
Abstract
Background
Natriuretic peptides have broad indications during heart failure and the detection of left ventricular dysfunction in high-risk patients. They can also be used for the diagnosis/management of other cardiac diseases. However, very little is known regarding their use in routine practice.
Methods
We examined all biological tests performed from February 2010 to August 2015 in two districts from the French Brittany, covering 13,653 km2 and including 22,265 physicians. We report the settings and conditions of N-terminal pro-B-type natriuretic peptide (NT-proBNP) measurements (the only locally natriuretic peptide available).
Results
From a total of 3,606,432 tests requested in 557,650 adult (older than 20 years) patients, only 56,653 (1.6%) included at least one NT-proBNP measurement. NT-proBNP measurements gradually increased, from 9188 in 2011 to 12,938 in 2014 (P < 0.001). Most NT-proBNP tests were measured in urban laboratories (72.7%) and in private (62.9%) non-hospital/clinics laboratories; they were mostly ordered by general practitioners (66% compared with 11% by cardiologists). The number of NT-proBNP measurements increased with age up to 80–90 years, and 70.3% of tests were measured in ≥75 years patients. Creatinine and electrolytes were not associated with NT-proBNP in 15.8% and 19.7% of tests, respectively.
Conclusion
Among a very large cohort, we observed that natriuretic peptides remain largely undermeasured. NT-proBNP is mostly measured in elderly patients, and its interpretation may be hazardous in up to 16% of all individuals because no measurement of creatinine was associated to NT-proBNP.
Introduction
Heart failure (HF) is a common and severe condition, in which biomarkers may be of great value. During the last two decades, several biomarkers have been demonstrated to present strong prognostic and/or diagnostic significance in patients with suspected/proven HF.1–5 B-type natriuretic peptide (BNP) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) have been the most extensively studied HF biomarkers and are currently used.2–5 The recent European and American guidelines recommend the use of BNP/NT-proBNP for the diagnosis and prognostic assessment of HF with a class 1 A level.6,7 Other potential indications for BNP/NT-proBNP evaluation include the follow-up and guided therapy of HF patients, the detection of left ventricular dysfunction in high-risk patients and the diagnosis/management of other cardiac diseases.8–12
In contrast with the large body of scientific validation for the performance of BNP/NT-proBNP in cardiovascular events, little is known regarding the use of these biomarkers in routine practice. In 2015, a Spanish study showed that BNP/NT-proBNP was available in only 65% of emergency departments. 13 The European Federation of clinical Laboratory Medicine has started an audit on cardiac biomarkers use and implementation in laboratories since 2006. 14 They showed an increase in natriuretic peptide implementation and use from 67% to 77% between 2013 and 2019.15,16
The recent application of big data analysis in medicine has opened new frontiers, such as the development of predictive models and personalized medicine, the surveillance of drug and device safety, the use of clinical decision support systems and population-level health analyses.17,18 Another unexplored potential application of biomarker big data analysis is the evaluation of medical procedures.
The defining
Methods
The rUBIDIuM study is a retrospective analysis of all tests (DNA and serology excluded), performed between the 17 February 2010 and 30 August 2015, across 22 laboratories from French Brittany, which comprises 13,653 km2 and 4527 physicians. The detailed methods have been reported previously. 20
Briefly, we collected demographic characteristics, the lists of biological tests requested, the dates of requests, the physicians who ordered the tests and the tests results, from all patients older than 20 years who visited a participating laboratory during the study period. Data were automatically collected by a ‘middleware’, after a complete de-identification process.
All laboratories were equipped with Roche Instruments, analysed NT-proBNP as the unique natriuretic peptide and used the same threshold values for its interpretation. For suspected HF in a non-acute setting, the threshold value is set at 125 ng/L. 21 For suspected HF in an acute setting, the rule-out threshold value is at 300 ng/L, whereas the rule-in threshold values are at 450 ng/L for patients <50 years, 900 ng/L for patients 50–75 years and 1800 ng/L for patients >75 years. In addition, 69.2% of measurements were performed in non-hospital/clinics laboratories, suggesting that diagnosis/follow-up of non-acute HF was the most frequent clinical situation.
The study protocol was approved by the ethics committee of Avicenne hospital, and the Commission Nationale de l’Informatique et des Libertés, the French agency that regulates the protection of data, reviewed and approved the study. ProbaYes, a data science research organization in Montbonnot (France), and Christophe Meune, MD, PhD, had exclusive access to the data and signed a privacy agreement with Roche Diagnostics, the study sponsor.
The study sponsor played no role in the data analysis or interpretation, the writing of the manuscript, or the publication process.
The endpoints of the present study included the numbers of NT-proBNP tests over time, any associated tests and the characteristics of the patients and physicians who ordered the test.
Statistical analysis
Quantitative data are expressed as the mean ± standard deviation or the median (interquartile range); categorical variables are expressed as counts and percentages. Variations in results over time were examined by comparing the yearly results between 2011 and 2014, to consider full-year periods. To analyse the distribution of tests according to patient age, we considered the age at the first measurement and reported the results stratified by decade.
Numerical variables were compared using Student’s t-test, whereas the chi-square test was used to examine differences in frequency. All statistics were performed based on the a priori hypothesis that, due to the large population studied, the values would be normally distributed. Due to the large sample size, a P-value <0.001 was considered significant.
All data aggregations and analyses were performed by ProbaYes, using Python language and numeric computation libraries.
Results
NT-proBNP measurements
Among the 3,606,432 analyses requested for 557,650 distinct adult patients (older than 20 years), only 56,653 (1.6%) included at least one NT-proBNP measurement, which was ordered for 27,527 distinct patients (4.9% of the study population) by 22,265 distinct physicians.
NT-proBNP measurements gradually increased when patients were stratified by 10-year age categories, up to 80–90 years, and 39,828 (70.3%) of all measurements were ordered in elderly patients (aged 75 years or older), including 31,563 tests (55.7%) in patients ≥80 years and 7605 tests (13.4%) in patients ≥90 years (Figure 1).
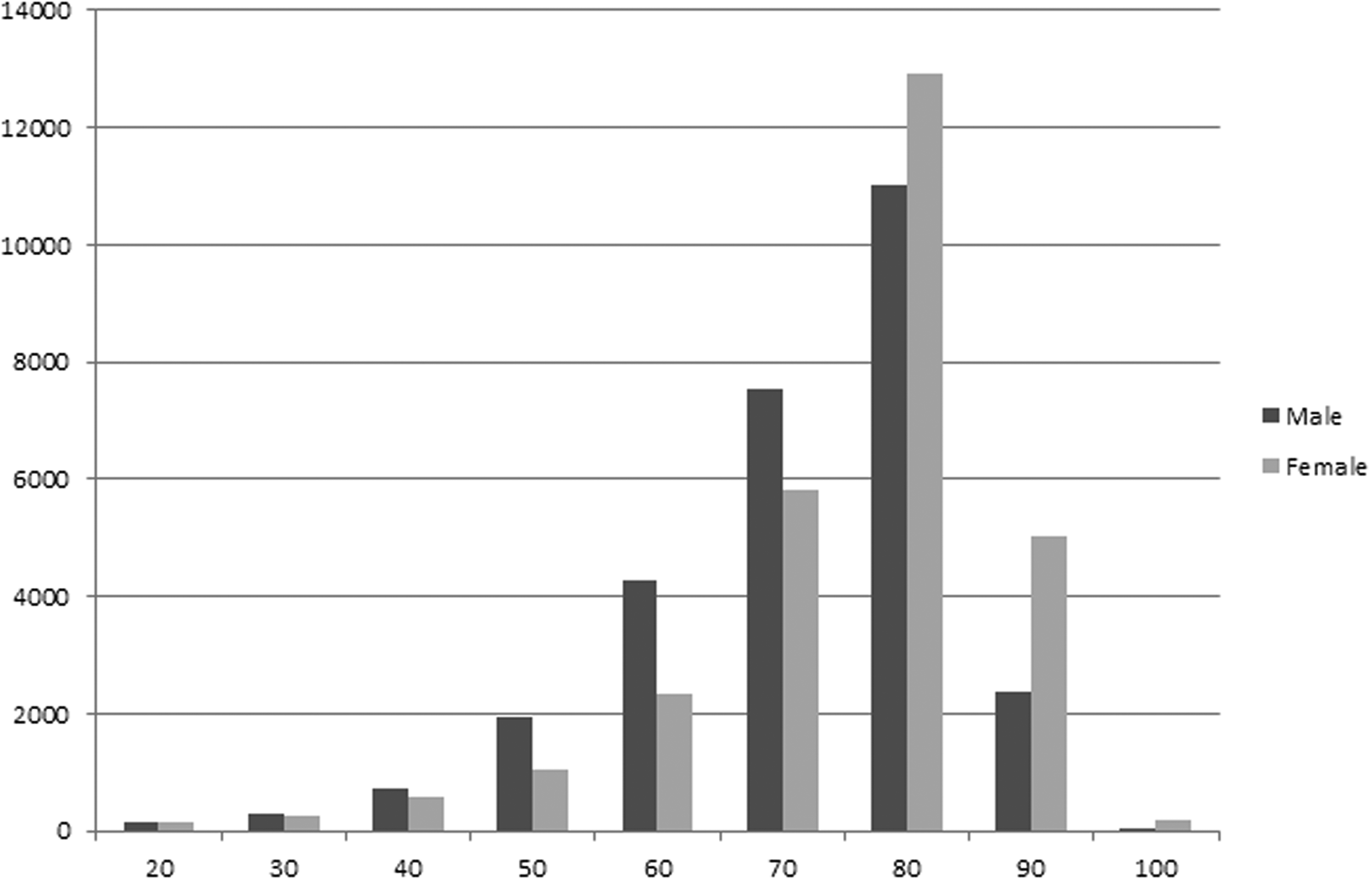
Number of NT-proBNP measurements across the 10-year age categories, among 3,606,432 patients.
NT-proBNP was more often measured in men than in women, until the age of 80 years (P < 10−5), at which point it was more often measured in women than in men, with an overall sex ratio of 1.0.
The number of NT-proBNP measurements gradually increased over time, from 9188 in 2011 to 12,938 in 2014 (P < 0.001), both overall and for all 10-year age categories (Table 1).
NT-proBNP measurements across the 10-year age categories, from 2011 to 2014.*
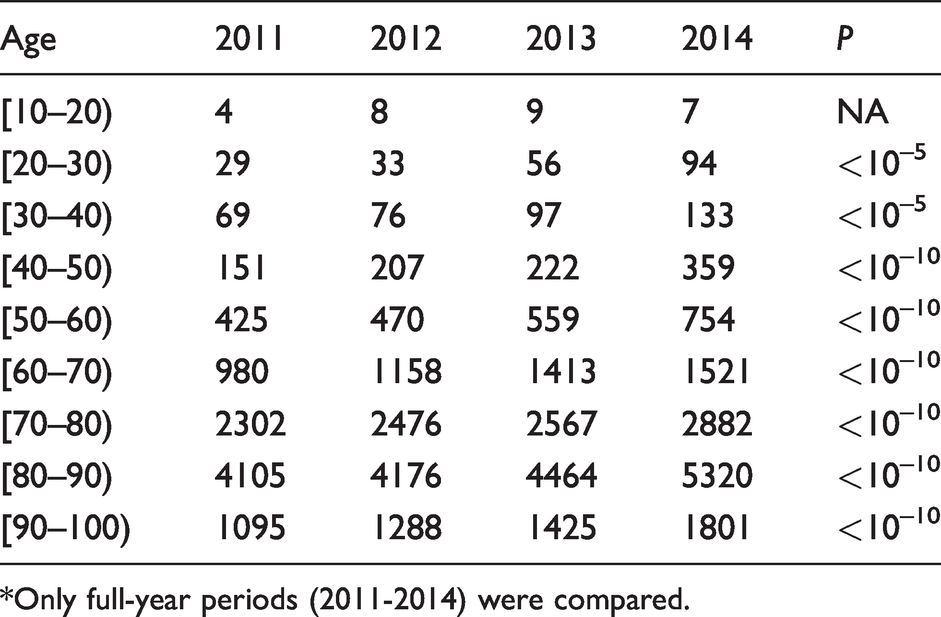
*Only full-year periods (2011-2014) were compared.
During the entire study period, 41,168 (72.7%) measurements were performed in urban laboratories, whereas 15,485 were performed in rural laboratories (27.3%); 15,286 (27.0%) tests were performed in hospital/clinic laboratories, 5,719 (10.1%) were measured in laboratories dedicated to the emergency department (ED) and 35,648 (62.9%) were measured in non-hospital/non-clinics laboratories.
We were able to identify the physicians who ordered 36,492 NT-proBNP measurements (64.4%), whereas they were unknown for the remaining 20,161 tests (35.6%). General practitioners (GP) represented the primary source of requesters (76.0%), followed by cardiologists (12.8%), pneumologists (8.1%), anaesthesiologists (1.6%) and gerontologists (0.9%).
Associated analysis
The following analyses were associated with NT-proBNP orders: creatinine was ordered in 84.2% of total NT-proBNP measurements, electrolytes in 80.3%, haemoglobin A1C (HbA1C) in 70.7%, haemogram in 69.9%, liver enzymes in 30.4% and troponin in 20.6%. NT-proBNP, electrolytes and creatinine were on the same request in 76.2% of all orders.
Most NT-proBNP measured concentrations without associated creatinine orders were increased; 92.2% were >125 ng/L and 75.0% were >300 ng/L.
Patients without associated creatinine measurements versus those with NT-proBNP and associated creatinine were younger (mean [95% confidence interval (CI)] of 75.0 years [64.0 to 83.0] versus 79.5 [69.0 to 86.0], P < 10−5), without gender difference (males 47.3% versus females 48.3%, P = 0.250). The tests have been often ordered by GPs (67.7% versus 65.6%, P = 0.046), measured in rural areas (29.5% versus 26.6%, P = 0.0003) and less often measured in clinics/hospital laboratories (37.3% versus 41.0%, P = 3.3.10−5).
Discussion
Our analysis of a very large cohort showed the following. First, a gradual increase in NT-proBNP measurements was observed over time; however, overall, NT-proBNP remains largely undermeasured. Second most NT-proBNP tests are ordered by GPs and measured in older patients. Third, the interpretation of NT-proBNP may be hazardous in up to 16% of patients because creatinine was not simultaneously measured.
Nearly 20 years have passed since the BNP and ICON studies were published, and an algorithm was proposed to interpret BNP concentrations in the setting of acute dyspnoea.2,3 A position paper, published in 2008, addressed 10 key messages for clinicians, including recommendations regarding measurements for the diagnosis and risk stratification of HF, for the guided-therapy of chronic HF and the screening for left ventricular dysfunction in high-risk patients. 4 In 2012, the European Society of Cardiology (ESC) introduced the use of NPs as diagnostic and prognostic tools in patients with suspected acute/chronic HF, with a grade IIa level of evidence. 21 The same year, a position statement from the ESC study group on biomarkers, added the continuity of care in HF patients, pulmonary embolism, acute coronary syndrome and intensive care medicine to the list of NPs’ indications. 22 HF is a pandemic disease, with an approximate prevalence of 2.4%.23,24 A large survey performed in France, from 2008 to 2009, reported a similar prevalence. 25 The prevalence and the time course of HF progression and the prevalence of all cardiovascular diseases (HF, coronary artery disease and pulmonary embolism) suggested that NP should have emerged as one of the most frequently ordered tests.24,26 In contrast, in our very large cohort of 3,606,432 analysis orders for 557,650 distinct adults, NP tests represented only 1.6% of all analyses.
Several hypotheses can be generated to explain the low penetrance of NPs testing in routine care. A lack of NPs measurement availability has been hypothesized. Thus, a survey by the Spanish Society of Cardiology, in 2015, reported that NPs testing was available in only 65% of laboratories, whereas surveys performed in 2013 and 2014 among 531 laboratories in Europe and North America reported that 67% and 58% of the laboratories offered NPs measurements, respectively. 13 The CARdiac Marker Guideline Uptake in Europe (CAMARGUE) study started in 2006 by the European Federation of clinical Laboratory Medicine (EFLM) has focused on the implementation and use of NPs in clinical laboratories. They showed a continuous increase of NPs implementation in laboratories from 68%, 67% to 77%, respectively, in their 2009, 2013, 2019 surveys.14–16 In our study, all laboratories belonged to the Biorance group, were equipped with Roche instruments and were able to measure NT-proBNP during the study period. This was consistent with a previous French survey performed in 2010, which reported a 92 and 99% availability of NP measurements, respectively, in hospitals and private laboratories. 27 Another hypothesis could be that the cost of the test may represent another limitation to its acceptance and broad use. However, the majority, if not all, of potential indications for NPs measurements (including acute and chronic HF, coronary disease, pulmonary disease, high-risk population such as diabetes) are fully covered and costs reimbursed by the French National health insurance. We, therefore, assume that a lack of knowledge regarding NPs measurements during the study period, especially among GPs, and/or the feeling that the interpretation of NPs measurements is complex may be plausible explanations. Similarly, the increase in NT-proBNP measurements observed from 2010 to 2015 may be attributed to a broader knowledge concerning NPs measurements among physicians, rather than the improved availability of measurements or any marked increase in the prevalence of HF or other cardiovascular diseases.
We report here that NT-proBNP was ordered by GPs in 76.0% of cases, followed by cardiologists in 12.8% of cases. This is consistent with a previous French study, which reported that emergency physicians were the most frequent requesters in hospital laboratories, whereas GPs were the most frequent requesters in private laboratories. 27 Relative to the number of physicians working in the studied region (61.08% of GPs and 2.49% cardiologists, among those who could be identified), cardiologists recommend NT-proBNP measurements more frequently than GPs.
In our study, we observe a gradual increase in NT-proBNP measurements with age: 70.3% of all measurements were performed in patients aged 75 years or older. This finding is consistent with the increased prevalence of HF with age, averaging 10% in older patients.21,28 This finding is also consistent with the fact that older patients are more complex to manage and have more comorbidities, resulting in increased uncertainty among physicians.29,30 A recent study reported the lack of accuracy of BNP measurement in patients older than 80 years with dyspnoea. 31 However, the authors examined the addition of BNP to a multiscore assessment, which was at least already good. In addition, they measured BNP, not NT-proBNP, and did not use age-adjusted threshold values; this may have resulted in lowered the performance of the test.3,32 As NT-proBNP was the only NP measured in our study, we cannot comment on BNP measurements in older patients.
Understanding the caveats of using NPs is pivotal to avoiding false interpretation. Some non-cardiac conditions can cause NPs elevation, which weakens their positive predictive value. In contrast, other conditions may lower NPs concentrations, affecting their negative predictive value. Renal function and body mass index have been known for more than a decade to affect NPs concentrations. Obesity reduces NPs synthesis, whereas NPs are cleared by the kidneys and thus increase in concentrations when renal failure occurs.4,22 Most of NT-proBNP were measured in non-hospital/clinics laboratories, meaning that the main indication should be suspected or follow-up of HF in a non-acute setting. If considering a threshold value of 125 ng/L (as recommended for suspected CHF), 92.2% of NT-proBNP measurements not associated with creatinine measurements were >125 ng/L. We assume that without creatinine measurements, NT-proBNP results are impossible to interpret, particularly among older patients who experience frequent renal dysfunction. 33 In our study, we observed that the omission of creatinine testing occurred significantly more frequently when the NT-proBNP was measured in rural areas and private laboratories. Isolated NT-proBNP also tended to be ordered more frequently by GPs (P = 0.046, which was a non-significant difference according to the adjusted level of significance we adopted). Ten years ago, the French government enacted a law stating that biologists are responsible for interpreting tests and can change the test orders if needed. Therefore, an effort should be made to disseminate timely and accurate information regarding recent recommendations to all physicians, including biologists. The systematic implementation (using laboratory’s software) of creatinine with each NP measurement may be recommended.
Laboratories generate a very large amount of data and are particularly suitable for big data analyses. To ensure the generalizability of our results, we collected data over a large study period, in a large area, resulting in 3,606,432 analysis orders for 557,650 distinct adults. We also focused our attention on French Brittany, as this region shares several characteristics, such as age distribution, the density of physicians and mortality rates, with the general French population, represents both urban and rural populations and is less susceptible to migratory variations than most other French regions. 20 In addition, there is a north–south gradient in medical condition in France, with the French Brittany representing the average for the incidence of cardiovascular disease as well as for the number of tests performed by each laboratory. 27
Limitations
Some limitations deserve consideration. First, we were unable to identify the specialties of all physicians. Second, we assumed that NPs are largely undermeasured, given the prevalence of HF but also some other cardiovascular diseases in which NPs should be measured; however, we cannot comment on the exact number of HF patients in the study region. Based on our findings that the majority of NT-proBNP were measured in non-hospital/clinics laboratories, and on the study period, we assume that suspected/follow-up of HF was the main indication of NT-proBNP measurement. However, our study does not allow to determine the exact indication for NT-proBNP measurement as well as the changes in patients’ management induced by the findings of elevated NT-proBNP concentrations.
Conclusion
Among a very large cohort, we observed a gradual increase in NT-proBNP measurements between 2011 and 2014 especially in elderly, but NT-proBNP remains largely undermeasured. Because of no creatinine co-request in up to 16% of all individuals, NT-proBNP interpretations may be hazardous.
Footnotes
Acknowledgements
We thank Nicolas Garnier and Abel Betraoui from Probayes for their assistance with data analysis. We thank Nicolas Dubois from Biorance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data analysis by ProbaYes and the logistical support for the study were funded by Roche Diagnostics, which did not contribute to the study design or analysis, the decision to publish results, or manuscript preparation. The investigators were not personally remunerated.
Ethical approval
The ethics committee (Comite Local d’Ethique pour la recherche clinique Avicenne-jean verdier-rené muret) approved this study (rec number: CLEA-2017–041).
Guarantor
CM.
Contributorship
FXG and CM: researched literature and wrote the first draft. FXG, SM, TB: data analysis. ProbaYes: statistical analysis. POS: revised the article. CM conceived the study, gained ethical approval, data analysis and revised the article. All authors reviewed and edited the article and approved the final version of the article.