
Abstract
Background
Current guidelines document persistent rectal bleeding as an alarm symptom in patients presenting to primary care. We studied whether a faecal immunochemical test could assist in their assessment.
Methods
From December 2015, faecal immunochemical tests were routinely available to primary care when assessing patients with new-onset bowel symptoms: general practitioners were encouraged to include faecal haemoglobin concentration (f-Hb) within any referral to secondary care. Results with f-Hb ≥10 μg Hb/g faeces were defined as positive. The incidence of significant bowel disease (SBD: colorectal cancer [CRC], higher-risk adenoma [HRA: any ≥1 cm, or three or more] and inflammatory bowel disease [IBD]) at subsequent colonoscopy, referred symptoms and f-Hb were recorded.
Results
Of 1447 patients with a faecal immunochemical test result and colonoscopy outcome, SBD was diagnosed in 296 patients (20.5%; 95 with CRC, 133 with HRA, and 68 with IBD). Four hundred and sixty-two patients (31.9%) reported rectal bleeding: 294 had f-Hb ≥10 μg Hb/g faeces. At colonoscopy, 105/294 had SBD versus 14/168 with rectal bleeding and f-Hb <10 μg Hb/g faeces (P < 0.0001), comprising one case of CRC (0.6%), 12 HRA (7.1%) and one new case of IBD (0.6%); further, the single cancer and 8 of the 12 HRA were located in the descending colon.
Conclusion
Patients with rectal bleeding and f-Hb <10 μg Hb/g faeces are unlikely to have SBD and could be investigated by sigmoidoscopy alone. Using the faecal immunochemical test to guide investigation of patients with rectal bleeding is a rational and practical way forward.
Keywords
Introduction
Rectal bleeding can be a symptom of underlying colorectal disease and convention dictates that, as such, potential cancer must be considered. The National Institute for Health and Care Excellence (NICE) guideline NG12 states: Refer adults using a suspected cancer pathway referral for colorectal cancer (CRC) if aged 50 and over with unexplained rectal bleeding … and consider referral for CRC in adults aged under 50 with rectal bleeding and unexplained … abdominal pain, change in bowel habit, weight loss, or iron‑deficiency anaemia.
1
Measurement of faecal haemoglobin concentration (f-Hb) with a faecal immunochemical test (FIT) has been advocated as a good rule-out test for significant bowel disease (SBD).
3
NICE Diagnostics Guidance (DG30) recommends the use of faecal immunochemical tests for haemoglobin (FIT) at a threshold of <10 μg Hb/g faeces, but only in ‘people without rectal bleeding but with unexplained symptoms that do not meet the criteria for a suspected cancer pathway referral’.
4
However, patients reporting rectal bleeding may not have detectable f-Hb: we reported that rectal bleeding symptoms associated with undetectable f-Hb carry a low risk of SBD. 5 We determined whether using FIT with a cut-off of <10 μg Hb/g faeces could assist in the assessment of patients presenting to primary care with rectal bleeding.
Methods
The methods used have been previously detailed. 5 In summary, from December 2015, quantitative FIT analysis was available to primary care. If patients presented with new-onset lower bowel symptoms, general practitioners (GP) were recommended to request f-Hb. Patients were instructed to collect a single sample of faeces and to return the FIT device immediately to the GP surgery and they were then delivered to Blood Sciences, Ninewells Hospital and Medical School, Dundee. Analysis was performed on one HM-JACKarc analyser (Hitachi Chemical Diagnostics Systems Co., Ltd, Tokyo, Japan). Results with f-Hb ≥10 μg Hb/g faeces were defined as positive. Patients referred to endoscopy were investigated within six weeks of referral. Any diagnosis of significant bowel disease (SBD: colorectal cancer [CRC], higher-risk adenoma [HRA: any ≥ 1 cm, or 3 or more] and inflammatory bowel disease [IBD]) was confirmed by a consultant pathologist. The symptoms reported by GPs on patient referral forms submitted to secondary care were collected to allow a subgroup of those reporting rectal bleeding to be defined. Clinical outcomes of those reporting rectal bleeding were compared between those with f-Hb above and those below the f-Hb cut-off of 10 μg Hb/g faeces. Chi-square tests were performed using MedCalc statistical software (MedCalc Software, Mariakerke, Belgium).
Results
Of 1447 patients with an f-Hb and colonoscopy outcome seen in the first year of the service, SBD was diagnosed in 296 patients (20.5%; 95 with CRC, 133 with HRA and 68 with IBD). Six hundred and sixty-seven (46.1%) of the 1447 had f-Hb <10 μg Hb/g faeces.
Four hundred and sixty-two of investigated patients (31.9%) reported rectal bleeding as a symptom, of whom 293 had f-Hb ≥10 μg/g faeces. At colonoscopy, 105/293 (35.7%) patients with rectal bleeding and f-Hb ≥10 μg/g faeces had SBD versus 14/168 (8.3%) with rectal bleeding and f-Hb <10 μg Hb/g faeces (P < 0.0001) (Table 1). In the patients with rectal bleeding and f-Hb ≥10 μg/g faeces, there were 25 cases of CRC (8.5%), 39 HRA (13.3%) and 25 cases of IBD (14.0%). In contrast, of the 168 patients with rectal bleeding and an f-Hb <10 μg Hb/g faeces, there was one case of CRC (0.6%), 12 HRA (7.1%) and one new case of IBD (0.6%); further, the single cancer and 8 of the 12 HRA were found in the descending colon.
Prevalence of significant bowel disease (SBD), encompassing colorectal cancer (CRC), higher-risk adenoma (HRA) and inflammatory bowel disease (IBD) in patients with rectal bleeding stratified by faecal haemoglobin concentration (f-Hb).
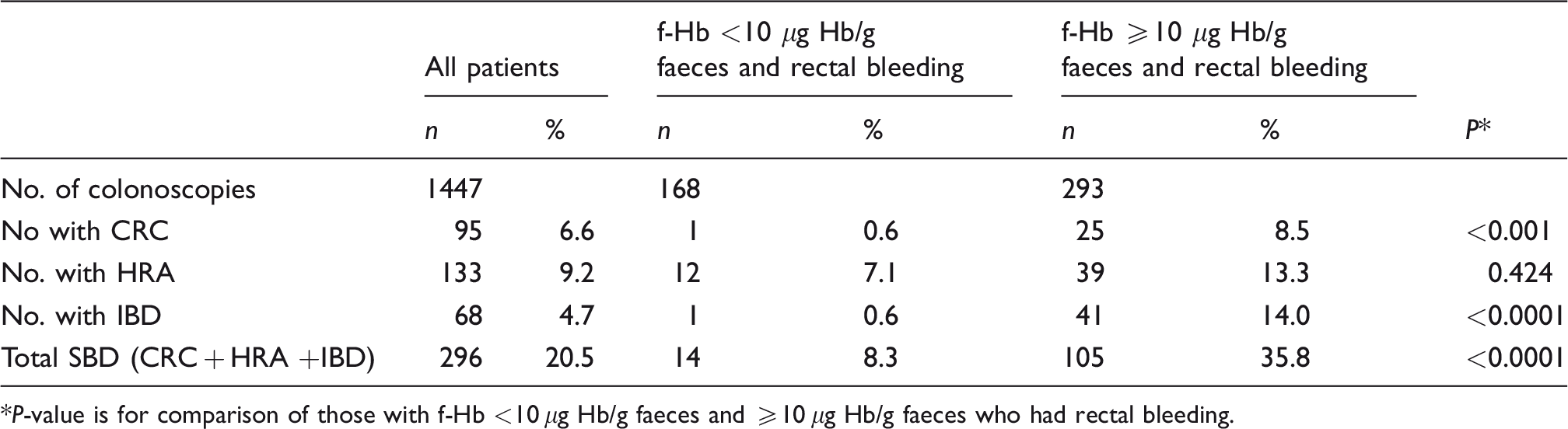
*P-value is for comparison of those with f-Hb <10 μg Hb/g faeces and ≥10 μg Hb/g faeces who had rectal bleeding.
Rectal bleeding with f-Hb <10 μg Hb/g faeces is associated with a very low yield of SBD. Further, in this cohort, the clear majority of the SBD could have been detected by sigmoidoscopy alone, missing only four HRA.
If patients with rectal bleeding and f-Hb <10 μg Hb/g faeces had been triaged to sigmoidoscopy rather than full colonoscopy, this would have saved endoscopy resource without detriment to the patient; if a colonoscopy equates to two points of endoscopy time, and a sigmoidoscopy one point of endoscopy time, then 168 units would have been saved over the year. Even more could be saved by watching and waiting those patients with irregular symptoms.
Discussion
FIT have been recommended for the assessment of patients presenting in primary care with lower bowel symptoms3,4: f-Hb is the most important factor to be considered when deciding which patients would benefit most from referral 6 and a low f-Hb can be used in primary care as a rule-out test to exclude SBD.3–5 However, rectal bleeding, with or without other lower bowel symptoms, is generally considered as a ‘red flag’ symptom,1,2 requiring urgent referral, irrespective of the f-Hb. Here, we have shown that patients reported to have rectal bleeding are unlikely to have SBD if f-Hb <10 μg Hb/g faeces. In contrast, more than one-third of such patients with f-Hb >10 μg Hb/g faeces had SBD.
Patients presenting with rectal bleeding harbour real fears and need an explanation. They require an objective assessment; a full history, clinical examination and a full blood count are essential. We have shown that FIT could provide further objective evidence of the risk of underlying SBD. Furthermore, we have demonstrated that, in the presence of an f-Hb <10 μg Hb/g faeces, patients with persistent rectal bleeding can be safely investigated by sigmoidoscopy alone, thereby enabling more efficient use of endoscopy resources. Safety-netting measures should also be in place for these patients if they continue to experience rectal bleeding and/or other symptoms due to the small chance that SBD may not be detected at sigmoidoscopy. Our results indicate that using FIT to guide investigation of patients with rectal bleeding is a rational and practical way forward and that current referral guidelines require further attention.
Footnotes
Acknowledgements
Lynne Taylor, Department of Blood Sciences, Ninewells Hospital and Medical School, Dundee, made up and distributed FIT kits to GP practices. Alpha Laboratories Ltd, Eastleigh, Hants, are thanked for their support for the laboratory analyses.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGF has undertaken paid consultancy with Immunostics Inc., Ocean, NJ, USA, and Hitachi Chemical Diagnostics Systems, Co., Ltd, Tokyo, Japan, and has received support for attendance at conferences from Alpha Labs Ltd, Eastleigh, Hants, UK. Other authors have no interests to declare.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the Chief Scientist Office (grant number ASM/14/4).
Ethical approval
The study was approved by the North of Scotland Research Ethics Committee (Reference number 15/NS/0101).
Guarantor
JD.
Contributorship
JD, JAS, CM, RJCS and CGF conceived and planned the study. JAS supervised, and RMcC undertook the FIT analyses. JD and CGF performed the data analysis. CM, CGF and JD prepared drafts of the article. All authors contributed significantly to interpretation of the data and to the writing of the article.