
Abstract
Background
The role of chronic inflammation in the pathogenesis of atherosclerosis has been unequivocally proven. However, the prognostic impact of C-reactive protein, a marker of inflammatory response in patients with acute myocardial infarction has not been fully clarified. Furthermore, there is no direct comparison of the diagnostic accuracy of C-reactive protein and high sensitivity C-reactive protein in the acute myocardial infarction population.
Methods
In this prospective observational cohort study, 344 patients with acute myocardial infarction were enrolled. All-cause mortality was a primary endpoint. Patients were followed prospectively for a median of six years.
Results
The correlation between high sensitivity C-reactive protein and C-reactive protein (r = 0.99; P < 0.001) and the diagnostic accuracy (98.6%) was high. The ROC analysis revealed that C-reactive protein and high sensitivity C-reactive protein had a low AUC for prediction of mortality (C-reactive protein: 0.565, 95% CI [0.462–0.669], vs. high sensitivity C-reactive protein: 0.572, 95% CI [0.470–0.675]) or major adverse cardiac events (C-reactive protein: AUC 0.607, 95% CI [0.405–0.660], vs. high sensitivity C-reactive protein: AUC 0.526, 95% CI [0.398–0.653]) when assessed at time point of acute myocardial infarction. In contrast, longitudinal inflammatory risk assessment with serial C-reactive protein measurements in the stable phase of the disease revealed a 100% specificity, 100% negative predictive value, 32% sensitivity and 12% positive predictive value of C-reactive protein to predict long-term mortality. The Kaplan Meier analysis showed a significant survival benefit for patients at low residual inflammatory risk (P = 0.014).
Conclusion
C-reactive protein and high sensitivity C-reactive protein provide a similar diagnostic accuracy, highlighting that C-reactive protein might replace high sensitivity C-reactive protein in routine assessments. Furthermore, low inflammatory status during the stable phase after acute myocardial infarction predicts favourable six-year survival.
Introduction
The clinical prognosis of patients presenting with acute myocardial infarction (AMI) has improved over time due to several factors as the introduction of potent platelet inhibitors,1–5 improvement in dosing and combinations of drugs 6 and in stent technologies. 7 Nevertheless, AMI patients still experience adverse events, which might be related to the residual inflammation, for which C-reactive protein (CRP) is an established biomarker. It is well documented that inflammatory processes contribute to atherogenesis, plaque dysfunction and thrombosis.8,9 However, the mechanisms leading to this association are poorly understood, but it seems intuitive that a chronic systemic inflammatory state triggers cardiovascular (CV) events most likely due to endothelial dysfunction and the close cellular link between inflammation and thrombosis. 10
It seems of utmost importance to identify patients presenting with AMI with a chronic inflammatory burden and at risk for the development of major adverse cardiac events (MACE), but there is still a lack of appropriate tools available for sufficient risk stratification in this patient population.8,11 Some studies assessing CRP concentrations in patients presenting with AMI and who undergo percutaneous coronary intervention (PCI) propose CRP as a robust candidate for the identification of people at high risk of developing adverse events.12,13 However, it is unclear to what extend CRP can be used for risk stratification in patients during AMI and PCI. Furthermore, it is controversially discussed whether high-sensitivity C-reactive protein (hsCRP) is more sufficient in risk stratification in this vulnerable patient population compared with CRP and whether hsCRP can be substituted for CRP in clinical use. The advantages of CRP over hsCRP seem clear, such as: universal availability in any laboratory and cost efficiency. Therefore, the question arises of the added value of measuring hsCRP. However, until now, data on validating hsCRP are scarce. Therefore, we aimed to (i) compare the diagnostic accuracy of hsCRP vs. CRP; (ii) investigate the prognostic value of hsCRP vs. CRP for prediction of all-cause death and MACE when assessed at the time point of AMI and (iii) assess the prognostic impact of increased serial CRP concentrations on patients’ outcome.
Methods
Study design and setting
Within this prospective observational cohort study, a total of 344 patients with AMI were consecutively enrolled. Fifty-four individuals had missing CRP and hsCRP values and were subsequently excluded for the final analysis, resulting in a study population of 290 patients for the present analysis. Of these 290 patients included in the primary analysis, 165 patients had a follow-up blood draw and were considered for the long-term analysis. A detailed flow chart of the composition of our patient cohort is shown in Figure 1. The population comprises AMI patients, who were included between July 2012 and February 2014 at the Medical University of Vienna (Austria). All patients were older than 18 years. Inclusion criteria were written informed consent obtained before the study entry, treatment with prasugrel or ticagrelor for AMI and age >18 years. The only exclusion criterion was participation in another trial. AMI was defined in accordance to the guidelines of the European Society of Cardiology. 14 The study was approved by the Ethics Committee of the Medical University of Vienna (1051/2012) and conducted in accordance to the current criteria of the Declaration of Helsinki.
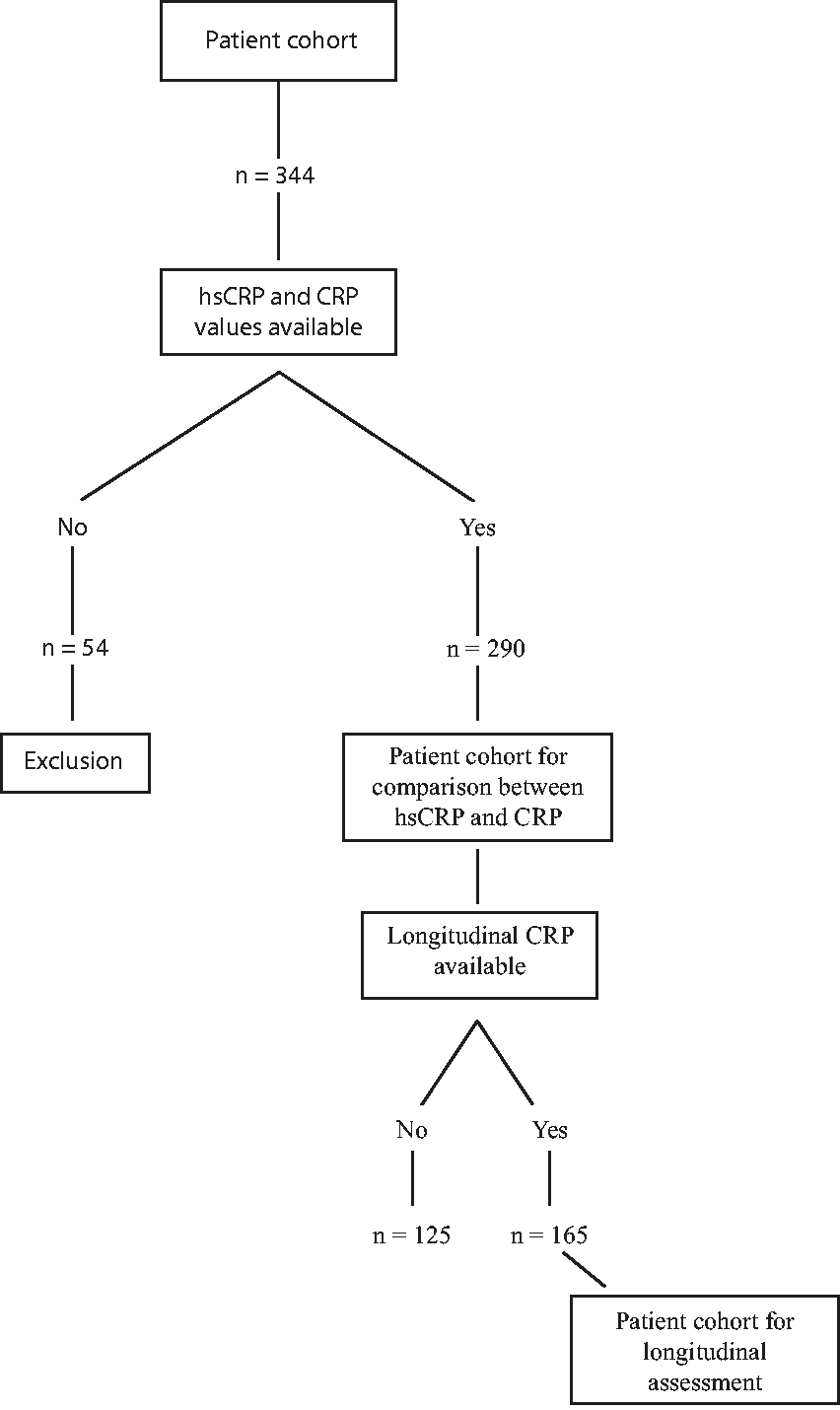
Flow chart of patient cohort.
Clinical follow-up and study endpoints
Patient-relevant characteristics were assessed via the patients' electronic medical records of the Medical University of Vienna and a standardized follow-up procedure. Data assessment was performed by specially trained chart reviewers that inserted predefined patient characteristics into a record abstraction form to analyse the registry further. The primary endpoint was defined as long-term all-cause mortality. Incidence of MACE within one year after discharge was regarded as our secondary endpoint. MACE was defined as non-fatal myocardial infarction, non-fatal stroke and CV death.
The date and cause of all-cause mortality were obtained via the Austrian national registry of death. The respective cause of death was defined according to the 10th revision of the International Code of Diseases (ICD-10).
Biomarker assessment
Peripheral venous blood samples of all participants were taken at the time of study inclusion (after acute event). Routine laboratory parameters were analysed and processed according to local laboratory standards. Follow-up CRP values were assessed during subsequent hospitalizations.
CRP and hsCRP concentrations were assessed at the Department of Laboratory Medicine of the Medical University of Vienna. For this purpose, venous blood samples were drawn (VACUETTE® CAT Serum Sep Clot Activator; 8 mL). Laboratory parameters were analysed according to the standard operating procedures of the department.
CRP was measured with turbidimetric immunoassay on Roche Diagnostics Cobas c 701/702. The detection limit was 0.2 mg/L; the measurement range was between 0.6 and 350 mg/L. The intra-assay imprecision profile of the CRP assay is 0.0793 mg/L for a mean value of 3.66 mg/L and 0.0676 mg/L for a mean value of 1.41 mg/L.
HsCRP was measured with particle-enhanced turbidimetric immunoassay on Roche Diagnostics Cobas c 701/702. The detection limit was 0.15 mg/L; the measurement range was between 0.15 and 20 mg/L. The intra-assay imprecision profile of the hsCRP assay is 0.04 mg/L for a mean value of 4.13 mg/L and 0.012 mg/L for a mean value of 0.511 mg/L.
Cardiac troponin T was measured with enzyme-linked immuno-culture assay on Roche Diagnostics Cobas e 801. The detection limit was 2.5 ng/L; the measurement range was between 3 and 10,000 ng/L. The intra-assay imprecision profile of the troponin T assay is 0.525 pg/mL for a mean value of 12.5 pg/mL and 3.76 pg/mL for a mean value of 166 pg/mL. All assays were performed according to manufacturer instructions.
When comparing CRP and hsCRP, hsCRP was chosen as a reference value. An established cut-off for hsCRP of >2 mg/L was used to stratify patients with high vs. low CRP or hsCRP at the time point of AMI.9,12 Additionally, during the stable phase of the disease, after AMI discharge, patients were stratified into two groups: at high vs. low inflammatory risk. High inflammatory risk was defined as CRP >2 mg/L at any time point of assessment during the stable phase of the coronary artery disease (CAD) (starting six months after hospital discharge for AMI). Patients at low residual inflammatory risk had low CRP (≤2 mg/L) at all time points of assessment during the stable phase of the CAD (starting six months after hospital discharge for AMI). Out of 344 patients, 165 patients had a longitudinal CRP assessment during the stable phase of the disease, starting at six months after AMI (available for two to six time points). A mean of 2.6 measurements had been performed per patient. Measurement was done upon non-scheduled clinical contacts. Patients with acute infections and tumour diseases were excluded from the analysis.
Statistical analysis
Discrete data are presented as counts and percentages. Continuous variables are shown as means and their respective standard deviation (SD). The Spearman ranks correlation test was used for computations of associations. A Bland-Altman analysis was performed to determine the 95% limits of agreement between both methods. Receiver operating characteristic (ROC) analysis was used to assess the predictive accuracy of CRP and hsCRP to predict long-term mortality and MACE within one year in patients after AMI.
A log-rank test was used to compare survival between patients with low residual inflammatory risk and high residual inflammatory risk. Kaplan Meier analysis was used for comparison of survival. Statistical significance was defined by two-sided P-values < 0.05. Statistical analyses were performed using SPSS 26.0 (IBM SPSS, USA).
Results
Patient cohort
Detailed baseline characteristics are summarized in Table 1. In short, out of the entire study population (n = 290, mean age: 59 ± 12 years; 80% male gender) presenting with AMI, a representative number of participants were presenting with STEMI (n = 174; 60%). The majority of patients had CV risk factors as high blood pressure (63%), smoking history (73%), or family history of CAD (50%). Diabetes mellitus was diagnosed in 21% of patients. The use of beta-blockers (94%), statins (93%) and proton pump inhibitors (75%) was high.
Baseline characteristics.
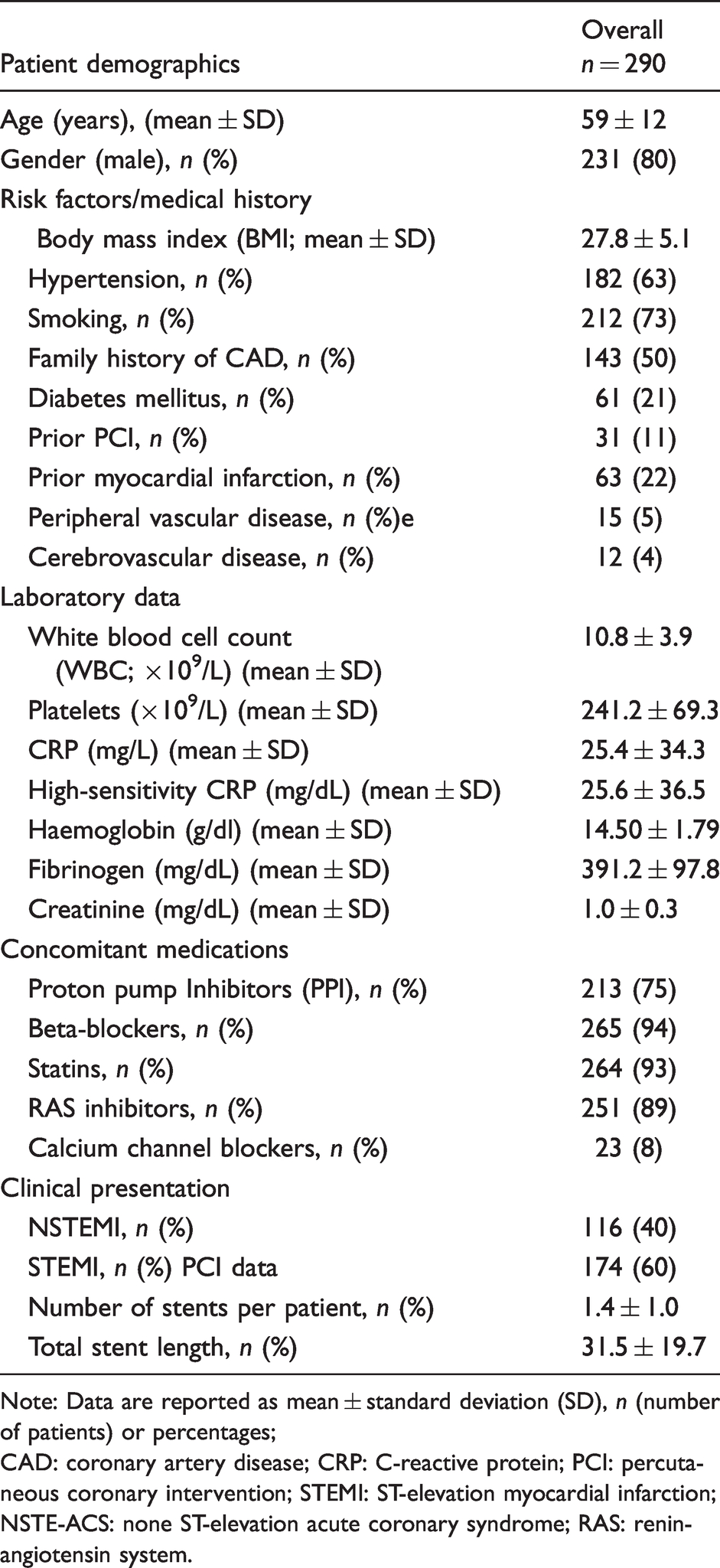
Note: Data are reported as mean ± standard deviation (SD), n (number of patients) or percentages;
CAD: coronary artery disease; CRP: C-reactive protein; PCI: percutaneous coronary intervention; STEMI: ST-elevation myocardial infarction; NSTE-ACS: none ST-elevation acute coronary syndrome; RAS: renin-angiotensin system.
Classification on the basis of CRP measurements on admission
Classification of patients to low vs. high hsCRP and CRP values based on established cut-offs was determined on the basis of 290 (84.3%) valid patient protocols. When both hsCRP and CRP were divided into high and low values and compared, a diagnostic accuracy of 98.6% was found: 92.8% were described as both high (true positive) and 5.9% as both low (true negative). Only 1.4% of patients (n = 4) were high in the CRP test, but low in hsCRP (false positive), 0% were false negative (Table 2).
Agreement of CRP and hsCRP values according to a cut-off value of 2 mg/L (hsCRP was chosen as reference).
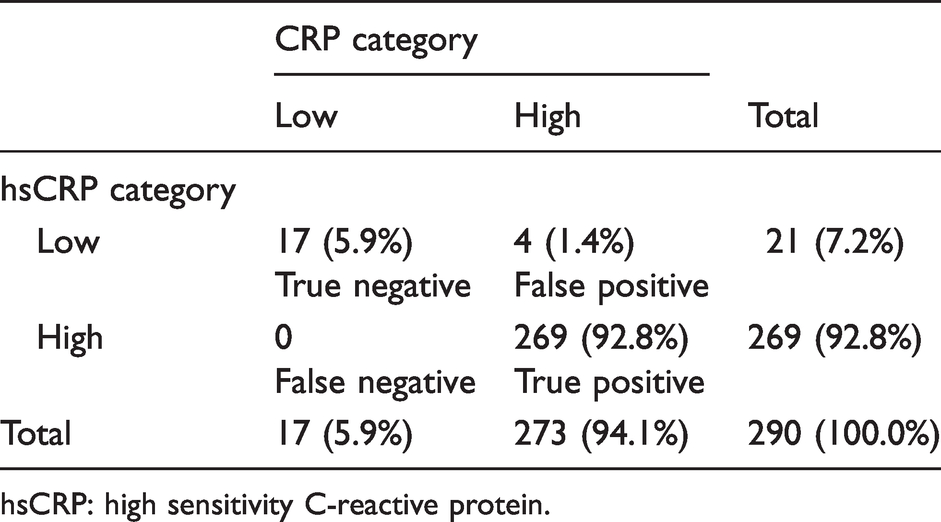
hsCRP: high sensitivity C-reactive protein.
Overall agreement between the two CRP methods based on the entire cohort of CRP measurements
The agreement between both methods was determined on the basis of 290 (84.3%) valid patient protocols. There was a high correlation between hsCRP and CRP (r = 0.99; P < 0.001) (Figure 2(a)). The relevant intraclass correlation coefficient (ICC) was 0.994, 95% CI (0.993–0.995).
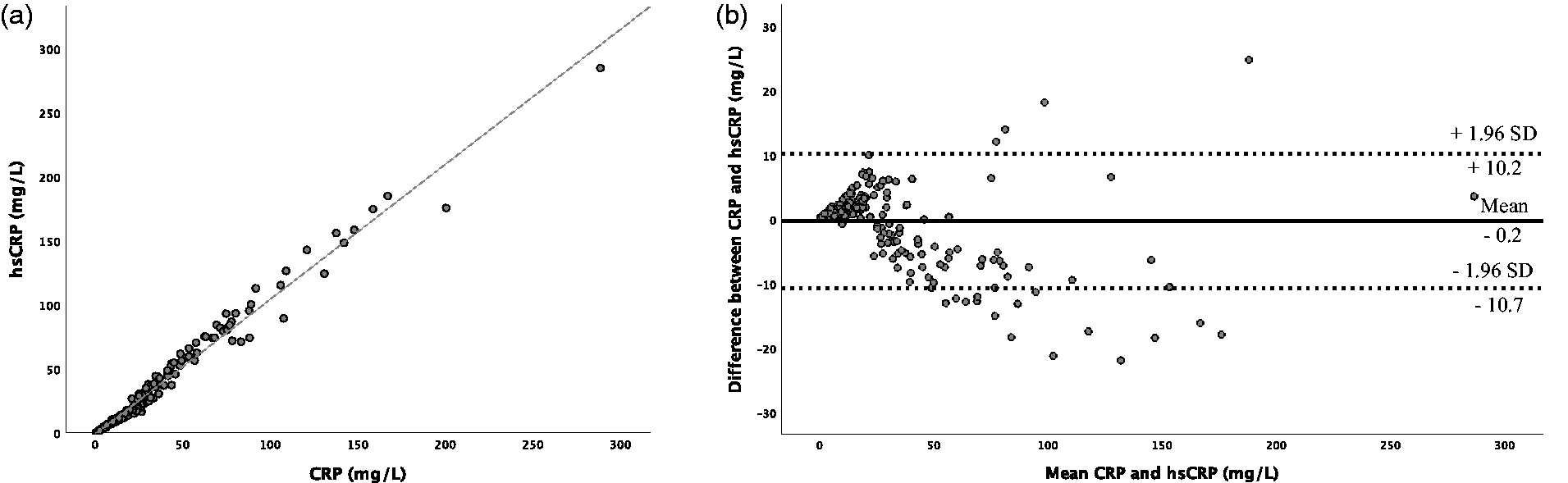
(a) Correlation between hsCRP and CRP and (b) Bland-Altman plot comparing CRP with hsCRP.
In the Bland-Altman analysis, the average difference was –0.23 ± 5.34 mg/L. The difference between both measurements was within –10.7 and +10.3 (±1 SD, 95% limit of agreement, LOA) (Figure 2(b)). Fifteen (5.2%) values were below –10.7 and four (1.4%) were above +10.3. With increasing levels, the agreement between both methods was less accurate, as shown in Figure 2(b).
Overall agreement on short-term and long-term risk stratification
Among the entire cohort (n = 290), 37 individuals (10.8%; including 16 patients [43.2%] with a fatal CV event) died after a median follow-up time of six years. ROC analysis was used to compare CRP and hsCRP to predict long-term mortality and MACE within one year.
When assessed at the time point of AMI, CRP and hsCRP had a low and similar AUC for prediction of mortality. The AUC for CRP was 0.565, 95% CI (0.462–0.669), P = 0.228 compared with 0.572, 95% CI (0.470–0.675), P = 0.184 for hsCRP (Table 3). In comparison, troponin-T (measured upon admission) had a higher but still not sufficient AUC for prediction of mortality (AUC 0.635, 95% CI [0.554–0.717], P = 0.010).
ROC curve estimates for prediction of long-term mortality and one-year MACE.
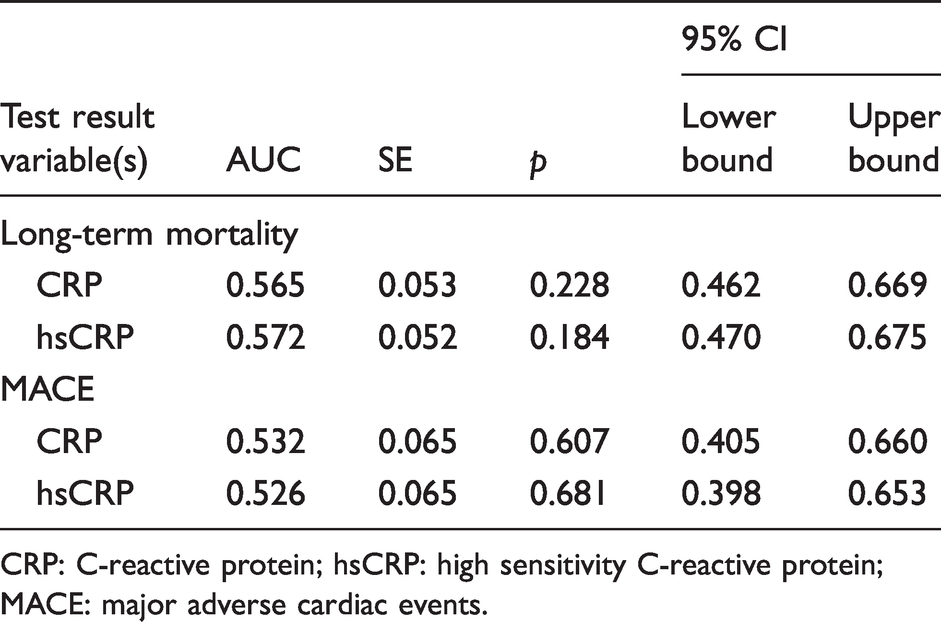
CRP: C-reactive protein; hsCRP: high sensitivity C-reactive protein; MACE: major adverse cardiac events.
Neither CRP (AUC 0.532, 95% CI [0.405–0.660], P = 0.607) nor hsCRP (AUC 0.526, 95% CI [0.398–0.653], P = 0.681) predicted MACE within one year of PCI (Table 3).
Longitudinal assessment of CRP after hospital discharge
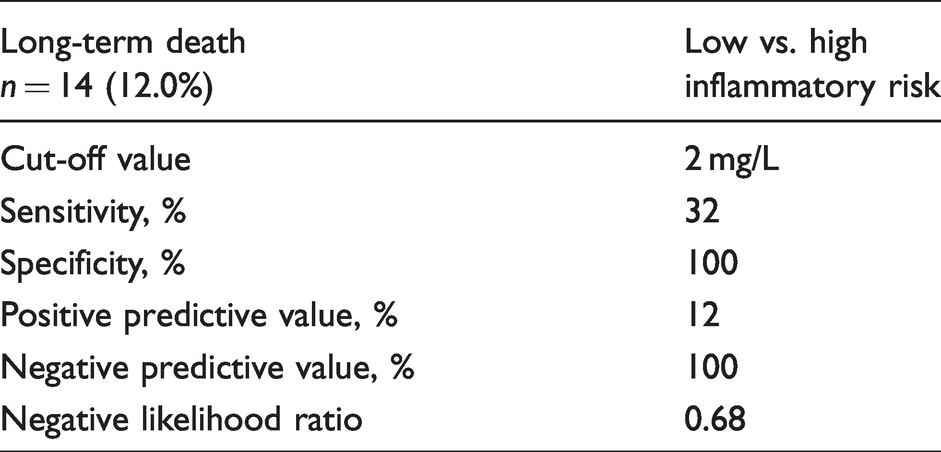
Of 165 patients with serial CRP assessment, 117 (71%) were at high inflammatory risk, and 48 patients (29%) at low inflammatory risk according to the previously established cut-off. All-cause death was observed in 14 patients (12.0%) with high residual inflammatory risk compared with no patients with low residual inflammatory risk (P = 0.012) (see Table 1 in supplemental appendix). Inflammatory risk assessment with serial CRP measurements had 100% specificity and 100% negative predictive value, 32% sensitivity and 12% positive predictive value (Table 4). The Kaplan Meier survival analysis highlighted a higher risk of long-term death (P = 0.014) for individuals with high residual inflammatory risk as compared with patients with low residual inflammatory risk (Figure 3).
Statistical estimates for the prediction of long-term mortality in patients assigned to the low vs. high inflammatory risk.
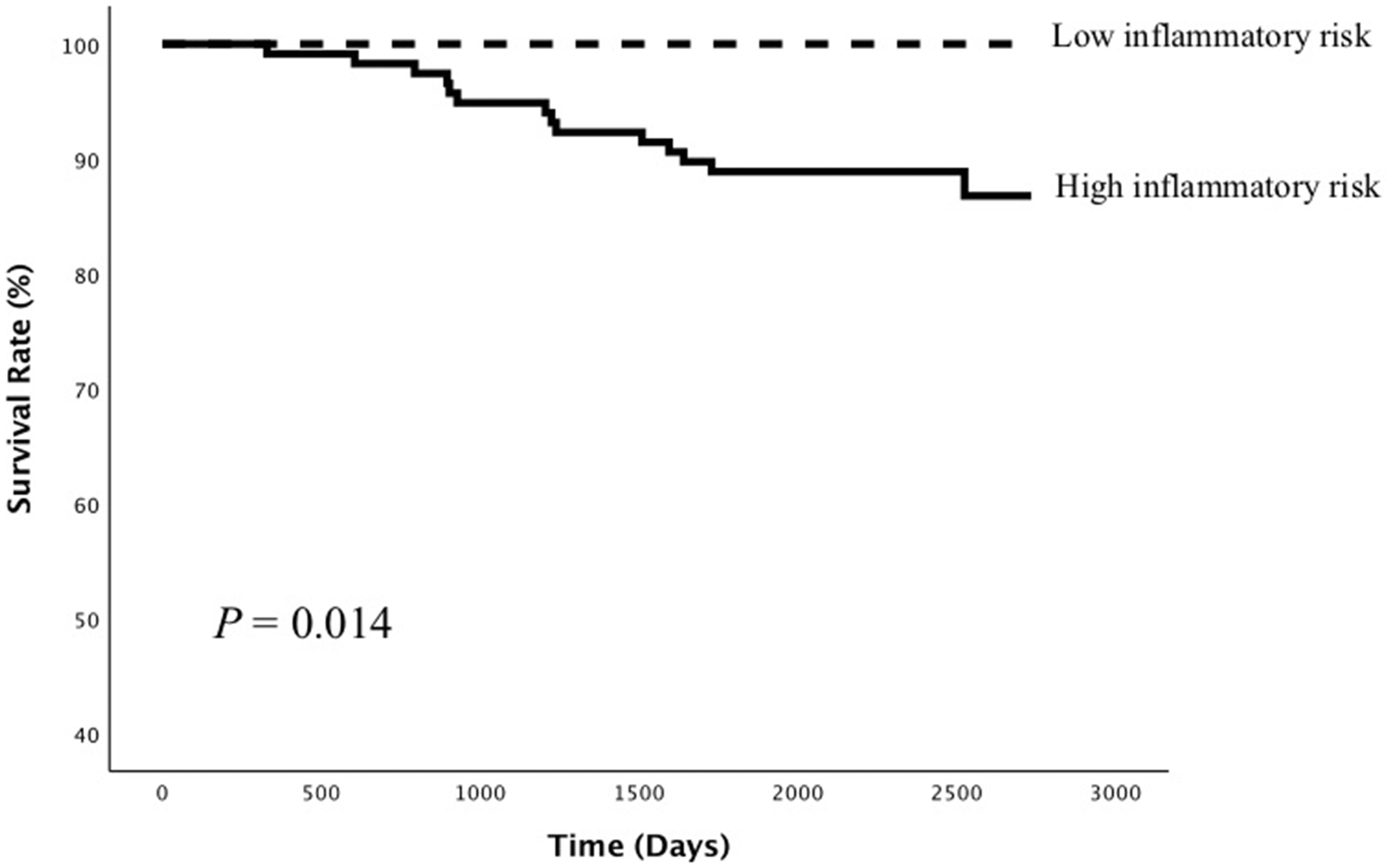
Survival curves of all-cause death between patients with high vs. low inflammatory risk.
Discussion
The current analysis is – to the best of our knowledge – the most extensive comparison of the diagnostic accuracy of CRP and hsCRP in the acute phase of AMI and as continual assessment. Besides, we investigated the association of high residual inflammatory risk assessed during the stable phase of the disease with patients’ outcomes. Our data highlight that
CRP and hsCRP show a high degree of correlation and agreement and hsCRP might be replaced by CRP in the acute phase of AMI. CRP and baseline hsCRP assessed in the acute phase of AMI do not predict long-term mortality or one-year MACE in patients undergoing PCI. Low CRP values at all serial assessments after AMI discharge are associated with an excellent negative predictive value of 100% for long-term mortality.
Diagnostic accuracy of hsCRP vs. CRP
Within the present investigation, we showed that the diagnostic accuracy of CRP compared with hsCRP was high (98.6%). The main historical difference between CRP and hsCRP was that CRP had been postulated to be sensitive within the range of 10 to 1000 mg/L, while hsCRP shows the highest sensitivity in the range from 0.5 to 10 mg/L. 13 Due to this difference, some older studies assumed that hsCRP is more accurate in predicting CV events than CRP.13,15 However, the sensitivity of CRP changed over time, and our study clearly shows that there is a high correlation and agreement between CRP and hsCRP values. The high correlation between these measurement methods shows that the information obtained from both is virtually interchangeable, questioning whether hsCRP still should be assessed in patients with available CRP measurements. Our data clearly highlight that the measurement of hsCRP does not provide any additional benefit. Thus, by omitting an additional hsCRP measurement, not only costs can be saved but the additional effort can be reduced. However, we observed that with increasing CRP concentrations, the agreement between both methods was less accurate, which is, however, of less relevance as those patients would be already classified with high inflammatory risk.
hsCRP and CRP as predictors for cardiovascular risk
The definition of an elevated CRP has evolved. Older studies indicated that in patients with established CV diseases, CRP values of >3 mg/L could be considered as elevated and >10 mg/L as highly elevated.16,17 However, more recent studies assume that CRP values of >2 mg/L can be regarded as already increased.9,12 Based on these studies, we have chosen our cut-off value of 2 mg/L.
CRP concentration is routinely measured to stratify risk in acute coronary syndrome.18,19 However, the mechanisms that link CRP concentrations with CV morbidity and mortality in these patients remain controversial. In accordance with a previous study from Kennon et al., we were able to show that in patients presenting with AMI, neither baseline CRP nor baseline hsCRP concentrations were associated with all-cause mortality. 20 Therefore, we have shown that both baseline CRP and baseline hsCRP concentrations did not provide prognostic information on outcomes in patients with AMI undergoing PCI. These results are in line with previous observations showing that CRP's independent power to predict CV disease has not been as powerful as expected.20–23 However, there is no doubt of the key role of chronic inflammation in the pathogenesis of atherosclerosis and plaque instability and its future use of CRP as a marker of coronary risk in apparently healthy individuals. 24 In line, patients with diabetes mellitus represent a special population with a heightened inflammatory status, which should be further investigated in future trials.25,26
Low serial CRP as an independent predictor for favourable long-term outcome
Of utmost interest, in our study, low residual inflammatory risk was associated with 100% long-term survival in patients with AMI undergoing PCI. Some studies could find an association between single pre-procedural CRP and clinical outcomes after AMI.27–29 However, there is little evidence for the association of post-procedural CRP and clinical outcomes. A study of Pokharel et al. showed that a single hsCRP at 30 days postmyocardial infarction or PCI has no association with clinical outcomes. 30 Kalkman et al.’s results support our findings that low residual inflammatory risk is associated with a favourable outcome. 12
In our study, the positive predictive value of 12.0% was low which is consistent with a multicentre prospective trial by Bogaty et al. 31 Another study, in contrast, has postulated that CRP can be used for risk stratification in patients with AMI. 32 In line with our study, other analyses had demonstrated that inflammatory status is a strong predictor for adverse clinical outcomes in patients in a stable phase of atherosclerotic disease, even when LDL cholesterol was reduced by PCSK9.33,34 Suppression of chronic systemic inflammation might therefore reduce this risk, as all patients with low inflammatory risk survived in our study.
Prevalence of high residual inflammatory risk
Within the present investigation, in almost half of the patients with AMI undergoing PCI, serial CRP was available. A high percentage of those patients (70.9%) presented with high residual inflammatory risk. Compared with Kalkman et al., the prevalence of patients with high residual inflammatory risk in our study risk was slightly higher (70.9% vs. 63.5%). 12 This might be due to the definition of high inflammatory risk in our study. While in our study high inflammatory status was defined as a CRP >2 mg/L at any time point of assessment during the stable phase of the disease, Kalkman et al. defined high residual inflammatory risk with two high CRP values. 12 In contrast, Kuch et al. observed a lower prevalence of patients with a high residual inflammatory risk of 55.8%, which might be due to a higher CRP cut-off point of 3 mg/L. 32
Clinical implications
Inflammation plays a crucial role in increasing cardiovascular risk and all-cause mortality. We were able to show that serial low CRP values are positively associated with long-term survival.
Future strategies for the treatment of AMI might include immunosuppressive therapy to reduce the increased risk of mortality. The CANTOS trial (Canakinumab Anti-Inflammatory Thrombosis Outcomes Study) showed that targeting the interleukin 1ß innate immunity pathway with canakinumab in patients with previous myocardial infarction and a hsCRP >2 mg/L led to a significantly lower rate of CV events independent of lipid lowering. 9 Furthermore, Ridker et al. showed that the extent of CRP reduction was associated directly with the magnitude of clinical benefit. 9 In the JUPITER trial, Ridker et al. have shown that rosuvastatin significantly reduces the incidence of major CV events in healthy patients without hyperlipidaemia but with elevated hsCRP concentrations. 35 Our data highlight that low serial CRP values after AMI and PCI were independently and directly associated with favourable survival. Importantly, CRP or hsCRP during AMI were not reliable predictors of all-cause mortality. Further studies are needed to investigate if reducing the inflammatory burden in this particular patient population can decrease CV events and mortality.
Limitations
One potential limitation of this study is that it is based on data from a single high-volume care centre, limiting the generalizability of our results. Another limitation is the relatively small sample size and the large proportion of patients with STEMI. Moreover, there was no standardized follow-up procedure and serial CRP measurements were only available in 48% of cases in our study.
Conclusion
CRP and hsCRP provide a similar laboratory sensitivity and accuracy, which implicates that CRP can replace hsCRP in routine assessments. Interestingly, patients with low residual inflammatory risk during the stable phase after AMI have excellent six-year survival. Importantly, inflammatory status during the acute phase of AMI does not provide prognostic information on the patient’s outcome.
Supplemental Material
sj-pdf-1-acb-10.1177_00045632211004651 - Supplemental material for Comparison of high-sensitivity C-reactive protein vs. C-reactive protein for diagnostic accuracy and prediction of mortality in patients with acute myocardial infarction
Supplemental material, sj-pdf-1-acb-10.1177_00045632211004651 for Comparison of high-sensitivity C-reactive protein vs. C-reactive protein for diagnostic accuracy and prediction of mortality in patients with acute myocardial infarction by Felix Hofer, Thomas Perkmann, Gloria Gager, Max-Paul Winter, Alexander Niessner, Christian Hengstenberg and Jolanta M Siller-Matula in Annals of Clinical Biochemistry
Supplemental Material
sj-pdf-2-acb-10.1177_00045632211004651 - Supplemental material for Comparison of high-sensitivity C-reactive protein vs. C-reactive protein for diagnostic accuracy and prediction of mortality in patients with acute myocardial infarction
Supplemental material, sj-pdf-2-acb-10.1177_00045632211004651 for Comparison of high-sensitivity C-reactive protein vs. C-reactive protein for diagnostic accuracy and prediction of mortality in patients with acute myocardial infarction by Felix Hofer, Thomas Perkmann, Gloria Gager, Max-Paul Winter, Alexander Niessner, Christian Hengstenberg and Jolanta M Siller-Matula in Annals of Clinical Biochemistry
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of the Medical University of Vienna (1051/2012) and conducted in accordance to the current criteria of the Declaration of Helsinki.
Guarantor
JMSM.
Contributorship
FH: analysed data and wrote paper; TP: designed study; GG: collected data; MPW: collected data and contributed important reagents; AN: contributed important reagents; CH: contributed important reagents; JMSM: performed study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.