagnosed with colorectal cancer each year. 5 Bowel Cancer UK has highlighted this increasing health challenge with its ‘Never Too Young Campaign’ and the associated report launched in 2020. 6
Detection of early onset colorectal cancer (EOCRC), defined as diagnosis aged under 50 years, is challenging due to the non-specific nature of symptoms, which have a poor positive predictive value (PPV) for colorectal cancer in this age group, and the relative frequency of benign colorectal disease (e.g. irritable bowel syndrome, IBS) and other significant bowel disease (SBD, e.g. advanced adenoma or inflammatory bowel disease, IBD). Investigation of all symptomatic patients in this age group by colonoscopy is not possible, due to both the inherent risks of colonoscopy and the limits of colonoscopy capacity, which has decreased further in the wake of the COVID-19 pandemic. Alternative triage tests for CRC in this age group are therefore critical.
Faecal immunochemical tests for haemoglobin (FIT) are routinely used in colorectal cancer screening programmes around the world and in the UK are also recommended by national guidance to support the triage of symptomatic individuals presenting to primary care who may require further investigation to exclude colorectal cancer. 7 This guidance advocates the use of FIT in certain patients aged over 50; however, there have been limited studies looking at the performance of this test specifically in a younger population. Notably, a recent subgroup analysis of the NICE FIT study showed that in younger individuals FIT has a positive predictive value of 11.5% at a cut-off of 150 μg/g, with a negative predictive value (NPV) greater than 99.5%. 8 In light of this, more recent guidance has been published by the Association of Coloproctology of Great Britain and Ireland and the British Society of Gastroenterology, recommending the use of FIT in primary care to triage adults of any age with symptoms of suspected colorectal cancer. 9
This study aimed to review whether a positive FIT result (defined as faecal haemoglobin [f-Hb] ≥10 μg Hb/g faeces [ug/g]) is associated with colorectal cancer in symptomatic adult patients aged under 50 years presenting to primary care.
Materials and methods
Study population
All f-Hb results from within the Berkshire and Surrey Pathology Services network in the time period 1 June 2019–31 October 2020 were obtained from the Winpath Enterprise laboratory information system (LIMS). There were no restrictions on requesting in place throughout this time period. Data extracted included specimen date, clinical details, patient age, patient sex and the faecal haemoglobin result. The following results were excluded from the data analysis: patients aged under 18 years or 50 years old or older at the time of sampling, results from secondary care or health screening programmes and results from patients with no NHS number recorded. Results from military locations and Hounslow, South West London, or Berkshire West Clinical Commissioning Groups (CCGs) were excluded, as these locations were not likely to refer patients into the three local trusts (Royal Surrey Foundation Trust, Ashford and St Peters Foundation Trust and Frimley Health Foundation Trust) for which lists of colonoscopies and cancer diagnoses were available. Ninety-nine patients had more than one primary care f-Hb result in the time period, and all results from these patients were excluded (n = 205).
FIT analysis
F-Hb concentrations were determined by faecal immunochemical test on the OC-SENSOR PLEDIA analyser (Eiken Chemical Co. Ltd, Tokyo, Japan) at Royal Surrey County Hospital. Samples were collected by patients into manufacturer-specific FIT collection devices (OC-Auto Sampling Bottle 3, Eiken Chemical Co. Ltd, Tokyo, Japan) and returned to the laboratory, where they were stored at 2–10°C until analysis. The analytical range of the OC-SENSOR PLEDIA is 6–200 μg/g, which is extended to 50,000 μg/g by performing an on-board dilution.
Outcomes data
Lists of colonoscopies performed at the three local trusts in the time period 1 June 2019–1 November 2021 were obtained from the local colorectal cancer teams. Lists of colorectal cancer diagnoses in adult patients aged under 50 in the time period 1 June 2019–1 November 2021 were obtained from the three local Somerset Cancer Registries. This was designed to ensure that cancer diagnoses in patients not followed up with colonoscopy were also captured. Only diagnoses within 12 months of the FIT test were taken into account for the data analysis. Results, colonoscopies and diagnoses were matched using NHS numbers.
Analysis of data
Data was reviewed using Microsoft Excel. A cut-off value of 10 μg/g was used for positivity as per NICE guidance. 7 Wilson’s 95% confidence intervals (CI) for sensitivity and specificity, and Mercado-Wald 95% confidence intervals for positive and negative predictive values were calculated using Analyse-it (Analyse-it Software, Leeds, UK) and are given in brackets. Analyse-It was also used to perform receiver operating characteristic (ROC) curve analysis and generate an area under the curve (AUC). Results reported as >50,000 μg/g were treated as 50,000 μg/g for the statistical analysis.
Results
Demographics of patients tested
A total of 3119 patients aged under 50 had a FIT test in the time period 1 June 2019–31 October 2020. The median age was 41 years (interquartile range, IQR: 34–46 years, range: 18–49 years). Of the total number of patients included in this study, 1271 patients (40.8%) were male and 1848 (59.2%) were female. Figure 1 shows the age range of patients with an f-Hb result and the split between male and female patients at each age. Ages of patients included in the study population.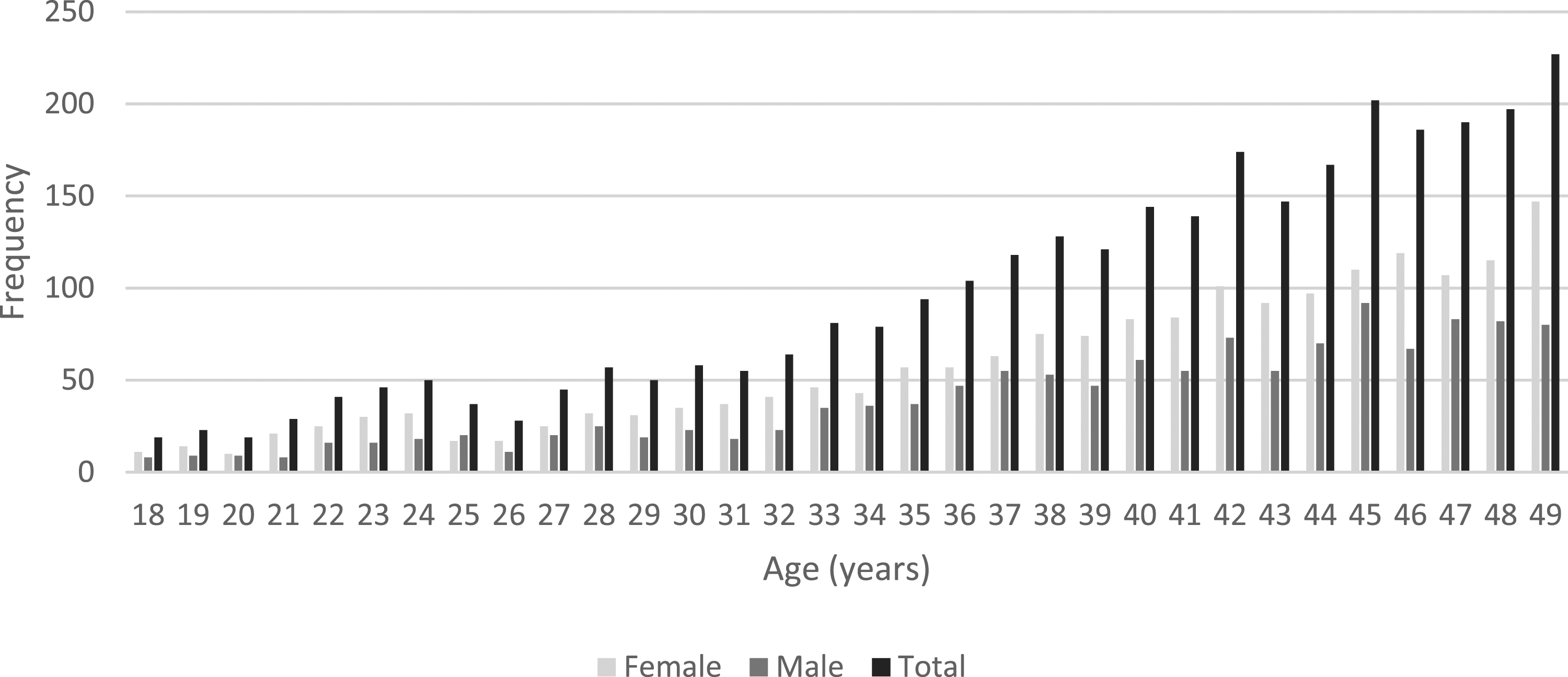
f-Hb results
A total of 437 patients (14.0%) had a positive f-Hb result (≥10 μg/g). Figure 2 shows the spread of f-Hb results ≥10 μg/g. The median positive result was 61 μg/g (IQR: 17–408 μg/g, range: 10–>50,000 μg/g), and the median age of patients with a positive result was 41 years (IQR: 34–45, range: 18–49). Spread of positive faecal haemoglobin (f-Hb) results included in the study.
Of all the patients included in the study, 618 underwent colonoscopy during the defined time period; 11.7% of those with a negative f-Hb result (313/2682) and 69.8% of those with an f-Hb result ≥10 μg/g (305/437). Outcomes are shown in Figure 3. Summary of clinical outcomes for all patients included in the study. SCR: Somerset Cancer Registry.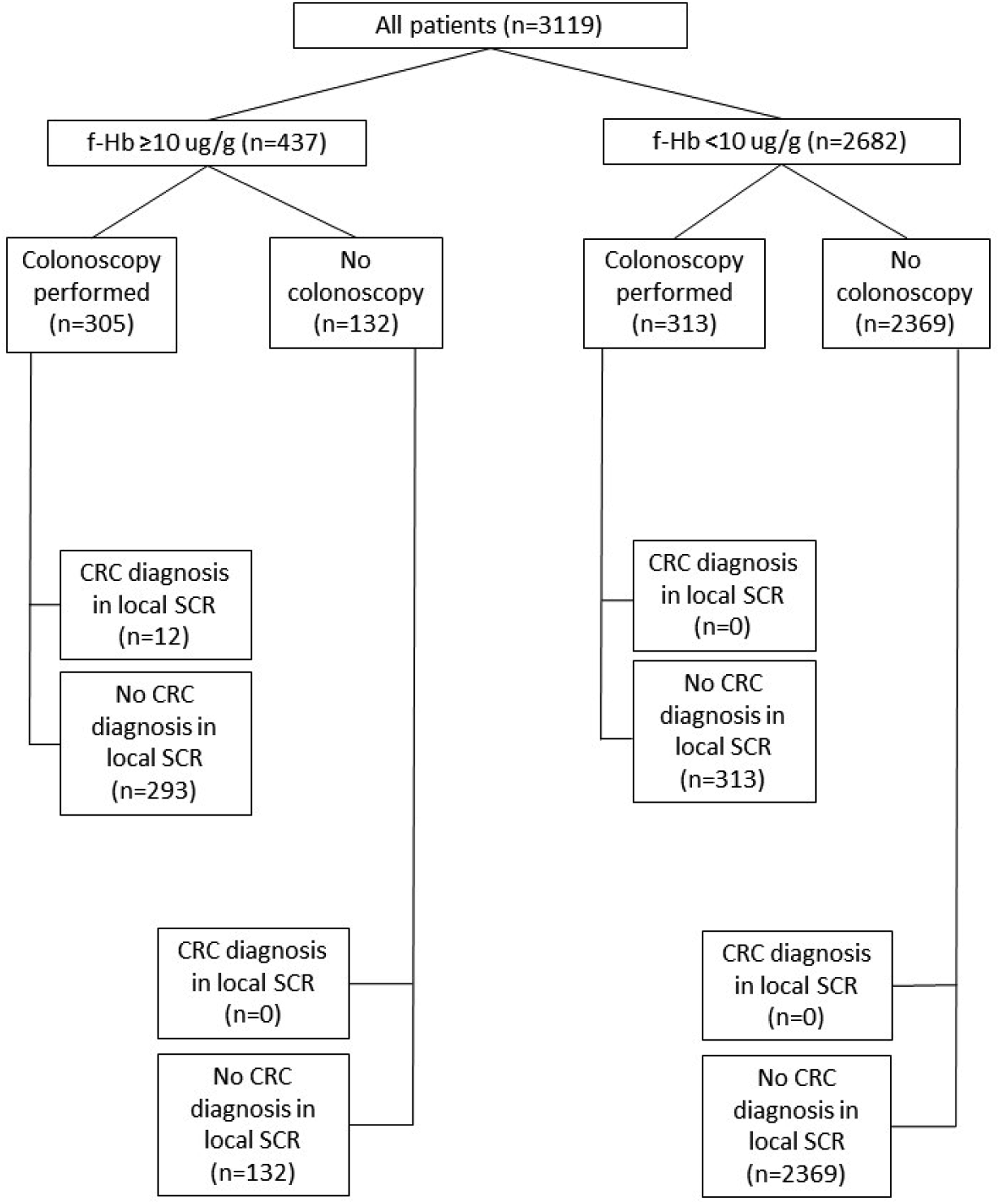
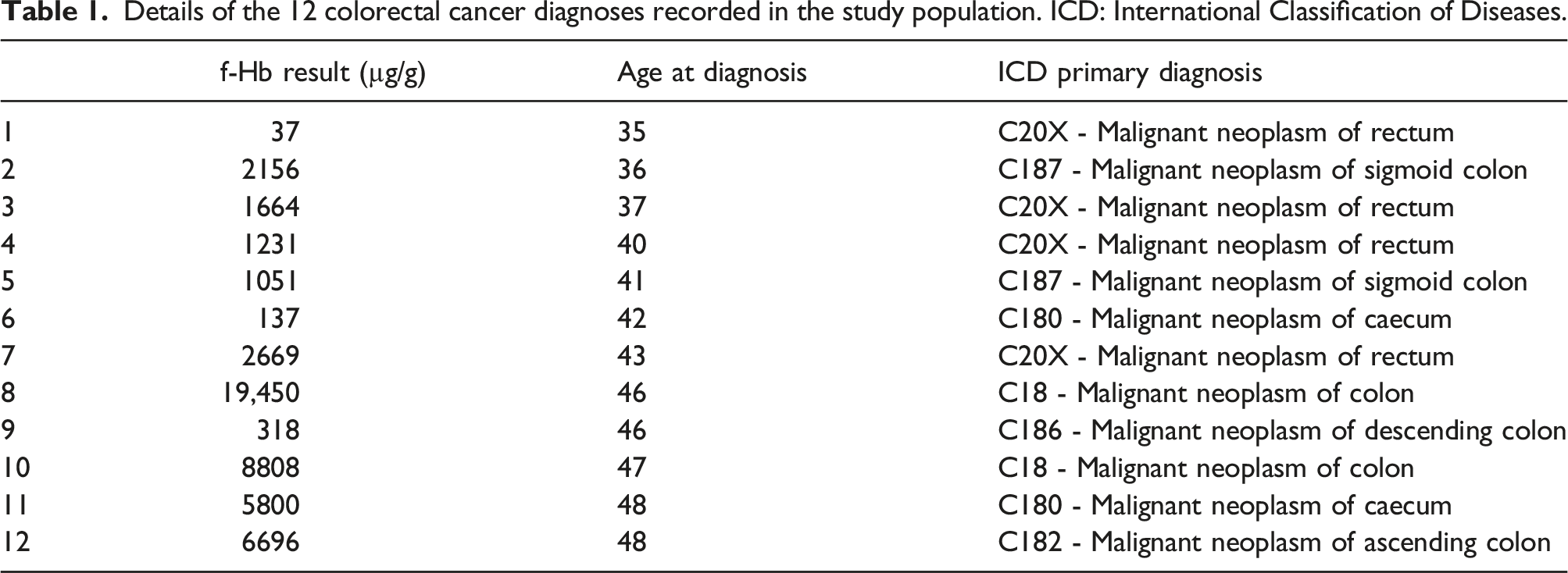
Details of the 12 colorectal cancer diagnoses recorded in the study population. ICD: International Classification of Diseases.
Based on the data from all 3119 patients with an f-Hb result, and a cut-off of 10 μg/g, sensitivity was 100% (95% CI: 75.8–100%), specificity was 86.3% (95% CI: 85.1–87.5%), PPV was 2.7% (95% CI: 2.5–3.0%) and NPV was 100%. ROC curve analysis gave an AUC of 0.885 (95% CI: 0.822–0.949) (Figure 4). Receiver operating characteristic (ROC) curve analysis.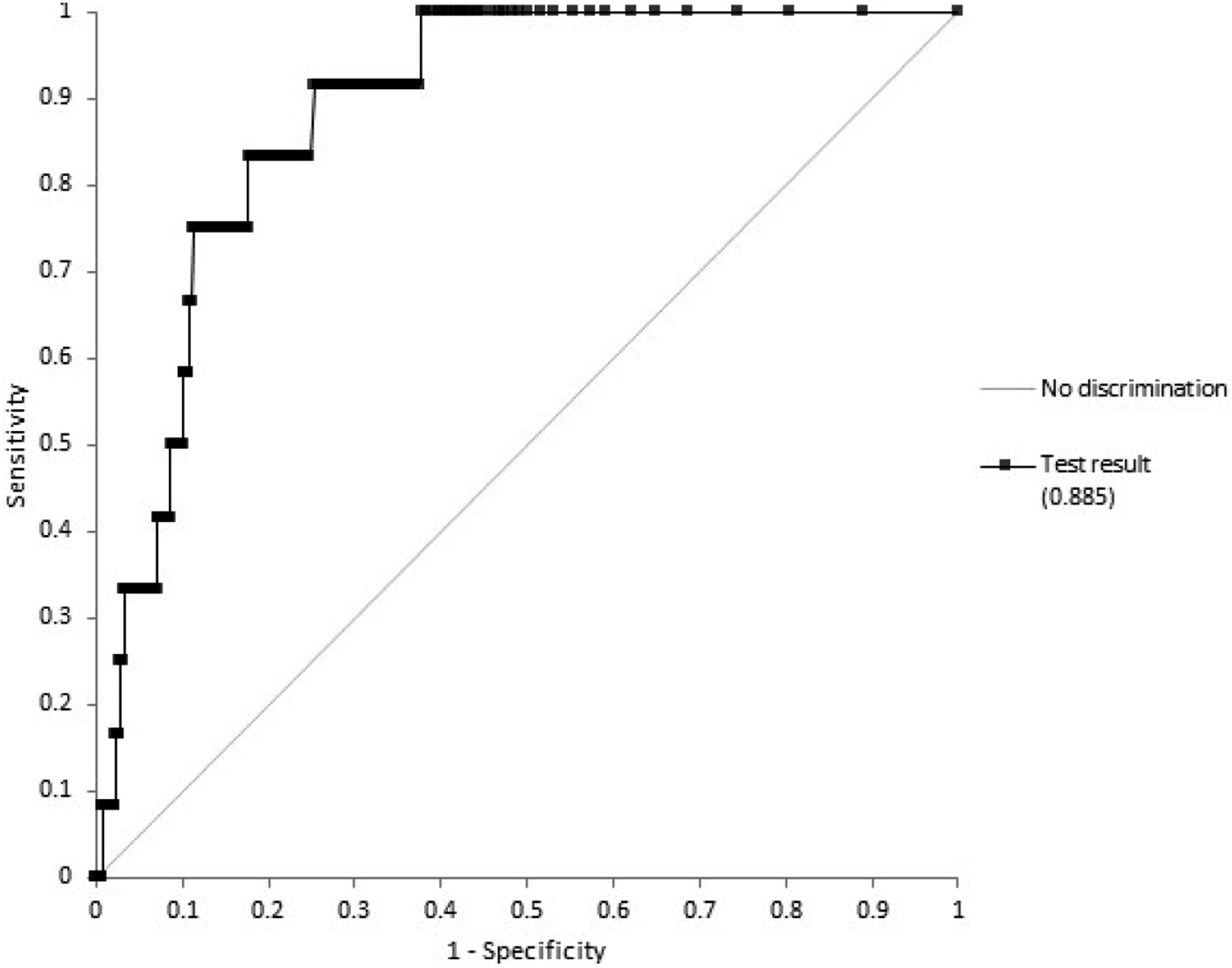
After re-analysis of the data using a cut-off for positivity of 150 μg/g, sensitivity was 83.3% (95% CI: 55.2–95.3%), specificity was 95.2% (95% CI: 94.4–95.9%), PPV was 6.2% (95% CI: 4.7–8.2%) and NPV was 99.9% (95% CI: 99.8–100%).
Discussion
This retrospective service evaluation demonstrates that in our local population, FIT has frequently been requested in adult patients under the age of 50 years old. The frequency of requests increased with age, and a majority of those investigated were women; these demographics were similar to the population in another study looking at the use of FIT in a symptomatic population aged under 50. 8 This study also reported a positivity rate of 19.2% in patients aged under 50, which is similar to the 14.0% reported here. The rates of referral for colonoscopy seen here were similar to 3 month referral rates reported by another service evaluation looking at symptomatic patients aged 50 and over (11.7% vs. 9.9% of those with a negative FIT and 69.8% vs. 74.1% of those with a positive FIT), 10 suggesting the test is being used similarly in both populations. A limitation of this study is that the study period overlapped with the COVID-19 pandemic; therefore, access to colonoscopy was reduced, meaning the use of FIT and referral patterns in primary care may have been affected.
The data presented here suggest that FIT has a specificity for CRC in this age group similar to that seen in other studies looking at all age groups;8,10–13 however, the sensitivity was higher in our study than any of these others. The PPV reported here is less than half than that seen in another study by D’Souza et al., which focussed on patients aged under 50; 8 however, one large study from Spain 11 showed similar results in a subgroup analysis of patients aged under 50 for sensitivity (93.1% vs. 100%), specificity (88.5% vs. 86.3%), PPV (2.6% vs. 2.7%) and NPV (99.97% vs 100%). This is reflected in the prevalence of CRC in the populations investigated in each study; the prevalence in the study by Pin-Vieito et al. was 0.3%, 11 in our evaluation was 0.38% and in the study by D’Souza et al. was 1.5%. 8 This is likely to be explained by the different populations these studies investigated; D’Souza et al. used data from the NICE FIT study, which involved patients who had been urgently referred with bowel cancer symptoms, 14 whereas both our service evaluation and the study reported by Pin-Vieito et al. investigated a primary care population including all individuals with symptoms whose primary care providers requested a FIT test. These individuals were likely to have concerning but less urgent symptoms, and were likely to be more representative of test performance in a real life clinical setting, therefore reducing the risk of spectrum bias.
The relatively low PPV reported in our evaluation suggests a higher rate of false positives than in older populations. This is to be expected due to the low prevalence of CRC and higher prevalence of other SBD in this age group. In this service evaluation, we did not investigate SBD as an endpoint; however, this was investigated by D’Souza et al., who found that in their urgently referred population the prevalence of SBD was 46.1% at the 10 μg/g cut-off used. 8 Although their study showed that the diagnostic performance of FIT for SBD was not as good as for CRC, there may therefore be a role for FIT in this population to guide urgent referral for SBD of all kinds, including CRC.
Several studies have investigated the appropriateness of 10 μg/g as a cut-off for positivity in younger patients and some have proposed a higher cut-off for positivity in younger populations; Turvill et al. 12 suggested a cut-off of 37 μg/g in patients aged under 60 vs. 19 μg/g in patients aged 60 and over, while an earlier publication from the same group recommended a cut-off of 46 μg/g in patients aged under 65 vs. 12 μg/g in those aged 65 and over. 15 A cut-off of 150 μg/g has been investigated in a number of studies as a proposed cut-off for urgent investigation,16–20 including the NICE FIT study. 14 A meta-analysis 13 showed that use of this cut-off across all age groups would detect 60% of CRC, and a subgroup analysis of the NICE FIT study showed that in younger individuals FIT has a positive predictive value of 11.5% at a cut-off of 150 μg/g6. Re-analysis of our data using this cut-off improved the specificity and positive predictive value of FIT in this population.
NICE guidelines recommend that a PPV of 3% is used as a criterion to guide urgent referral for further investigations. 7 On the basis of our data, a cut-off of 10 μg/g would not meet this in patients aged under 50; however, our data supports urgent referral for patients with a f-Hb above 150 μg/g.
Data regarding the nature of symptoms in our population was available for 2655 of the 3119 patients (85.1%); however, it should be noted that this was taken from clinical details entered into the LIMS at requesting and may not be comprehensive. The most common symptoms recorded were a change in bowel habit (45.5%) or abdominal pain (26.0%); however, a significant number also reported symptoms considered more worrying such as blood in the faeces (25.0%), anaemia (7.1%) or weight loss (6.9%), suggesting our population included patients with a wide variety of symptoms.
Recently published international management guidelines from the Delphi Initiative for Early Onset Colorectal Cancer (DIRECt) group highlighted the use of FIT in patients aged under 50 as an area of controversy, and although they did not recommend its use in patients with alarming symptoms (such as blood in the faeces, unexplained iron deficiency anaemia or unexplained weight loss) due to concerns over delayed diagnosis, false negatives and poor referral rates to colonoscopy following a positive FIT, they did suggest that FIT-based triage of patients with vague symptoms (including abdominal pain or change in bowel habit) may be of value. 21 On this basis, our data suggests FIT may be a valuable triage tool in patients with both high- and low-risk symptoms, although further prospective studies looking at patients based on severity of symptoms would be of value.
Individuals aged under 50 years typically have a delayed diagnosis of CRC as it is only considered once all other more benign conditions have been excluded. This data supports the use of FIT as an early triage tool for patients under 50 presenting with lower GI symptoms suggestive of CRC that is cheap and easy to request and carry out. Our data supports other published studies suggesting that a higher cut-off may be more appropriate in this younger population. Further work is required with a suitably powered real world population of symptomatic younger patients to confirm the diagnostic utility of FIT in this age group.
Footnotes
Acknowledgements
We would like to thank the clinical audit and Somerset Cancer Registry teams at each of the three local trusts who assisted with collection of colonoscopy and outcome data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not required.
Guarantor
Sally C Benton,
Contributorship
RT – project design, data interpretation and writing the manuscript. SCB – project design, contribution to manuscript and review.