
Abstract
Background
Serum high-sensitive C-reactive protein (hs-CRP) concentrations independently predict the development of diabetes, metabolic syndrome and cardiovascular disease. However, the impact of dietary factors on serum high-sensitive C-reactive protein concentrations in diabetic patients has received limited attention. We aimed to investigate the association between dietary factors and high-sensitive C-reactive protein , among diabetic patients with and without hypertension and healthy subjects.
Methods
In this cross-sectional study, diabetics with (n = 325) and without hypertension (n = 599) and healthy individuals (n = 1220) were recruited in Mashhad, Iran. Dietary intake was assessed by 24-h recall. Biochemical parameters including serum high-sensitive C-reactive protein were measured using standard protocols. Stepwise multiple regression analysis was used to predict whether serum high-sensitive C-reactive protein concentration was associated with dietary constituents.
Results
High-sensitive C-reactive protein was significantly higher among hypertensive and non-hypertensive diabetic patients compared with healthy subjects (P < 0.001). The dietary intake of zinc + 6.4% and calcium −3.4% and body mass index +3.9% explained approximately 13.7% of the variation in serum high-sensitive C-reactive protein among diabetic hypertensive patients. Approximately 9.7% of the variation in serum high-sensitive C-reactive protein in diabetic non-hypertensive patients could be explained by body mass index, and intake of sodium, iron and cholesterol. In the healthy subjects, approximately 4.4% of the total variation in serum high-sensitive C-reactive protein concentration could be explained by cholesterol consumption and waist circumference.
Conclusion
Serum high-sensitive C-reactive protein concentrations were found to be a significant predictor for hypertensive and non-hypertensive diabetic subjects. There was a significant association between dietary factors include zinc, iron, sodium and cholesterol and serum high-sensitive C-reactive protein, while there was an inverse association between dietary calcium and serum high-sensitive C-reactive protein in diabetic hypertensive individuals.
Introduction
The prevalence of diabetes mellitus is increasing globally and has become a challenging issue for public health in both developed and developing nations.1,2 In 2015, the number of people with diabetes mellitus was estimated to be approximately 415 million by the International Diabetes Federation (IDF). 3 Approximately 7.7% of Iranian adults (2 million adults) have diabetes mellitus. 4
Raised serum inflammatory markers, that include high-sensitive C reactive protein (hs-CRP), are reported to be associated with several non-communicable conditions including obesity 5 hypertension, 6 metabolic syndrome, 7 diabetes mellitus and cardiovascular disease. 8 hs-CRP is a marker of systemic inflammation and is produced by the liver in response to pro-inflammatory cytokines such as interleukin 6 (IL-6). 9
Inflammatory factors are thought to be involved in the pathogenesis of insulin resistance, 10 diabetes mellitus 11 and metabolic syndrome, 12 and it has been suggested that an elevated hs-CRP should be added to the definition of metabolic syndrome. 8 Although there is a positive association between several factors such as smoking, 13 physical inactivity, 14 waist circumferences (WCs), 15 body mass index (BMI) 15 and serum hs-CRP, the relationship between specific dietary components and serum hs-CRP is unclear. A significant inverse association has been shown between some dietary items including fruits and vegetables, 16 fish and poultry, 17 dietary fiber, 18 oleic acid 19 and serum hs-CRP, whereas a significant positive association has been reported between the consumption of red meat, 20 trans-fat, 21 and saturated fat 22 and serum hs-CRP. Other studies have reported no significant association between consumption of fiber, 23 carbohydrate, protein, total fat 22 and trans fatty acid 24 and serum hs-CRP. In this study, we aimed to investigate the association between the intake of energy and macronutrients including carbohydrate, fat and protein, antioxidants including vitamins E and C, and the other specific dietary components such as potassium, calcium, magnesium, phosphorus, iron, copper, zinc, selenium, iodine, folate and sodium and the level of serum hs-CRP among diabetics with and without hypertension and within healthy subjects, derived from a large sample of Iranian adults.
Methods
Study design and subject selection
This cross-sectional study is a part of ongoing large cohort study entitled Mashhad stroke and heart atherosclerotic disorder (MASHAD) study. 25 As previously described in detail, 25 in the first phase of the MASHAD study, participants were drawn from three regions in Mashhad using stratified cluster randomized sampling. Each region was divided into nine sites centred upon Mashhad Healthcare Center divisions. Households with individuals of eligible age between 35 and 65 years were identified and contacted by telephone to arrange an appointment for the formal physical examination. 25 Finally, from a total of 2,427,117 residents of Mashhad city, 11,800 individuals were chosen to participate in the study, of whom a total of 9761 participants, mean age 48.1 years old agreed to participate. The demographic, anthropometric and lifestyle data were obtained by two expert health-care professionals and a nurse. Exclusion criteria were pregnancy and lactation, established cardiovascular disease, cancer or chronic kidney and consumption of dietary supplements. All diabetic subjects who were either hypertensive (n = 325) or non-hypertensive (n = 559) were selected for this sub-study. Healthy individuals (subjects without any history of cardiac disease, metabolic abnormalities or clinical disorders categorizes as healthy individuals), drawn from the same region were matched with the case participants as a healthy group (n = 1220) (control group).
Anthropometric and biochemical measurements
Anthropometric measurements, including weight, height, WC and hip circumference were measured by trained nurses. All of the anthropometric measurements were made in duplicate and the average value recorded. BMI was computed as weight in kilograms divided by the square of height in metres. Resting blood pressure was measured three times using a standardized protocol and the mean of these records was reported as subject’s blood pressure. Fasting blood samples were obtained early in morning after a 12 h fast and stored at −80℃. Enzymatic methods and auto-analyser (BT3000 biotechnical instruments company, Spain) were used to measure serum triglycerides (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (FBG) and hs-CRP. Low-density lipoprotein cholesterol (LDL-C) was calculated using Friedewald formula if serum TGs concentrations were lower than 400 mg/dL. 26 The intra- and inter-assay coefficients of variation of FBG were ≤1.72% and ≤1.16%, respectively. The intra- and inter-assay coefficients of variation of lipids profile were less than 5%. The intra- and inter-assay coefficients of variation of hs-CRP were ≤2.27% and ≤8.52%, respectively. The standard protocols for the anthropometric and biochemical assessment have been reported previously. 25
Assessments of dietary intakes
Data on the dietary intake of the study participants were collected using 24-h recall, by a trained interviewer. For the analysis of the dietary intake, Dietplan6 software was used (Forest field Software Ltd, UK).
Assessment of metabolic disorders
Blood pressure equal or greater than 140/90 mmHg was defined as hypertension. 27 Individuals with an FBG ≥7 mmol/L) or higher on two separate tests, or those under treatment with oral hypoglycaemic agents or insulin were considered to be diabetic. 28
Assessment of other variables
Demographic and lifestyle information including age, smoking status, medical history and drug use were obtained by expert interviewers using a structured questionnaire. Physical activity level (PAL) was measured using the James and Schofield human energy requirements equations 29 and was calculated as the total energy expenditure (TEE): basal metabolic rate (BMR) ratio over a 24-h period. Questions on physical activity were based on the James and Schofield equations and were selected from those used in the Scottish Heart Health Study (SHHS)/MONICA questionnaire. Questions were included to assess the time spent on activities during work (including housework), outside work and in bed (resting and sleeping). 30
Statistical methods
Statistical analysis was undertaken with SPSS software version 16.0 (SPSS® Inc., Chicago, IL). Normality of data was assessed by using the Kolomogorov-Smirnov test. We used parametric tests for normally distributed data and non-parametric test for non-normally distributed data. Between-group comparisons of continuous variables were assessed by one-way ANOVA for parametric data and Mann-Whitney for non-parametric data. Chi-square test was used for assessment of categorical data between groups. The dietary intakes were found to be non-normally distributed and were therefore compared using Mann-Whitney tests. Nutrient intakes adjusted for total energy intake through the residual method and expressed in grams, milligrams and micrograms. To predict the associations of serum hs-CRP concentrations and dietary intake, we used linear regression analysis. To enable adjustment for potential confounding factors, we entered into the equation the factors age, sex, smoking, PAL, BMI, WC, SBP, DBP, LDL-C, HDL-C, FBG, TC and TG. A P value of <0.05 was considered significant.
Results
General characteristics and anthropometric measurements in diabetic hypertensive, diabetic non-hypertensive patients and healthy subjects
General characteristics and anthropometric measurements in patients and healthy subjects. a
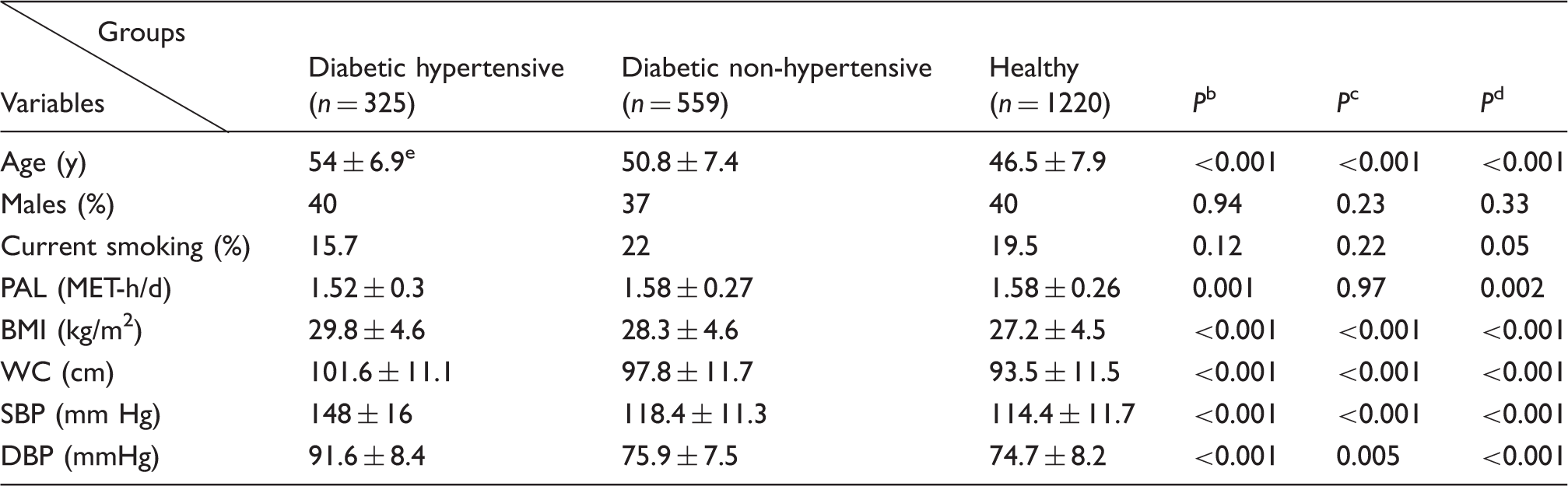
PAL: physical activity level; BMI: body mass index; WC: waist circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Continuous data were compared by one-way ANOVA and categorical variables were compared by chi-square test.
Diabetic hypertensive in compared with the healthy.
Diabetic non-hypertensive in compared with the healthy.
Diabetic hypertensive in compared with the Diabetic non-hypertensive.
Mean ± standard deviation.
Clinical and biochemical parameters
Serum biochemical measurements in patients and healthy subjects. a
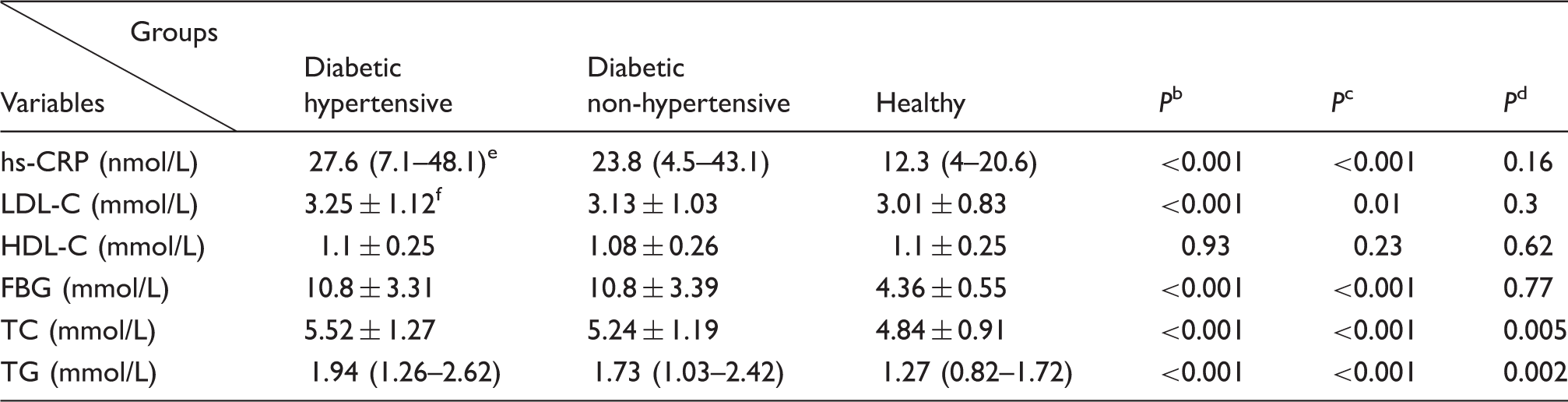
hs-CRP: high-sensitive C-reactive protein; LDL-C: low-density lipoprotein-cholesterol; HDL-C: high-density lipoprotein-cholesterol; FBG: fasting blood glucose; TC: total cholesterol; TG: triglyceride.
Continuous data were compared by one-way ANOVA or Mann-Whitney and categorical variables were compared by chi-square test.
Diabetic hypertensive in compared with the control.
Diabetic non-hypertensive in compared with the control.
Diabetic hypertensive in compared with the diabetic non-hypertensive.
Median (interquartile range).
Mean ± standard deviation.
Dietary intake of macro- and micronutrients in diabetic hypertensive, diabetic non-hypertensive patients and healthy subjects
Comparison of macro- and micronutrient dietary intakes between patients and healthy subjects. a
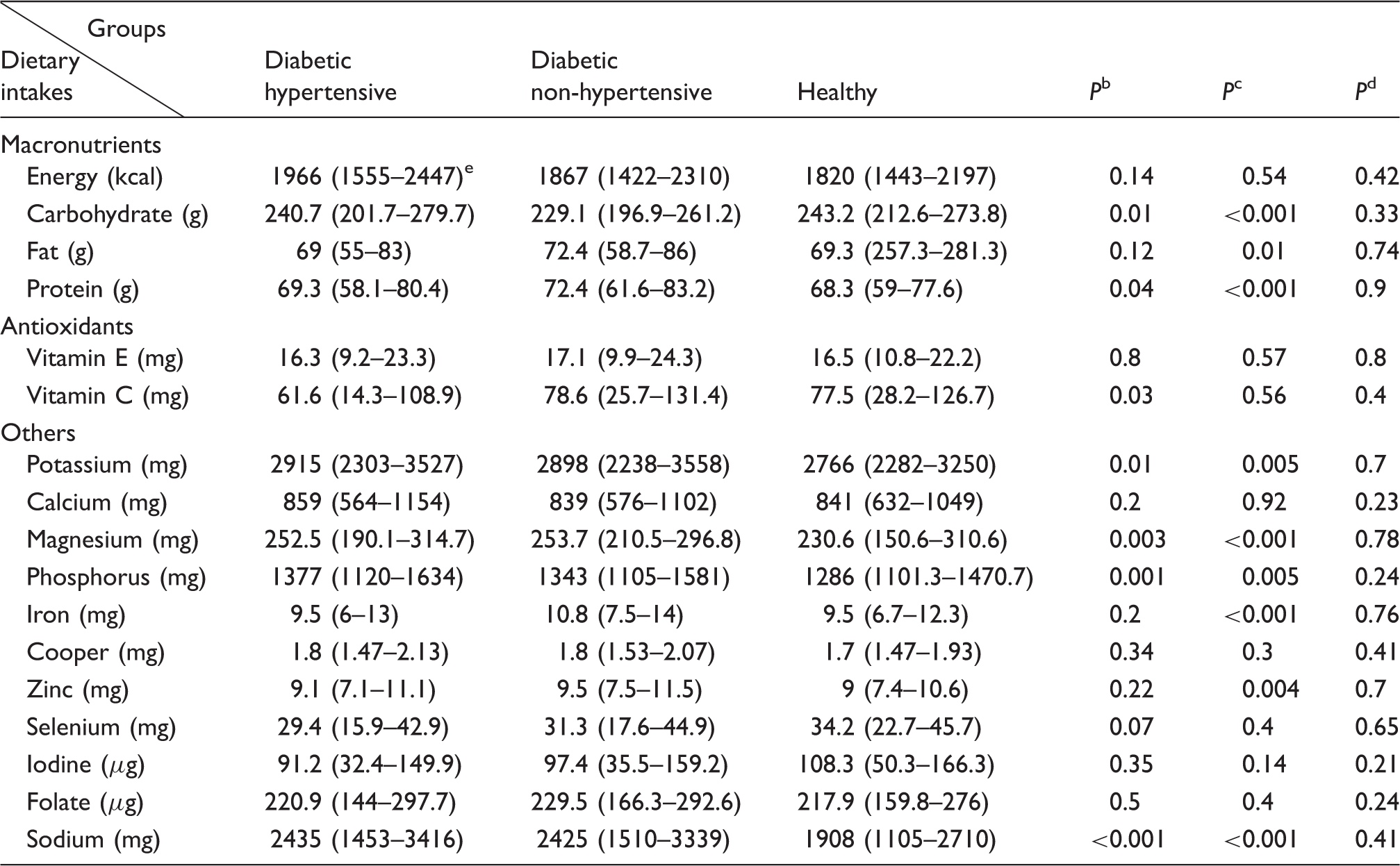
Obtained using Mann-Whitney test.
Diabetic hypertensive in compared with the healthy.
Diabetic non-hypertensive in compared with the healthy.
Diabetic hypertensive in compared with the diabetic non-hypertensive.
Median (interquartile range).
Multivariate analysis
Multifactorial analysis of serum high sensitive C-reactive protein in diabetic hypertensive patients. a
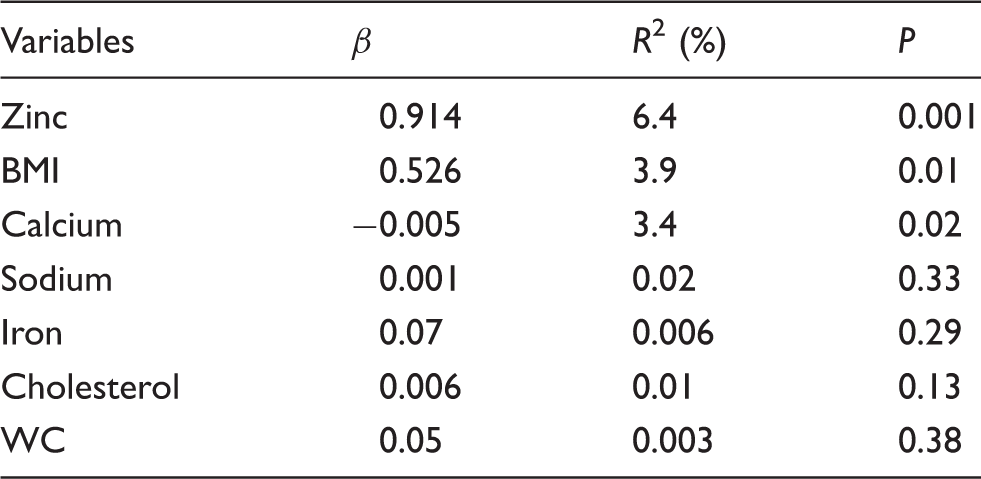
BMI: body mass index; WC: waist circumference.
Linear regression was used.
Multifactorial analysis of serum high sensitive C-reactive protein in diabetic non-hypertensive patients. a
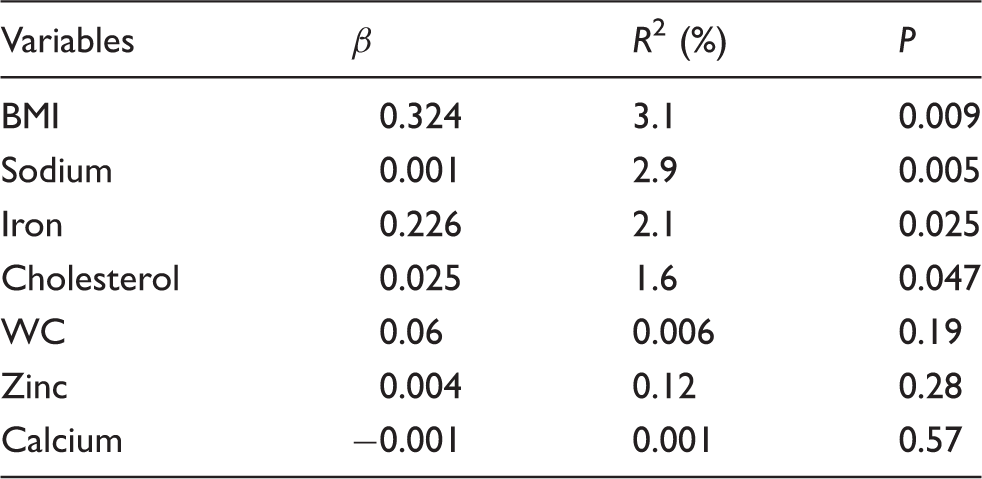
BMI: body mass index; WC: waist circumference.
Linear regression was used.
Multifactorial analysis of serum high sensitive C-reactive protein in healthy subjects. a
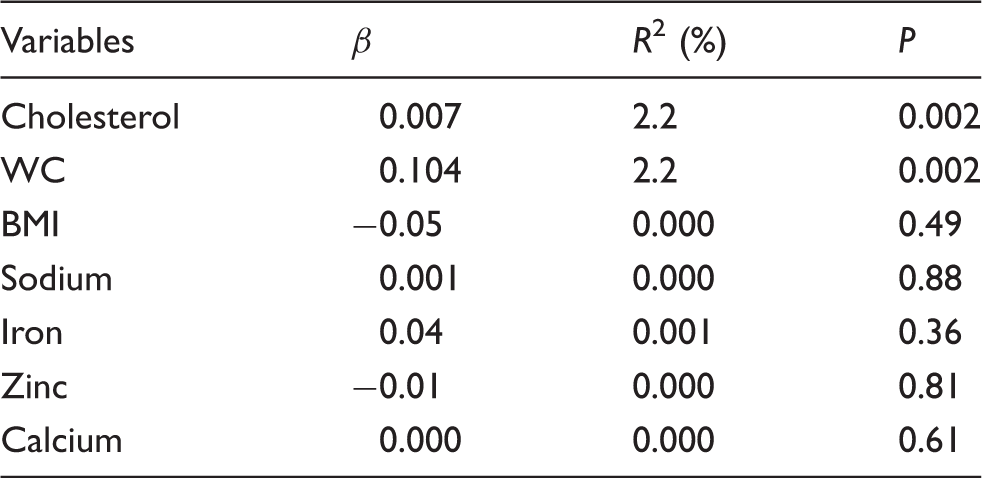
BMI: body mass index; WC: waist circumference.
Linear regression was used.
Discussion
The results of the current study showed that serum hs-CRP concentrations in diabetics with and without concomitant hypertension, were significantly higher than healthy individuals. In addition, some dietary items as well as some anthropometric parameters were significantly related to serum hs-CRP concentrations. To the best of our knowledge, this is the first study investigating the association between serum hs-CRP with dietary intake in healthy and diabetic hypertensive and diabetic non-hypertensive patients. It appears that hs-CRP concentrations increased in association with both diabetes mellitus 8 and hypertension, 6 and hypertension is highly prevalent among diabetic patients 31 ; we therefore divided the diabetic patients into two subgroups.
While it has been shown previously that zinc supplementation reduces serum inflammatory markers such as hs-CRP and IL-6 among obese young women, 32 in our study, zinc was positively associated with hs-CRP in the diabetic hypertensive patients, suggesting more studies particularly longitudinal studies might be needed to clarify this relationship.
We found a significant association between the intake of iron and hs-CRP among diabetic non-hypertensive patients. It has been shown previously that a high consumption of iron is associated with increased risk of coronary heart disease (CHD) and type 2 diabetes.33,34 Indeed, it has been previously suggested that iron could cause an increased production of reactive oxygen species, oxidative stress and inflammation. 35 Results of a recent meta-analysis have shown that the intake of heme iron is positively associated with CHDs, 36 possibly related to the potential tissue-damaging inflammation which may be caused by heme iron in the oxidation of LDL.36–38
We found that serum hs-CRP concentrations in both diabetic subgroup patients were approximately two-fold higher than healthy individuals. In addition, BMI was significantly associated with elevated serum hs-CRP in both diabetic groups. Earlier reports have indicated that obesity, BMI, insulin resistance and metabolic syndrome are positively associated with low-grade inflammation particularly elevated blood hs-CRP.12,15,39–42 It has been suggested that an increased production of inflammatory markers such as IL-6 and tumour necrosis factor-alpha (TNF-α) associated with obesity, result in an increased synthesis and secretion of hs-CRP by the liver, and this may also lead to insulin resistance and diabetes mellitus among obese individuals.41,43 Following a healthy lifestyle, including a healthy diet and increased physical activity, both of which can normalize weight might be helpful to protect against elevated hs-CRP and several chronic diseases related to it.
We found an inverse association between dietary calcium and serum hs-CRP among diabetic hypertensive. There are limited data on the relationship between dietary calcium and serum hs-CRP concentrations. However, in a previous study examining the association between dairy products (highly source of calcium) intake and inflammatory markers such as hs-CRP and IL-6 and TNF-α, a significant reverse association was found between consumption of servings of dairy products per week and inflammatory markers. 44 In addition, in a study of Iranian women, a significant inverse association was found between the intake of low-fat dairy and hs-CRP though the relationship between intake of total dairy products and hs-CRP was not significant. 45 With regard to the inverse association between calcium intake and insulin resistance, obesity and CHD risk,46–49 and the positive association between BMI and serum hs-CRP concnetration,15,39 it is possible that our results on calcium intake and hs-CRP might be explained through an impact of dietary calcium on body weight.
Dietary intake of sodium was also associated with hs-CRP among diabetic non-hypertensive patients. A direct role of sodium in stimulation of inflammatory response and hypothesis that proposed sodium may increase the gene expression of inflammatory factors might be the possible mechanisms to explain the role of sodium in increasing inflammatory response.50,51 An association between sodium intake and serum CRP, which may be influenced by BMI, was found in a previous observational study, 52 which is consistent with our results. In their study, Zhu et al. 53 found a significant direct association between higher sodium intake and adipocyte dysfunction and inflammation among adolescents. However, in a recent randomized controlled clinical trial, investigating the effect of Dietary Approaches to Stop Hypertension (DASH diet), which contained restricted amount of sodium, on inflammation in gestational diabetes, there was no significant difference between serum hs-CRP among intervened and control groups. 54
We also found a significant positive association between cholesterol intake and hs-CRP concentration in the diabetic, non-hypertensive and healthy individuals. Hypercholesterolaemia and atherosclerosis are related to the consumption of high-fat, high-cholesterol diets, causing an accumulation of cholesterol in immune cells such as macrophages, which increases inflammatory response. 55 Furthermore, the results of a previous rodent study indicated that hepatic inflammation occurs by dietary cholesterol, rather than liver steatosis, suggesting dietary cholesterol should be considered as a salient factor of hepatic inflammation. 56
With respect to the significant positive association between WCs and plasma hs-CRP in healthy participants in this study, previous studies have investigated the relationship between component of metabolic syndrome and serum hs-CRP, and it has been shown that central obesity is a major determinant of increased hs-CRP in metabolic syndrome. 57 Similarly, other reports have indicated that WC is an important determinant of serum hs-CRP.15,58 In a study conducted among healthy men, there was a significant association between abdominal adipose tissue and elevated hs-CRP, suggesting that although the best predictor of CRP levels is the amount of total body fat, abdominal fat deposition should be considered as a major determinant of an inflammatory metabolic state. 59
This study has some limitations. The cross-sectional study design cannot be used to impute causality. Furthermore, we obtained dietary intake of the study participants using self-report questionnaire, which indicated measurement bias. Finally, we used 24-h food recall to collect dietary intake. Although this method has been widely applied, it depends on memory and under- or over-reporting might lead to imprecision.
In conclusion, our findings highlight the significant association between serum hs-CRP concentration in diabetics with and without hypertension and demonstrate that BMI and some dietary constituents including zinc, iron, sodium and cholesterol have a significant association with serum hs-CRP. Dietary calcium might have a protective effect against elevated hs-CRP in diabetic patients. More longitudinal studies, particularly randomized clinical trial using more population will be required to clarify the exact association between serum hs-CRP and dietary intake in diabetic patients.
Footnotes
Acknowledgements
The participation of the staff of Cardiovascular Research Center of the Mashhad University of Medical Science is gratefully acknowledged. We thank all the participants in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved and funded by Mashhad University of Medical Sciences (MUMS).
Ethical approval
This study was approved by the Mashhad University of Medical Sciences Ethics Committee; Reference number: 84135.
Guarantor
MGM.
Contributorship
MB and SSKH contributed equally to this work including study design, data management, data analysis and interpretation and writing the drafts of this project; AHB, ME, MS and MN: were involved in protocol development, gaining ethical approval, data collection and study conduction; GF: data interpretation and revision of the drafts. MGM and ME: Researched literature conceived the study and mentored all steps of the project. All authors reviewed and edited the manuscript and approved the final version of the manuscript.