
Abstract
In the last decade, the introduction of the serum-free light-chain (sFLC) assay has been an important advance in the diagnosis and management of plasma cell dyscrasias, particularly monoclonal light-chain diseases. The immunoassay was developed to detect free light chains in serum by using anti-FLC antibodies which specifically recognised epitopes on light chains that were ‘hidden’ in intact immunoglobulins. Since its introduction in 2001, there have been several publications in the English language literature discussing the clinical utility as well as analytical limitations of the sFLC assay. These studies have highlighted both positive and negative aspects of the assay particularly with regard to its sensitivity and specificity and the technical challenges that can affect its performance. The contribution and significance of the sFLC assay in the management of light-chain myeloma, primary amyloid light-chain (AL) amyloidosis and non-secretory myeloma are well recognised and will be addressed in this review. The aim of this article is to also review the published literature with a view to providing a clear understanding of its utility and limitations in the diagnosis, prognosis and monitoring of plasma dyscrasias including intact immunoglobulin multiple myeloma (MM) and monoclonal gammopathy of unknown significance (MGUS). The increasing interest in using this assay in other haematological conditions will also be briefly discussed.
Introduction
Monoclonal gammopathies are plasma cell dyscrasias, characterised by proliferation of a single neoplastic clone of plasma cells. This is usually associated with an excessive production of monoclonal proteins (paraprotein) composed of either an intact immunoglobulin and/or an increased production of either kappa (κ) or lambda (λ) light chains. Phenotypically, monoclonal gammopathies may range from being clinically benign, as in monoclonal gammopathy of undetermined significance (MGUS), or symptomatic, as in multiple myeloma (MM) with end-organ damage including bone marrow suppression, bone destruction and renal damage.
The diagnosis of monoclonal gammopathies is based on measurement of monoclonal paraprotein either circulating in serum or excreted in urine. 1 Approximately 15–20% of patients with myeloma only have production of free monoclonal light chains (light-chain myelomas) and these may not be detected as a distinct monoclonal band on serum electrophoresis due to limited sensitivity of this method. An additional 1–2% of myeloma patients are non-secretory, thus without a detectable band on routine electrophoresis. Monoclonal light-chain diseases were diagnosed by measurement of free light chains excreted in urine also known as Bence-Jones proteins (BJP); a more sensitive method than serum electrophoresis for the detection of light chains but limited by renal threshold and function.
In 2001, the diagnosis of light-chain diseases was revolutionised by the introduction of a new serum assay.
2
This assay was originally set up using polyclonal antisera obtained from sheep immunised with human BJP. Once purified, the antisera were digested with pepsin to produce F(ab)2 fragments, these fragments were then adsorbed onto polystyrene latex particles to enhance stability and sensitivity (Figure 1).
3
This method provided an improved sensitivity for the determination of serum-free light-chain (sFLC) compared to previous methods. In addition to quantification, the method also allowed indirect determination of monoclonality by using the κ:λ ratio. This assay is now widely used and recommended by the International Myeloma Working Group Consensus Panel (IMWG) as a complementary test to serum protein electrophoresis (SPEP) and immunofixation (IFE) in all newly diagnosed patients with plasma cell dyscrasias.
4
Overview of the process to produce polyclonal serum samples to free light chains. (a) All plasma cells produce both intact immunoglobulin and relevant free light-chain molecules (up to 40% excess). Free light chains can either be κ or λ with λ-free light chains pre-dominantly existing as dimers. Epitopes used for specific detection of free light chains are to be found on the ‘hidden’ region (marked in red) on the constant and variable domain of the free light chain. These are hidden when the light chain is integrated into an intact immunoglobulin molecule but exposed when the light is produced as a free molecule. (b) Free light chains purified from the urine of patients with light-chain myeloma are injected into sheep in addition to adjuvants by the manufacturer. The sheep is then bled weeks later to retrieve serum samples containing a polyclonal response to the free light chains. (c) These serum samples are further affinity purified and digested to produce (Fab’)2 and bound to latex particles to enhance stability and sensitivity. (d) Signal is generated when the latex particle-bound antibody fragments bind to free light chains from test serum samples leading to cross linking and immune complex formation. A laser beam aimed at these immune complexes leads to laser scatter. Measurement of this laser scatter (nephelometry) or of the unscattered laser light (turbidimetry) can be used to quantify free light-chain amount.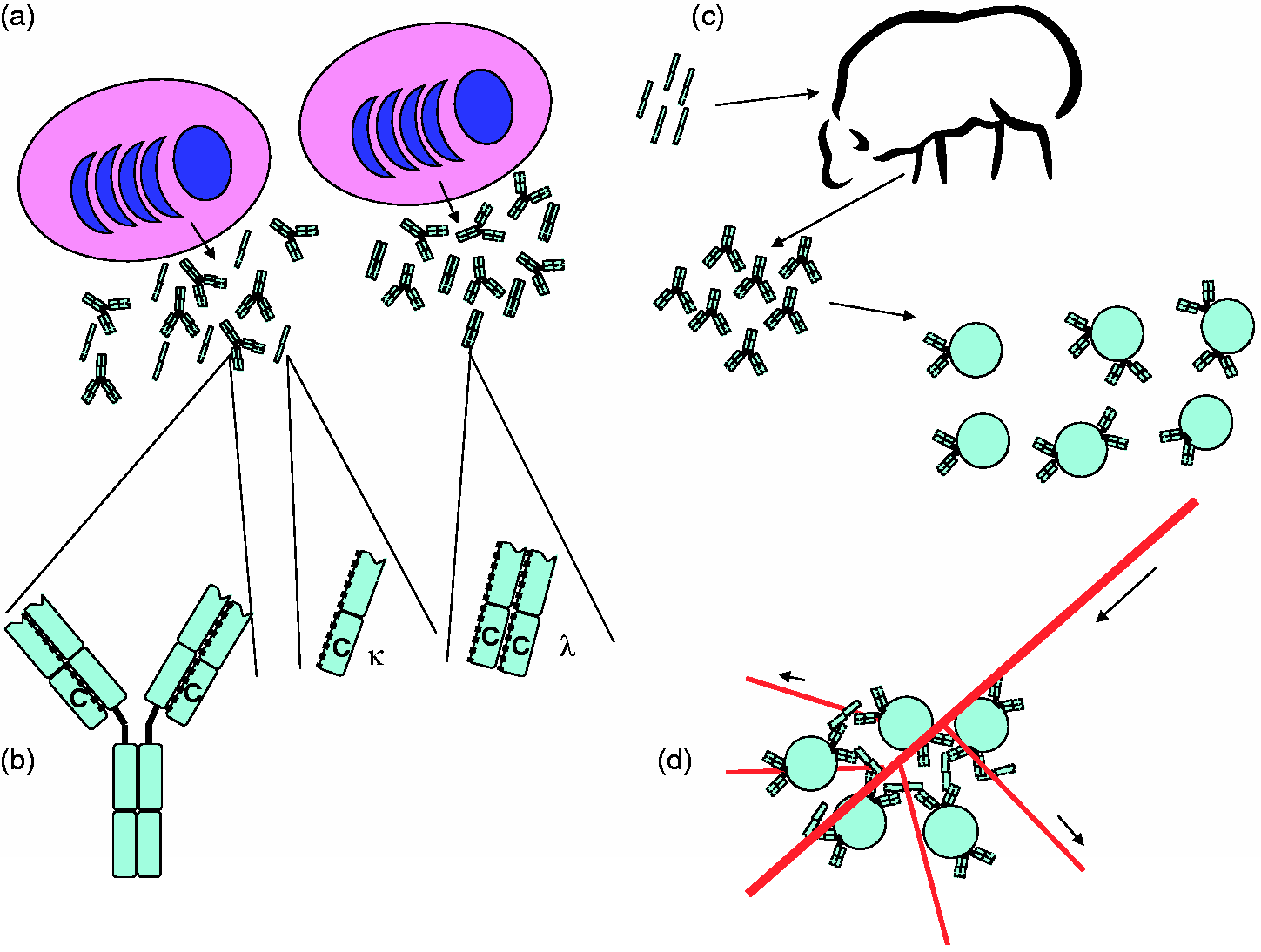
sFLC assay is an important addition to clinical pathway of management of plasma cell dyscrasias. Addition of sFLC assay to sIFE almost obviated the need for 24-h urine IFE, where compliance is often poor. Other utilities of this assay are owing to shorter half life of sFLC; a better marker of early remission and early relapse and a prognostic marker for the identification of risk of progression in benign monoclonal gammopathy.
This review has been prepared with a view to discuss the scope and utility of the sFLC assay in diagnosis, prognosis and monitoring of light-chain diseases and other plasma dyscrasias including intact immunoglobulin MM and MGUS as well as to provide a clear understanding of its technical limitations and analytical pitfalls. The increasing interest in using this assay in other haematological and non-haematological conditions will also be discussed.
Clinical utility of sFLC assay
The detection of intact immunoglobulins and immunoglobulin-free light chains in serum and urine is of paramount importance in the diagnosis, prognosis and management of patients with plasma dyscrasias. In addition, the short physiological half life of sFLC in blood (κ: 2–4 h and λ: 3–6 h) potentially allows this to be used as a serum marker for real-time monitoring of response to treatment as well as disease progression.
Intact immunoglobulin myelomas can be diagnosed and monitored using a combination of SPEP, IFE and densitometry, which allows the quantification and characterisation of the monoclonal protein. However, the lower limit of detection using SPEP alone is 500–2000 mg/L, thus limiting the sensitivity and utility of this assay for detecting low concentrations of monoclonal light chains commonly seen in light-chain diseases, non-secretory and oligo-secretory myelomas. Combination with IFE improves the sensitivity for the detection of sFLC but does not allow quantification of the paraprotein. For more than 100 years, the detection of BJP in urine was considered a gold standard in the diagnosis and monitoring of light-chain diseases with detection limits as low as 10–40 mg/L. However, the quantification of FLC in urine requires a 24-h urine collection and the detection of FLC using this assay is dependent on proximal tubular resorption and residual renal function, thus potentially becoming unreliable for diagnosis in both early stages and advanced light-chain myeloma.
The new sFLC assay in 2001 addressed both these issues; it appeared to be a highly sensitive and reproducible assay using rate nephelometry to accurately quantify small amounts of FLC in serum (lower detection limits for FLC: 0.2 mg/L) 5 and, being a serum assay, eliminated the need for 24-h urine collections and variability due to renal threshold or renal function. 6 In the last decade, this assay has become increasing available and adopted into clinical practice, particularly in the diagnosis and monitoring of patients with light-chain myelomas, non-secretory myelomas 7 and light-chain diseases like primary amyloid light-chain (AL) amyloidosis8,9 and light-chain deposition disease (LCDD). 10
Reference ranges for sFLC assay
Early studies by Katzmann et al. 5 using the sFLC assay established the reference ranges for κ (3.3–19.4 mg/L) and λ (5.7–26.3 mg/L) free light chains and a diagnostic range for κ/λ ratio using reference serum samples from 282 healthy donors between the ages of 21 and 90 years. Although twice as much free κ chains are produced daily compared to λ chains, the slower renal excretion of the dimeric λ chain makes the normal κ/λ ratio to be around 0.55 (range: 0.26–1.65). Polyclonal production of free light chains can increase markedly during infections or in inflammatory states resulting in an increase in the absolute values of both κ and λ chains with a relatively unchanged κ/λ ratio. In contrast, haematological malignancies and plasma dyscrasias producing monoclonal κ or λ FLC with suppression of the alternate light chain display a skewed distribution with altered κ/λ ratio. In summary, increased concentrations of one of the sFLCs with an abnormal κ/λ ratio indirectly reflect the presence of clonal plasma cell expansion requiring further investigation. Algorithms have been established for the use of sFLC assay in the diagnosis of patients with suspected monoclonal gammopathies.11,12 Concentrations of the individual sFLCs along with the altered κ/λ ratio have steadily gained importance in the diagnosis, prognosis and monitoring of these patients.
An interesting relationship exists between sFLC concentrations and renal function; excessive light-chain production and subsequent filtration through renal glomeruli can damage renal tubules with resultant tubular dysfunction whilst renal failure due to any cause can independently raise sFLC concentrations secondary to reduced filtration rate. Patients with renal failure were noted to have elevated κ and λ concentrations with ratios falling just outside the established ranges. Hutchison et al. 13 measured κ and λ concentrations in 688 patients with chronic kidney disease without monoclonal gammopathies and established a new ‘normal’ sFLC ratio range for patients with renal failure (0.37–3.1). This new renal range has been subsequently validated and found to be useful in diagnosing monoclonal gammopathies in patients with pre-existing renal disease.14,15
Role in diagnosis
There have been several publications endorsing the diagnostic sensitivity of the sFLC assay for all forms of monoclonal gammopathies, particularly, light-chain myelomas, non-secretory and oligo-secretory myelomas (secreting low concentrations of monoclonal protein in serum/urine), primary amyloidosis and light-chain deposition diseases. Limited early studies after its introduction demonstrated high sensitivities in the range of 96–100% in light-chain myelomas at the time of presentation.6,16 These have been reproduced to date in various studies from different centres.17–19 The lower detection limits of the serum assay have been particularly useful in early diagnosis and quantification of paraprotein in light-chain myeloma and non/oligo-secretory myeloma, which were difficult to detect previously using SPEP or even urine electrophoresis (UEP) in some cases.
The role of sFLC assay in the diagnosis of monoclonal gammopathies gained recognition in 2006, when the IMWG incorporated sFLC assays into the diagnostic criteria stating that in patients with no detectable M-component, an abnormal sFLC ratio on the sFLC assay can substitute and satisfy this criterion.20,21 The Working Group have since published further updates and specific guidelines for sFLC analysis in MM and related disorders4,22 recommending its use in all newly diagnosed patients with plasma cell dyscrasias. The recommendation also includes the use of sFLC assay in patients with solitary plasmacytoma, smoldering (asymptomatic) myeloma and MGUS as in these patients an abnormal result is associated with higher risk of progression to symptomatic myeloma.23–25
Can sFLC assays replace 24-h urine IFE in diagnosis of monoclonal gammopathies?
Urine IFE combined with 24-h urine quantification for light chains (BJP) has been considered the most sensitive diagnostic test for monoclonal gammopathies with predominant light-chain production. The introduction of the sFLC assay into clinical practice has raised the question whether this assay could safely replace the urine assay in the diagnosis of these conditions.
A retrospective study by Katzmann et al. 26 using data from 428 patients with paired urine and serum tests showed that the combination of sIFE with sFLC assay identified 99.5% of the patients with abnormal urine IFE. Only two patients were missed using the serum assays: one with a false-positive result and one with idiopathic Bence-Jones proteinuria requiring no further medical intervention. Nowrousian et al. 27 analysed 378 paired samples from 82 patients attending the myeloma clinic at the time of presentation and during the course of their disease. They concluded that sFLC was significantly more sensitive for detecting monoclonal FLC than urine IFE and was more reliable for monitoring disease course and response to treatment.
Two other prospective studies addressed the same question; however, in contrast to the previous studies where patients were mainly recruited from haematology/myeloma clinics, these studies investigated consecutive requests from a wider general population including primary care requests and other clinical specialities. Only 40–50% of samples had accompanying paired urine samples. Beetham et al. 28 found that their local reference interval was lower than that previously published and recommended that κ/λ results be interpreted with reference ranges appropriate for the analyser and the population under evaluation. The authors did not find significant difference in either test and concluded not to remove urine BJP from the investigation panel. In contrast, data from Hill et al. 29 validated the published reference range with 97% (551/568) of their normal serum samples falling within the range. Using FLC in the initial screening, they noted false-positive tests but did not miss any significant pathology. The authors concluded that a combination of SPEP, IFE and sFLC assays could be used as screening tests also taking into consideration the cost implications, availability and handling issues associated with routine urine analysis.
These studies have highlighted that although in retrospective studies and select cohorts from haematology and myeloma clinics the sFLC assay has both high sensitivity and specificity, results from a more general cohort in routine laboratory practice show higher false-positive rates (no paraprotein identified on IFE). The negative predictive value of the assay was high thus making it less likely to miss significant light-chain disease with a normal result. This view was endorsed by the IMWG in 2008 when they recommended FLC could replace 24-h urine IFE for the purpose of screening for monoclonal gammopathies (with the exception of AL amyloidosis), but advocated the use of the urine assay once the diagnosis of monoclonal gammopathy was made. 22 From the currently available literature, it is clear that more prospective case–control studies in undiagnosed populations will be needed before the role of the sFLC assay in diagnosis of monoclonal gammopathies is accurately defined.
Role in prognosis and risk stratification
The role of sFLC ratio in early detection, prediction of progression and risk stratification of monoclonal gammopathy has been evaluated by several groups since the introduction of the serum assay in 2001. Recent retrospective studies of well-characterised cohorts of patients with monoclonal gammopathies have revealed that a significant proportion of patients with symptomatic MM (36–90% in different studies) have had preceding MGUS (M-protein <3 g/L, bone marrow plasma cells <10%) or smoldering myeloma (SMM: M-protein >3%, clonal plasma cells >10%, no end-organ damage) for months to years before clinical progression.30–32 The prevalence of MGUS has been estimated to be 3–5% of the general population over the age of 70 years with progression to MM at the rate of 1% per year.33,34
The presence of an abnormal κ/λ ratio at baseline has been shown to be an independent risk factor for progression to symptomatic myeloma in MGUS, SMM and solitary plasmacytoma,23–25,35,36 and risk stratification models have been described incorporating sFLC assay into multivariate parameters. 37 These risk stratification models help to differentiate patients with clinically significant pre-malignant conditions from those having laboratory abnormalities without increased risk. However, most of the published models have been derived from retrospective analysis of well-characterised and documented cohorts. One may need prospective, international, multi-centre studies to validate these risk stratification models in routine clinical practise.
International staging system for multiple myeloma.
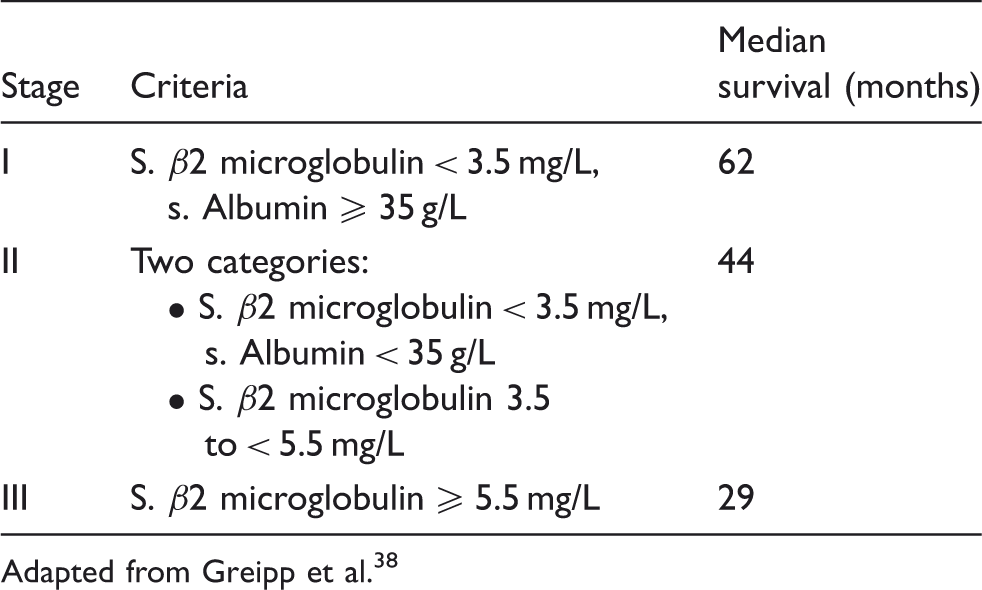
Adapted from Greipp et al. 38
Subsequently, other studies have independently assessed the prognostic role of sFLC assay in newly diagnosed patients with MM and have variably compared it with other well-documented prognostic factors, the ISS or even the older Durie-Salmon staging system.39–44 All these studies show either univariate and/or multivariate association of FLC measurements and ratio in the prognosis of newly diagnosed patients. The ISS may merit a review and update in the light of these findings. The Hellenic Myeloma Study Group has recently published a re-evaluation of prognostic markers in MM patients including sFLC ratio and lactate dehydrogenase (LDH). 45
Similarly, sFLC concentrations have been identified as an independent risk factor for poor prognosis in a retrospective analysis of patients with primary systemic amyloidosis (AL).46,47 Taking these findings into consideration, revised prognostic staging system and new response criteria for patients with AL amyloidosis have been recently published incorporating sFLC measurements and cardiac biomarkers.48,49 sFLC measurements and ratio clearly have an important prognostic role in various forms of monoclonal gammopathies both in terms of prediction of disease progression and in terms of prediction of response to treatment. Further standardised guidelines regarding its contribution to risk stratification would improve and enhance the maximum clinical utility of this assay in routine practice.
Serum-free light chains as a biomarker for response
sFLC analysis is now acknowledged as a reliable marker of response in patients with light-chain MM. A study performed by Bradwell et al. 16 showed that all patients with urine BJP positive myeloma with residual disease following therapy were reliably identified using the sFLC assay. This study examined a subgroup of patients who had undetectable urine BJP following therapy but continued to have an abnormal sFLC ratio, suggesting sFLC to be a sensitive marker for minimal residual disease in this group. Unfortunately, the correlation between urine BJP and sFLC has not been addressed in this paper. 16 In another study, sFLC response was reported to be a useful measure of early response in patients with intact Immunoglobulin MM and relatively high light-chain load. 40
The use of sFLC as a response marker in myeloma has been endorsed by the IMWG and British Council for standards in Haematology (BCSH) Guidelines. 50 The revised International Uniform response criteria have recommended addition of sFLC for better response characterisation in patients with oligosecretory disease. 20 Achieving a normal sFLC ratio with absence of paraprotein and absence of clonal plasma cells in the marrow is defined as stringent complete response (sCR); a new category in the revised criteria. This is now a recommended standard for response characterisation during trial reporting involving myeloma patients. Doublet therapy in the form of combination of steroid and chemotherapeutic agent had been the main stay of myeloma therapy over the years. In the last few years, myeloma physicians have been investigating the use of triplet and quadruplet therapy for both newly diagnosed and relapsed myeloma patients. Response rates have consistently increased with use of these combinations from 60% 51 (historical) to approximately 100% in Phase II studies. 52 Within the various combinations studied, higher overall response rates along with deeper responses are now observed with trials incorporating combination of proteasome inhibitors with immunomodulatory agents, thalidomide and its analogues (IMiDs). Jakubowiak et al. 53 treated patients in a Phase I/II study with a combination of carfilzomib, lenalidomide and dexamethasone and observed a stringent complete response rate of 42%. 53 Although this represents a higher depth of response, it is yet to be shown in a prospective study that achieving stringent complete response provides a better overall survival advantage in myeloma patients. Evolving myeloma therapy with the higher responses observed has put a particular emphasis on response assessment. Examining both depth of responses achieved and early response assessment thereby allowing an opportunity to switch failing patients to suitable alternative therapy has now become crucial. sFLC analysis is potentially useful in these situations.
Up to a quarter of newly diagnosed myeloma patients present with renal impairment. 54 High sFLC concentrations have been shown to be directly nephrotoxic to renal epithelial cells. 55 A large proportion of patients presenting with renal impairment and myeloma are diagnosed with either cast nephropathy or light-chain deposition in the glomeruli on renal histology. The principal goal of myeloma treatment is renal recovery in the form of dialysis independence or improved glomerular filtration rate. In a multicentre study of 67 patients with myeloma and renal impairment, Hutchison et al. 56 showed that 71% of the 41 patients who had a sustained reduction in light chains by Day 12 became dialysis independent. The authors further demonstrated, using multivariate analysis, that reduction of involved sFLC (iFLC) by >50% was a significant factor associated with dialysis independence. Dimopoulos et al. 57 performed a retrospective study of myeloma patients treated at their centre with novel agents. In patients achieving a renal response, median iFLC reduction was 90% and urine M protein reduction was 98%. No direct correlations between the two assays were made in the paper and not all patients had sFLC measured. Validation of sFLC as a biomarker of response in myeloma patients with and without renal impairment has not been prospectively tested in a clinical trial.
The ability to measure sFLC presents a significant advance in the management of patients with AL amyloidosis. 58 The combination of sFLC and SEP with IFE will identify up to 98% of patients with AL amyloidosis. 9 The majority of patients with AL amyloidosis do not have an intact monoclonal protein in serum or urine. Therefore, serial use of sFLC during monitoring has been recommended by the IMWG. 22 A number of studies have supported serial use of sFLC as a response marker following therapy for AL amyloidosis.49,59 sFLC response has correlated with organ responses, progression-free survival and overall survival in some studies. The Mayo cohort study demonstrated that a higher sFLC concentration at presentation correlates with poor overall survival in patients with AL amyloidosis. 47 The clonal light chain is considered the ‘involved’ FLC (iFLC) and the other is referred to as the ‘uninvolved’ FLC (uFLC), with the numerical difference between the two denoted by dFLC. More recently, clinical response based on dFLC concentrations (iFLC–uFLC) post therapy has been devised. Patients achieving normal sFLC ratio with absent serum and urine monoclonal protein are classified as complete responders. Patients with <40 mg/L dFLC at end of therapy and 50% dFLC reduction are classified as very good partial and partial responders, respectively. These surrogate end points correlated with overall survival in a large AL amyloidosis patient dataset. 49 In summary, sFLC analysis is widely used and recommended in prognostication and response monitoring for patients with AL amyloidosis.
Waldenstrom’s macroglobulinaemia is a low-grade lymphoproliferative disorder with lymphoplasmacytoid morphology and IgM paraprotein in the serum. A single-centre study involving 42 patients showed that up to 83% patients had elevated iFLC concentration at presentation. 60 Leleu et al. 61 reviewed sFLC responses in both newly diagnosed and relapsed patients with Waldenstrom’s macroglobulinaemia. In their cohort of 48 patients, response defined by reduction in iFLC was observed earlier than IgM response by a median of one month. Earlier responses were more frequently observed in patients with advanced stage disease. In addition to response evaluation, use of elevated iFLC as a marker resulted in earlier detection of disease progression in this cohort compared to a rise in IgM concentrations.
Diagnosis and monitoring of patients with oligosecretory myeloma and AL amyloidosis following therapy is routinely performed by measuring monoclonal protein in serum and/or urine. Data have now emerged to support use of sFLC as a reliable marker for diagnosis and response monitoring for these patients. National Comprehensive Cancer Network (NCCN), IMWG and BCSH guidelines now recommend use of sFLC as a monitoring tool in these groups of patients.22,50 Ideally, clinicians would routinely measure sFLC following every cycle of therapy. Decisions in the form of stopping therapy, switching therapy or choosing autologous stem cell transplant as consolidation in eligible patients are made based on progress determined by this biomarker. Bone marrow assessment is still used routinely to confirm the sFLC findings (surrogate marker) at the end of therapy. However, cost, technical limitations of this assay and availability of sFLC assay in all centres are the main drawbacks precluding routine use in the UK.
Earlier institution of therapy based on biochemical markers may prevent new complications or worsening of end organ damage. There are no prospective studies validating benefit of earlier therapy guided by biomarkers, but these studies are difficult to perform as sensitivity and tolerability to therapy is heterogeneous among these patient groups, determined by patient age and biology of the plasma cell clone. The use of sFLC to monitor response/relapse in patients with intact Immunoglobulin (Ig) MM is less clear. Light-chain escape phenomenon, which is an observation of isolated increasing sFLC concentrations as manifestation of relapse in patients with previous intact Ig myeloma, has now been described in several case reports.62,63 Qu et al. 63 describe this phenomenon in 11 patients following the use of biological therapies. This reiterates that monoclonal protein does not follow a predictable relapse pattern during monitoring. There is now a sequence of therapies available to treat myeloma patients with thalidomide, bortezomib and lenalidomide licensed and approved for use in most countries. Patients relapsing following therapy frequently develop clonal tides following multiple relapses as elegantly demonstrated by whole genome sequencing in a single patient over a five-year period. 64 The subclones arising during relapse could potentially secrete a different monoclonal protein/light chain in comparison with the presentation sample. These clinico-pathological features emphasise the use of light-chain monitoring in patients with intact Ig myeloma.
Measurement of sFLC has been reported in other haematological malignancies. In a large case series of patients with chronic lymphocytic leukaemia (CLL), up to 60% of the patients had an abnormal sFLC ratio, which conferred a poor prognosis in this cohort compared to patients with normal ratio. 65 Maurer et al. 66 also demonstrated that 49% of CLL patients had either an abnormal sFLC ratio or a polyclonal elevation of sFLC. Both patients with monoclonal and polyclonal sFLC elevation had poor overall survival when compared to patients with normal sFLC concentrations. These results are yet to be demonstrated prospectively in a clinical trial and cannot be recommended to be used in routine practice. Elevated sFLC concentrations both monoclonal and polyclonal were observed in 32% of a total of 295 patients with diffuse large B-cell lymphoma. Elevated sFLC was demonstrated to be an independent adverse prognostic factor for event-free and overall survival when adjusted for International Prognostic Index in this group of patients. 67 This has also been demonstrated in patients with AIDS-related lymphoma. 68 Prognostic significance of sFLC elevation has also been demonstrated in a cohort of patients with Hodgkin’s disease. 69 The likely reasons for the observation of elevated light chains in this group of patients are renal dysfunction, tumour secretion, disruption of B-cell function and age. Further prospective evaluation is required before sFLC is incorporated as a poor prognostic marker in this group of patients with B-cell malignancies.
More recently, Pardanani et al. 70 demonstrated that polyclonal rise in immunoglobulins can be observed in patients with myeloid malignancies. This is thought to be secondary to a host derived immune response. Up to 33% of patients with primary myelofibrosis (PMF) and 46% of patients with myelodysplastic syndromes (MDS) had polyclonal rise in sFLC. This predicted an inferior overall survival in both subgroups. On the whole evidence is accumulating that abnormalities in the form of either monoclonal or polyclonal rise in sFLC is not infrequent in other haematological malignancies. Whether this observation represents a potential marker of B-cell activation and/or B-cell dysfunction needs further evaluation. The caveat is that polyclonal rise of sFLC may be observed as part of physiological aging and prospective studies performed to evaluate these observations should take this into account.
Analytical aspects of sFLC assay: pitfalls and limitations
Since the availability of the sFLC assay to measure sFLC concentrations, the interest in this assay and its clinical utility in diagnosis, monitoring and prognosis has risen exponentially, particularly for light-chain dyscrasias but also for a full range of other conditions including haematological malignancies and other non-haematological conditions, as discussed in the preceding sections. At the same time, there has been an on-going discussion and debate regarding the analytical limitations, pitfalls and technical difficulties with the serum assay. More recently, a new serum assay has been introduced using monoclonal antibodies to light chains (the N-latex assay) as opposed to polyclonal antibodies used in the older assay (Freelite™). 71 The following sections discuss the current analytical issues regarding sFLC measurement including a comparison between the two assays.
Antigen excess detection and non-linearity
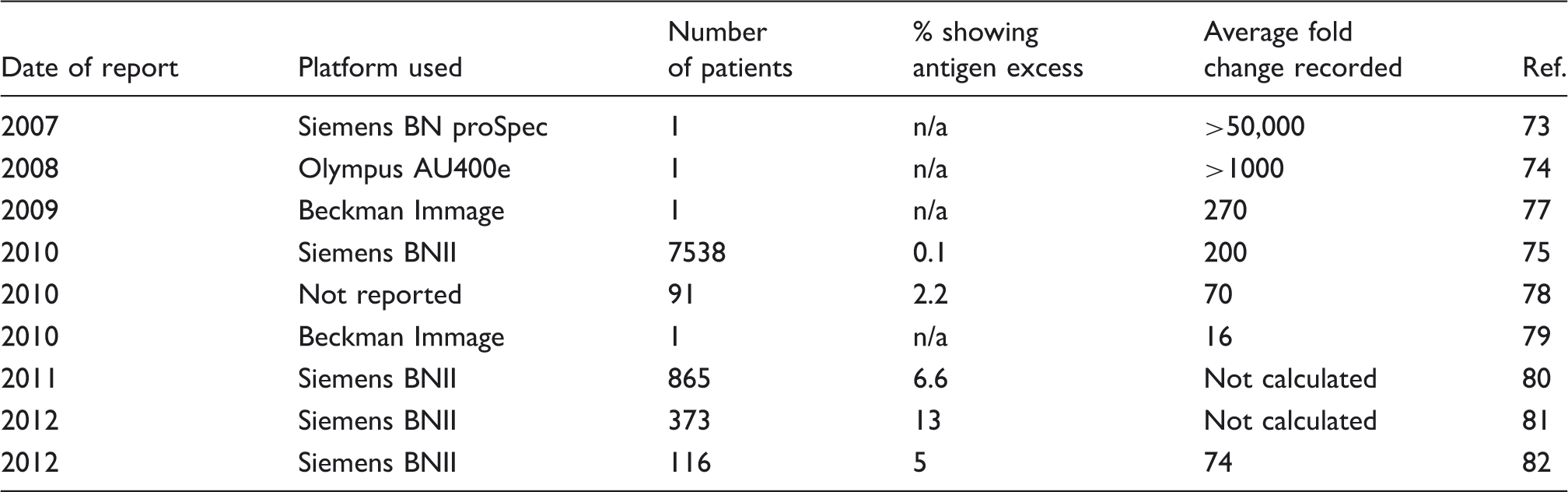
A common technical problem faced by users of the sFLC assay has been that of antigen excess and non-linearity resulting in over or under-estimation of the monoclonal protein. Due to the prerequisite of immune complex formation to produce a signal, both nephelometric and turbidimetric assays are vulnerable to antigen excess, otherwise known as the hook effect. This occurs when the concentration of the analyte goes beyond a threshold concentration, leading to the saturation of all possible binding sites on the detection antibodies with individual analyte molecules thus preventing any further immune complex formation. 72 This was first described to occur in the sFLC assay in a case report of an elderly female suffering from κ light-chain myeloma as determined by serum and urine IFE. 73 The initial serum dilution for FLC measurement at 1/100 on a BNproSpec nephelometer gave a result of <0.294 mg/L for the free κ and a similar free λ concentration. Further testing at a 1/32,000 dilution revealed the true value for κ to be >60,100 mg/L. 73 Evidence of antigen excess being reported with the Freelite™ assay while using a turbidimetry platform has also been described. 74
Examples in the literature of antigen excess.
Recently, two independent groups proposed that all samples should be screened at two separate dilutions (1/100 and 1/2000) to help detect antigen excess.80,81 The first of these studies showed that 12.7% of patients measured for κ FLC had at least a 2-fold difference between the two dilutions, the incidence was 3.1% for λ FLC. 80 It should be noted that the Freelite manufacturer classifies antigen excess as a ≥4-fold change in concentration over two separate dilutions with fold changes lower than that being accepted as non-linearity in the sample. 76 When this cut-off was applied to the first study, the incidence in κ FLC measurements was reduced to 5.4% of all samples measured. The second study using two separate dilutions showed that 7% of patients’ samples that initially showed normal concentrations of both κ and λ FLCs and a normal FLC ratio by a 1/100 dilution subsequently produced a κ FLC value that was at least 2-fold greater when diluted 1/2000. In addition, all but one of these patients showed a change in classification of their FLC ratio from normal to abnormal. Analysis of patients who presented with a high κ FLC after the initial 1/100 dilution showed that 21% of these patients showed a ≥2-fold change and 11% showed a ≥4-fold change. 81 Taken together, these data show that antigen excess is a definite phenomenon in the FLC assays and sufficient precautions should be taken by routine laboratories to try and detect at risk samples. Analysis of previous external quality assurance scheme reports for samples sent with high concentrations of sFLC has shown that multiple laboratories using a variety of different analyser platforms are not detecting accurate values of sFLC. 80 A second analysis showed that when the same high concentration sample was distributed on two separate occasions to users of the scheme, the majority of the laboratories incorrectly reported the sample on one of those occasions with 10% of users reporting the result incorrectly on both occasions. 81
The other recognised issue contributing to imprecision with the sFLC assay has been non-linearity on sample dilutions.77,83,84 This may be a combination of the immunoreactivity of the monoclonal FLC itself as well as lot-to-lot variations in the reagents and performance characteristics of the analysers. As stated above, the Freelite™ assay defines antigen excess as a greater than 4-fold change in concentration over two separate dilutions with fold changes lower than that being accepted as non-linearity in the sample. 76 The combination of antigen excess and non-linearity with resultant over- or under-estimation of sFLC values will have clinical implications. Previous reports have recommended that a variation in FLC measurements of <50% should not be considered as a marker for disease remission or progression.85,86 This has been further endorsed by the recent laboratory-based publications reporting high degrees of variations dependent upon the dilutions used and analysers.80,81 These reports also provide an analysis of returns from the UK national external quality assurance scheme (UK NEQAS) which show significant variations between the different analyser platforms used to perform the sFLC assay.
Overestimation of FLC measurements by nephelometry
In their ‘natural’ state, κ FLC exist in the serum as monomers, whilst λ FLC exist as dimers. It has been shown in some instances that polymerisation of monoclonal FLC can lead to dimers of κ FLCs and trimers of λ FLC.6,87 Both groups reported single patients with the value of sFLC being greater than 10-fold higher using the Freelite™ assay compared to the light-chain monoclonal band on sIFE quantified using densitometry. In both cases, this overestimation has been attributed to polymerisation of the monoclonal component leading to larger immune complex formation and greater scatter by nephelometry. As an extension of this concept, de Kat Angelino and group performed a comparison study using samples from 49 individual patients with monoclonal κ gammopathies, both at diagnosis and during follow-up. They compared two methods for κ FLC analysis; nephelometry and ELISA. The authors reported an exponential correlation between the two methods with the discrepancy being strongest for samples with high κ FLC concentrations. They postulated that this discrepancy could result from either an overestimation using nephelometry due to polymerisation and larger aggregate molecules or conversely, an underestimation using ELISA due to a ‘covering up’ of relevant epitopes during the polymerisation process, leading to a theoretical reduction of binding in a solid phase. 87 This concept warrants further larger investigation in the future and potentially poses yet another pitfall in the clinical interpretation of laboratory results.
N-latex assay v/s Freelite™ assay
In 2011, a new assay for the measurement of free light chains in serum samples using nephelometry was released by Siemens called the N-latex FLC assay. This assay differed from the pre-existing Freelite™ assay due to its use of mouse derived monoclonal antibodies 71 as opposed to the sFLC assay which used digested F(ab)2 fragments from sheep-derived polyclonal antisera to measure the sFLC concentrations. 2 In addition, the N-latex assay is currently only validated to work on Siemens-based BN systems analysers whilst Freelite™ assay for sFLC can be used on multiple platforms including the Siemens analysers (www.bindingsite.com/freelite accessed on 13 March 2013).
Analytical differences between these two assays have to be presumed to be due to the different detection reagents used as well as the different affinities and specificities of the antibodies. Studies to analyse the concordance between the two assays have produced varied results. One study comparing the two assays in different cohorts of patients found that the overall performance was similar with respect to sensitivity and specificity in diagnosing a monoclonal gammopathy. 88 The same study also reported that the direct concordance between the two assays was lowest when measuring λ light chains (concordance 85%) and was particularly noticeable in patients with higher amounts of free light chain (>200 mg/L) with values reported using the Freelite™ assay being 5 - to 10-fold higher than those with the N-latex assay. 88 A second study comparing the two assays found a poorer concordance between the two assays with λ light-chain measurement and κ light-chain measurement showing 74% and 81% concordance, respectively. 82 Other discordant results were seen with the N-latex assay in patients with renal impairment but no monoclonal gammopathy; 10% of this cohort showed free λ light chains above the normal reference range but with normal κ/λ ratios. 88 Other studies have also shown a level of discordance between the two assays in individuals without monoclonal gammopathy, suggesting that the N-latex assay reference range be increased to 29 and 37 mg/L for κ- and λ-free light chains, respectively, to help harmonise with the existing Freelite™ assay. 89 These data therefore highlight the importance of using the same assay (kit) to monitor individual patients.
The same study concluded that while the two assays had a similar level of statistically significant non-linearity, this non-linearity was seldom clinically significant (one case). However, the Freelite™ assay appeared to show a significantly greater vulnerability to antigen excess compared to the N-latex assay, particularly with free κ samples, although this should be taken in the context of the study design carried out in this report.89,90 Other work has highlighted discordant results between the two assays on the serum samples of the same patient that could either be due to antigen excess in the N-latex assay or reduced binding by the assay because of the monoclonal nature of the reagent. 82
Lot-to-lot variation of the N-latex assay was shown to be 7.5% and 10% for the κ and λ reagents, respectively, 89 compared to the previously reported variation of 20–45% with the Freelite™ assay. 77 A more recent study carried out a direct comparison of lot-to-lot variation found in the two assays and reported a similar variation of between 3.57 and 7.12%. 82 In contrast, a recent study evaluating the diagnostic accuracy of both assays to detect monoclonal FLC in patients with acute kidney injury (AKI) and MM showed that the N-latex assay did not detect a monoclonal component in 4% of patients tested, with this possibly being attributed to antigen excess or limitation of epitope detection due to the use of monoclonal antibodies. 56
Sample variation between centres
sFLC measurement is covered by the UK NEQAS within the UK. Previous work analysing the variation generated across centres measuring the same sample have produced large coefficient of variance (CV) % values.80,81 Both of these datasets however focused on samples that displayed antigen excess properties rather than more linear samples. Due to the relatively recent release of the N-latex assay, there is significantly more data and more participants of the EQA scheme using the Freelite™ assay.
Variation in measurement of serum-free kappa, lambda and serum-free light-chain ratio using Freelite™ assay by The Binding Site across different platforms.
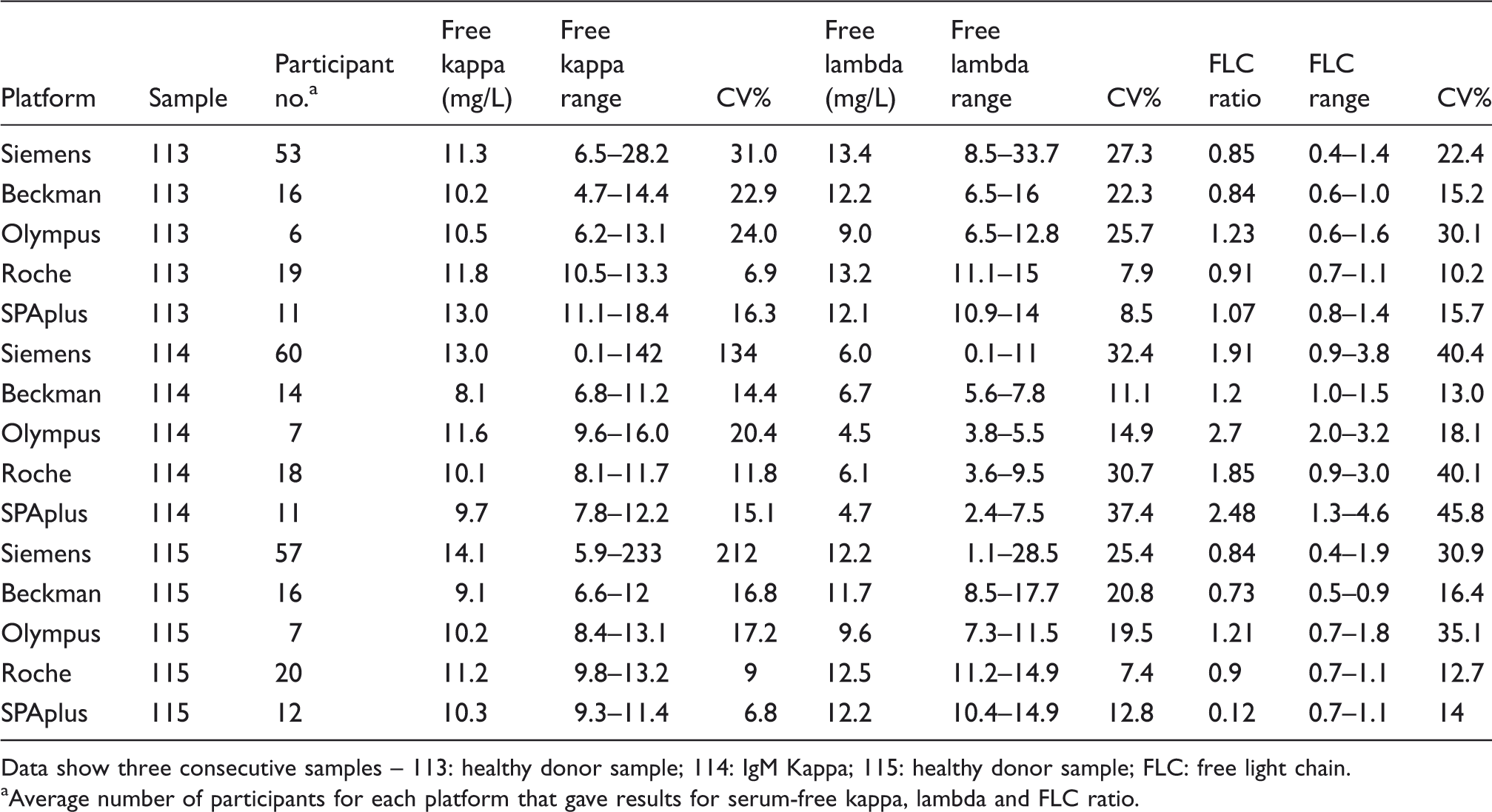
Data show three consecutive samples – 113: healthy donor sample; 114: IgM Kappa; 115: healthy donor sample; FLC: free light chain.
Average number of participants for each platform that gave results for serum-free kappa, lambda and FLC ratio.
EQA performances of N-latex and Freelite™ assay on two different platforms.
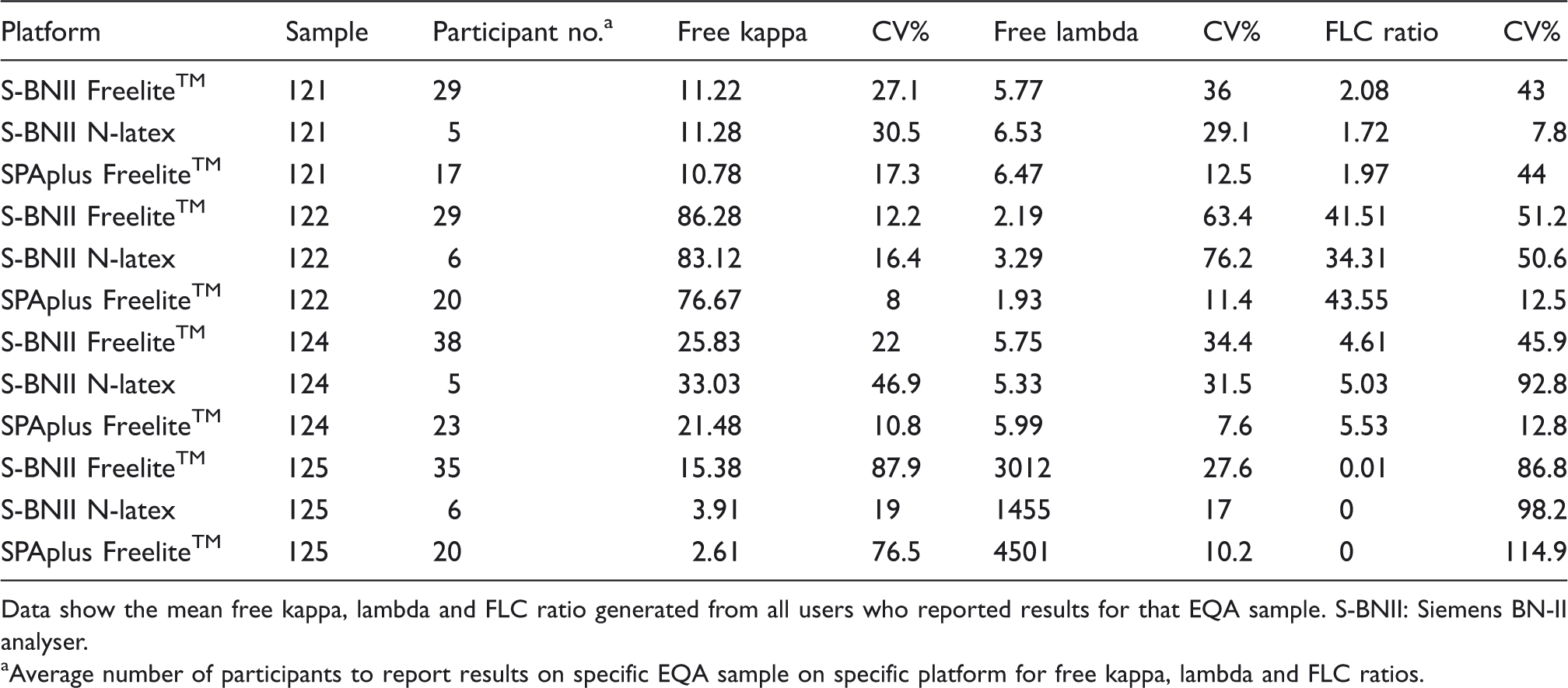
Data show the mean free kappa, lambda and FLC ratio generated from all users who reported results for that EQA sample. S-BNII: Siemens BN-II analyser.
Average number of participants to report results on specific EQA sample on specific platform for free kappa, lambda and FLC ratios.
Conclusion
This review highlights that despite the increasing clinical utility of sFLC analysis in diagnosis, monitoring and prognosis of patients with light-chain dyscrasias, other haematological and non-haematological conditions, there clearly exist technical and analytical issues regarding the currently available assays. Both clinicians and laboratory personnel should be aware of the limitations of the assays and its implications in clinical practice, particularly in light of significant variations in results imposed by intrinsic properties of monoclonal proteins as well as performance differences between the tests, reagents and platforms used for analysis. It is therefore advisable to monitor individual patients using the same analytical conditions, wherever possible. This balanced understanding would be important when defining response criteria and establishing clinical practise guidelines in the future.
Footnotes
Acknowledgements
This article was prepared at the invitation of the Clinical Sciences Reviews Committee of the Association for Clinical Biochemistry & Laboratory Medicine. Results from the UKNEQAS scheme have been included with kind permission from Dr Egner. We also thank him for his critical review of the analysis.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
N/A.
Guarantor
MVB.
Contributorship
All authors have contributed to manuscript writing, editing and amendments. All authors have reviewed the final manuscript.