
Abstract
Background
A rise and/or fall in high sensitivity cardiac troponin (hs-Tn) is critical in defining acute myocardial injury and therefore the diagnosis of acute myocardial infarction. A significant rise in hs-Tn is not well defined in current guidelines. Calculation of a z-score for two consecutive hs-Tn measurements is a method-independent measure of dynamic troponin elevation. However, the association of hs-Tn z-score with outcomes for unselected emergency department admissions is unknown. Moreover, the association of non-dynamic troponin elevations, as defined by a normal z-score, with clinical outcomes remains to be assessed.
Methods
We retrospectively calculated z-scores for patients presenting to emergency department over 18 months who had serial troponin measurements with at least one result >99th percentile using the Abbott hs-TnI assay. We assessed the association of z-score with discharge diagnosis, cardiac interventions, inpatient mortality, length of stay and readmission rates.
Results
There were 2062 presentations for 1830 patients where a z-score was calculated. Z-score was elevated in 1080 presentations. Dynamic troponin elevation (z-score ≥ 2) was associated with acute myocardial infarction (OR = 9.1, P < 0.01), admission to an inpatient unit (95 vs. 88%, P < 0.01), increased inpatient length of stay (97 vs. 65 days, P < 0.01), inpatient coronary intervention (21 vs. 6%, P < 0.01) and mortality (4.4 vs. 2.4%, P < 0.05) compared with myocardial injury with a static troponin elevation.
Conclusions
Z-score is an assay-independent tool to alert clinicians of significant, dynamic troponin elevation and acute myocardial injury. It is associated with poorer clinical outcomes.
Introduction
High-sensitivity cardiac troponins (hs-Tn) are the preferred markers of myocardial injury. 1 In the Fourth Universal definition of myocardial infarction, myocardial injury is defined as a cardiac troponin with at least one concentration above the 99th percentile upper reference limit. Myocardial injury is considered acute when there is a rise and/or fall in hs-Tn concentration. 1 Acute myocardial infarction (AMI), on the other hand, is defined by presence of acute myocardial injury and clinical evidence of acute myocardial ischemia such as chest pain or new ischemic ECG changes. 1
While hs-Tn dynamics are critical in defining acute myocardial injury and AMI, there is little guidance as to what constitutes a significant change in concentration. Both absolute numeric changes (absolute delta) and percentage changes (percent delta) have been proposed with varying cut-off values, at varying re-testing intervals. Absolute delta has been proposed to offer improved diagnostic performance.2–4 However, absolute delta cut-offs are assay specific and add complexity to serial troponin interpretation, particularly for clinicians working across different health services. 5 Pretorius et al. proposed a variation of a reference change value that converted the difference in serial hs-Tn measurements into a probability or z-score, with a z-score greater than 1.96 considered to represent a true change in troponin at the 95% confidence level. 5 This concept was also mentioned in the Cardiac Society of Australia and New Zealand guideline for the assessment of suspected ACS, stating that for patients with troponin close to the 99th percentile, changes of >2–3 standard deviations are unlikely to reflect normal biological variability. 6 Using a z-score as opposed to an absolute or percentage change has the benefits of being independent of the hs-Tn assay used and is comparable across assay platforms for serial troponin results. 7 Z-score is also independent of the initial admission troponin concentration; for instance, the use of absolute hs-Tn change can be misleading in patients with chronic kidney disease whereby baseline hs-Tn is already elevated. 8 Furthermore, z-score calculation can be automated and co-reported with subsequent hs-Tn results in real-time to simplify interpretation and facilitate timely cardiac interventions for high-risk patients. 5
With regard to clinical performance, in a retrospective study of patients presenting to the emergency department with symptoms suggestive of ischemic chest pain, Pretorius et al. showed that a hs-Tn z-score cut-off of 1.96 had good diagnostic performance for an adjudicated diagnosis of Type 1 AMI across multiple assay platforms, with a specificity of 0.94–0.98 and sensitivity of 0.69–0.79 depending on the platform. 5 Similar performance for the diagnosis of AMI was also recently shown using z-scores for the Roche hs-TnT assay. 9 Overall, the performance of z-score was equivalent to an absolute delta change and better than a relative delta change for the diagnosis of AMI.5,9
Despite the excellent diagnostic accuracy of z-scores for the diagnosis of AMI, there have been few studies assessing the association with other cardiac diagnoses and cardiac intervention. Additionally, clinical outcomes of patients with non-dynamic troponin elevations (as defined by a normal z-score) remain largely unknown.
In this study, we aimed to assess the association of z-score and clinical outcomes including discharge diagnosis, cardiac interventions, length of stay and readmission rates by retrospectively calculating z-scores for patients presenting to our emergency department who had serial troponin measurements performed on the Abbott Architect high sensitivity troponin (hs-TnI) assay. The analysis was done prior to the introduction of automated co-reporting of z-score with serial hs-TnI so that diagnosis and intervention was independent of the z-score result.
Methods
Patient data
The Royal Melbourne Hospital maintains an advanced clinical data warehouse, which links together data from a variety of source systems including the patient administration system, laboratory information system and the emergency department information system. Data were extracted from the warehouse using structured query language (SQL) for all presentations to the emergency department where the arrival date was between 1 January 2018 and 30 June 2019 inclusive. Patients who had more than one hs-TnI result within 24 h of arrival were included for analysis. Results for hs-TnI, creatinine and eGFR data were retrieved. Length of stay was calculated as the difference in hours between the arrival to and departure from the emergency department, and between the admission and discharge times of the inpatient stay. Primary diagnosis was retrieved for both emergency and inpatient stays. Discharge diagnosis codes, which were unrelated to a cardiac pathology and had a low overall frequency in each group (n < 5), were grouped together into the non-cardiac miscellaneous group.
Procedure coding data were retrieved and analysed for cardiac procedures (see online Appendix 1). Unplanned re-presentation was defined as a presentation to the emergency department within 28 days of being discharged from either the emergency department or inpatient stay. Unplanned readmission was defined as an admission with 28 days of hospital discharge where there was no documented intention to readmit.
Troponin Z-score calculation
Z-scores were calculated using the two consecutive hs-TnI results with specimens collected within 24 h. hs-TnI was performed using the Abbott Architect high-sensitivity troponin assay (Abbot Diagnostics, Abbott Park, IL). The assay has a coefficient of variation (CV) of 4% at a concentration of 20 ng/L and the troponin concentration at a CV of 10% for this is 4.7 ng/L. Sex-specific 99th percentiles for the assay are 26 ng/L for males and 16 ng/L for females. Only serial results where at least one of the results was above the sex specific 99th percentile were included.
Z-scores were calculated as described by Pretorius et al.
7
using the following equation

In equation (1), Δ is the difference between the serial troponin concentrations. SDAnalytical is the analytical standard deviation for the assay at the given mean troponin concentration. This was determined empirically for the Abbott Architect hs-TnI assay plotting the analytical SD for replicate troponin analysis over the range 10–200 ng/L which gives a linear relationship between SDAnalytical and troponin concentration (SDAnalytical = 0.03×TnI +0.5) (Supplemental File S1). SDBiological is the biological SD which was fixed at a value of 2 ng/L which is consistent with short term quoted intra-individual CVs of 5–15% for the Abbott Architect assays for Troponin concentrations values in healthy individuals. 10 A z-score greater than 1.96 is considered to represent a significant change at the 95% confidence level. For our analysis, a significant change was rounded off to a z-score greater than or equal to 2 after consensus from our clinical units.
Troponin Z-score interpretation
Patient episodes where the initial hs-TnI was greater than five times the sex specific 99th percentile (80 ng/L for females and 130 ng/L for males) were excluded, as these elevations have a high (>90%) positive predictive value for Type 1 acute coronary syndrome regardless of subsequent dynamic changes and indicated further inpatient evaluation.2,11
Presentations with an hs-TnI elevation above the sex-specific 99th percentile but less than five times the upper limit of the 99th percentile and an elevated z-score were classified as ‘acute myocardial injury’. Presentations with an hs-TnI elevation above the sex-specific 99th percentile but less than five times the upper limit of the 99th percentile and a normal z-score were classified as ‘myocardial injury’.
Statistics
Extracted data was imported into the R statistical computing environment for further analysis. 12 Proportions were expressed as percentages and non-parametric variables such as length of stay were presented as median and interquartile range. Normally distributed data were expressed as mean (±one standard deviation). Difference in proportions was assessed using chi-squared tests and difference in non-parametric variables was assessed using the Wilcoxon rank sum test with a P-value of <0.05 indicating significance.
Results
Troponin data
There were a total of 17,824 emergency presentations with at least one hs-TnI request over the study period (Figure 1). For 7088 presentations, more than one hs-TnI results were available in the first 24-h period. There were 3842 presentations for which the first and second hs-TnIs were both below the sex-specific 99th percentile, and 1184 presentations where the initial hs-TnI was greater than five times the sex-specific 99th percentile. These presentations with normal or extremely elevated hs-TnI were excluded from the analysis as specified in the method. Z-score was calculated for the remaining 2062 presentations. The median time between the collection of first and second hs-TnIs was 5.7 h (IQR 3.8–7.8 h).
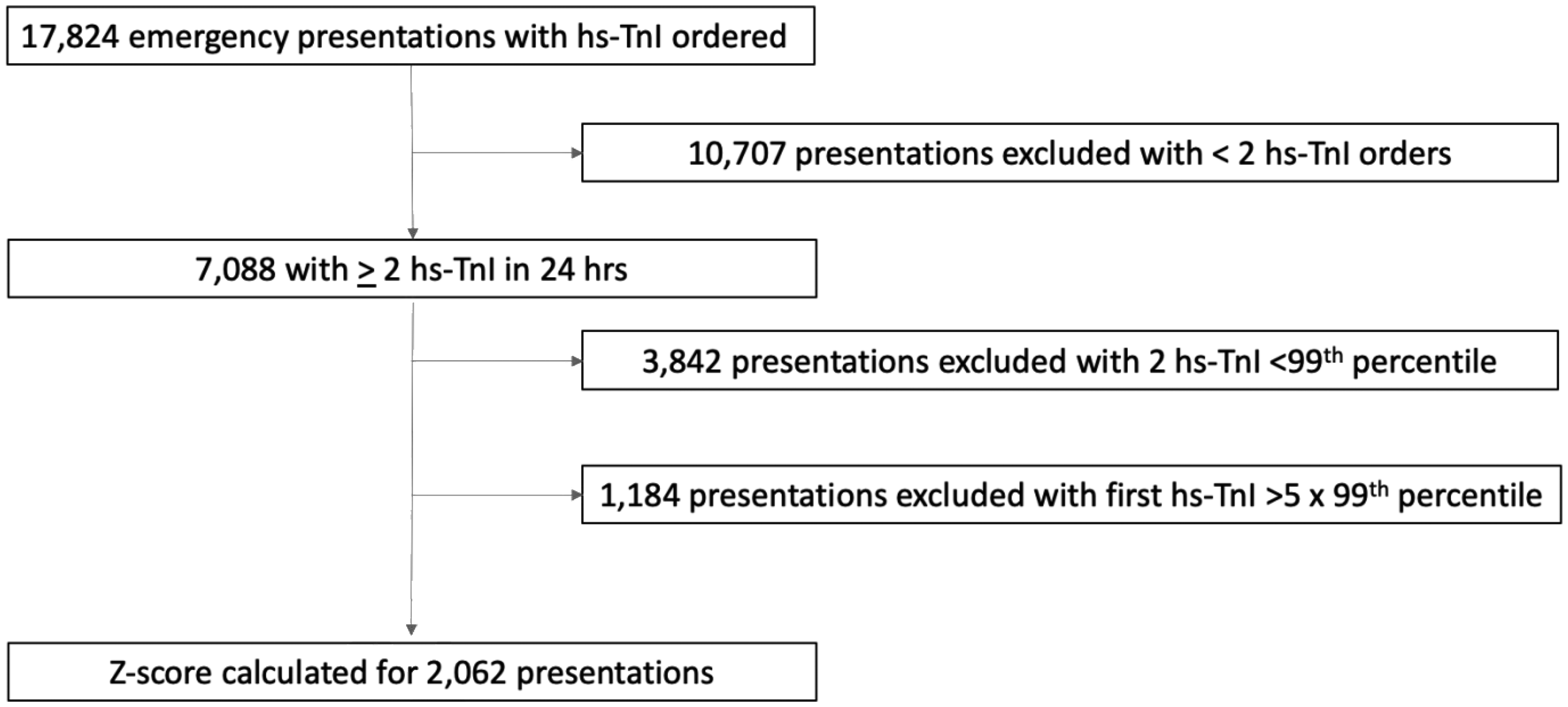
Flow chart for inclusion of presentations for analysis.
Patient characteristics
There were 2062 emergency presentations with eligible z-scores for a total of 1830 individual patients (1013 male and 817 female). Males were younger with a median age of 74 years (IQR 60–83) with females having a median age of 78 years (IQR 68–85) (P < 0.01). Z-score was elevated in 1080 (52%) presentations. Patient characteristics of the normal and elevated z-score cohorts are presented in Table 1. There was a higher proportion of male in the elevated z-score cohort (59% vs. 52%, P < 0.01). Initial hs-TnI and age were similar, presenting renal function differed with a higher proportion of CKD stage 1,2 and lower proportion of CKD stage 4,5 subjects in the high z-score cohort compared with normal z-score cohort (Table 1).
Patient characteristics and clinical outcomes for emergency presentations with acute myocardial injury and non-acute myocardial injury defined by troponin z-score.
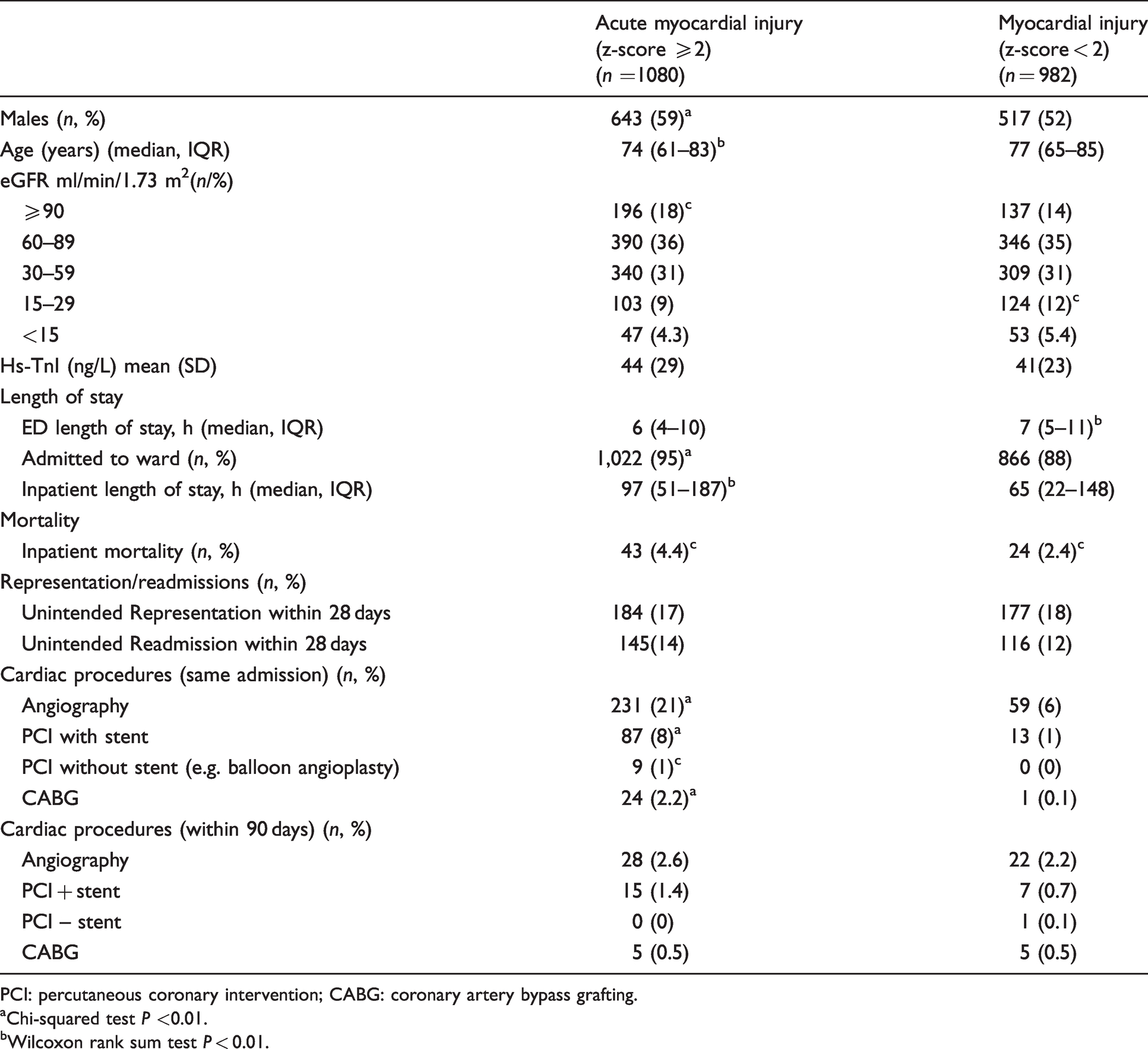
PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting.
aChi-squared test P <0.01.
bWilcoxon rank sum test P < 0.01.
Association of hs-TnI z-score with clinical outcomes
In the elevated z-score group, there was a higher proportion of AMI diagnosis (18% vs. 2.4%, P < 0.01), higher incidence of cardiac arrest (1.3% vs. 0%, P < 0.01) and paroxysmal tachycardias (2.6% vs. 1%, P < 0.05) and a lower number of ‘chest pain of an ‘unspecified cause’ diagnosis (3.6% vs. 10.9%, P < 0.01) when compared with the normal z-score cohort (Table 2). There were no differences in diagnoses of angina pectoris, COPD, heart failure, pulmonary embolism, stroke or sepsis between the groups.
Discharge diagnoses with acute myocardial injury and non-acute myocardial injury defined by troponin z-score.
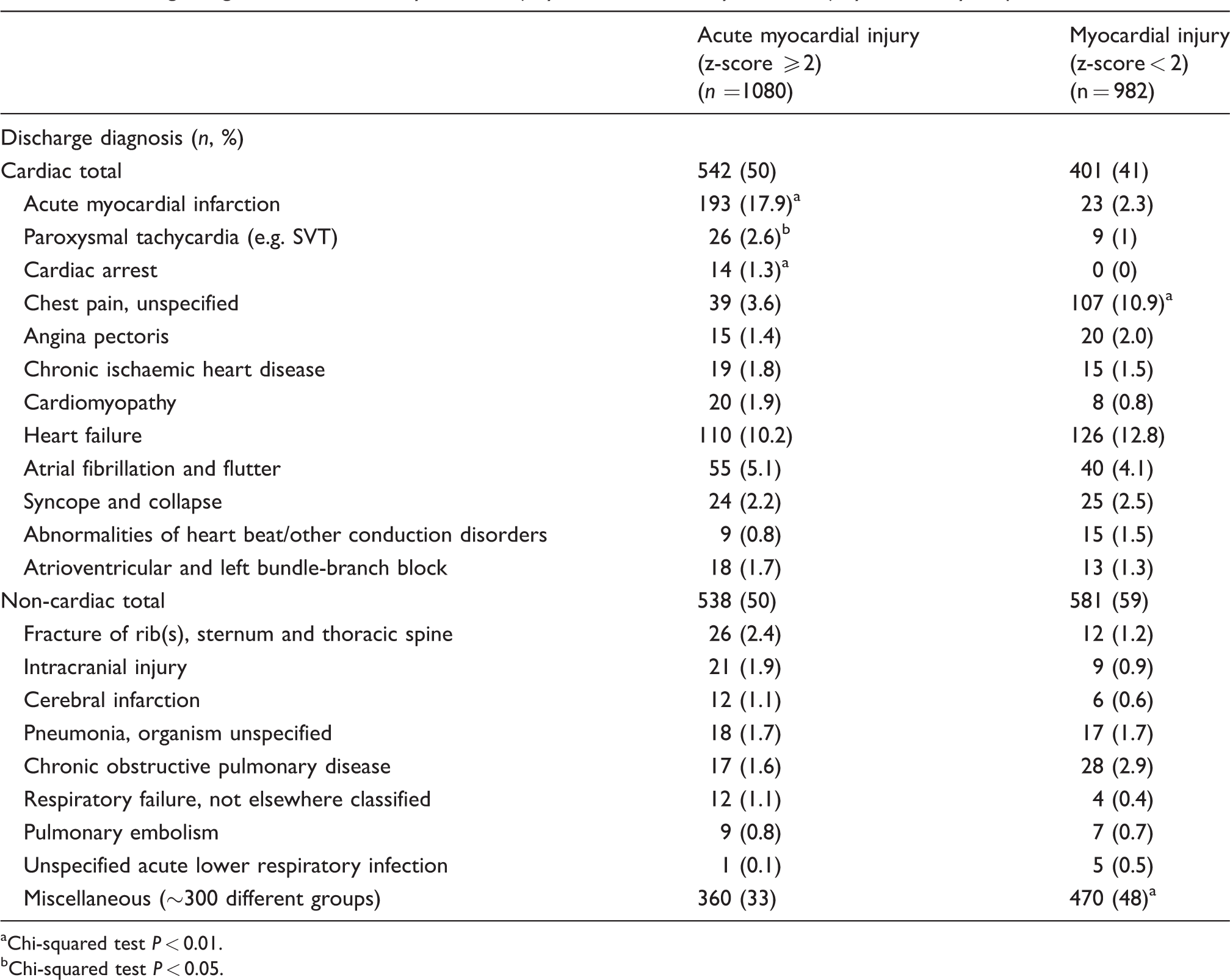
aChi-squared test P < 0.01.
bChi-squared test P < 0.05.
The prevalence of AMI diagnosis in all episodes eligible for z-score calculation was 10.4%. The use of elevated z-score alone for a diagnosis of AMI had a sensitivity of 89% and specificity of 51% (Table 3). In comparison, elevated hs-TnI on the first or second sample in ED had a sensitivity of 67% and 99%, with a specificity of 13% and 5%, respectively. Subjects with elevated z-score were more likely to have a diagnosis of AMI on discharge, with an odds ratio (OR) of 8.7 (P < 0.0001). Elevated hs-TnI on the first sample was not associated with AMI (P = 0.05), elevated hs-TnI on the second sample had an OR of 4.3 (P = 0.01).
Z-score and troponin status in predicting acute myocardial Infarction.
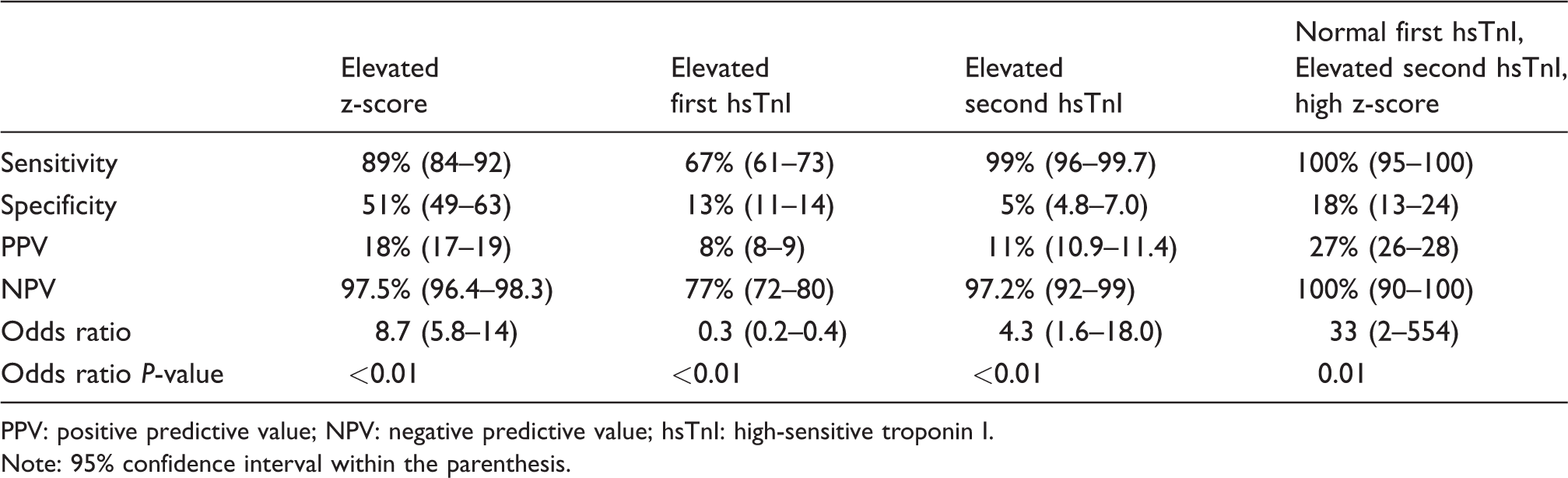
PPV: positive predictive value; NPV: negative predictive value; hsTnI: high-sensitive troponin I.
Note: 95% confidence interval within the parenthesis.
Emergency department length of stay was longer for patients with a low z-score (7 h vs. 6 h, P <0.01). Significantly more patients with elevated z-scores were admitted to an inpatient unit than those with a normal z-score (95% vs. 88%, P < 0.01). For those patients admitted, inpatient length of stay was significantly longer for patients with an elevated z-score (97 h vs. 65 h, P <0.01), inpatient mortality was also higher (4.4% vs. 2.4%, P = 0.018). Following discharge, unintended readmission and unintended representation within 28 days did not differ between groups (17% vs. 18% and 14% vs. 12%, P = 0.59 and P = 0.3, respectively).
With regard to cardiac procedures, patients with an elevated z-score were more likely to undergo angiography (21% vs. 6%, P <0.01), PCI with stenting (8% vs. 1%, P <0.01) and CABG (24% vs. 1%, P <0.01) during the same admission (Table 1). For inpatients who proceeded to angiography, the rate of PCI with stent was higher in patients with an elevated z-score (38% vs. 22%, P < 0.05). There was no significant difference in cardiac procedures performed in the outpatient setting (within 90 days postdischarge) between the high and normal z-score groups.
Discussion
Measurement of cardiac troponin is mandatory in all patients with suspected non-ST elevation acute coronary syndrome). 2 With the evolution and widespread uptake of higher sensitivity hs-Tn assays, elevations above the 99th percentile upper reference limit are common in diseases other than AMI, 13 leading to an increased proportion of emergency presentations with elevated hs-Tn results.14,15 When hs-TnI was first introduced to our hospital in 2013, there was an increase in the proportion of patients admitted via emergency department while the rate of interventional cardiac procedure and the number of AMI diagnosis remained unchanged when compared with the period when non-high sensitivity troponin assay was used. 6 Similar to previous findings, we note in this study that only 46% of emergency department admissions with a mild-to-moderate hs-TnI elevation had a final discharge diagnosis relating to cardiac associated pathology, and only 10.4% had a final diagnosis of AMI. Troponin elevations that may not be due to an ACS can be a source of confusion within emergency departments with flow on effects for patient disposition and hospital length of stay, particularly since chest pain is one of the most common presentations to emergency departments worldwide. 16 The holy grail is therefore to rapidly differentiate AMI1,2 requiring inpatient treatment, from a heterogeneous group of pathologies causing chronic myocardial injury and non-dynamic/persistent hs-Tn elevation.
High sensitivity troponin rises rapidly, usually within 1 h of symptom onset. 17 What constitutes a significant hs-Tn rise is controversial, affected by the assay used, baseline hs-Tn concentration and timing of serial sampling. A significant change was stated as >20% change between serial hs-Tn samples in the Fourth Universal Definition of Myocardial infarction Consensus for patients post cardiac procedures. 1 The European Society of Cardiology Working Group on Acute Cardiac Care recommends a significant change of >50% where the initial hs-Tn concentration was ≤99th percentile or >20% when the initial concentration was >99th percentile. 18 However, the least significant change in hs-Tn differs between assays due to variation in assay-specific precision and published biological variation values. 7 For instance, an Abbott hs-TnI serial troponin of 2 and 7 ng/L constitutes a 250% change, and yet the calculated z-score is normal at 1.7 and not significantly different according to assay-specific variation. Similarly, for an elevated hs-TnI serial troponin of 22 and 28 ng/L, this constitutes a 27% change, the calculated z-score remains normal at 1.8. Z-score has been proposed as a tool to assist clinical interpretation of hs-Tn changes across immunoassays. In a prospective study with serial hs-Tn collection at 0, 2 and 6 h, z-score was found to have similar diagnostic accuracy for AMI across different hs-Tn assays. 5 However, to date, there is no real-world data to evaluate clinical outcomes and patients with dynamic vs. non-dynamic hs-Tn elevations as defined by z-score. The 2020 European Society of Cardiology guideline provided some assay-specific absolute 1 h and 2 h serial hs-Tn cut-off as a guide. 2 However, re-testing interval of 1–2 h is not always practical in most ED, and the use of rule in and rule out absolute delta may cause confusion for clinicians who work across multiple locations with different hs-Tn assays.
In this study, we retrospectively explored the relationship between z-score and clinical outcome data prior to the introduction of automated z-score reporting in our laboratory information system. We found presentation with an elevated but non-dynamic (z-score < 2) hs-TnI was associated with a higher length of stay within the emergency department (7 h vs. 6 h, P < 0.01). The longer length of stay for the non-dynamic hs-TnI cohort was likely due to the need for a second hs-TnI concentration in low risk patients with elevated initial hs-TnI. Review of these cases showed that the majority (61%) were patients presenting with chest pain and admitted to the emergency short stay unit for serial hs-TnI monitoring, and then discharged with no underlying pathology being identified. The low cardiac risk is reflected by the higher rate of non-specific chest pain and miscellaneous non-cardiac diagnoses in the discharge documentation. The higher prevalence of CKD stage 4 and 5 in the non-dynamic cohort might also have contributed to the initial elevated hs-TnI, since up to 70% of CKD subjects have persistently elevated hs-Tn without cardiac symptoms. 8
In stark contrast, presentation with elevated and dynamic (z-score ≥ 2) hs-TnI was associated with a higher rate of hospital admission and longer inpatient length of stay. Despite presenting with an initial hs-TnI concentration comparable to the normal z-score cohort, a high z-score was associated with poorer inpatient outcomes including a higher rate of cardiac arrest and inpatient mortality. In addition, the diagnosis of AMI was eight-fold higher and inpatient cardiac intervention was three-fold higher compared with the normal z-score cohort, confirming the role of z-score as a useful marker of acute myocardial injury and that cardiac risks are associated with the dynamics of hs-TnI release rather than the absolute magnitude in patients presenting with mild-to-moderate hs-TnI elevation.
The use of z-score alone was reasonably sensitive (89%) but was not specific (52%) for a diagnosis of AMI; this is because other non-cardiac diagnoses are still prevalent in the high z-score cohort. Compared with a z-score study using Beckman-Coulter hs-TnI assay in a cohort presenting with symptoms of ACS to predict Type 1 AMI, our sensitivity was higher (89% vs. 79%), but specificity was lower (52% vs. 93%). 5 The subject selection differs as we applied the z-score to all emergency presentations with serial hs-TnI measurements and did not pre-select patients with documented ACS symptoms or ECG changes. Our study therefore reflects real-world request pattern of hs-Tn in the emergency department, whereby a normal z-score ruled out AMI in 97.5% of subjects with at least one elevated hs-TnI (odds ratio for AMI, 8.7, P < 0.01). Although a low second hs-TnI alone independently ruled out AMI in 97.2% of subjects, The odds ratio of an elevated second hs-TnI for AMI was lower at 4.3. A combination of a low first troponin and an elevated second troponin with a low z-score had a 100% negative predictive value for AMI in this cohort. This indicates the potential for z-score to replace assay-specific absolute delta changes specified in AMI rule out algorithms and should be validated in larger studies.
Postdischarge parameters did not differ between the groups. The normal z-score cohort was more likely to be directly discharged from emergency department; the 28-day representation and readmission rates were similar to the high z-score cohort. hs-TnI elevation is known to be associated with adverse outcomes and patients with myocardial injury have a poor prognosis with mortality similar to patients with myocardial infarction. 19 Postdischarge cardiac interventions also did not differ between the groups.
Our study has several limitations. This was a single-center study and our findings are reflective of local disease prevalence and may not apply to other institutions. However, with the exception of trauma presentations, the case mix of our emergency department is similar to other metropolitan hospitals in developed countries in terms of volume and prevalence of AMI. 15 Our median serial hs-TnI collection interval was 5.7 h, and the clinical outcome might differ with an earlier resampling timeframe. Australian guidelines for suspected ACS suggest repeat testing at 2–3 h for high sensitivity assays. 6 Neumann et al. found that the required absolute delta between serial hs-Tn is greater in the late resampling (120–210 min) cohort compared with the early resampling (45–120 min) cohort to achieve the same negative predictive value for AMI. 15 The retrospective nature of our study was necessary, as patient outcome measures will be influenced after the introduction of automated calculated z-score reporting in our electronic medical record. Our study has the strength of direct extraction of discharge and intervention outcome data, and therefore was not prone to observer bias from manual medical record review. Unlike other prospective studies, we applied the z-score to all presentations with at least one elevated hs-TnI value without pre-selection for acute coronary syndrome using clinical criteria. This reflects real-world troponin request pattern in emergency departments. We used the Abbott Architect hs-TnI assay and our results may not be generalizable to other assay platforms, although as shown by Pretorius et al., the z-score has benefits of being platform-independent relative to absolute or relative delta measurements. 5
In summary, the use of calculated z-score as a quantitative dynamic measure of serial troponins was associated with higher odds of AMI diagnosis, hospital admission rate, inpatient cardiac intervention rate, inpatient length of stay and mortality. Automated calculation of z-score is transferable across hs-Tn assays and can be a powerful tool to alert clinicians of dynamic elevated hs-Tn in real-time, thereby enabling rapid triage of AMI risk, improve emergency department workflow and cost saving via overall reduced hospital length of stay.
Supplemental Material
sj-pdf-1-acb-10.1177_0004563221992812 - Supplemental material for Troponin least significant change (z-score) is associated with poor clinical outcomes in patients presenting to the emergency department
Supplemental material, sj-pdf-1-acb-10.1177_0004563221992812 for Troponin least significant change (z-score) is associated with poor clinical outcomes in patients presenting to the emergency department by Joel D Smith, Kai'En Leong, Timothy Fazio and Cherie Chiang in Annals of Clinical Biochemistry
Footnotes
Acknowledgements
The authors wish to acknowledge Dr. Carel Pretorius, Pathology Queensland for assistance and advice in the development of the z-score for our assay.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This retrospective validation study was approved by the Melbourne Health Office for Research (Project Number QA2019134).
Guarantor
JDS.
Contributorship
JDS, TF, KL and CC conceived the study. TF extracted the data. JDS performed the data analysis. JDS wrote the first draft of the article. All authors reviewed and edited the article and approved the final version of the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.