
Abstract
Background
Current sampling and transport conditions of samples in general practice can result in pseudohyperkalaemia. This study was undertaken to determine, in a general practice setting, whether there is any difference in haemolysis obtained when using BD Vacutainer® Rapid Serum Tubes (BD RST) compared with using BD Vacutainer® SST™ II Advance Blood Collection Tubes (BD SSTII).
Methods
Blood was collected from 353 patients requiring blood sampling who were attending 31 general practitioner practices in Belgium. For each patient, two BD SSTII tubes and two BD RST tubes were drawn in a randomized order. One of each pair of tubes was inverted five times, the other was not. Serum potassium concentration, serum LDH activity and haemolysis index were measured in each sample.
Results
There was no significant difference in measured potassium concentration according to tube type (P = 0.16). Measured LDH activities were 1.7% higher in serum collected into BD SSTII tubes compared to BD RST tubes (P = 0.02). When comparing serum from unmixed BD RST with BD SSTII tubes, there was a slight reduction in the haemolysis index but no significant difference in measured potassium concentration or LDH activity. Risk of hyperkalaemia was 4.8 times higher in serum from tubes that were incompletely filled compared to those that were filled with the correct amount of blood.
Conclusion
Both types of blood tubes are suitable for the measurement of serum potassium and LDH in patients from general practice. Tube inversion does not improve the accuracy of either serum potassium or LDH measurement. Blood tubes should be filled to the level recommended by the manufacturer to avoid artefactual increases in measured serum potassium concentration and LDH activity.
Introduction
Detecting hyperkalaemia in patients attending general practice is important. Hyperkalaemia may result from many causes, including renal failure, treatment with ACE inhibitors, potassium-sparing diuretics or other drugs and, if severe enough, can result in sudden death.1–3 In a study from 2010 of patients registered with a general practice in Belgium, the overall proportion of patients with hyperkalaemia was 15%. 4 However, a significant proportion of instances of hyperkalaemia may be artificial and be factitious in nature. Such factitious hyperkalaemia may arise from, e.g. inappropriate procedures for specimen collection, specimen processing and handling and specimen transport.5–7
In general, the reliable monitoring of serum potassium concentrations in patients attending general practitioners (GPs) can be difficult. A typical blood sample may be collected in the surgery in the morning and remain in the practice for up to several hours until collection. Once collected, further delays may occur while the transport vehicle collects specimens from other surgeries before finally delivering them to the laboratory several hours later. Although GPs and transport companies can be instructed about optimal sample storage conditions in order to minimize haemolysis, haemolysis does remain a widespread problem. Although centrifugation of specimens has been introduced in some surgeries, in many instances, this is not an option because small practices do not have the time or resources to do this. In a pilot study, dual samples were taken from 50 patients where one sample from each patient was transported as collected, and the other sample was centrifuged within 5 min and the serum was transferred into a different tube prior to transportation. The results were largely similar. A systematic search of PubMed did not provide any additional methodological solutions to the problem.
BD has recently released a new serum tube with a thrombin-based rapid clot activated solution that enables clot formation in 5 min (BD Vacutainer® Rapid Serum Tubes, BD RST) compared with 30 min for the conventional BD SST II Advance tube (BD SSTII). Studies of this new type of container in hospital patients have shown slightly lower mean values for measured LDH and potassium compared to values obtained using either the BD SST II tube 8 or standard lithium-heparin plasma separator tubes. 9 One explanation for this difference is that the rapid clotting promoted by the BD RST tubes leads to a more compact and robust clot, which results in less red cell disruption and therefore a reduction in haemolysis. The present study was therefore undertaken to determine the effect of using the BD RST tube to collect blood from patients in GP surgeries and ascertain whether it resulted in reduced haemolysis and therefore fewer instances of factitious hyperkalaemia.
Materials and methods
Participating GPs were provided with all materials necessary for the blood collection, together with an overview card with the exclusion criteria and the tube-handling protocol. Additionally, a poster was supplied for the surgery waiting room to inform patients that their GP was participating in a trial in which patients could volunteer to participate. Patients over the age of 20 who visited their GP to have a blood test were included in the trial after signing an informed consent form. Exclusion criteria were age, samples collected at night or during weekends, samples collected in laboratories and those instances where it was considered that participation could interfere with a patient’s current or future medical treatment.
Devices and handling procedures
Study tubes.
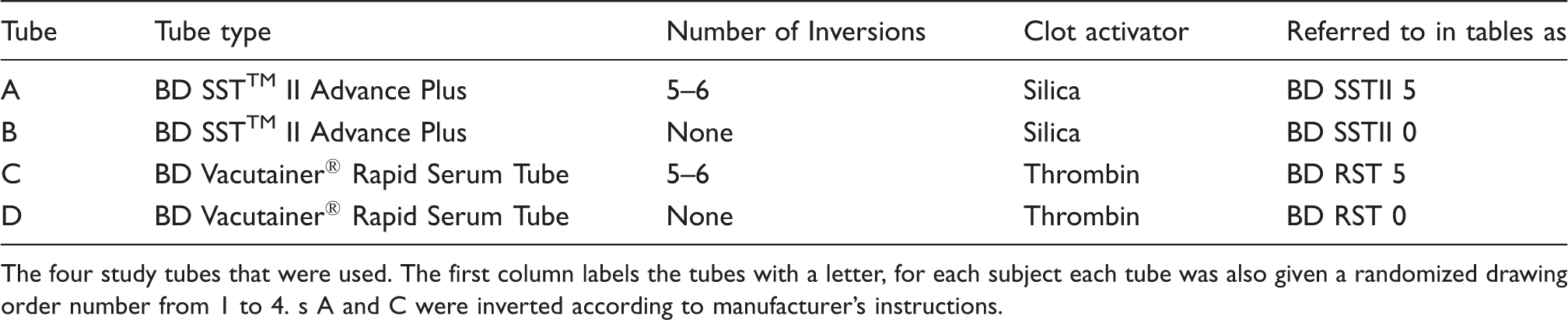
The four study tubes that were used. The first column labels the tubes with a letter, for each subject each tube was also given a randomized drawing order number from 1 to 4. s A and C were inverted according to manufacturer’s instructions.
Each bag was completed with an informed consent form and a data report form (DRF). Each GP marked the date and time of venipuncture, use of ACE-inhibitors or diuretics by the patient, location, any difficulty during venipuncture and confirmation of correct mixing of the tubes on the DRF. The receiving laboratory added transport time and correct fill volume to the DRF. Incorrect filling was defined as the blood concentration being less than 10% below the mark on the tube.
Laboratory procedures
Prior to starting the study, inter-laboratory testing was performed, to verify harmonization of test results, including haemolysis index and centrifugation practices. All research forms, except the informed consent forms, were anonymized. For each patient, four serum tubes were taken, two BD RST and two BD SSTII tubes. The drawing order of these four serum tubes was randomized, and for each patient, the drawing order of the four tubes was indicated on the study bag. One tube of each type was inverted five times, according to the manufacturer’s recommendations, while the other tube of each pair was not. Serum potassium, LDH and haemolysis index were measured on all samples according to standard laboratory procedures. The potassium and LDH assays were performed on either a Roche Modular System or an Olympus AU680 analyser according to the manufacturer’s instructions. With these fully automated methods, there was no need for blinding of test results. Reference values for serum potassium for both laboratories are 3.5–5.1 mmol/L, and for LDH, less than 248 U/L for the Practimed Tessenderlo laboratory and less than 480 U/L for the MCH Leuven laboratory. The haemolysis index was displayed as six categories ranging from ‘normal’ to ‘+++++’. Those categories represent the following concentrations (mg/L) of serum haemoglobin: ‘normal’ = <50; ‘+’ = 50–99; ‘++’ = 100–199; ‘+++’ = 200–299; ‘++++’ = 300–500 and ‘+++++’ = >500. All movements (from collection point to delivery) of the serum tubes were marked on the registration forms.
Statistical analysis
This study was designed to investigate whether there was a difference in measured serum potassium, LDH and haemolysis index in blood collected in BD RST and blood collected in BD SST II tubes. The effect of mixing by inversion and incompletely filling the tubes on these parameters was also studied.
Serum potassium concentrations and LDH activities are continuous rather than discrete variables and were analysed by the following model: y = β0 + β1Subject + β2Tube + β3Inversion + β4(Tube × Inversion) + error, where y is either the response or the natural log of the response, depending on the distribution of the data. The model reported differences for each possible combination of the different tube types (e.g. BD RST 5 inversions versus BD RST 0 inversions).
Each subject is accounted for as a grouping variable for the continuous responses. Haemolysis index, hyperkalaemia and elevated LDH activity were evaluated using logistic regression analysis. Additional characteristics, such as transportation time, location of sample collection and correct filling, were taken into account as independent variables. Differences in the proportions of increased results were calculated and tested using a Fisher exact test for each of the transport systems. The Fisher test was conducted for the entire matrix and, if significance was found, additional testing was done to isolate the source of difference. Finally, Bland–Altman analysis was performed for measured serum potassium and LDH values.
The study was undertaken in accordance with the requirements of the Helsinki declarations. All patients gave written informed consent and the study protocol was approved by the Medical Ethical Board of University Hospitals K.U. Leuven (No. S52761).
Results
Description of the population
Two regional Laboratories analysed blood samples: MCH Leuven and Practimed Tessenderlo. Of the 31 participating GPs, five worked with MCH Leuven and 26 with Practimed Tessenderlo. Blood samples were taken between 26 April 2011 and the 20 June 2011.
Characteristics of the study population by laboratory and tube type (last five lines).
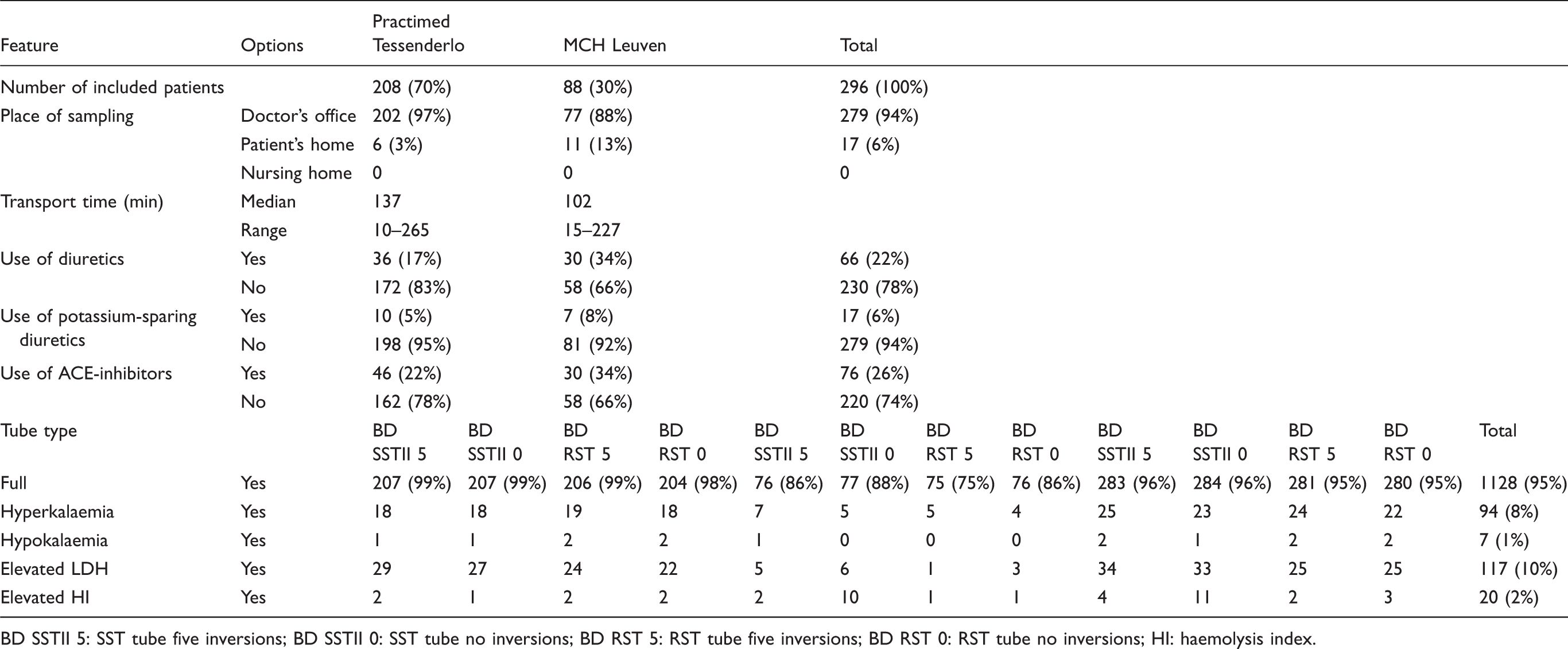
BD SSTII 5: SST tube five inversions; BD SSTII 0: SST tube no inversions; BD RST 5: RST tube five inversions; BD RST 0: RST tube no inversions; HI: haemolysis index.
Of the all included samples, 6% were taken at the patients’ homes; all other samples were taken at the GPs’ offices. There were some difficulties in collecting the blood in 14 (5%) of the samples. Transport time – from pick-up in the GP’s office until arrival in the laboratory – ranged from 10 to 265 min. Out of the 296 subjects included in the study, 22% were on diuretics, 6% on potassium sparing diuretics and 26% on ACE-inhibitors.
A total of 1128 (95%) of all 1184 tubes received were completely filled. Nine of the 31 GPs delivered at least one serum tube that was incompletely filled. Hyperkalaemia was observed in 8% of all the tubes; 10% showed elevated LDH concentrations and 2% had an abnormal haemolysis index (of which 80% were only slightly haemolysed, being in category ‘+’).
Performance of the different tubes
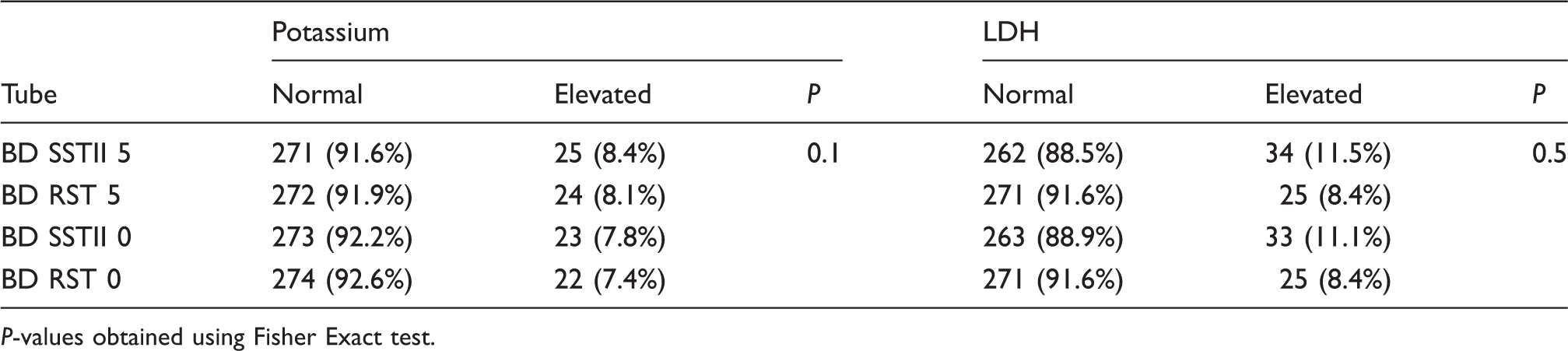
Measured LDH activities in serum collected in BD RST tubes were lower than in serum collected from SSTII tubes (P = 0.02), although there was no observed difference in measured potassium concentration (Table 3). There was little or no difference in serum potassium and slightly lower serum LDH concentrations in the BD RST compared with the BD SSTII tubes. There was no significant difference between BD RST and BD SSTII tubes for hyperkalaemia and elevated serum LDH (Table 4). The Bland–Altman plot showed that the different tubes had no influence on the mean potassium values in our results (Figure 1).
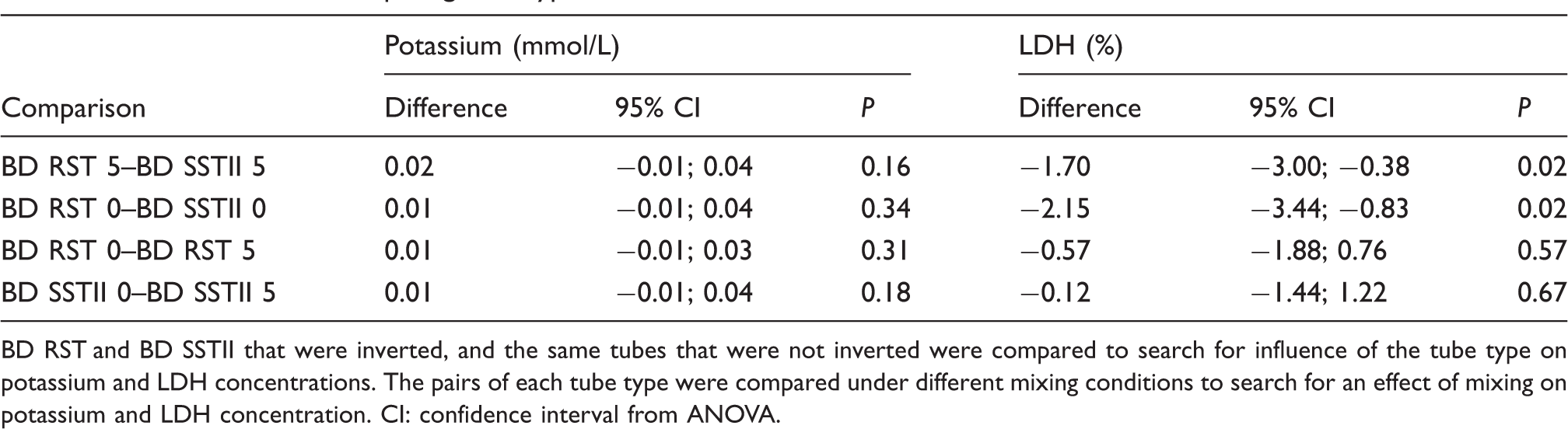
Bland–Altman analysis of difference between both serum tubes according to mean potassium values. K: potassium, 5 Inv: the serum tube was inverted five times. Difference when comparing tube types and inversions. BD RST and BD SSTII that were inverted, and the same tubes that were not inverted were compared to search for influence of the tube type on potassium and LDH concentrations. The pairs of each tube type were compared under different mixing conditions to search for an effect of mixing on potassium and LDH concentration. CI: confidence interval from ANOVA. Proportion of normal and elevated serum potassium and LDH concentrations for the different tube types. P-values obtained using Fisher Exact test.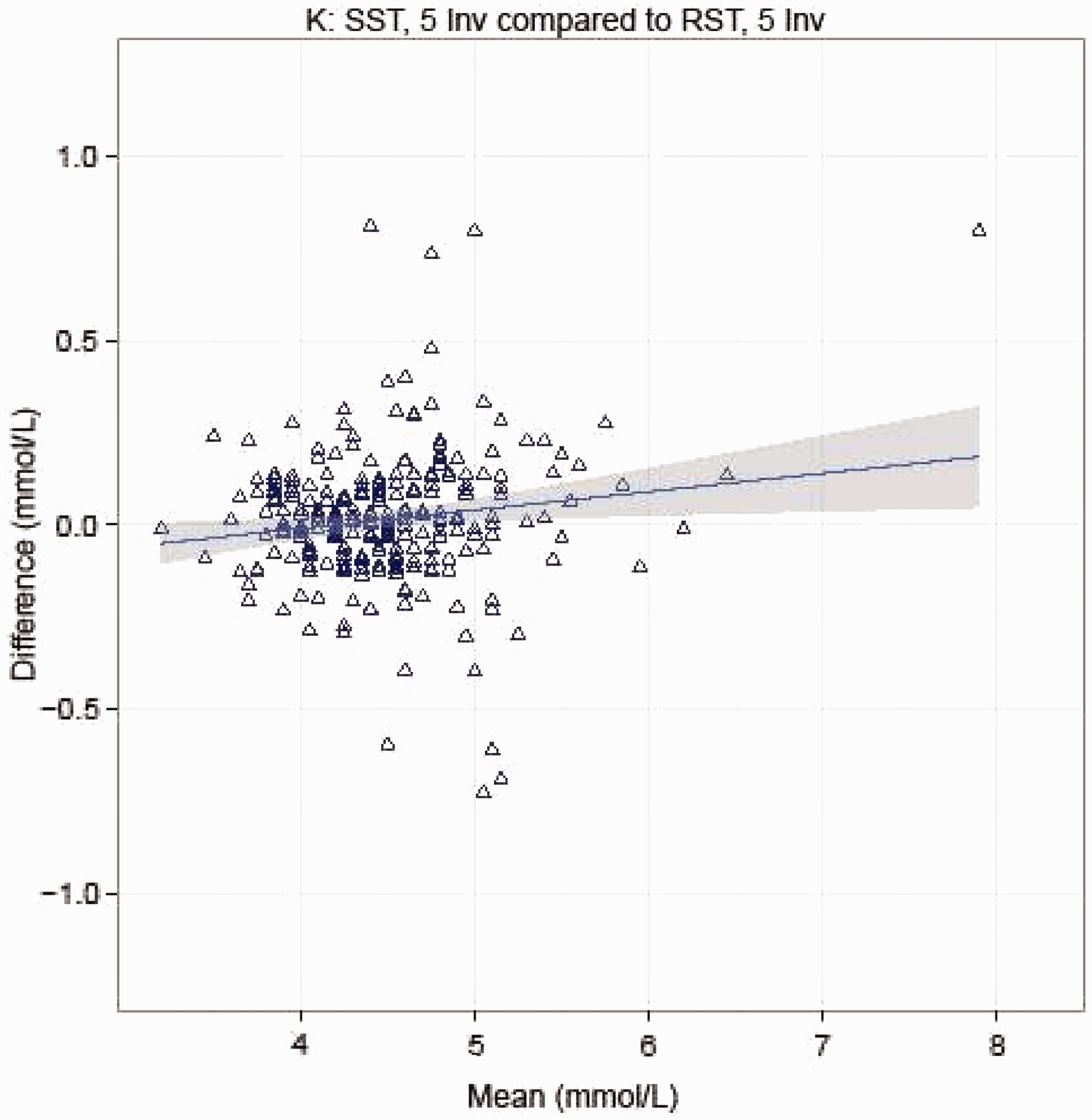
Effect of correct mixing
Mixing the tubes resulted in little or no difference in measured serum potassium or LDH compared with values obtained in those that were not mixed (Table 3). It also did not result in any significant difference in the incidence of hyperkalaemia or elevated serum LDH activity (Table 4).
The unmixed BD RST produced slightly improved sample quality (based upon Haemolysis index) when compared with the unmixed BD SSTII (P = 0.05). The Bland–Altman plot showed that this had no influence on the mean potassium values in our results (not shown).
Effect of other variables
Influence of characteristics on outcome measures.
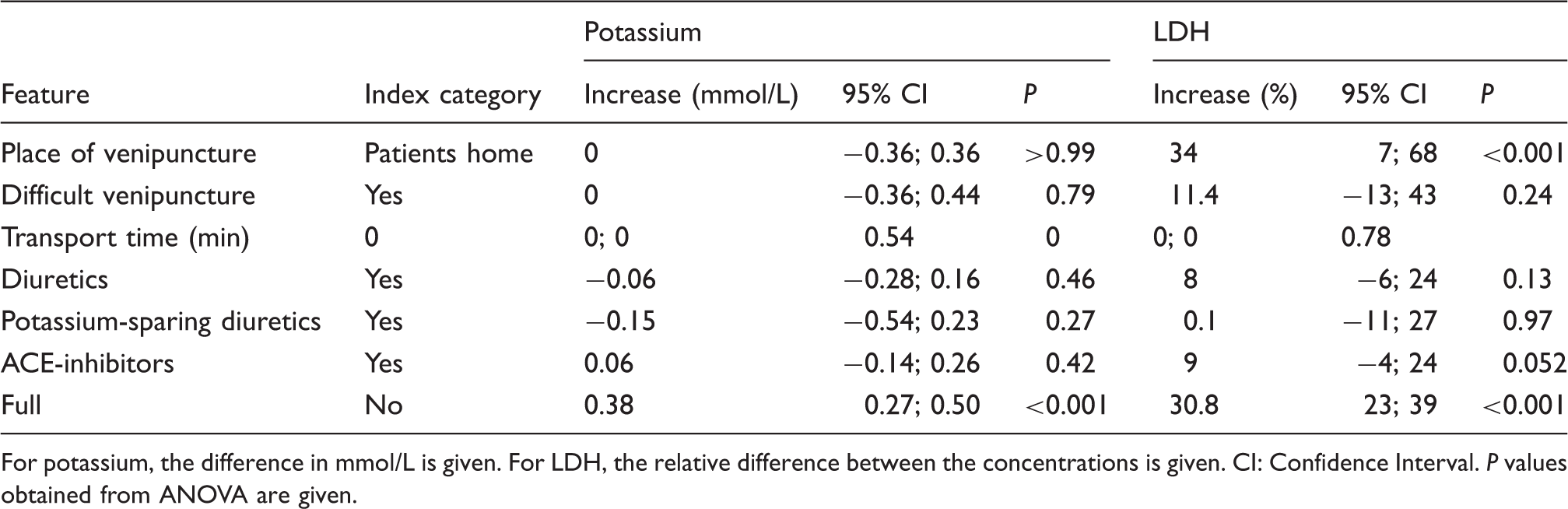
For potassium, the difference in mmol/L is given. For LDH, the relative difference between the concentrations is given. CI: Confidence Interval. P values obtained from ANOVA are given.
The other covariates, namely, place of venipuncture, transport time, diuretic medication and treatment with ACE inhibitors all showed no effect on measured serum potassium concentration or LDH activities (Table 5).
Discussion
The BD RST tubes showed no benefit over the BD SSTII tubes in preventing hyperkalaemia or increased LDH activities. Although the results for the BD RST tubes showed a statistically significant small difference in LDH activities compared to the BD SST II tubes, these are not clinically significant, as the bias is only 1.7 U/L.
In addition, correct mixing of the tubes made no significant difference in preventing hyperkalaemia or elevated LDH activities. However, the BD RST is likely to produce a slightly improved sample quality than the BD SSTII tube when not inverted. Serum in those tubes that were incompletely filled, however, showed higher mean serum potassium and higher LDH values, and nearly a five times higher risk of hyperkalaemia than serum in tubes that were correctly filled.
The overall prevalence of hyperkalaemia in this survey was 8% which was lower than the proportion found in the GP-based Intego database, in which 15% of all potassium values measured in one year were too high. 4 In a US hospital-based study, hyperkalaemia was found in 1–10% of all of the samples studied. 10 In one publication, in a hospital environment, the mean LDH and potassium values were slightly lower for serum obtained by collecting blood into the BD RST tubes than serum obtained by collection into the BD SST II tubes. 8 In our GP practice-based study, slightly lower means for LDH activity were also observed in serum collected into the BD RST tubes, but no effect was observed on the potassium concentrations.
A search on PubMed using the terms ‘pseudohyperkalaemia OR spurious hyperkalaemia OR pseudohyperkalaemia OR spurious hyperkalaemia OR pseudohyperkalaemia OR factitious hyperkalaemia’ returned no study results either in favour of or against an effect of correct mixing or correct filling of the tubes on potassium concentrations.
Seamark et al. 7 investigated the effect of the transport time of serum tubes from the general practitioner’s office to the laboratory on the presence of hyperkalaemia. They found that transport time was not a significant predictor variable, a finding confirmed in the present study.
Two laboratories and 31 GPs collaborated with this study. Together, they processed 353 sets of tubes of which 296 could be used for analysis. This means that a sufficiently large sample of the adult people population visiting their GP for a blood draw was included and distributed over two large regions of the country. All samples were taken in a daily clinical situation as part of routine clinical practice. Our results therefore reflect the normal routine situation and we believe this limits the effect of potential selection bias on our results.
The effect of tube handling on each of the three outcomes (potassium concentration, LDH activity and haemolysis index) is independent and no statistical adjustment has been made. The study was not undertaken to show superiority or equivalence of one tube but rather an observational study to explore handling issues. For observational studies, no statistical power is calculated for the study as no formal hypothesis is tested.
Missing or incomplete data are a potential source of bias though with a large sample size (n = 296), the missing data would not have impacted the conclusions made from the study.
The use of two different laboratories with different ranges (at least for LDH) could be considered a possible problem. However, all comparisons have been performed within and not between laboratories, and we corrected for the laboratory during analysis. The prevalence of a raised haemolysis index in our survey was very low. Therefore, we did not analyse this parameter in detail. It is strange that almost all (10/11) incompletely filled tubes were found in one of the regions and related to one of the laboratories. Although we do not have a reasonable explanation for this finding, it does not influence our conclusion in this respect.
In conclusion, this study has essentially showed no difference between the performance of the BD RST and BD SST II tubes when used correctly. Any significant differences observed between analyte concentrations measured were small and not clinically significant. Even when the tubes were not mixed after blood collection, there was no observed difference in tube performance. However, the study has shown that it is essential that both type of blood collection tube are filled to the correct volume since under-filling tubes results in elevated analyte values being obtained. We therefore strongly recommend that all those involved in blood collection are made aware of the importance of correct filling of tubes, and the potential implications of unreliability of any results obtained, if tubes are not filled correctly.
Footnotes
Acknowledgements
We would like to thank all the general practitioners and the laboratory teams that cooperated voluntarily in the study. We also thank Marina Devis for providing all the practical support to the study.
Declaration of conflicting interests
Statistical analysis of the data collected by the clinical and academic authors (TH, FB, RB, VB, JV and NB) was completed by the BD statistical team (the producer of the tubes used in the study), and partially checked by the second author (FB). All interpretations and conclusions are by the clinical and academic authors, who declare no conflict of interest.
Funding
All study material was supplied by BD. There was no additional funding for this study.
Ethical approval
The study protocol was approved by the Ethical Medical Board of University Hospitals K.U. Leuven (S52761).
Guarantor
FB.
Contributorship
TH completed the study protocol and was the main organizer of data collection drafting and revising the manuscript. FB formulated the study and design, conducted part of the analysis and discussed the draft manuscript. RB helped in designing the study and protocol and engaged in a critical discussion of the draft manuscript. VB and JV helped in designing the protocol and organization of the data collection and engaged in a critical discussion of the draft manuscript. SC, KB and RR helped in designing the protocol, analysing results and engaged in a critical discussion of the draft manuscript. NB formulated part of the analysis and contributed to the draft manuscript. All authors agreed on the final version of the manuscript.