
Abstract
Background
Faecal calprotectin has been widely used as a non-invasive marker of intestinal inflammation in children. Measurement of faecal haemoglobin using faecal immunochemical test is well established in adults for detection of colorectal cancer. In adults, faecal haemoglobin has been recommended as a reliable tool to aid identification of those at low risk of significant bowel disease and has also been used in inflammatory bowel disease to assess mucosal healing.
Aims
We aimed to evaluate the performance of faecal haemoglobin in the paediatric population and compare it with faecal calprotectin.
Methods
Children being assessed in the paediatric gastroenterology clinic for bowel symptoms had a sample sent for both faecal calprotectin and faecal haemoglobin. Samples were collected over a 10-month period from November 2018 to September 2019. Faecal haemoglobin was measured using an OC-Sensor. Faecal calprotectin was measured using Liason®Calprotectin.
Results
One hundred forty three samples were returned for faecal haemoglobin and in 107 a paired faecal calprotectin was also available. Faecal haemoglobin correlated with faecal calprotectin, Spearman’s rank coefficient 0.656 (P < 0.0001). There were 35 patients with faecal haemoglobin >20 μg/g and in 32 of these patients faecal calprotectin was >200 μg/g; 74 patients with faecal haemoglobin and 38 patients with faecal calprotectin underwent colonoscopy. Patients with normal histology had faecal haemoglobin <4 μg/g; faecal haemoglobin >20 µg/g was associated with signification inflammation
Conclusion
Our study is the first to compare faecal haemoglobin and faecal calprotectin in a paediatric population. Results suggest that faecal haemoglobin correlates with faecal calprotectin and, as in adults, may be useful to rule out significant bowel disease. A faecal haemoglobin >20 μg/g was consistent with significant histological inflammation.
Keywords
Introduction
Calprotectin is a member of the S100 family of proteins derived predominantly from neutrophils. It is found in body fluids in an amount proportionate to the severity of any existing inflammation which led to the concept of its measurement in faeces as a surrogate marker of gastrointestinal inflammation. Faecal calprotectin (FCP) is recommended by NICE for use in children to differentiate between inflammatory bowel disease (IBD) and non-IBD. 1 In patients with known IBD, FCP has been shown to correlate with disease severity on colonoscopy and to predict relapse. 2
Measurement of faecal haemoglobin (f-Hb) using a faecal immunochemical test (FIT) is well established worldwide in colorectal cancer (CRC) screening programmes and was recommended by NICE for symptomatic patients at low risk of CRC. 3 However, during the COVID-19 pandemic, in the context of reduced colonoscopy availability, f-Hb has been recommended in all patients as part of the referral pathway, the amount of f-Hb present informing triage. 4 In adults, f-Hb has been shown to be reliable as an objective way of identifying patients with an extremely low risk not only of CRC but of significant bowel disease (i.e. CRC, higher-risk adenomas and IBD) thus avoiding invasive investigation. 5 Studies in countries where f-Hb is freely available for CRC screening but access to FCP is limited, have shown that f-Hb is a reliable marker for predicting mucosal healing in patients with ulcerative colitis (UC). 6
The aim of this study was to evaluate the performance of f-Hb in the paediatric population and compare it with that of FCP.
Methods
Patients
This prospective study looked at children being assessed for bowel symptoms in the paediatric gastroenterology clinic at a tertiary children’s hospital. When clinicians requested a FCP, they were prompted to request f-Hb from the same sample. FCP but not f-Hb results were available to clinicians for clinical management. Samples were collected over a 10-month period from November 2018 to September 2019. Patient demographics and final clinical diagnoses are shown in Table 1. One patient aged 19.7 years with IBD not yet transitioned to adult care was included; all other patients were aged less than 18 years.
Demographics and final diagnoses of all patients.
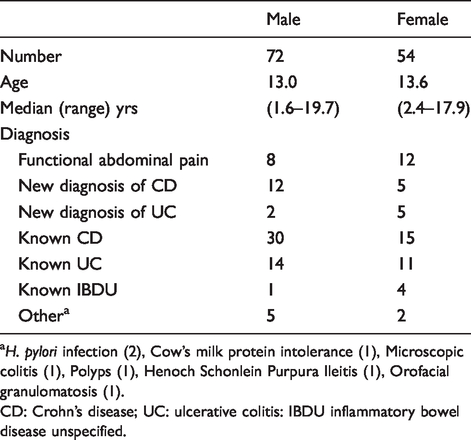
aH. pylori infection (2), Cow’s milk protein intolerance (1), Microscopic colitis (1), Polyps (1), Henoch Schonlein Purpura Ileitis (1), Orofacial granulomatosis (1).
CD: Crohn’s disease; UC: ulcerative colitis: IBDU inflammatory bowel disease unspecified.
Calprotectin and FIT sampling
Samples for FCP were taken into a screw top pot and stored frozen prior to analysis. f-Hb samples were taken into an Eiken specimen collection device using the sampling probe in the lid and returned to the laboratory at the earliest opportunity. The specimen collection devices were stored at 4°C until analysis, which took place within a week of receipt. The laboratory is accredited by the UK Accreditation Service to ISO 15189 standards. FCP was measured using a chemiluminescence immunoassay using Liason®Calprotectin (DiaSorin, Saluggia, Italy). f-Hb was measured by immunoturbidimetry using a single OC Sensor (Eiken Chemical Co Ltd, Tokyo, Japan). The coefficients of variation were <12% for FCP and 2.8% at 14 μg/g and 3.0% at 91 μg/g for f-Hb. External quality assurance was achieved via satisfactory performance in the relevant United Kingdom National External Quality Assessment Service schemes. The lower limits of quantification were 12.5 μg/g and 4 μg/g and the upper limits of the measuring range were 2800 μg/g and 200 μg/g for FCP and f-Hb, respectively.
Colonoscopy
Colonoscopy was carried out where clinically indicated using bowel preparation according to standard hospital protocol. All endoscopies were done by an independent endoscopist and tissue was obtained for histological examination. Clinical outcomes were reviewed from electronic records for all patients in whom f-Hb and FCP samples were collected.
Statistics
Data were analysed using Analyse-It software for Microsoft Excel (Leeds, UK). Spearman’s correlation coefficient was used to assess the correlation between FCP and f-Hb. Statistical significance was determined by a P-value of <0.05.
Ethical considerations
The study was approved as a quality improvement project by the clinical effectiveness unit and consent was obtained from carers and patients as appropriate.
Results
One hundred forty three samples were received from 126 patients of whom 72 patients were male (57.1%).
One hundred forty three samples were received for f-Hb and all were processed, 113 were received for FCP and, of these, six were insufficient for analysis. Sixty-three patients underwent colonoscopy of whom, 38 had provided samples for both f-Hb and FCP (Figure 1).
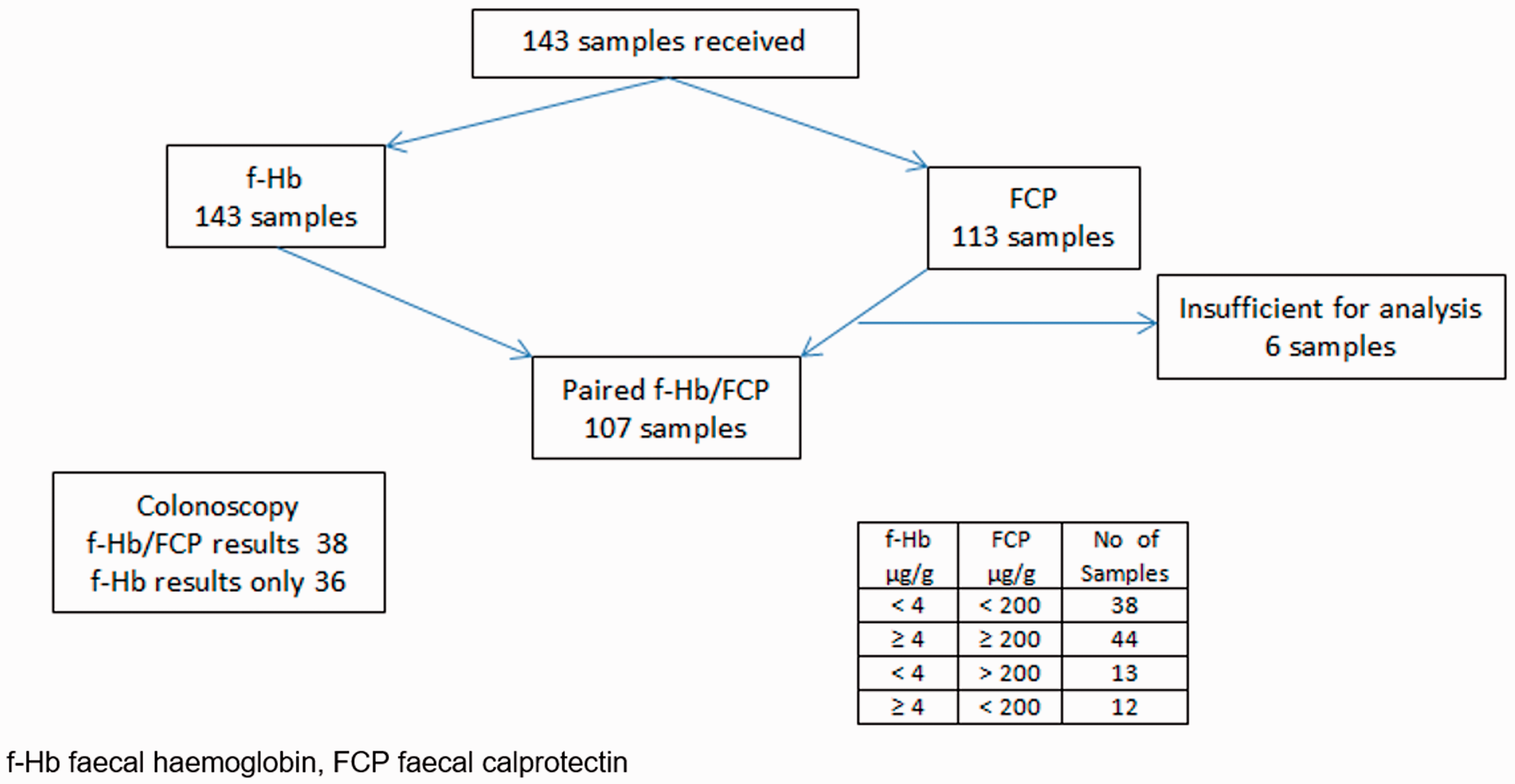
Study flowchart. f-Hb: faecal haemoglobin; FCP: faecal calprotectin.
Fifteen patients provided two samples; the time interval between samples was a median of 3.1 months (range 0.3–9 months). One patient provided three samples, two and eight months after the first.
In the 107 paired samples, f-Hb positively correlated with calprotectin with a Spearman’s rank coefficient 0.656, P < 0.0001. There were 35 samples with f-Hb >20 μg/g and in 32 of them FCP was >200 μg/g (Figure 2).
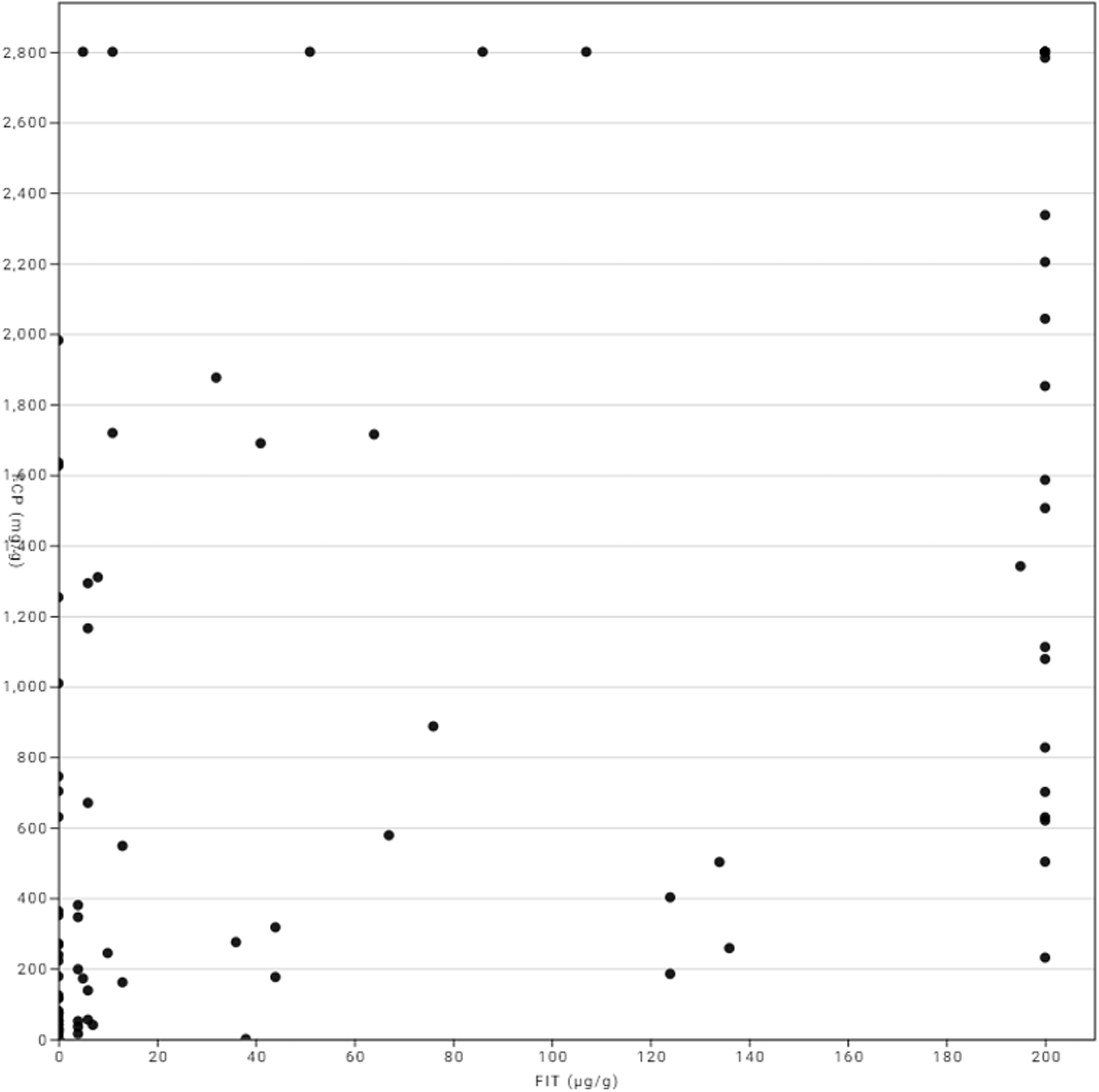
Correlation of faecal haemoglobin and faecal calprotectin.
Twenty patients had a diagnosis of functional abdominal pain. FCP was <200 μg/g in 19. The f-Hb result was <4 μg/g in 16 of the 20 patients. Four patients had f-Hb ≥4 μg/g. Paired FCP was <200 μg/g in three and unavailable in one. However, in two patients, although the FCP from the paired samples was 15 μg/g and <12.5 μg/g, previous measurements on samples sent from Primary Care prior to referral to clinic were 105 μg/g and 176 μg/g, respectively.
One hundred sixteen samples were from 99 patients with IBD, 32 with UC, 62 with Crohn’s disease (CD) and 5 with inflammatory bowel disease unclassified (IBDU). Twenty-four were new diagnoses of IBD (17 CD and 7 UC). Eighty-three f-Hb samples had a paired FCP and the f-Hb result was <4 μg/g and FCP < 200 μg/g in 22 and f-Hb ≥4 μg/g and FCP >200 μg/g in 41.
In 12 patients with IBD, f-Hb was <4 μg/g and FCP was >200 μg/g. No change in management was made in four of these patients and in three a non-intestinal source of inflammation potential contributing to the raised FCP and requiring antibiotic treatment, was identified (peri-anal abscess, infected cheilitis and upper respiratory tract infection). A further patient had a significantly elevated FCP of 1635 μg/g but only minimal intestinal inflammation on histology and was treated for gastrointestinal reflux. Three of the 12 were offered escalation of treatment, 2 with CD and 1 with IBDU. One patient had a new diagnosis of CD with predominantly small bowel lesions.
In eight patients with IBD, f-Hb was ≥ 4 μg/g but FCP was <200 μg/g. Six had no change in management, one with an f-Hb of 44 μg/g and FCP of <12.5 μg/g had escalation of treatment. One patient with UC with an f-Hb of 124 μg/g but calprotectin of < 200 μg/g was found to have Clostridium difficile and was treated with antibiotics.
Thirty-eight patients in whom both f-Hb and FCP were available and an additional 36 in whom only f-Hb was available, underwent colonoscopy. The comparison of f-Hb and FCP with histological findings is shown in Figure 3. All patients with normal histology had an f-Hb <4 μg/g; a result of >20 μg/g was associated with the presence of significant inflammation.
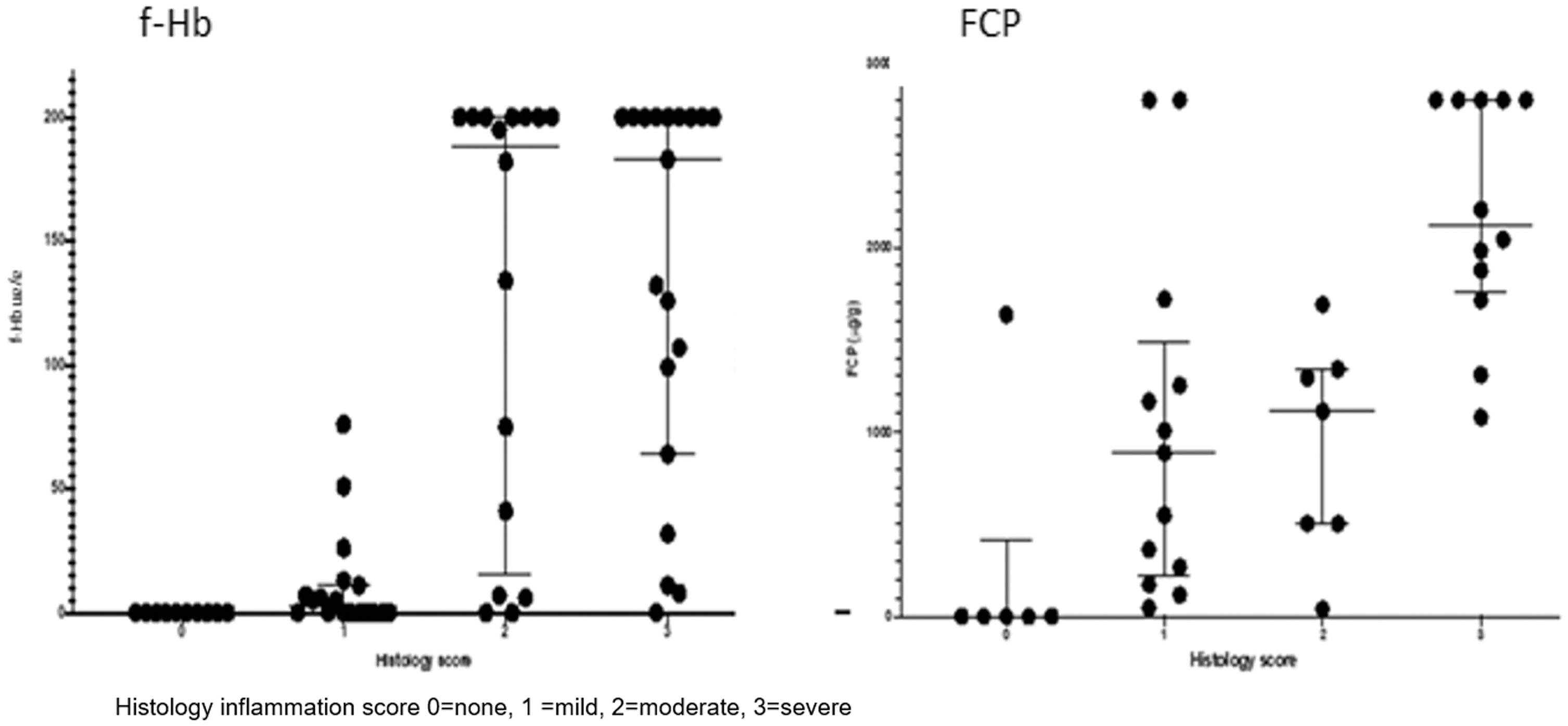
Correlation of faecal haemoglobin and faecal calprotectin with histology findings. Histology inflammation score 0 = none, 1 = mild, 2 = moderate, 3 = severe.
Discussion
When using faecal markers it is essential to establish cut-offs appropriate for the clinical context. Our study showed that an f-Hb of >20 μg/g was associated with the presence of significant inflammation and that all patients with normal histology had f-Hb <4 μg/g.
A meta-analysis evaluating eight studies involving 394 children with IBD and 321 non-IBD patients, calculated the pooled sensitivity and specificity of FCP for the investigation of suspected IBD to be 97.8% and 68.2%, respectively. 7 All the studies included had used a cut-off of 50 μg/g or 100 μg/g. Using similar FCP cut-offs, another meta-analysis revealed pooled sensitivity and specificity in children of 92% and 76%, respectively. 8 It also calculated that if FCP was used for screening for IBD there would be 35% reduction in endoscopy but that diagnosis would be delayed in 8% because of a false negative result. When FCP cut-offs have been compared, it has been shown that increasing the cut-off results in greater specificity, reaching a plateau at 200–300 μg/g. 9 In our unit, based on this and evaluation of in-house laboratory and clinical data, we use a cut-off of 200 μg/g for FCP for a new suspected IBD or possible relapse in a patient with known IBD.
Quantitative measurement of faecal haemoglobin using f-Hb now forms the basis of many national CRC screening programmes for asymptomatic populations and is used for testing those with bowel symptoms. Current NICE guidance recommends a cut-off for faecal haemoglobin of 10 μg/g in symptomatic patients at low risk of CRC to prompt referral on an urgent lower gastrointestinal cancer pathway. 3 Lowering the threshold to any detectable blood increases sensitivity 6 and systematic review has indicated that, at a threshold f-Hb of around 10 μg/g, significant bowel pathologies may be present in 22.5–93% of those in whom CRC is not found. 10 f-Hb has been shown to be superior to FCP when used in addition to clinical information as a screen to stratify patients with bowel symptoms and reduce endoscopy referrals to secondary care.5,11
Various studies have looked at the performance of f-Hb in IBD. A meta-analysis of six studies involving 639 patients, calculated pooled sensitivity and specificity of FIT for predicting mucosal healing in UC of 77% (95%CI 72–81%) and 81% (95% CI 76–85%), respectively, using a f-Hb cut-off equivalent to 20 μg/g. 5 The median ages of the patients in these studies ranged from 30 to 50 years, but three studies12–14 included some children and teenagers. One of these three studies compared FIT and calprotectin with endoscopic activity in 92 patients with UC (age range 16 to 80 years) using cut-offs for FCP of >250 μg/g and f-Hb equivalent to >20 μg/g. 13 It showed that FCP and f-Hb agreed well with a correlation coefficient of 0.64 and that f-Hb was more sensitive than calprotectin for predicting mucosal healing in patients with UC. In adults with CD, f-Hb has been shown to have equivalent sensitivity to FCP for mucosal healing, although is less sensitive in disease affecting only the small bowel.15,16 This may be because of the lower likelihood of significant blood loss from lesions of this site compared with those in the colon but could also reflect a degree of degradation during transit. Like FCP, f-Hb has been shown to increase in inflammatory bowel disease prior to relapse. 17
The two biomarkers have different aetiologies. Calprotectin reflects inflammation in the gut based on the degree of inflammatory infiltration of the gut mucosa, whereas f-Hb measures blood loss from intestinal mucosa. Either mechanism may be appropriate in the context of ruling out significant disease, for example in a primary care setting, and the use of a single test in both adults and children as an initial screen has potential advantages. However, the difference in mechanism may be relevant in determining the most appropriate marker for use in different contexts in established IBD, for example FCP may have better predictive accuracy for endoscopic activity, whereas f-Hb is more sensitive for mucosal healing. 18 Difference in mechanism and timescale to resolution may explain why two of our patients with functional abdominal pain, who had previously had a marginally raised FCP, had elevation of f-Hb.
Whilst FCP has become firmly established in gastrointestinal practice, there are various practical issues relating to its use. There are a number of commercial assays available for calprotectin and quantitative agreement between them is suboptimal with results up to three-fold higher being recorded according to the method used. 19 However, assays for measurement of f-Hb are also subject to heterogeneity and individualization of diagnostic thresholds may be appropriate. 20 Samples for FCP are usually sent in screw top pots and whilst it has been shown to be stable for three days at room temperature a mean decrease of 28% has been demonstrated at seven days. 21 In contrast, once collected into a specimen collection device, f-Hb is stable for at least 14 days at room temperature. 22 Some hospital laboratories do not have the facility to measure FCP ‘in house’ which adds to the cost and increases the time taken to receive results. Since the NICE DG30 recommendations, 3 many laboratories have added f-Hb to their repertoire. f-Hb tends to be considerably cheaper than FCP and because of its use in two-week wait referral pathways for adult patients who may have cancer, results may well be returned more quickly than FCP in some laboratories. The use of f-Hb has improved compliance in bowel cancer screening programmes in adults. 23 More of our patients returned the f-Hb specimen collection devices than the screw top pots required for FCP analysis, suggesting that in the paediatric population as well, collection of samples in this way may be more acceptable. It has been shown that there is decreased detection of HbF (but not common haemoglobin variants) using current f-Hb analysers, such that results might be expected to be 50% of the expected concentration. 24 There may be caveats associated with the use of f-Hb in infants but IBD occurs extremely rarely at this age and there are also issues with use of FCP in this age group as the reference range is significantly elevated in neonates and infants; age-related reference ranges for FCP have also been proposed for use in older children. 25
Although our study included only a small cohort of patients, it represented the spectrum of children in paediatric gastroenterology practice. However, we acknowledge that more data are required from both patients and healthy controls.
Conclusion
Our study is the first to compare f-Hb and FCP in a paediatric population. We found that all patients with normal histology had an f-Hb < 4 μg/g and that an f-Hb > 20 μg/g was consistent with the finding of significant inflammation. Our results suggest that f-Hb correlates with FCP and has potential to be used to differentiate between functional bowel disease and gastrointestinal inflammation in children. In patients without red flag features, the absence of f-Hb could support a conservative management strategy. In children, as has been suggested for adults, f-Hb may be a useful diagnostic test in primary care where the main focus is to rule-out pathology and triage referral. In a specialized clinic, it may be useful addition to the test repertoire to assess mucosal inflammation and healing in patients with known IBD, especially UC.
Footnotes
Acknowledgements
We would like to thank Mast for providing reagents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work was approved and registered as a quality improvement project with the clinical effectiveness unit (9534)
Guarantor
RMA.
Contributorship
RMA conceived the study and assisted with sample analysis. KS and SN were involved in protocol development and patient recruitment. All authors were involved in data analysis and writing of the manuscript.