
Abstract
Objectives
High concentrations of low-density lipoprotein cholesterol (LDL-C) are a risk factor for cardiovascular disease. We validated the efficacy of the Martin method is useful in the estimation of LDL-C concentrations was validated in Japanese populations and derived a modified Martin method for easy laboratory information system applications.
Methods
We created 3 subject groups, including 2664 health check-up participants registered with the Resource Center for Health Science, 29,806 clinical patients (A) in the Gifu University Hospital, and 113,716 clinical patients (B) in the Fujita Health University Hospital. Each method to estimate serum LDL-C concentrations (Friedewald formula, Martin method and modified Martin method) was validated by correlation analysis with serum LDL-C concentrations measured using a direct method
Results
The correlation coefficients with the direct method in terms of the Friedewald formula, Martin method, and modified Martin method were 0.963, 0.972 and 0.970 in the health check-up participants; 0.946, 0.962 and 0.961 in clinical patients A; and 0.961, 0.979 and 0.978 in clinical patients B, respectively. Concordance ratios with using the direct method in the Friedewald formula, Martin method and modified Martin method were 82.8%, 85.5% and 85.3% in the health check-up participants; 76.4%, 80.5% and 80.2% in clinical patients A; and 76.1%, 82.6% and 82.6% in clinical patients B, respectively.
Conclusion
Our results show that the Martin and modified Martin methods display good performance in terms of the estimation of LDL-C concentrations among triglyceride concentrations of a wide range, and they may thus be useful for estimating LDL-C concentrations.
Introduction
High blood cholesterol concentrations are critical risk factors for cardiovascular disease (CVD). In particular, low-density lipoprotein cholesterol (LDL-C) concentrations are adopted for risk assessment and treatment goals in principal guidelines such as those of the European Society of Cardiology/European Atherosclerosis Society (2019 ESC/EAS Guideline) and American College of Cardiology/(2019 ACC/AHA Guideline).1,2
The beta-quantification (BQ) method, which is the international standard method for serum or plasma LDL-C level measurements, 3 requires ultracentrifugation and is not suitable for routine clinical assays. Moreover, regulations allow the use of LDL-C concentrations estimated by the Friedewald formula only for patients with triglyceride (TG) values of <400 mg/dL. Furthermore, previous reports have demonstrated that LDL-C values estimated by the Friedewald formula in patients with TG values of <400 mg/dL deviated from those measured by the BQ or direct methods.4–14
Several studies have reported unique methods for estimating LDL-C developed for the improvement of consistency with the LDL-C concentrations established by the BQ method.4–8 Martin reported a new method to estimate LDL-C concentrations with variable TG to very-low-density lipoprotein cholesterol (VLDL-C) ratios by TG concentrations and non–high-density lipoprotein cholesterol (HDL-C) concentrations. 15 The Martin method was revealed to be a superior approach to the Friedewald formula by several studies in estimating LDL-C concentrations,16–19 whereas only a few reports have demonstrated its use in Japanese populations .20,21 Previous studies involving Japanese participants have been validated using under fasting conditions but have not been confirmed in populations who participated without fasting, including clinical patients. Furthermore, the Martin method is not suitable for use in the laboratory information system (LIS) because it requires selection of TG concentrations to VLDL-C ratio from 180 patterns by TG and non–HDL-C concentrations. 15
This study aimed to revalidate the suitability of the Martin method when applied to samples obtained from Japanese participants under fasting conditions who underwent health check-ups, and samples obtained from clinical patients under fasting and non-fasting conditions analysed using two different protocols for LDL-C measurement. We also sought to validate the utility of a novel, modified Martin method, designed for LIS-related applications.
Materials and methods
Study populations
Characteristics of health check-up participants and clinical patients.
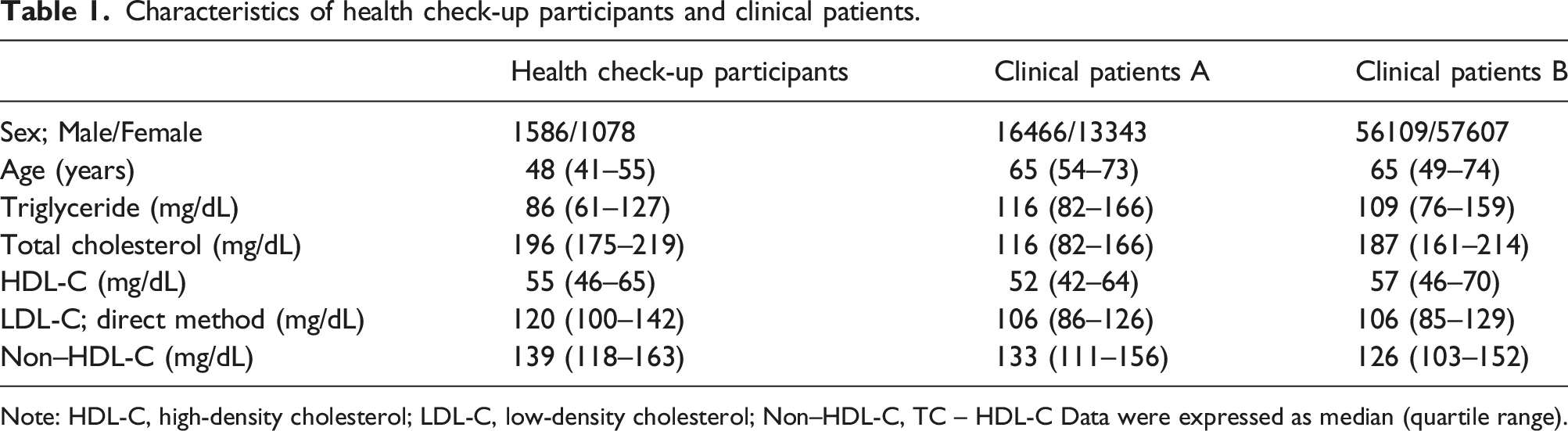
Note: HDL-C, high-density cholesterol; LDL-C, low-density cholesterol; Non–HDL-C, TC – HDL-C Data were expressed as median (quartile range).
Lipid measurement and calculation
Serum TG level measurements were performed by employing the free-glycerol elimination lipoprotein-lipase and glycerol kinase method using ‘Cholestest TG’ (SEKISUI Medical Co., Inc.) in health check-up participants and clinical patients A and ‘DETAMINAR L TG Ⅱ’ (Hitachi Chemical Diagnostics Systems Co., Ltd.) in clinical patients B. Serum TC level measurements were performed by employing the cholesterol esterase- and cholesterol oxidase-related method using ‘Cholestest CHO’ (SEKISUI Medical Co., Inc.) in health check-up participants and clinical patients A and ‘DETAMINAR L TC Ⅱ’ (Hitachi Chemical Diagnostics Systems Co., Ltd.) in clinical patients B. Serum HDL-C and LDL-C concentrations were measured by employing the homogeneous enzymatic assay method using ‘Cholestest N HDL’ and ‘Cholestest LDL’ in health check-up participants and clinical patients A and ‘MetaboLead HDL-C’ and ‘MetaboLead LDL-C’ (Hitachi Chemical Diagnostics Systems Co., Ltd.) in clinical patients B. The LDL-C concentrations were estimated by the Friedewald formula (LDL-C-F; [TC] − [HDL-C] − [TG]/5) and the Martin method (LDL-C-M; [TC] − [HDL-C] − [TG]/variable factor). 22 The TG to VLDL-C ratios were calculated by (TG)/([TC] − [HDL-C] − [LDL-C-D]).
Derivation of the modified Martin’s LDL-C estimation method for LIS applications
The factors for TG to VLDL‐C ratios derived by modified Martin method.
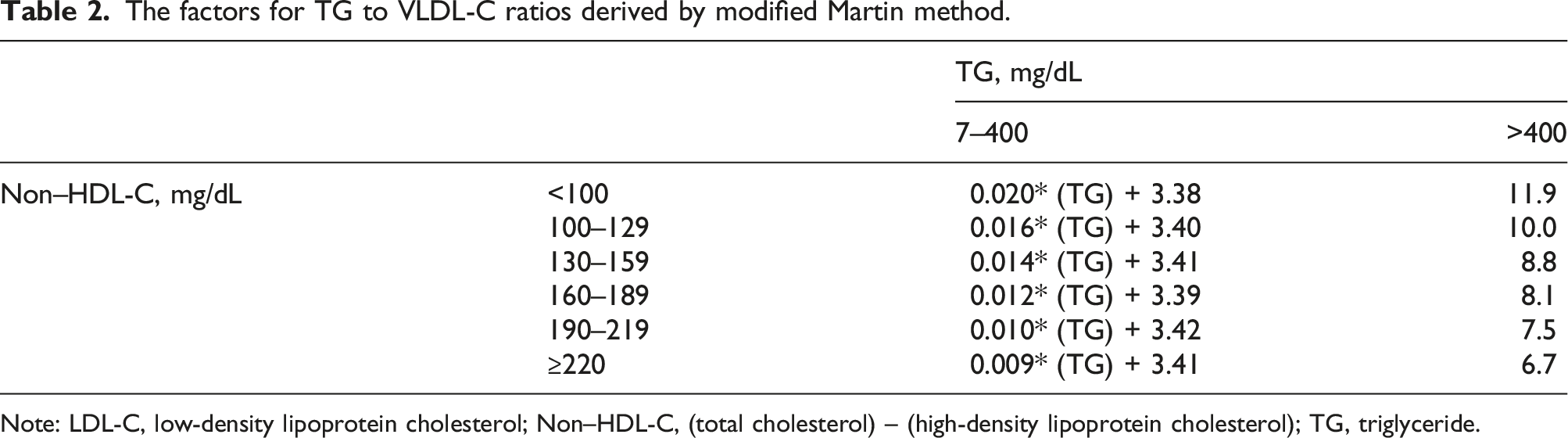
Note: LDL-C, low-density lipoprotein cholesterol; Non–HDL-C, (total cholesterol) – (high-density lipoprotein cholesterol); TG, triglyceride.
Statistics
We estimated the suitability of LDL-C evaluations using Spearman’s rank correlation coefficient, Deming regression analysis, 23 and Bland–Altman analysis. 24 The concordance of the LDL-C strata between each method was assessed using the Kappa coefficient method. All statistical analyses were performed using JMP 13.2.1 and R 4.1.0.25,26
Results
The distribution of TG to VLDL-C ratios
Figure 1 shows the distribution of TG to VLDL-C ratios calculated by LDL-C-D in health check-up participants, as well as in clinical patients A and B. In health check-up participants and clinical patients A and B, the median (25th–75th percentile) of TG to VLDL-C ratios was 5.50 (4.00–6.78), 4.71 (3.73–5.89) and 6.22 (5.10–7.61), respectively. Because the Friedewald formula estimates LDL-C by fixing the TG to VLDL-C ratio at 5.00, variations in the TG to VLDL-C ratio are sources of error in the LDL-C estimation. The TG to VLDL-C ratio contributions less than 4.50, causing an underestimation compared with LDL-C-F, were 34.1%, 44.2% and 13.8%, respectively. Similarly, the TG to VLDL-C ratio contributions over 5.50, causing an overestimation compared with LDL-C-F, were 46.4%, 32.1% and 65.9%, respectively. TG to VLDL-C ratio distributions calculated by TG/(TC – HDL-C – LDL-C-D) in health check-up participants (a), clinical patients A (b), and B (c).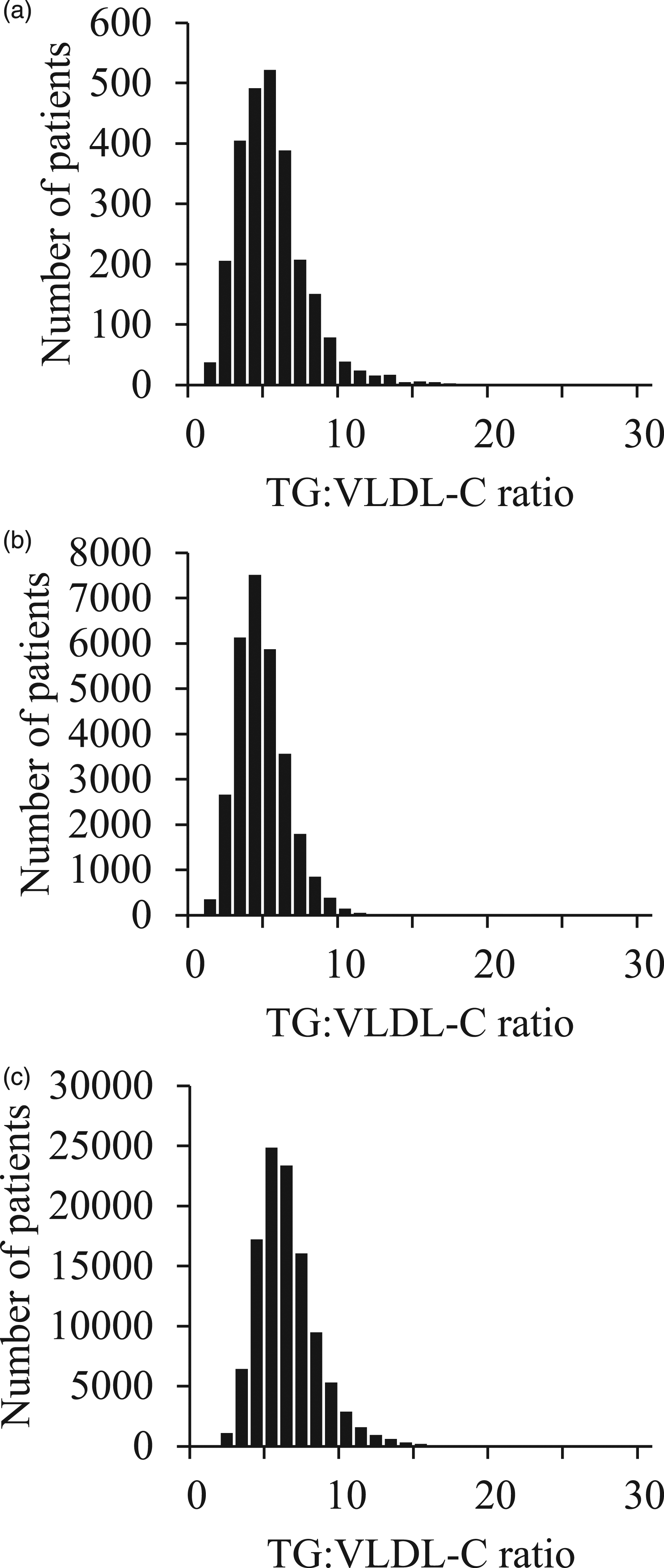
Correlations and biases between LDL-C-D and estimated LDL-C
The performance on method of LDL-C estimation reference to the direct method.
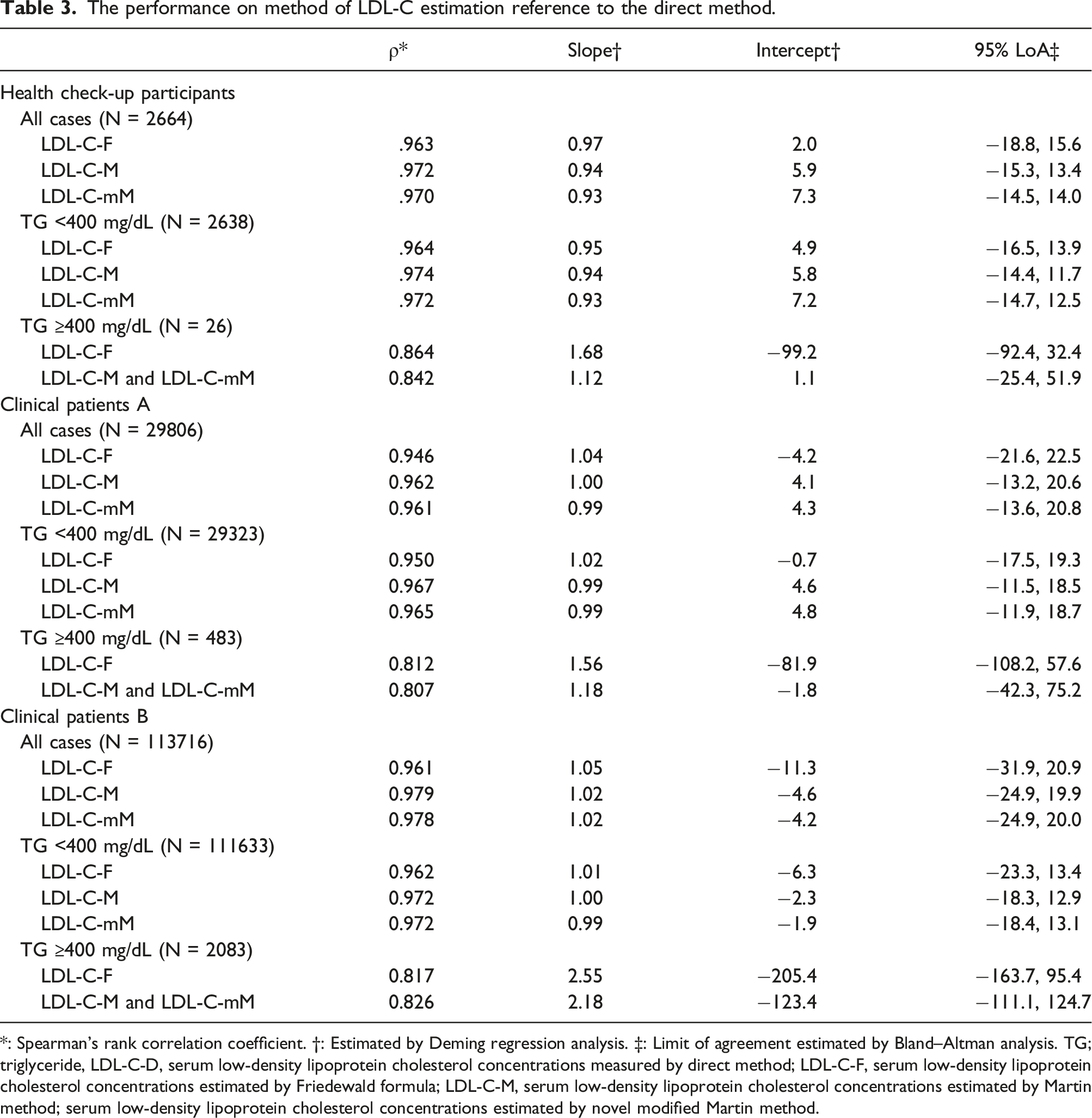
*: Spearman’s rank correlation coefficient. †: Estimated by Deming regression analysis. ‡: Limit of agreement estimated by Bland–Altman analysis. TG; triglyceride, LDL-C-D, serum low-density lipoprotein cholesterol concentrations measured by direct method; LDL-C-F, serum low-density lipoprotein cholesterol concentrations estimated by Friedewald formula; LDL-C-M, serum low-density lipoprotein cholesterol concentrations estimated by Martin method; serum low-density lipoprotein cholesterol concentrations estimated by novel modified Martin method.
LDL-C concentrations strata for intervention strategies on ESC/EAS guidelines
The overall concordance ratios with ESC/EAS guideline classification by LDL-C-D in health check-up participants were 82.8%, 85.5% and 85.3% in LDL-C-F, LDL-C-M and LDL-C-mM, respectively. Moreover, those in clinical patients A were 76.4%, 80.5% and 80.2% and those in clinical patients B were 76.1%, 82.6% and 82.6%, respectively. The concordance ratios for LDL-C-F, LDL-C-M and LDL-C-mM among subjects with TG ˂400 mg/dL were 83.2%, 85.7% and 85.6% in health check-up participants, 77.0%, 81.1% and 81.0% in clinical patients A, and 77.0%, 83.0% and 83.0% for clinical patients B, respectively. The concordance ratios for LDL-C-F and LDL-C-M among subjects with TG 400 mg/dL or higher were 38.4% and 53.8% in health check-up participants, 39.5% and 42.0% in clinical patients A, and 27.6% and 59.1% in clinical patients B. In all subject groups, Kappa coefficients between LDL-C-D and LDL-C-M or LDL-C-mM were higher than those between LDL-C-D and LDL-C-F (Figure 2). Concordance of LDL low-density lipoprotein-C concentrations strata for intervention strategies on ESC/EAS guidelines in health check-up participants (a), as well as clinical patients A (b) and B (c) referring to LDL-C-D low-density lipoprotein-C measured using the direct method.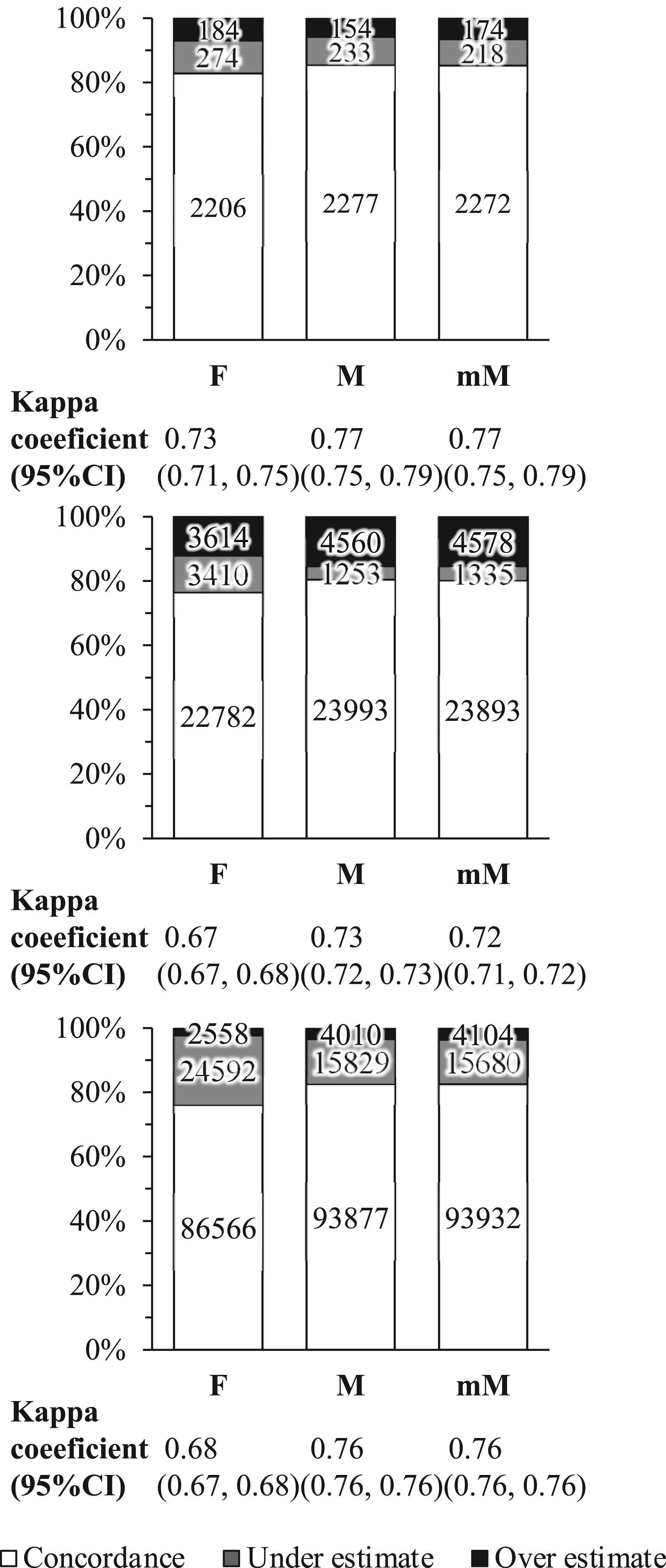
Discussion
The present study evaluated the Martin method for serum LDL-C level estimation by correlation with serum LDL-C concentrations measured by the direct method in health check-up participants and clinical patients. Furthermore, we derived a novel modified Martin method, which could be applied to LIS, and evaluated its performance. This study has several limitations. First, the reference method of this study is the direct method and not the gold standard BQ method. Second, we used only reagents manufactured by SEKISUI Medical Co., Inc. and Hitachi Chemical Diagnostics Systems Co., Ltd. in both subject groups; thus, a potential difference in reagent variety was not addressed. However, we found that both LDL-C-M and LDL-C-mM correlated better with LDL-C-D than LDL-C-F, and higher concordance in the LDL-C strata could be observed on the ESC/EAS guideline.
The Friedewald formula for LDL-C estimation also has its limitations because it should be used in patients with TG values of ˂400 mg/dL and fasting samples. Previous studies showed that LDL-C values estimated using the Friedewald formula deviated from those obtained by the EQ and the direct methods. Various alternative methods have been established to estimate LDC-C and showed better correlations with the BQ method or direct method than the Friedewald formula.4–8 Among them, the Martin method is an innovative and highly reliable method because it uses variable TG to VLDL-C ratios obtained by large-scale lipid profile datasets measured by the BQ method. 15 The benefits of this method have been demonstrated in several previous studies that have shown it to be highly compatible with the BQ method and the direct methods.16–19 Moreover, the Martin method requires choosing one of the 180-pattern of factors from the TG and non–HDL-C values, which is not practical for LIS application. We modified the Martin method into the 12-pattern formula based on the TG and non–HDL-C values to simplify LIS implementation. The 12-pattern formula could be simpler to implement in LIS than the 180-pattern formula. The performance of this approach may vary with different study populations, whereas only few studies have reported Japanese subject-related results. Similar to previous studies, our results showed that the Martin method correlates better with the direct method than the Friedewald formula.16–19 This study yielded better correlations and more convergent LoA in LDL-C-M and LDL-C-mM compared with LDL-C-F not only in the health check-up participant and clinical patient groups but also in clinical patients with different reagents. Because sera from clinical patients were sampled any time regardless of fasting, LDL-C-M and LDL-C-mM might be superior to estimate LDL-C concentrations with or without fasting. However, all estimates tended to be higher than LDL-C-D with TG ≥400 mg/dL. Previous reports showed that the two methods have superior correlation, but that errors occur via differences in reactivity in CM, VLDL and IDL fragments. 27 Our results indicated that clinical patients A and B using different reagents had comparable correlation coefficients, especially in TG <400 mg/dL patients. However, there were several cases with estimated LDL-C values by LDL-C-F, LDL-C-M and LDL-C-mM substantially higher than LDL-C-D measurement values in clinical patient B with LDL-C-D < 100 mg/dL. These cases were presumably affected by the presence of non–LDL-C enriched in TG such as VLDL-C, which cannot be included in the measurement of the direct method in clinical patients B. In addition to the difference in the subject populations, this might be caused by the measurement reagent differences for the direct method, representing the reference method. 28 For TG ≥400 mg/dL, LDL-C-M and LDL-C-mM might still be better than F, although this aspect might still require further improvement.
The Friedewald formula reportedly underestimates the CVD risk.10,29 We obtained similar results in this study. Concordance ratios of LDL-C level strata for intervention strategies on ESC/EAS guideline with the direct Martin method in all subject groups were higher than those by the Friedewald formula, with improvement of concordance ratios by reduction of the underestimation. Therefore, the Martin method could be more useful to assess the CVD risk than the Friedewald formula. Furthermore, this study shows that not only the former but also the modified Martin method derived by us for LIS application yield better correlation and concordance of LDL-C strata on ESC/EAS guideline with the direct method than the Friedewald formula. LDL-C-mM could be potentially applied for LIS easier than the former Martin method as it relies on selecting the formula from 12 patterns by TG and non–HDL-C concentrations. Therefore, our results indicate that not only the Martin method but also the modified Martin method are useful for estimating serum LDL-C concentrations, especially for LIS-related applications as a pre-treatment examination.
Conclusion
We derived the modified Martin method for simple LIS application and the validation of the Martin and the modified Martin methods in health check-up participants and clinical patients. Both the Martin and the modified Martin methods resulted in better correlations with the direct method than the Friedewald formula, hence these methods are valid for LDL-C concentrations estimation. In particular, the modified Martin method could be potentially useful for LDL-C estimation on LIS-related applications.
Supplemental Material
Supplemental Material - Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application
Supplemental Material for Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application by Hidekazu Ishida, Yasuko Yamamoto, Midori Saito, Yuya Ishihara, Takashi Fujita, Mariko Ishida, Yohei Kato, Yuzuru Nohisa, Hidetoshi Matsunami, Masao Takemura, Tadayoshi Hata, Hiroyasu Ito and Kuniaki Saito in Annals of Clinical Biochemistry
Supplemental Material
Supplemental Material - Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application
Supplemental Material for Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application by Hidekazu Ishida, Yasuko Yamamoto, Midori Saito, Yuya Ishihara, Takashi Fujita, Mariko Ishida, Yohei Kato, Yuzuru Nohisa, Hidetoshi Matsunami, Masao Takemura, Tadayoshi Hata, Hiroyasu Ito and Kuniaki Saito in Annals of Clinical Biochemistry
Supplemental Material
Supplemental Material - Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application
Supplemental Material for Validation of the Martin method to estimate low-density lipoprotein cholesterol concentrations in Japanese populations and a modified method for laboratory information system application by Hidekazu Ishida, Yasuko Yamamoto, Midori Saito, Yuya Ishihara, Takashi Fujita, Mariko Ishida, Yohei Kato, Yuzuru Nohisa, Hidetoshi Matsunami, Masao Takemura, Tadayoshi Hata, Hiroyasu Ito and Kuniaki Saito in Annals of Clinical Biochemistry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Fujita Health University Graduate School.
Ethical approval
Gifu University Hospital Clinical Research Ethics Board (2021-A059) and the Fujita Health University Research Ethics Board (FM21-093) approved this study.
Guarantor
KS.
Contributorship
HI, YY and TM researched literature and conceived the study. HI gained ethical approval, data analysis, and wrote the first draft of the manuscript. HI, YY and TM involved in the investigation. MS, YI, TF, MI, YK, YN, HM, MT and TH involved in the supply of clinical laboratory data. TH, HI and KS involved as supervision and project administration. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.