
Abstract
Background
Faecal immunochemical tests for haemoglobin have been recommended to assist in assessment of patients presenting in primary care with lower bowel symptoms. The aim was to assess if, and which, additional variables might enhance this use of faecal immunochemical tests.
Methods
Faecal immunochemical test analysis has been a NHS Tayside investigation since December 2015. During the first year, 993 patients attending colonoscopy were invited to complete a detailed questionnaire on demographic background, symptoms, smoking status, alcohol use, dietary fibre, red and processed meat intake, physical activity, sitting time, dietary supplement use, family history of colorectal cancer, adenoma, inflammatory bowel disease and diabetes. Significant bowel disease was classified as colorectal cancer, advanced adenoma or inflammatory bowel disease.
Results
A total of 470 (47.3%) invitees agreed to complete the questionnaire and 408 (41.1%) did. Unadjusted odds ratios for the presence of significant bowel disease compared with undetectable faecal haemoglobin increased with increasing faecal haemoglobin and for faecal haemoglobin 10–49, 50–199, 200–399 and ⩾400 μg Hb/g faeces were 0.95 (95% CI: 0.16–5.63), 2.47 (0.55–1.03), 6.30 (1.08–36.65) and 18.90 (4.22–84.62), respectively. Rectal bleeding and family history of polyps were the only other variables with statistically significant (P < 0.05) odds ratios greater than 1.00, being 1.88 (1.13–3.17) and 2.93 (1.23–6.95), respectively. Odds ratios adjusted for all other variables showed similar associations, but only faecal haemoglobin and family history of polyps had significant associations.
Conclusions
Faecal haemoglobin is the most important factor to be considered when deciding which patients presenting in primary care with lower bowel symptoms would benefit most from referral for colonoscopy.
Keywords
Introduction
The demand for colonoscopy has increased over recent years throughout the United Kingdom (UK). There are a number of plausible reasons for this, including (i) the positive publicity surrounding the four UK bowel screening programmes emphasising the benefits of detecting early disease, (ii) the information given to participants with negative screening test results that medical care should be sought if lower bowel symptoms are experienced between screening episodes, (iii) efforts encouraging all members of the public to seek care if symptoms arise, including the Be Clear on Cancer, 1 Detect Cancer Early 2 and other local and regional campaigns and (iv) the influence of relevant charities and well-known individuals in the media. However, it is very well documented that diagnosis of significant bowel disease (SBD), which includes colorectal cancer (CRC), advanced adenoma (AA: any >10 mm diam or three or more) and inflammatory bowel disease (IBD), is challenging, since there are often no specific symptoms, and lower bowel symptoms are very common and mostly related to problems other than SBD.3,4
In consequence, it would be of great value if a simple, relatively inexpensive investigation could be used to assist in the triage of patients presenting in primary care with lower bowel symptoms through assessing the risk of SBD and the priority for colonoscopy and, indeed, if this complex, expensive, time consuming and potentially risky investigation would be of any benefit to the individual. Currently, there is increasing evidence that faecal immunochemical tests (FIT) for haemoglobin (Hb) are of significant value in this clinical setting5,6 as well as in screening. 7 Bowel cancer screening using FIT leads to a significant increase in uptake when compared with the previous card-based guaiac faecal occult blood tests,8,9 which also adds to the already high demands for colonoscopy. Recent reviews have detailed the evidence for FIT,10,11 and the considerations, challenges and constraints involved in setting up a service for FIT 12 have been documented recently to facilitate adoption of the recommendations of the National Institute for Health and Care Excellence in Diagnostic Guidance 30 (DG30). 13 This states that quantitative FIT are recommended for adoption in primary care to guide referral for suspected CRC in people without rectal bleeding who have unexplained symptoms but do not meet the criteria for a suspected cancer pathway referral outlined in the NICE guideline on suspected cancer (NG12). 14
It is known that FIT are imperfect as a diagnostic test and some cases of SBD would be missed using faecal haemoglobin concentration (f-Hb) alone.5,6,10,11 In part, this may be because a single cut-off f-Hb of 10 μg Hb/g faeces is recommended 13 in spite of the facts that f-Hb is higher in men than women and rises with age15,16 and deprivation.16,17 Moreover, signs and symptoms, even if they have low positive predictive value, might add value. 14 A number of risk-scoring systems have been developed, 18 and the COLONPREDICT 19 and FAST Score 20 approaches include f-Hb in their algorithms. However, these require additional information to the f-Hb. Thus, the aim of this study was to assess if, and which, additional variables to the f-Hb would enhance the use of FIT in the assessment of patients presenting in primary care with lower bowel symptoms.
Methods
Since December 2015, a quantitative FIT service has been routinely available to NHS Tayside primary care. General practitioners (GP) were encouraged to request a FIT on all patients presenting in primary care in NHS Tayside with lower bowel symptoms, irrespective of age or symptoms. FIT kits were made up of written information detailing the rationale for measuring f-Hb, one specimen collection device (Kyowa-Medex Co., Ltd, Tokyo, Japan) and a pictorial patient instruction sheet. Practice nurses distribute a FIT kit to each patient selected for investigation of lower bowel symptoms. Patients are instructed to collect a single sample of faeces and return the FIT device immediately to the GP’s surgery. The devices are then returned at room temperature via the GP routine sample collection service (a daily courier service) to Blood Sciences, Ninewells Hospital and Medical School, Dundee, and stored at 4°C prior to analysis: f-Hb is measured using a single HM-JACKarc (Kyowa Medex Co., Ltd, Tokyo, Japan), which has an analytical working range of 7 to 400 μg Hb/g faeces. Samples with results above the upper analytical limit are not diluted and re-assayed, but reported as ⩾400 μg Hb/g faeces. Results with f-Hb ⩾10 μg Hb/g faeces are defined as positive, this cut-off f-Hb being exactly as recommended in NICE DG30. 13 The analyser is operated Monday–Friday and results reported electronically to the requesting GP to provide rapid result turnaround. The laboratory is accredited by the United Kingdom Accreditation Service (UKAS) to ISO 15189 standards. Patients referred to endoscopy are investigated within six weeks of referral. The NHS Tayside endoscopy units participate in the accreditation scheme of the Joint Accreditation Group on Gastrointestinal Endoscopy. All findings were recorded on the endoscopy reporting system by the endoscopists. The diagnoses of CRC, AA and IBD were confirmed by a gastrointestinal pathologist: the nature of all biopsied or excised lesions and the stage of all CRC, using both Dukes’ and TMN systems were documented. AA was defined as any adenoma (A) ⩾ 10 mm maximum diameter and/or ⩾ 3 A. The extent, severity and nature of any IBD were also recorded.
For a period of one year, before undergoing further investigation, usually colonoscopy, all patients referred who had an f-Hb result available were sent an invitation letter (from RJCS) with a study Patient Information Sheet enclosed. The letter was sent at least one week before the appointment to allow the patient sufficient time to decide whether or not to participate. Patients indicated their willingness to take part either via telephone, email or a reply slip. Patients who expressed an interest were approached by a member of the research team when attending the endoscopy units and, after giving consent, completed a short questionnaire based on validated question sets from a range of instruments which have been used successfully for data collection on a study of people attending family history clinics. 21 The exclusion criteria were those patients who were deemed unfit and did not go forward for colonoscopy and those unable to give consent to complete the questionnaire. The domains and items were: demographic background, symptoms (categorized as rectal bleeding, change of bowel habit to looser motions, constipation, abdominal pain, weight loss, frequency of bowel movements) smoking status, alcohol intake, dietary fibre, red and processed meat intake, physical activity, sitting time, dietary supplement use (folate, vitamin D, fish oils), drug history (including prescribed aspirin and other anticoagulants) and family history of CRC, adenoma or IBD. In addition, participants were asked whether they have ever been diagnosed with diabetes. Questions on diet were adapted from the University of Cambridge EPIC-Norfolk Food Frequency Questionnaire (FFQ). 22 Data from the FFQ were converted into dietary fibre intake using McCance and Widdowson’s Composition of Food 23 and Food Portion Sizes from the Food Standards Agency. 24 Dietary fibre was classified as a risk factor according to whether or not the patient met the recommendation of the Scottish Government Dietary Goals of 30 g per day of dietary fibre. 25 Higher risk alcohol intake was identified using the Alcohol Use Disorders Identification Test Consumption questionnaire. 26 Physical activity was measured using questions adapted from the short form International Physical Activity Questionnaire. 27 Patients were considered as meeting physical activity guidelines if they undertook ⩾5 days moderate intensity activity for ⩾ 30 min and/or walking for at least 30 min per day or 150 min per week. Height, weight and waist circumference were also measured and body mass index (BMI) calculated.
Data on all specimens received for FIT were retrieved from the laboratory database and manually linked using the community health index unique identifying number with the NHS Tayside electronic patient record and this study questionnaire database.
All potential predictors of risk of SBD, together with interactions between clinically important variables, were initially assessed using univariable logistic regression. Age was converted to a categorical variable, as was f-Hb. Factors identified as statistically significant predictors were included in a multivariate logistic regression and stepwise techniques applied.
Results
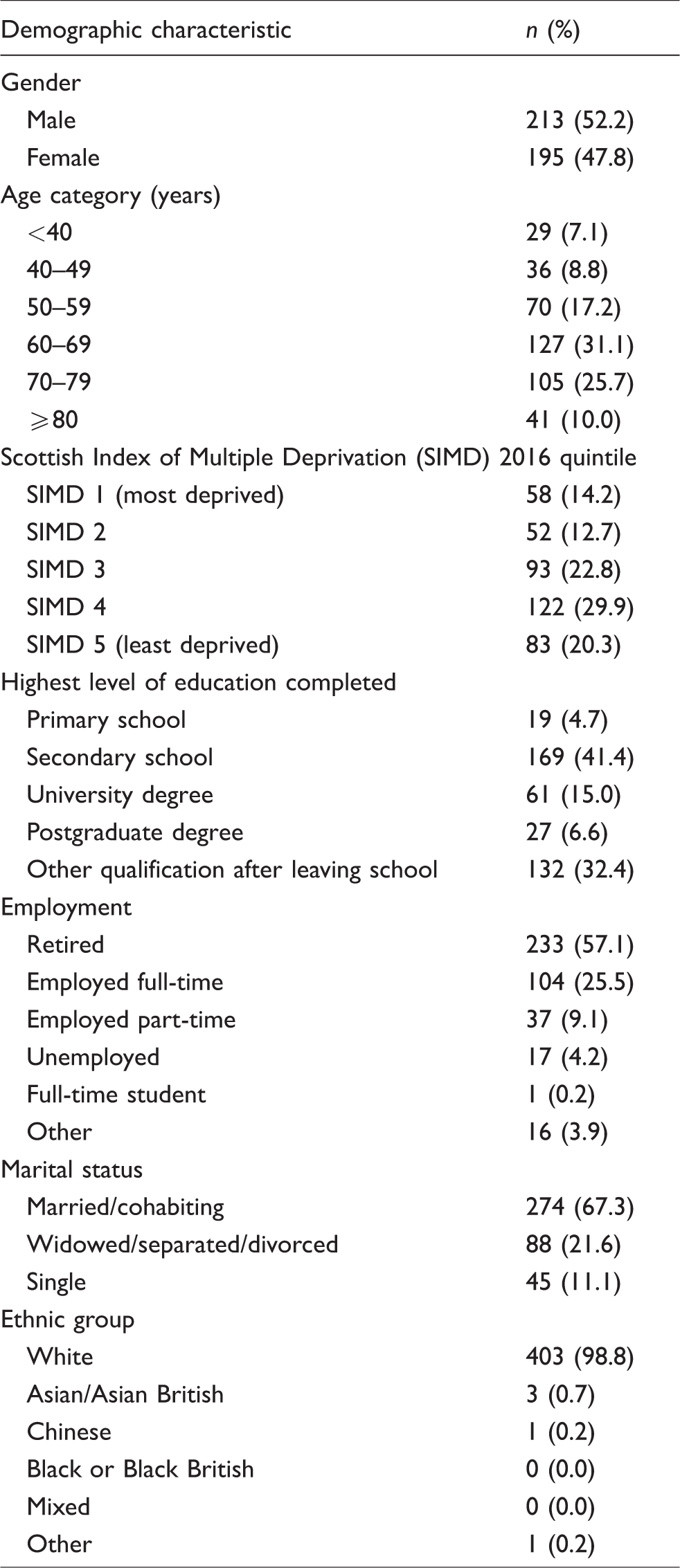
A total of 993 patients who were referred for colonoscopy were invited to complete the study questionnaire: 470 (47.3%) of these agreed to participate, but 62 participants did not complete the questionnaire, with reasons including non-attendance or cancellation of the colonoscopy appointment or time constraints in the endoscopy units. Demographic characteristics of the 408 patients who completed the study questionnaire and gave a wide spectrum of information on variables of interest are shown in Table 1.
Demographic characteristics of 408 patients completing the study questionnaire.
Seventy-two patients had SBD detected at colonoscopy, comprising 18 CRC, 27 AA and 27 new cases of IBD. Table 2 shows the prevalence of risk factors and the results of initial univariate analysis performed to identify which factors showed association with SBD.
Prevalence of potential risk factors and number of patients with significant bowel disease (SBD: colorectal cancer, advanced adenoma or IBD) found at colonoscopy.
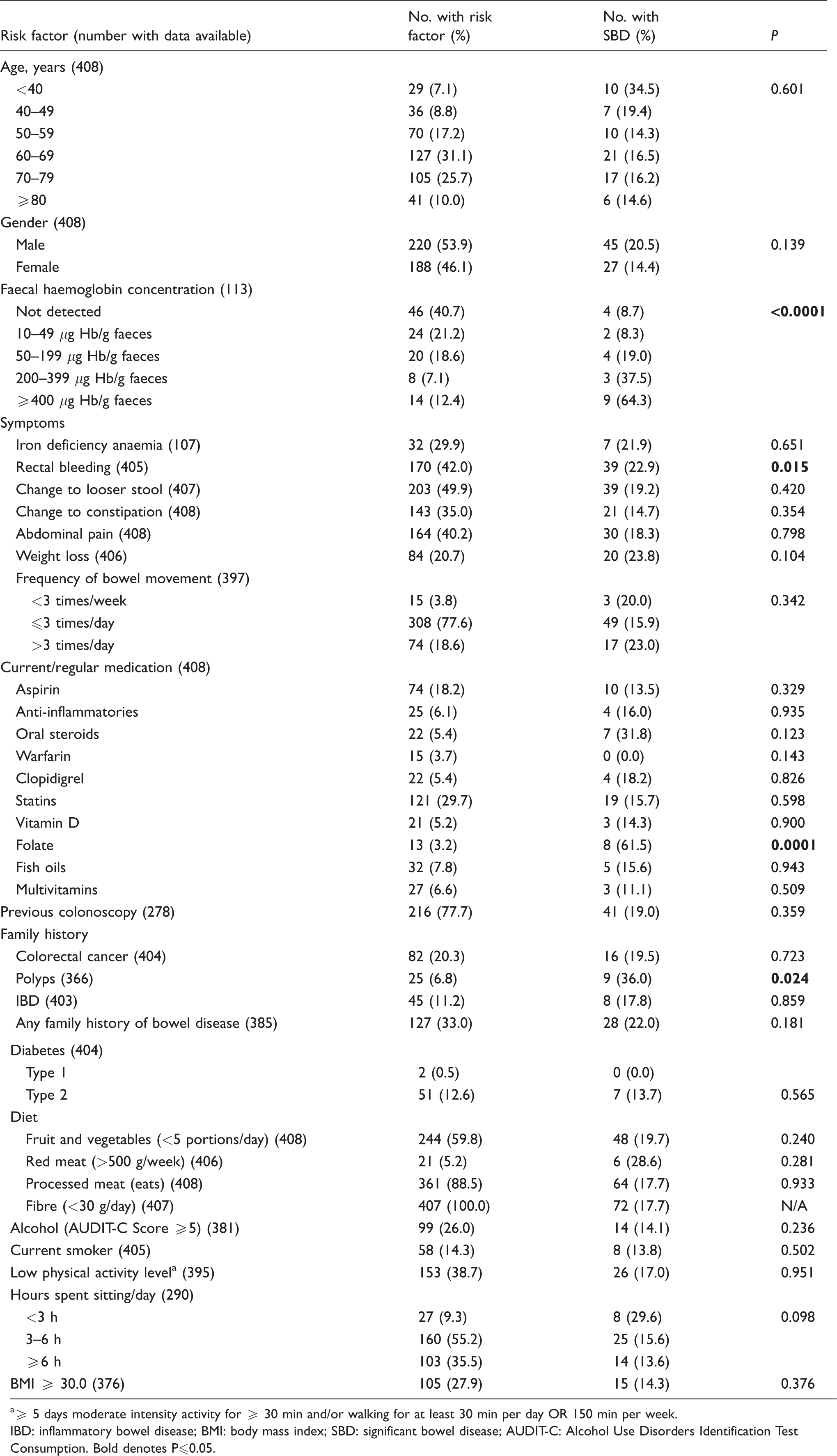
a⩾ 5 days moderate intensity activity for ⩾ 30 min and/or walking for at least 30 min per day OR 150 min per week.
IBD: inflammatory bowel disease; BMI: body mass index; SBD: significant bowel disease; AUDIT-C: Alcohol Use Disorders Identification Test Consumption. Bold denotes P⩽0.05.
Elevated f-Hb, rectal bleeding and family history of polyps had statistically significant (P < 0.05) unadjusted OR > 1.00 and therefore showed association with an increased risk of SBD. Folate also showed a significant association, although the number of patients taking this supplement was small. Unadjusted and adjusted (for all other variables) OR for each of the variables for which OR were >1.00 for either are shown in Table 3. It should be noted that, after adjustment, rectal bleeding was no longer significantly associated with SBD, leaving only elevated f-Hb and family history of polyps.
Unadjusted and adjusted a odds ratios (OR) for significant bowel disease (SBD: colorectal cancer, advanced adenoma and inflammatory bowel disease).
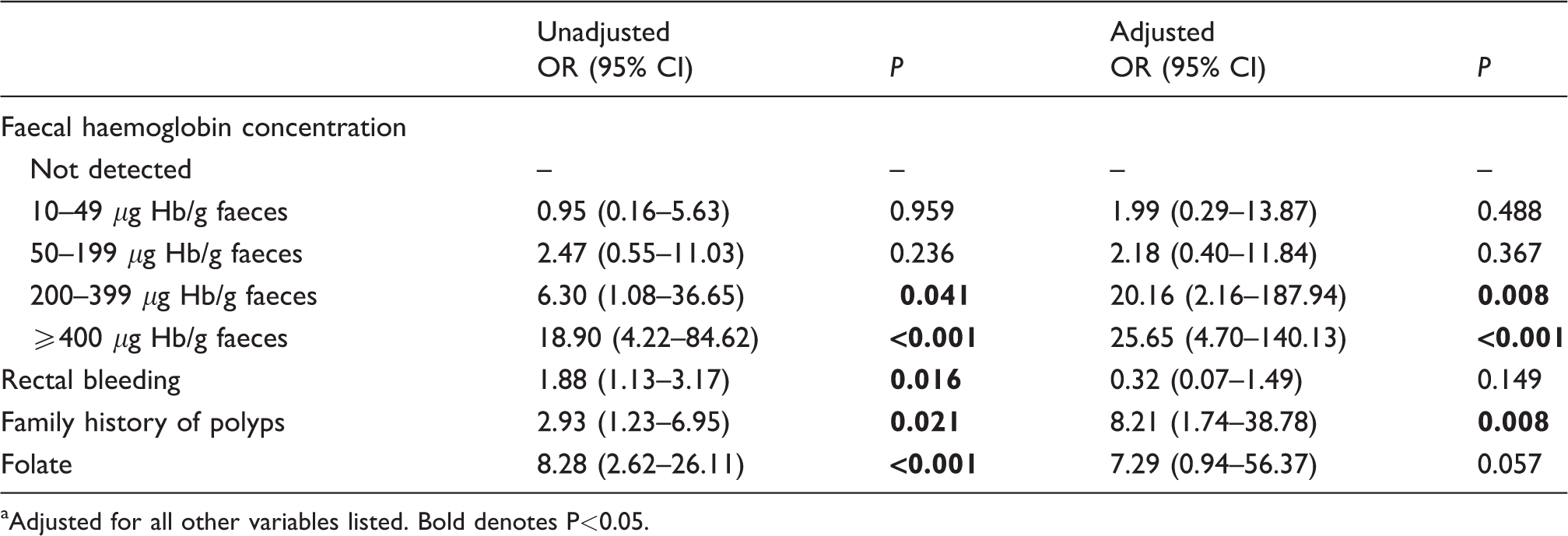
aAdjusted for all other variables listed. Bold denotes P<0.05.
Additional univariate analysis of risk factors was performed when also including low-risk adenomas (LRA, n = 48) along with SBD. As with analysis for SBD only, increasing f-Hb (P < 0.0001) and use of folate (P = 0.004) were significant predictors of SBD plus LRA. However, in contrast to analysis for SBD only, rectal bleeding was not a statistically significant risk factor (P = 0.148), nor was a family history of polyps (P = 0.052).
Discussion
There are still many controversies regarding the use of FIT in assessment of patients presenting in primary care with lower bowel symptoms.10–12 There is no doubt that FIT can assist in the triage of such patients, but it is still unclear what other information might improve the diagnostic accuracy of this simple, inexpensive investigation. In this study, a large number of possibly useful variables have been investigated in a cohort of patients completing a comprehensive questionnaire.
It was thought that age and male gender would be important variables associated with the finding of SBD, since these are very relevant in the known incidence of SBD. Indeed, these factors, along with f-Hb, are the only variables included in the FAST Score, 20 one of the risk scoring systems advocated, but not as yet proven to be of value in routine clinical practice. However, in this study, these variables did not have unadjusted, or adjusted for other variables, OR > 1.00 and of statistical significance (Table 3). Apart from rectal bleeding, which has been demonstrated to have higher positive predictive value than other symptoms associated with lower bowel disease, 14 other symptoms were not significantly associated with the finding of SBD at colonoscopy. It is also important to note that even rectal bleeding did not have a predictive value that was independent of f-Hb. This confirms the findings in an earlier study, in which three published evaluations of the use of FIT in assessment of the symptomatic undertaken in Scotland showed that the diagnostic accuracy of FIT was superior to the symptoms-based approach of the original 2015 NICE NG12 guideline. 28 Moreover, a very recent study from Spain 29 reports similar findings and states that referral of all patients should be guided by f-Hb irrespective of symptoms, rather than just in those not meeting the criteria for a suspected cancer pathway referral outlined in the 2017 NICE guidelines (NG12). 14 Rectal bleeding was not significantly associated with risk when LRA were also assessed along with SBD. This is perhaps to be expected given previous evidence that LRA are less likely to bleed. 30 Another factor that was significant was, unsurprisingly, a family history of the presence of polyps: family history has been incorporated into another rather complex risk-scoring approach requiring incorporation of 11 variables. 19 Other variables, including medication, diet, alcohol intake and activity were not associated with the finding of SBD.
Folate intake was also statistically significantly associated with an increased risk of SBD, although only 13 patients reported regular use. A very recent publication reports on long-term follow-up of 2524 participants in a trial of folate and vitamin-B12 supplementation versus placebo for prevention of osteoporotic fractures, reporting CRC risk to be significantly higher in those taking the supplements. 31 It has previously been suggested in a large randomized controlled trial 32 that folate supplementation shows association with risk of AA, with elevated metabolised plasma folate acting as an inhibitor of natural killer cell cytokine inhibitors. 33 However, a systematic review and meta-analysis of studies on folate status and CRC risk showed no significant effect. 34 Moreover, of the eight cases of SBD in patients taking folate in this study, the majority had IBD rather than advanced neoplasia (one CRC, two AA and five new IBD cases). When the 48 patients with LRA were included with SBD, only one patient with LRA reported taking a folate supplement. Therefore, although the association of folate with risk of SBD in our cohort is intriguing, speculation around this finding is limited by the sample size.
However, the most important factor, with the highest statistical significance and OR is elevated f-Hb, that is, all f-Hb higher than the cut-off of 10 μg Hb/g faeces used in this study. In addition, the higher the f-Hb, the greater the OR. This is explained by the fact that it has been shown by a number of groups that f-Hb is directly related to the severity of lower bowel disease.30,35 In consequence, it may well be that risk-scoring systems do not add significant value and that f-Hb should be considered as the most important criterion for referral from primary care for colonoscopy.
This study has advantages over others in that many variables that could be associated with SBD have been examined by questionnaire administered by a member of the research team in person. One limitation is that this is a relatively small study, which reflects the real difficulties in administering questionnaires to patients awaiting clinical investigations or treatment. Another limitation is that, as shown in Table 1, the group that completed the questionnaire was generally older, less deprived and well-educated, retired, white and married: this cohort may not reflect the characteristics of other patients presenting in primary care in other locations. In addition, the items in the questionnaire relate to current habits only and may, therefore, be subject to reverse causality. A further weakness of the study is that all patients who were included had already been referred for an endoscopy: however, this is a weakness of most studies on FIT in assessment of patients presenting in primary care with symptoms. 36
In conclusion, this study has demonstrated that f-Hb is the most important variable to consider when patients presenting in primary care are considered for referral for colonoscopy due to lower bowel symptoms, although clinical impressions and the results of the full blood count may be of considerable value in this regard.10,11 Further evaluations of published and new risk-scoring strategies involving other variables and more complex approaches to deciding on referral for colonoscopy are clearly required before they can be recommended for routine clinical use.
Footnotes
Acknowledgements
Lynne Taylor, Department of Blood Sciences, Ninewells Hospital and Medical School, Dundee, made up and distributed FIT kits to GP practices. Alpha Laboratories Ltd, Eastleigh, Hants, are thanked for their support for the laboratory analyses.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGF has undertaken paid consultancy with Immunostics Inc., Ocean, NJ, USA, and Kyowa-Medex Co. Ltd, Tokyo, Japan, and has received support for attendance at conferences from Alpha Labs Ltd, Eastleigh, Hants, UK. Other authors have no interests to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Chief Scientist Office (grant number ASM/14/4).
Ethical approval
The study was approved by the North of Scotland Research Ethics Committee (reference number 15/NS/0101).
Guarantor
JD.
Contributorship
JD, RJCS, JAS, CM, AA and CGF conceived and planned the study. JAS supervised, and RMcC undertook, the FIT analyses. JD and LL undertook administration of the questionnaire. JD, RJCS and CGF performed the data analysis. JD, RJCS and CGF prepared drafts of the article. All authors contributed significantly to the writing of the article.